
Abstract
Background:
Autistic adults often experience high levels of stress and difficulties in coping with stressors in everyday life. The aim of this study was to evaluate the effectiveness of mindfulness-based stress reduction (MBSR) groups, adjusted for autistic adults in an outpatient context.
Methods:
We conducted a two-arm, parallel-group, randomized controlled effectiveness trial during the years 2018–2020. Autistic adults (N = 77) were recruited from outpatient services and randomized to either MBSR (n = 39) or treatment as usual, TAU (i.e., continued regular services, n = 38). We used linear mixed models with random intercept to analyze the effects of intervention on self-rated perceived stress (primary outcome), as well as mental health, mindfulness skills, quality of life, and autism acceptance (secondary outcomes). In addition, we collected qualitative data at exit discussions in the MBSR groups and examined the transcription using thematic content analysis.
Results:
Participants (52% female) had a mean age of 40 years, with a majority being unemployed at the time of inclusion (64.9%) and having at least one co-occurring psychiatric diagnosis (87%). The completion rate in the MBSR group was 81%. A comparison of the slopes of the two groups showed a greater reduction of perceived stress from pre- to postintervention in the MBSR group than in the TAU group (Perceived Stress Scale total score: between-group effect size d = 0.55 [0.20–0.90] at postintervention and d = 0.61 [0.13–1.10] at the 3-month follow-up). Likewise, symptoms of mental health problems decreased more in the MBSR group (Hospital Anxiety and Depression Scale total score: between group d = 0.64 [0.23–1.05] at postintervention and d = 0.70 [0.14–1.26] at the 3-month follow-up). No changes in autism acceptance or general quality of life were observed in this study. Qualitative analysis indicated that participants perceived the MBSR group as inclusive and safe. Moreover, they appreciated both the conveyance of mindfulness techniques and the change in their approach (a “new mindset”) regarding stress. The participants also reflected on the challenges of continued practice after completed intervention.
Conclusions:
The MBSR groups for autistic adults may be an effective intervention in a clinical context. Future studies should examine the facilitators and barriers for the long-term maintenance of the acquired benefits.
Community Brief
Why is this an important issue?
Autistic adults often experience high levels of stress and difficulties in coping with everyday stressors, such as sensory overload or social stressors. Mindfulness-based stress reduction (MBSR) is a group program that promotes the ability to be in the present moment (mindfulness) and related techniques for coping with stress. The program is based on mindfulness exercises and experiences rather than lectures.
What was the purpose of this study?
The purpose of this study was to evaluate the effectiveness of the MBSR groups for autistic adults in an outpatient health care context.
What did the researchers do?
The 77 participants in the study were randomly assigned into one of the two study conditions: 39 participants took part of the MBSR group while 38 participants continued their treatment as usual (including, for example, medical treatment, physiotherapy, occupation therapy, or counseling). Those participants who were randomized to continued treatment as usual could take part in the MBSR program during the following term. In this study, MBSR was adjusted for autistic adults’ needs following previous participants’ feedback.
We used self-report questionnaires to collect data before and 3 months after the program. In addition, we recorded group discussions at the end of each MBSR group, to collect the participants’ views and lived experiences.
What were the results and conclusions of the study?
Participants had a mean age of 40 years and 52% of them were female. Most participants (64.9%) were not studying or working at inclusion, and 87% had at least one co-occurring psychiatric diagnosis. In the MBSR group, 81% of the participants completed the program.
When we compared self-reported stress in the two groups (MBSR and treatment as usual), we found that participants in the MBSR group received greater benefit from the program than those who received continued treatment as usual. The MBSR group participants experienced improved stress coping and mindfulness skills. Moreover, well-being increased more in the MBSR group. However, there were no changes in autism acceptance or general quality of life, in either of the two groups.
What is new about the findings?
This is the first effectiveness study of MBSR for autistic adults conducted in an outpatient setting and showing positive effects on stress reduction and well-being. In the group discussions, the participants in the MBSR group described that MBSR provided important hands-on tools for coping with stress. They also experienced a positive change in their “mindset” or approach to stress, and their own thoughts and reactions in stressful situations. The participants also discussed the challenges of continuing with mindfulness training and maintaining the skills learned after finishing the program at the clinic.
How will these findings help autistic adults now or in the future?
