
Abstract
Background:
Autistic people often face significant challenges in navigating health care systems, particularly during the vulnerable perinatal period. Many report inadequate care, feeling misunderstood, and being unsupported in addressing their health needs. We explored the pregnancy and early parenthood experiences of Autistic individuals in Australia, addressing the unique health care barriers they may face.
Methods:
To address the study aims, we interviewed 19 Autistic participants living in Australia about their pregnancy and early parenthood experiences. We conducted interviews using multiple modes, including written responses, virtual meetings, or phone calls to ensure accessibility. We analyzed the data using reflexive thematic analysis.
Results:
We constructed four key themes from the data. The first theme, “Pregnancy was good for me,” reflected feelings of body positivity and empowerment during pregnancy. Theme 2, “Hyperfocus as an understatement,” illustrated participants’ intense desire to gather information on every aspect of pregnancy and parenthood, which both facilitated and hindered their well-being. The third theme, “Lost in the system,” described the social drain caused by unpredictable health care interactions. The final theme, “Making things work for me,” detailed the coping mechanisms and strategies participants used to manage the demands of pregnancy and early parenthood.
Conclusions:
Our findings amplify the stories of competence and empowerment among Autistic parents, highlighting their experiences of resilience and agency in navigating these life transitions. It acknowledges the positive aspects of Autistic parenthood, which are often overlooked in research, and seeks to enhance the evidence base to inform health care practices that better meet the needs of Autistic parents. Importantly, these findings have broader implications for improving health care in other areas where Autistic people face similar challenges. By focusing on the localized experiences within Australia’s health infrastructure, this research provides insights that contribute to more effective inclusive health care interventions, ensuring that Autistic individuals receive the support they need during these critical life stages.
Community Brief
Why is this an important issue?
Autistic people often find it hard to get the right help from doctors and nurses, especially during pregnancy and early parenthood. Many feel that the care they receive is not good enough, and they often feel they are not understood or supported.
What was the purpose of this study?
We interviewed 19 Autistic people in Australia about their experiences during pregnancy and early parenthood.
What did the researchers do?
Our team was made up of Autistic and non-autistic researchers. A small group of Autistic parents served as advisors for the project. We talked to 19 Autistic people living in Australia about their experiences during pregnancy and early parenthood. They shared their stories through writing, online meetings, or phone calls to make it easy for them to take part. We then carefully studied what they told us to find common themes in their experiences.
What were the results of the study?
We found four main ideas from the information shared. The first idea, “Pregnancy was good for me,” showed that many reported feeling positive and strong about their bodies during pregnancy. The second idea, “Hyperfocus as an understatement,” described how participants wanted to learn everything about pregnancy and parenthood, which sometimes helped but also caused stress. The third theme, “lost in the system,” talked about how confusing and tiring it was to deal with frequent medical appointments with different nurses and doctors. The last idea, “Making things work for me,” showed the ways participants coped and found strategies to handle pregnancy and early parenthood.
What is new or controversial about these findings?
Our findings show that many Autistic parents feel strong, capable, and positive about their pregnancy experiences, despite the challenges and barriers. This is an important finding that celebrates the resilience of Autistic parents. The study also highlights the stories of Australian participants. This is different from other studies that included people from different countries.
What are potential weaknesses in the study?
This study only reflects the themes across 19 people, so their stories may not represent all Autistic people who experience pregnancy and parenthood in Australia. The results mainly reflect Australian experiences and might not apply to other countries with different health care systems.
How will these findings help autistic adults now or in the future?
Our findings show that Autistic people are strong and capable during pregnancy and parenthood. This research looks at the good sides of being an Autistic parent, which are often ignored. It helps health care workers understand how to better support Autistic parents. The study also gives ideas to make health care better in other areas where Autistic people need help.
Background
In recent years, there has been an increasing focus on the perinatal experiences of Autistic individuals within the health care system.1–7 Autistic* people have sensory and physical challenges distinct from their non-autistic peers, and the impact that they may have during the childbearing and rearing years is still poorly understood.8–10 Qualitative research exploring the birth and labor experiences of Autistic people consistently highlights challenges with health care interactions, unmet communication needs, and heightened sensory and physical experiences.2–5,8 Furthermore, emerging research indicates that Autistic people have a higher risk of prenatal depression and anxiety9–12 and report a lower satisfaction 6 with their prenatal experience, largely attributed to consequences arising from the Triple Empathy problem. 13 Navigating medical systems that are not designed to meet Autistic needs during this vulnerable time may intensify stress and anxiety while negatively impacting the quality of care received by both parent and infant, highlighting the importance of providing tailored support and services to this cohort. Finally, research shows that Autistic people face higher rates of pregnancy complications, including preterm birth, cesarean delivery, and preeclampsia.1,9,10 Despite this, significant gaps remain in our understanding of fertility challenges, pregnancy loss, 14 termination, and preterm birth 12 among Autistic individuals.
Beyond the challenges related to pregnancy, the first months of early parenthood can be similarly tumultuous for an Autistic person. Becoming a parent marks a major life transition for all individuals and families,15,16 bringing new challenges and routines that extend beyond, but are connected to, a person’s experiences of pregnancy. Early parenthood, defined for this study as the period immediately following birth and into the first 3 months of the child’s life, introduces distinct dynamics that reshape daily life, identity, and relationships. This phase encompasses postpartum recovery for the birthing parent, newborn care, bonding, adjusting to new roles and routines, and managing the emotional and physical changes experienced by all parents. 21 Autistic parents often face several challenges during this time, including feeling less confident in their parenting abilities, experiencing isolation in their parenting role, and challenges related to the bidirectional miscommunication that occurs between an Autistic parent and their health care provider.7,16 They also report disproportionately high interactions with child protective services and frequent questioning by service providers about their capacity to parent. 22 Many Autistic parents express a strong need for more support with parenting in general, as well as with specific skills such as breast/chestfeeding—where they often feel insufficiently supported.15,23 Autistic parents also report positive experiences of parenthood (e.g., reporting deep feelings of fulfilment in their role 7 ); however, these positive experiences are not frequently reflected in research.
While the extant research has provided a general overview of the pregnancy and parenthood experiences of Autistic individuals, much of the qualitative work that documents participant’s experiences has been conducted predominantly in the United Kingdom.2,6,8 The findings may not generalize to other contexts where health care systems can vary considerably. In Australia, factors such as implementation of a universal health care screen, broad uptake of supplementary private health insurance, the availability of midwifery services with emerging options for continuous care, and the option of shared care with general practitioners may shape unique experiences of pregnancy and early parenthood specific to the country.24–28 Therefore, this qualitative research aims to explore the health infrastructure available to Autistic individuals in Australia and contribute to the development of evidence-based practices that improve support during this significant life transition by addressing the following research question: What are the experiences of Autistic individuals in Australia throughout the stages of their pregnancy and early parenthood?
Methods
Positionality statement
This research was led by the Aspect Research Centre for Autism Practice (ARCAP), a participatory research center that includes Autistic and non-autistic researchers. The lead author (A.M.A.L.) is a non-autistic autism researcher, birthing parent, sibling to an Autistic young adult, and surrogate. Her own diverse birthing experiences as a same-sex parent with surrogacy experience influenced her role and desire to conduct this research, having personal experience confronting rigid health care systems that are one size fits all. She assembled an advisory team of Autistic individuals to make central the Autistic experience, comprising four parents and one midwifery practitioner. The advisors, who were compensated for their expertise, played a key role at critical stages, including study development, refining interview questions, data interpretation, article writing, and designing research outputs. Their contributions are further reflected in their authorship on this article. In addition to the advisory team, the broader research team included a midwifery practitioner and two midwifery researchers, whose recognition of the need for greater understanding helped shape the study and provided valuable context and insights.
Recruitment and participants
Following ethical approval from Griffith University Ethics Committee (GU Ref No: 2024/143) and The Royal Children’s Hospital Melbourne (HREC106159), we sought expressions of interest using social media and mailing list of ARCAP. Participants were required to be over 18 years of age, reside in Australia, be currently pregnant or have been pregnant in the last 5 years, and either have a formal autism diagnosis or self-identify as Autistic. If participants were currently pregnant, they were interviewed about their pregnancy experience and then contacted after birth for follow-up questions. If participants had already had their child or children, they were interviewed about both pregnancy and early parenthood during their interview.
We used questions on the expression of interest to determine eligibility. Out of 88 eligible participants who completed the expression of interest, we selected and invited 27 individuals for interviews through purposive sampling to ensure diverse representation across pregnancy types (e.g., multiples, singleton), geographic location (e.g., rural, metropolitan), pregnancy outcomes (e.g., termination, loss), ethnicity, and gender (e.g., non-binary, female). Five of those participants did not respond to the invitation, and the other four were eliminated for concerns around authenticity of autism diagnosis. This process resulted in 19 completed semi-structured interviews, with participants choosing their preferred interview mode—written, video, text, or phone—to enhance accessibility. Video and phone interviews ranged from 40 to 120 minutes (M = 68.9 minutes). Written interviews involved an interactive exchange to allow for question clarification. During the interviews, participants described their experiences with conception, pregnancy, and early parenthood. We recorded, transcribed, and pseudonymized the interviews and then imported them into NVivo 12 for analysis. Participants were compensated for their time with an e-gift card. The complete interview schedule is available in Supplementary Data. Of the 19 participants, 17 had a professional diagnosis of autism—10 of whom were diagnosed in adulthood—and 2 self-identified as Autistic. Participants identified as female (n = 15) and non-binary (n = 4) and were aged 26 to 42 (M = 33.6, SD = 4.7). Fourteen of the 19 participants reported having completed a tertiary qualification (see Table 1 for additional demographics), and 17 of the 19 participants had partners (including de facto relationships and marriages) at the time of the study. Seventeen of the 19 participants reported a co-occurring condition, with ADHD (n = 10) and anxiety (n = 10) being the most commonly identified. Other co-occurring conditions included depression, obsessive–compulsive disorder, anorexia and bulimia, sensory processing disorder, and fibromyalgia. Most participants who reported co-occurring conditions listed more than one. We have included these details, along with other demographic information, within the text to help preserve participants’ anonymity.