The MBSR groups for autistic adults may be a helpful support for autistic adults with high levels of stress in everyday life and co-occurring mental health problems. Aside from a clinical setting, as in this study, the program might also be suitable for other contexts.
What are potential weaknesses in the study?
Since the follow-up time in this study was only 3 months after the program, future research should examine if the acquired mindfulness skills and a new approach to stress hold over longer time.
Introduction
Adults diagnosed with autism spectrum disorder without intellectual disability (henceforth referred to as autistic adults) report many lifetime stressors and frequent experiences of stress in everyday life.1–3 Stressors denote perceived challenges and threats to social, psychological, or physical well-being that elicit a multilevel stress response (i.e., stress). For autistic adults, stress can arise from poor adjustment for their needs in many everyday settings (e.g., sensory overload), economic challenges, challenges with uncertainty and emotion regulation, as well as camouflaging as a response to stigma and minority stress.3–9 The individual’s appraisal of a stressor and the subsequent stress responses are associated with their perceived internal and contextual resources, for instance, an individual’s ability to cope with the challenges and social support. 10 However, autistic adults report difficulties in coping with everyday challenges, 1 and they may have poor access to support from others due to social exclusion and poor social outcomes.11,12 While experiences of some difficulties and obstacles are part of everyday life, long-term stress (repeated and maintained stress responses) is known to have negative cumulative effects on mental and physiological health. Mental health problems are common in autistic adults: a majority of autistic adults experience one or several co-occurring psychiatric conditions during their lifetime, including, for example, depression and anxiety disorders, as well as suicidal behaviors.13–15 As chronic stress is a risk factor for mental health challenges, interventions for stress reduction are pivotal to increase resilience and promote long-term well-being for autistic adults.2,11 Although still an emerging research field for autistic adults, the mindfulness-based stress reduction program (MBSR) 16 has been suggested as a promising option for stress reduction and improved mental well-being. 17
MBSR is a group-based mind–body intervention that aims at cultivating focused attention (awareness) to the experiences in the present moment and fosters a nonjudgmental approach (accepting and nonreactive) and curiosity toward the contents of these experiences. While not suppressing thoughts, MBSR encourages experimental defusion (dereification of internal experiences), for example, observing thoughts as mental events and not as real objects in the world. Furthermore, mindfulness meditation may facilitate a shift in self-related processing, for example, perceiving self as changing in relation to their context at the current moment, as well as increased compassion toward self and others. MBSR was initially developed for people with chronic pain, but has since been evaluated for various conditions such as depression, anxiety, and substance use 18 as well as work-related stress. 19 For autistic adults, however, the studies are still few.
Previous studies on MBSR and closely related interventions20–27 have shown promising preliminary results in reducing mental health problems in autistic adults. Most of the studies on MBSR have been rather small, often not including a control group or including groups of autistic adults who are not representative of those encountered in outpatient settings. Nevertheless, one study evaluated the effects of MBSR on perceived stress and coping difficulties in an outpatient setting 20 and despite a high level of psychiatric co-occurrence among the participants, they reported improvement regarding stress-related distress and coping difficulties at postintervention. However, given the open study design, no strong conclusions about the program’s effectiveness could be drawn.
Further evaluation of the MBSR in clinical settings is warranted to assess the program’s effectiveness in those contexts where future implementation can be planned. Since health care organizations struggle with providing effective support for autistic adults, we need methods that could both alleviate stress and prevent negative long-term effects on health and well-being. Autistic adults met in clinical settings often present with co-occurring mental health problems and social challenges and the delivery of interventions should be adjusted for their needs. 28 As previously emphasized, 12 the views of autistic people should be considered in treatment tailoring to improve acceptability and accessibility. Similarly, qualitative data could be used to gather autistic adults’ lived experiences of adjusted MBSR and their thoughts about continued practice postintervention. Although the studies within this field have so far mainly applied quantitative study designs, some qualitative data have stressed the importance of the group consisting of autistic individuals as well as inclusive and respectful setting and group facilitators. 29
The MBSR program evaluated here followed the original program contents, but the delivery was adjusted for autistic participant’s needs, 20 as described in the following section. The aim of the current study was to evaluate the effectiveness of the MBSR for autistic adults without intellectual disability, in an outpatient habilitation services context. More specifically, we evaluated whether the MBSR group participation would be associated with greater change in perceived stress (primary outcome), mental health problems, quality of life, mindfulness skills, and acceptance of autism diagnosis (secondary outcomes) from pre- to postintervention. Moreover, we conducted an additional qualitative analysis of postintervention group discussions regarding the lived experiences of MBSR group participation.