Participant Demographics
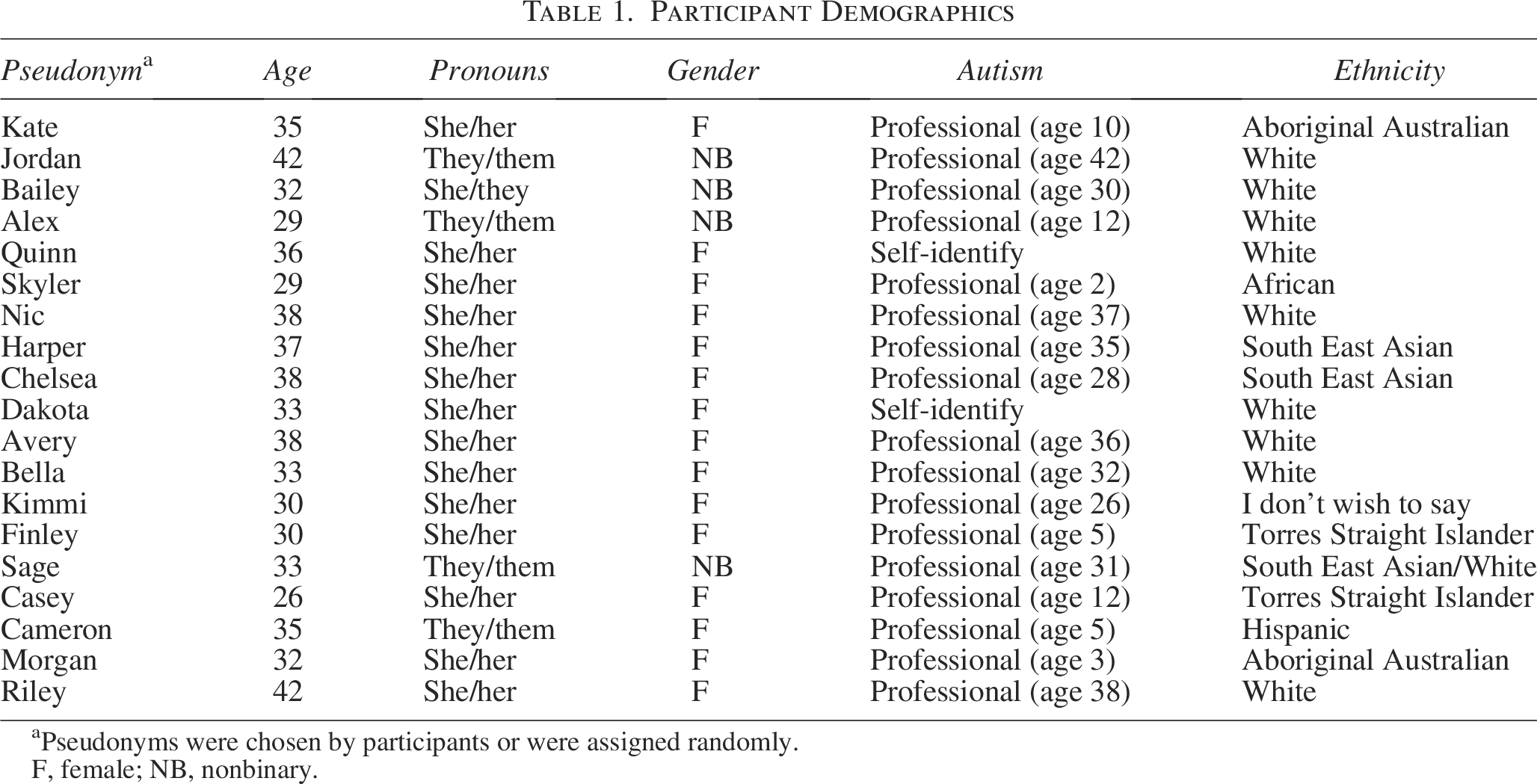
Pseudonyms were chosen by participants or were assigned randomly.
F, female; NB, nonbinary.
Data analysis
We conducted reflexive thematic analysis 29 to identify patterns of meaning across 19 in-depth interviews with Autistic participants from a range of backgrounds. This approach was chosen to center the voices of Autistic people in Australia who are pregnant, with the goal of constructing themes that convey their experiences and highlight the core ideas emerging from their stories.29–31 First, A.M.A.L. began familiarization with the data, coded the data using a combination of semantic and latent coding, and created patterns of meaning drawn from the dataset using an inductive process. After initial coding, A.M.A.L. met regularly with members of the research and advisory team to discuss and refine the codes. These meetings included both group discussions and one-on-one reviews, with particular input from B.R., an Autistic health care professional and researcher. The perspective of B.R. was central in shaping the findings, ensuring they reflected her perspective. The full research team and the advisory team worked collaboratively to refine the themes and ensure they authentically captured the participants’ experiences.
Results
We generated four themes from the stories shared by 19 people with diverse pregnancy and parenthood experiences (see Fig. 1). The quotes in this section have been reproduced verbatim and may contain grammatical errors.

Thematic map.
Theme 1: Pregnancy was good for me
This theme was central to the pregnancy experiences of many of the participants in this study, resonating throughout all stages of their journeys. For the majority, pregnancy was reported as a positive, transformative, and empowering experience that instilled a strong sense of purpose, pride, physical capability, and an overall reflection that pregnancy felt good.
Subtheme 1.1: I am competent
Participants reported feeling a sense of purpose and positivity during their pregnancies, enjoying their body changes and feeling “proud and good…and more beautiful” (Kate) than in their nonpregnant state.
I think I found myself quite almost a more healthier myself than I’d been before. I felt purposeful. I had something happening to me and I felt like it was really exciting that this new thing was going to happen… (Jordan)
Pregnancy fostered body positivity and a heightened awareness of positive body image, contrasting sharply with prior experiences of “awkwardness and body dissatisfaction” (Cameron) when not pregnant. Avery described these feelings of body positivity when reflecting on the time spent carrying her children:
I quite like being pregnant, the idea of having this other little being with you all the time. I don’t get concerned about body image, it’s a cool shape to be! It’s nice knowing that even when you don’t achieve much else on a given day you’re doing something for someone.
The positive body image also led to feelings of empowerment that were in sharp contrast to prior experiences, with participants frequently contrasting their pregnant selves with their nonpregnant identities. Avery described how “I have an incredibly busy mind and labour is one of those few experiences in life which is truly all encompassing where you can just be and just do what you need to do to cope with the challenges.” Nic talked about how pregnancy felt easy:
It was probably the first and sadly, only time just being able to get pregnant, and being pregnant and growing, that it was something that my body just did without me trying. Because everything else that I do in life requires a lot of effort on my part, and energy to have a somewhat successful outcome. But my body just did it and I didn’t have to [work hard for it.] It was just something that my body knew how to do.
Many participants reflected positively on their pregnancy, feeling “proud of my contribution” (Avery), “happy because I wanted to have a baby” (Bailey), and “hugely grateful” (Avery) for the experience. Bella shared how her pride and happiest moments came from “sharing that with [my partner]” and how that strengthened their connection and bond.
Subtheme 1.2: Social validation
Participants spoke of how their pregnancy heralded a period of positive regard and attention from their community, family, and colleagues. Nic said “I got a lot of accommodations from everyone when I was pregnant without having to justify it…without anybody questioning it.” She described: “People were all of a sudden, very caring… And all of a sudden, people did notice me. And I think that was nice as well for a change.”
Other participants also articulated the contrast between their prepregnancy and pregnancy experiences with others clearly, like Finley: “I felt like a queen bringing my baby home…I felt like I won a trophy. I got hosted and treated specially by my husband and community people. This had never happened before.” For some participants, this increased social validation was viewed as somewhat of a “double edged sword,” with the increased attention being accompanied by overwhelm and discomfort at times. Bella described this dichotomy:
I also found the kind of attention that I got from being pregnant difficult to deal with. We had to do the big reveal…And it was lovely, but it was really full on. Having the questions and just the general, the really high levels of excitement and lots of people. I don’t think I’ve talked to my family or my friends as much ever as I did in that kind of nine months, when they were like, “How are you going? Do you need anything?” So it was relentless…the questions and the extra attention, is what I found difficult.
Theme 2: “Hyperfocus as an understatement”
The majority of our participants reported that they engaged in extensive research on pregnancy and the health of their babies, which allowed them to channel all their thoughts and energy into their experience. However, this hyperfocus created issues in their day-to-day life as they struggled to find mental capacity for things that were not pregnancy or parenthood related.
Subtheme 2.1: Research helped me cope
All participants reported periods of hyperfocus. Harper jokingly described how she “was pretty focused, hyperfocused on the birth thing. But my partner, he seems concerned that he would call hyperfocus an understatement, I was so…I suppose, really, it was a full-time job for me.” This engagement in “huge amounts of research” (Avery) made them feel more prepared and helped them feel like they were doing everything right, as Kimmi explained: “I also did lots of research before so I knew exactly what I might expect so nothing was something I didn’t know they did.” Our participants enjoyed this process of researching because they “wanted to know absolutely everything about what it could be like and what could go wrong” (Avery). Quinn also talked about the benefits of researching:
You can still do that prep and still have issues, but, at least, if I did, I’d know where to go for the help as well. And so, that felt good to know that I knew next steps if it was needed… . Like I said, I really like to know the whys and ins and outs of things, makes me feel more sort of supported and in control… knowledge was really important for me, and feeling comfortable and supported to be able to get that knowledge. That was really important for me.