Methods
Study design and the clinical setting
We conducted a two-arm, parallel-group, randomized controlled effectiveness trial during the years 2018–2020, in the context of Region Stockholm, Sweden, publicly funded outpatient services for autistic adults. The outpatient services in Region Stockholm are organized to include separate care providers for habilitation (focusing on building functioning capacities in everyday life and active participation in life situations) and psychiatric health care (focusing on mental health problems). This effectiveness study was conducted at two outpatient habilitation service centers, recruiting from routine care and employing ordinary clinical staff. The participants in both conditions had ongoing services during the trial, for example, pharmacotherapy for mental health problems. The participants were randomly allocated to either MBSR or to continued treatment as usual (TAU), with a possibility of taking part in the MBSR program during the following term. The trial was approved by the Ethics Review Board in Stockholm (reg.no. 2018/1190-31) and the study was conducted in accordance with the Declaration of Helsinki. The trial was registered in the Clinical Trials (clinicaltrials.gov, reg.no. NCT05244265). All participants provided informed consent to participate.
Recruitment and inclusion procedure
Potential participants were reached through clinicians at habilitation centers in Region Stockholm as well as through the centers’ regular information channels such as websites, print materials, and waiting room brochures. The participants could then be self- or clinician referred to the screening at one of the outpatient habilitation centers involved in the study.
The screening session consisted of 60–90-minute structured individual interviews at the habilitation center, conducted by an experienced clinical psychologist and one of the MBSR teachers. First, the potential participant was informed about the intervention as well as requirements for participation in the research project. Second, the inclusion/exclusion criteria were assessed. As part of the screening, the participants also completed the Montgomery–Asberg Depression Rating Scale. 30 Lastly, medical electronic record data were retrieved for information on co-occurring psychiatric diagnoses and psychoactive drug prescriptions.
Designed as an effectiveness study, we aimed at including a sample of autistic adults, representative of outpatient unit clients. The inclusion criteria were as follows: having been diagnosed with autism (confirmed through patient case files, or assessment report), being ≥18 years old, able to participate in the group sessions, and understand the Swedish language. The exclusion criteria were as follows: diagnosis of intellectual disability, severe psychosocial life circumstances (e.g., being homeless), or having a severe psychiatric condition (e.g., acute suicidal behaviors or psychosis) that would hinder participation. The judgment of eligibility was made by the clinicians conducting the screening interviews.
The included participants received detailed written information regarding the project, the procedures, and the intervention, and were invited to a separate meeting for baseline assessments. Here, the participants got further oral information and were offered the opportunity to ask questions. Subsequently, the participants eventually provided consent for participation, completed baseline assessments, and were then randomized to either the MBSR group in the same term or to TAU, with a possibility to take part in the MBSR group during the following term.
Randomization
The participants were randomized in a 1:1 ratio in four separate blocks of up to 20 participants in each block. Randomization was conducted by a researcher not included in the T1 assessments, using an online random number generator (http://www.random.org). Neither the clinicians nor the participants were aware of the allocation at the time point for T1 assessments. After the T1 assessment, the allocation was revealed by opening the opaque envelope containing the information.
Power analyses
A sample size of 100 participants was required to provide 80% power (1-β) at a two-sided 5% α-level, with expectations of a medium-to-large effect size on the primary outcome. 20 However, the last block of participants to be randomized (planned September 2020) was not recruited due to the COVID-19 pandemic that made all group interventions impossible to conduct at habilitation centers. Therefore, 87 participants were assessed for eligibility, approximately 20 participants less than planned.
Measures
The participants completed a questionnaire assessing their sociodemographic and other background data, 31 while their diagnosis and use of psychoactive medicines were extracted from their clinical case records. The outcome variables were assessed at three time points: baseline (time point 1, T1), postintervention (T2), and 3-month follow-up (T3). All data were stored in an individual case report form (CRF), separate from the clinical case files.
Primary outcome
The primary outcome measure was the total score of the 14-item Perceived Stress Scale (PSS), 32 rated on a five-point (0 to 4) Likert scale, with higher scores indicating more perceived stress. The 14-item version of the PSS (score range = 0–56) was used to enable further analyses of the two PSS subscales 33 : perceived distress (seven items, scoring range 0–28, e.g., feeling nervous, stressed, upset, or out of control) versus perceived coping difficulties (four items, scoring range 0–16, e.g., confidence in own ability to handle personal problems, everyday hassles, or important changes). In this dataset, the internal consistency of the PSS was good, Cronbach’s α = 0.87 at T1.