Participants were “planners” (Alex) and were able to take advantage of their ability to hyperfocus and research at times when they had difficulty posing questions or expressing concerns to health care workers. As Quinn described earlier, the research helped her feel more in control. However, she also reported feeling like she “ended up having to hunt for my own resources and stuff because I didn’t really feel comfortable asking questions and because they did not listen to me.” Another example was Dakota, who experienced a high-risk pregnancy that required frequent monitoring by medical technicians, some of whom provided limited communication regarding procedures being performed or the status of her babies. She described how researching gave her a sense of control and confidence:
I, as a result, had obviously done what every good person does and done a lot of research into when they’re looking at the different types of blood vessels, what sort of pattern they’re looking for in the vessels. The least I know what’s happening, because I found that otherwise, I was like, “What’s going on? Why is that one upside down? That one seems fast, that one seems slow,” but they’ve all been fine.
Subtheme 2.2: Research overwhelmed me
While hyperfocus was a coping mechanism that gave participants a sense of control, it also led to overwhelming and exhausting experiences. Riley discussed how the constant need to research, absorb, and analyze information became exhausting and contributed to feelings of burnout. This intense focus, while initially beneficial, sometimes drove participants “mad,” (Avery) as they struggled to balance their all-consuming interest in pregnancy with the demands of daily life:
I found it extremely hard to gauge what was and wasn’t normal for the pregnancy. It was an extremely stressful and frightening time for me where I was scared for the wellbeing of bub and trying to interpret a confusing array of contradictory and sometimes nonsensical advice on pregnancy and what to expect. (Sage)
Theme 3: “Stuck in the system”
Theme 3 was constructed around participants’ feelings of challenging health care interactions, with one participant describing the experience as feeling “stuck in the system” (Avery). They expressed how social and communication barriers to good care—such as “the system being so overstressed and communication so poorly organised”—led to them “bearing the emotional load” (Avery) as they navigated inconsistent and unpredictable care. This overwhelm came from the social drain of pregnancy, challenges with communicating their needs and concerns, and trauma arising from feeling misunderstood by health care professionals. This was particularly salient for participants who did not receive continuous care and saw a different nurse, midwife, and doctor at each appointment.
Subtheme 3.1: Social drain
Participants stated that the emotional burden and “the social drain of having to meet a fresh new person every time from scratch made the appointments much more difficult” (Avery), which they attributed to the unpredictability of care, often receiving care from different midwifes, nurses, or doctors throughout pregnancy. Participants often recounted how “when you go to the hospital it’s like no one’s read your file. And that happened a lot,” (Alex). The anxiety related to this was extreme for some. Bailey said, “I hated going to midwife appointments. I never saw the same midwife twice; there was a different one each time. I would be so anxious not knowing who I was going to see.”
Avery’s experience was similar: “I found having to meet a new person each time very stressful especially having to go through history and answer the same questions every time.” While some participants understood that this was just how the system worked, it still resulted in disabling social drain, which was challenging to manage while pregnant or in early parenthood. Without consistent care and the resulting anxiety from the appointments, participants reported feeling that they “didn’t know what was happening a lot of the time” (Bailey). It also meant that disclosure was not beneficial or unlikely to result in meaningful support: “I don’t feel like they would really respond. They wouldn’t care, but it just doesn’t feel like it would make a difference somehow” (Dakota).
Subtheme 3.2: Communication overwhelm
A key contributor to negative experiences in the health care system was communication challenges with health care workers. Communication was described as a “barrier” (Skyler), and the ability to express themselves was compounded by sensory overload, stress, and anxiety. Many participants noted that appointments felt “quite rushed” (Dakota), and they often had to advocate assertively for their individual needs, which felt overwhelming. Bella mentioned that she didn’t want to “be too much of a pain,” a sentiment many participants attributed to societal pressures, particularly for Autistic women, to avoid being perceived as demanding. Participants were generally not confident in voicing their needs, which was summed up by Alex:
I find it hard to communicate because I’m being super polite and I don’t let people know when I need something, because I don’t want to disrupt them or impose something. But then I just get frustrated, and I get angry, and I get upset, but I internalize it all…So I can be waiting a long time for something that I need and it becomes unbearable. But then in hindsight I recognize it and I recognize that I should have spoken up.
For many, the challenge of communication went beyond expressing needs—it was also the extensive mental preparation required before each appointment which for many involved scripting responses (e.g., mentally rehearsing or preparing written notes around what to say in advance), researching topics, managing anxiety, and preparing to mask autistic traits. Avery noted that these appointments felt like an extra “thing on” her already full plate, often leaving her too drained to function afterwards. Some participants relied on partners or family members to communicate on their behalf, with mixed results. Alex shared:
Sometimes I need to speak to my mum or a support person in order for them to just talk for me, otherwise I’ll just get more and more anxious or frustrated and then upset. And then by that point, no one understands what’s happening. I’m just upset.
Issues such as “brain fog” (Avery), situational mutism, and challenges in “being able to articulate” (Riley) their concerns caused “the most anxiety” (Riley), making it harder to communicate. Participants often struggled to keep up with the pace of appointments, and redirecting conversations to focus on their priorities was an added challenge. They also reported pressure to be “super polite” (Alex) and mask their true feelings—“I’m very good at masking, 39 years of masking, I’m good at it” (Chelsea). The need to quickly process medical terminology and come up with questions on the spot added another layer of difficulty. As Finley described during labor, “I had difficulties understanding labor terms like pushing. The midwife and the doctors helped me, but it was difficult.” Participants reported that interactions became more manageable when they had time to process information and prepare, particularly when health care professionals communicated “clearly and calmly without social fluff and over the top emotions” (Sage).
Subtheme 3.3: “It kind of eroded my trust gradually.”
Unsurprisingly, health care that was not aligned with participants’ needs during a vulnerable time like pregnancy contributed to increased experiences of distress and burnout. Participants expressed frustration over health care workers who “did not trust my own experience of my own body…and just thinking I was being dramatic or whingey” (Avery) or doctors who “completely dismissed my disability needs and expressed fears” (Sage). Chelsea described seeing various doctors who were “very dismissive and went, ‘You can talk, you’re fine.’ So they would actually send me home.” Being dismissed or not taken seriously heightened participants’ frustration and often distress. Over time, these interactions contributed to participants’ experiences of trauma, as they felt invalidated or ignored in their health care interactions, which “kind of eroded my trust gradually because I didn’t believe everything” (Alex). Avery described how her lactation consultant ignored her attempts to communicate:
I had a terrible experience with a lactation consultant coming to help me hand express and me trying to politely tell her that no thank you I didn’t want her to “show me how” and her literally milking me without my consent and I was just in such shock that I sat there trying to be nice about it. I cried for hours after that. I assume there’s some weird social norm where people think “no thank you” means that people actually do want help but are trying to be nice when in reality I am trying to be nice by saying no thank you instead of saying “no, fuck off.” (Avery)
Alex described how, despite creating “a very clear plan of what I could and could not cope with,” and communicating that multiple times to allied health professionals involved in their care, they ultimately consented to an examination that directly contradicted the boundaries they had previously established. Reflecting on this experience, Alex stated, “Because I had said, ‘No,’ so many times. But over, I guess, a few weeks of saying, ‘No,’ eventually I had a midwife that didn’t listen, and so it was hard to say, ‘No,’ again.”
Theme 4: Making things work for me
Theme 4 was constructed from participants’ experiences of supportive care and low-demand environments. Hospitals, clinics, and doctor’s offices were challenging due to lights and smells, and many participants described the sensory challenges in hospitals as difficult and unbearable. In response, they devised strategies for themselves to transform these high-demand environments into more manageable low-demand settings.
Subtheme 4.1: Avoiding invasive testing and interventions
Subtheme 4.1 described how participants minimized their exposure to invasive testing or often held an “anti-interventionist” perspective (Riley). Avery described feeling frustrated by doctors who “kept asking us if we wanted further invasive testing despite research not indicating there was any reason to based on our baby’s condition.” She “wanted to do whatever was within my power… .which meant avoiding a lot of interventions.” Bailey’s experience was similar. She shared that she “didn’t want to be cut open and didn’t want an epidural” because she did not want excessive touch and many wanted to reduce the interventions.
Avoiding invasive procedures, or procedures in general, helped participants manage sensory sensitivities and reinforced their sense of control during an already physically and emotionally challenging time. Bella, for instance, shared her own sensory sensitivities: “I was a bit touch sensitive, particularly with strangers,” which made the “blood tests, and the measuring, and poking and prodding” during appointments overwhelming and heightened her anxiety.
Subtheme 4.2: “I’m a planner”
All participants valued clear plans: “I’m a planner, so everything is known when it can be” (Alex). Participants stated that having a “plan of preferences” (Avery) and “birth plan was a must cos with my autism I need to know exactly what’s going to happen” (Harper). For the participants in this study, the traditional “birth plan,” which happens around 8 months and is a short conversation at one appointment, was insufficient. Riley described this by saying:
I think for me and maybe for other neurodivergent people, it would be useful to have a really clear timeline from the start. And also the why. Because why aren’t we planning now? This seems really silly. I’ve got nine months, people. And for them there’s probably clear reasons why and everything, but I didn’t know that, so it made me quite upset.
For participants, planning meant being “prepared for what to expect for things that they couldn’t change” (Bella). Many participants appreciated receiving “one-on-one sessions” (Bailey) or “pictures of the room” (Bella) and speaking to professionals like the anesthetist beforehand to “explain the procedure, and then I also wanted to see her in person because sometimes I struggle to take in everything” (Alex). They also valued extra time spent “explaining things in a little more detail” (Bella), particularly regarding surgical procedures, medications, and who would be in the room for different appointments. “We also had stuff in the birth plans that was all about me anticipating what my sensory and social needs would be in a difficult situation” (Avery). Finally, planning also meant requesting accommodations, such as “low lighting and I didn’t want anyone to talk to me…or be touched by anyone except partner and birth support unless medically necessary” (Avery) and keeping “the minimum number of people needed in the room… knocking before you walked in” (Bella).