Secondary outcomes
The Hospital Anxiety and Depression Scale (HADS) is a 14-item questionnaire scored on a Likert scale (0–3) reflecting symptoms of anxiety and depression.34,35 The total score of the HADS ranges from 0 to 42, with higher scores indicative of more symptoms. The cutoff score for clinical symptom severity is ≥14. 36 The HADS has two subscales, each consisting of seven items (score range 0–21), and indicating the level of anxiety and depression symptoms, respectively. On both subscales, a score ≥8 represents clinical symptom severity. The internal consistency of the HADS was excellent in current data; Cronbach’s α = 0.93 at T1.
The Satisfaction with Life Scale (SWLS) is a five-item measure of general quality of life. Items are scored on a seven-point Likert scale (1–7, total score range: 5–35), with a higher score indicating more satisfaction with life. 37 The internal consistency of the SWLS was good; Cronbach’s α = 0.84 at T1.
Acceptance of autism was measured using a modified version of the Acceptance and Action Questionnaire-II (AAQ-II) 38 previously used for autism acceptance. 39 Its seven items are scored on a 0–7 Likert scale (total score range 0–49), higher scores indicating more difficulties in accepting their autism (e.g., feeling uncomfortable about the diagnosis and perceiving it as a hinder in life). In the current dataset, the AAQ had good internal consistency; Cronbach’s α = 0.88 at T1.
The Five Facet Mindfulness Questionnaire (FFMQ) 40 reflects the ability to act with awareness, observing and describing intrinsic and extrinsic events in a nonjudging and nonreactive manner. The Swedish version of the FFMQ 41 consists of 29 items, scored 1–5 on a Likert scale (total score range: 29–145), with higher scores indicating better ability to act with awareness. A clerical error at T2 for one of the randomized blocks (more specifically, error in copying of the FFMQ in the CRFs) resulted in large amounts of missing data (i.e., n = 15 participants missing 48% of FFMQ data at T2; these participants were from both the study groups). Therefore, these participants’ data were excluded at T2, and we only analyzed the FFMQ at the total score level in this study. The FFMQ had good internal consistency in the current data; Cronbach’s α = 0.78 at T1.
Secondary additional outcome: Treatment feasibility and participants’ lived experiences
Treatment feasibility was measured as (1) treatment completion (number of participants who started the treatment and attended at least five of the ordinary eight sessions, i.e., 63% of the sessions) and (2) adverse events (any inconvenience that participants spontaneously reported) and serious adverse events (any event requiring inpatient hospitalization) recorded in the individual CRF.
Moreover, qualitative feedback was obtained from the MBSR group through a semistructured group discussion at the end of the intervention period. The exit group discussion addressed the participants’ experiences of mindfulness practice, including their perceived benefits and factors facilitating and hindering their active participation in the MBSR program. Moreover, factors affecting continued mindfulness practice postintervention were discussed.
The MBSR intervention
The MBSR intervention16,42,43 followed the contents described in the treatment manual, while the delivery was adjusted to the needs of autistic adults based on feedback from previously participating autistic participants. 20 Briefly, the adaptations included the following: limiting group size to 8–10 participants; allowing immediate entry to the intervention room to avoid the waiting area; adjusting or removing sensory stimuli (e.g., ticking clocks, strong scents, bright lighting); assigning each participant a designated spot for the entire program; providing written agendas on a whiteboard for clarity and predictability; having two MBSR teachers to enable individual support in a separate room if needed; using clear, concrete language free from metaphors; removing metaphors from program content; giving full instructions for all exercises, even if previously covered; including a scheduled 15-minute break in each session; shortening some of the meditations to 10–25 minutes to support participants prone to restlessness, while maintaining the total duration of formal exercises (with repetitions added if needed); limiting the silent retreat to 5.5 hours, scheduled in a separate week; abbreviating workbook materials and providing audio recordings of exercises; and supporting voluntary homework planning upon request.