Discussion
The current study aimed to understand the pregnancy and early parenthood experiences of Autistic people in Australia. Overall, our findings amplify the stories of competence and empowerment among Autistic people during pregnancy and early parenthood, highlighting their resilience and agency in navigating these life transitions despite experiencing significant barriers throughout their health care interactions. While challenges were present—primarily due to barriers within Australia’s health care system 24 and the resulting heightened anxiety and stress—the collective narratives also revealed a strong sense of purpose and resilience. These stories highlighted how participants draw on their unique perspectives and experiences to navigate adversity and thrive. This emphasis is inconsistent with previous research focusing primarily on the challenges and barriers that Autistic people experience during pregnancy and early parenthood. 7 This new finding highlights a significant shift in understanding the experiences of Autistic individuals and aligns with recent calls by the Autistic community and researchers to recognize the strengths, resilience, and agency of Autistic people and to advocate for environmental changes and autism-friendly practices, moving away from a primarily deficit-focused narrative.32–34
Autistic participants in our study reported feeling competent and positive about their bodies and capabilities during pregnancy, describing their experiences as rewarding despite the challenges. They also noted a significant shift in social perceptions and support during pregnancy, contrasting sharply with their usual experiences, which highlighted newfound recognition and care from others. This shift has important implications for health care professionals. Autistic individuals often face barriers to parenthood, including increased scrutiny and frequent interactions with social services. 1 Systematic reviews of the topic tend to emphasize the difficulties and dissatisfaction they encounter, leaving medical professionals with limited understanding of how to leverage their strengths. Rather than questioning their capabilities, health care providers should seek to understand how being Autistic shapes their pregnancy and parenthood experiences, fostering trust and supporting their ability to flourish as parents. 35 Furthermore, health care practices must adapt to meet the needs of Autistic individuals, aligning with calls for more autism-friendly health care—a request that has been widely recognized in previous research.
Theme 3 highlighted the communication fatigue experienced by participants and the challenges of navigating Australia’s public health care system, where continuity of care is not always available. This is not unique to Autistic people; the additional burden of meeting new people, unpredictability, and anxiety about health care providers’ knowledge and attitudes toward autism makes it particularly impactful for them. Participants in our study reported experiencing anxiety, loss of trust in their health care professionals, and added stress when they were dismissed by their clinicians. Participants’ experiences discouraged them to disclose their autism to health care workers, which aligns with previous work on Autistic disclosure.36,37 Although the barriers and needs related to continuity of care for Autistic people are well-documented,24,38 our findings underscore the profound impact these challenges can have on mental health.
For Autistic individuals, continuity of care appears to be a particularly valued approach. Participants who received continuity of care reported its positive effects, whereas those who did not described how the absence of consistent providers exacerbated their social and communication challenges, contributing to barriers in care and eroding trust. Our findings suggest that continuity of care could mitigate these issues, fostering better communication and rebuilding trust in the health care system. Importantly, participants in this study also recognized and valued positive care experiences, demonstrating that they are clear about what good care means to them. Given the historical overreliance on proxy reporting in research evaluating the health care experiences of Autistic people, particularly in a community already vulnerable to systemic marginalization, these firsthand accounts are especially critical.39,40 Their lived experiences should be understood not only as valid but also as essential contributions to shaping more responsive and equitable health care systems.
Strengths and limitations
Although this study is strengthened by the diverse experiences and deep qualitative analysis, several limitations exist. The study reflects the stories of 19 individuals who are Australian and highly educated (14 out of 19 reported some tertiary education). Therefore, their experiences may not represent the diverse experiences of all Autistic people who experience pregnancy and parenthood. Each participant’s experience was influenced by their unique contexts, including geographical and cultural factors; however, these were not analyzed as part of the study beyond reporting them to the reader. The findings deeply reflect the Australian context and cannot be generalized to international contexts without considering the different medical contexts. In addition, the reliance on self-reported data may introduce bias, as participants might have provided responses influenced by social desirability or retrospective recall. The nature of qualitative research, which often involves deep personal and subjective narratives, can be influenced by retrospective recall. However, we included participants in this study who had been pregnant within the last 5 years and selectively recruited from our eligible participants to include people who were currently pregnant, had just had their baby, and had been pregnant in the last few years. This purposive sampling aimed to get a balanced picture of what Autistic people in Australia were currently experiencing.
Avenues for change
In Australia, efforts to implement a national indicator for disability identification—specifically how women are asked about their disability status—have been inconsistent, with non-standardized documentation across services. Developing national guidelines for identifying disability among women accessing maternity care, and making this data collection routine, is a critical first step toward systemic change.
26
Without reliable data on the number of Autistic parents giving birth in Australia, it will remain difficult to secure targeted funding or influence policy reform. At the individual service level, hospitals can begin by training staff in neuro-affirming approaches and autism awareness. Autism-friendly care that takes a strength-based perspective and prioritizes individualized support and reasonable accommodations is essential. In Australia, challenges our participants experienced relating to their interactions with health care workers such as rushed appointments, a lack of continuity, and a need for effective communication are deeply embedded in the health care systems, policies, and broader societal and cultural frameworks that support professionals. Addressing these challenges requires changes not only within health care settings and the people who work there but also in the systems and policies that underpin them. Recommendations from emerging neuro-affirming health care research34,38,41 suggest that health care environments can be improved for Autistic people by (1) improving predictability at appointments, (2) addressing sensory processing differences by adjusting things like waiting rooms or lighting, (3) enhancing patient–professional communication through clear, unambiguous language and written follow-up, (4) autism acceptance supported by belief in a strength-based framework of care, and (5) increased empathy toward Autistic patients.
26
Building on these existing recommendations which were all supported by our findings, we offer several practical changes to improve care for Autistic individuals during pregnancy and early parenthood, including:
Expanding birth planning documents to support Autistic people throughout the pregnancy and early parenthood journey, considering communication styles, sensory preferences, and planning needs Ensuring that health care providers are well-informed about individual needs by thoroughly reviewing patient files and providing extra time at appointments Recognizing the inherent capabilities of Autistic people as parents Supporting Autistic individuals’ need for information and research by providing neutral, research-based resources in accessible formats Documenting key points from appointments and sharing them, along with proactive information and references, to minimize the need for extensive research thereby reducing the anxiety-inducing effects of hyperfocus Promoting continuity of care by fostering consistent provider relationships to build trust and reduce communication fatigue Understanding and respecting participants’ preference to avoid invasive testing, minimizing excessive touch, and supporting their confidence in their bodies’ capabilities
This practical list and the findings from our study emphasize the importance of a tailored empathetic approach to care for Autistic individuals during pregnancy and early parenthood. By valuing Autistic individuals’ strengths, providing accessible information, fostering continuity of care, and prioritizing autonomy, health care professionals can create a more supportive and empowering health care experience. These practices not only enhance patient trust and well-being but also address the specific needs and preferences of Autistic individuals, promoting a more inclusive respectful approach to perinatal care. Bailey shared a crucial perspective—a call for health care professionals:
They think that autism is bad and assume that I must think the same, despite being autistic myself. Health professionals must think of autism like a disease, where you can live with it, but you would rather your kids not have to. But if instead they just thought of it as a different neurotype, with its own strengths and challenges, then maybe they could be more supportive of helping us find out what works best for our family.
Conclusions
This study enhances understanding of the pre- and postnatal experiences of Autistic people, filling a critical gap in maternal health care knowledge. Importantly, these findings have broader implications for improving health care in other areas where Autistic people face similar challenges, emphasizing the need for more inclusive and effective care to enhance quality of life. As an outcome of this research, our team developed an Australia-first digital platform offering resources for both Autistic women and the practitioners who support them (www.aspect.org.au/new-parents). The platform was codeveloped along with a team of Autistic parents who have guided the life cycle of this project. The platform aims to increase the knowledge and confidence of Australian maternal health care professionals, while also offering Autistic people validation and shared experiences of pregnancy and early parenthood. With evidence informed resources, policies at the hospital level can begin to be changed leading to more system-wide changes. Enhancing autism awareness and understanding of neuro-affirming health care practices (e.g., Doherty and colleagues SPACE Framework 41 ), actively listening to Autistic people’s stories, and collaborating to guide changes in care will result in improved pregnancy and early parenthood outcomes.
Footnotes
Author Disclosure Statement
The authors do not have any conflict of interest to disclose.
Funding Information
This project was funded by the Victorian State Government (FR-14372) Diverse Communities Mental Health and Wellbeing Grants Program, The Woodend Foundation, as well as the auDA Foundation 2023 Community Grants.
Authorship Confirmation Statement
A.M.A.L.: Conceptualization, investigation, data analysis, writing—original draft and review/editing, visualization, and project administration. B.R.: Design, data analysis, provided critical feedback on the article, and participated through the study as a member of the advisory team driving the research. R.Y.C.: Design, conceptualization, writing, data collection, and provided critical feedback on the article. C.B.: Served as a content specialist and provided critical feedback throughout the research and article. L.H.: Design, provided critical feedback on the article, and participated through the study as a member of the advisory team driving the research. H.C.: Design, provided critical feedback on the article, and participated through the study as a member of the advisory team driving the research. G.M.: Design, provided critical feedback on the article, and participated through the study as a member of the advisory team driving the research. C.E.: Design, conceptualization, editing, and provided critical feedback on the article. A.R.: Design, provided critical feedback on the article, and participated through the study as a member of the advisory team driving the research. V.G.: Design, conceptualization, editing, and provided critical feedback on the article. The article has been submitted solely to this journal and is not published.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.