The program included MBSR orientation followed by eight weekly group sessions (classes) and a 1-day (5.5 hours) silent retreat. The intervention provides formal (such as yoga, sitting meditation, body scan, and walking meditation) and informal mindfulness techniques (e.g., mindful eating, speaking and listening, and mindfulness of daily activities). Moreover, the program includes psychoeducation about stress, opportunities for reflection and reappraisal regarding own responses, challenges and strengths, as well as what it means to take care of ourselves and flourish.16,43The sessions one to five were primarily focusing on experiential learning of mindfulness meditation and yoga, as well as exercises cultivating acceptance and nonjudgmental appraisal of challenges, pleasant events, and own reactions. The sessions six to eight focused more on implementation of mindful awareness in everyday life, by observing their reactions and needs at the present moment and choosing an exercise based on these observations. Thus, the aim is to nourish behaviors and activities that express our innate capacity for well-being. 43
The MBSR teachers
The MBSR teachers were regular staff members from the habilitation centers, experienced in working with autistic adults. The teachers had further MBSR training by the Center for Mindfulness Sweden following international standards (iminetwork.org): at least one of the two teachers guiding each group was trained to level 1 of teacher training, and the other at least under training toward level 1. In addition, all included teachers were also continuously supervised during the entire study period by a highly experienced (level 3) certified international teacher trainer in MBSR currently active at the Center for Mindfulness Sweden.
TAU (continued regular services)
The interventions provided by regular services at baseline are described for both groups in Supplementary Table S1. There were no between-group differences at baseline regarding pharmacological or other services in the two groups.
During the trial time period (T1 to T3), the TAU group continued their usual services, for example, psychiatric services and pharmacotherapy, interventions from physiotherapist or occupational therapist, or counseling/support sessions provided by social workers or psychologists. The following term, the participants in the TAU group were offered the chance to take part in an MBSR group.
Statistical analyses
The IBM SPSS version 28 was used for statistical analyses and the alpha level was set at p = 0.05. The clinical and sociodemographic characteristics were described at baseline and the two groups (MBSR vs. TAU) compared using the chi-squared test for categorical and t-test for continuous variables.
The outcome data were approximately normally distributed and there were no extreme outliers (defined as outside the first or third quartile ±1.5). The outcome variables were analyzed using an intention to treat approach, including all allocated individuals, at all time points, in all analyses. Linear mixed models (LMMs) were applied to compare the slopes of the MBSR and TAU groups from preintervention to follow-up. The LMM was chosen to reduce the risk of type I errors, as well as to provide robust estimates in the presence of missing data or heteroscedasticity of residuals.44,45 The LMMs included a random intercept and variance components’ covariance structure. In addition, models with a random time (slope, in addition to random intercept) were tested. Since restricted maximum likelihood test (Akaike’s information criterion) indicated better fit without a random effect of time (slope), we report the models with random intercept only. Between-group effect sizes, presented as Cohen’s d, were calculated based on the (raw) pooled standard deviations and the mean values from the predicted LMM at postintervention (T2) and at the 3-month follow-up (T3). 46 Within-group effect sizes were calculated from T1 to T2, and presented as Cohen’s d.
Qualitative analysis
The semistructured exit group discussions were audiotaped, transcribed verbatim, and analyzed qualitatively using the Open Code program provided by Umeå University in Sweden (Open Code 4.03 (umu.se)). An inductive thematic analysis was conducted in several systematic steps. 47 First, one author (H.A.) read the transcribed material while also listening to the audiotaped discussion whenever there were uncertainties in the transcription. Then, the same author made summaries of segments of the text into condensed sentences, as a first step to generate the initial codes (level 1) and then gathered these into initial categories (level 2), which were further assembled into initial themes (level 3). The process of generating the initial codes, categories, and themes implied several checks and rereads of the original transcribed data. Thereafter, a senior researcher (T.H.) read the entire data material, reviewed the analysis, and suggested some changes to codes, categories, and themes. These suggestions were discussed and changes to the initial codes, categories, and themes were made until consensus was reached (H.A. and T.H.). H.A. generated the first version of a table presenting the results. To cross-check the trustworthiness of the thematic analysis, the results were triangulated to two experienced MBSR teachers (G.W. and C.E.), who received the results table, which was then discussed in a digital (videoconference) workshop. Moreover, the defining and naming of the themes were conducted at the workshop after a consensus discussion (H.A., T.H., G.W, and C.E.). Finally, the table presenting the results was refined after the workshop (H.A.). At this stage, the level 1 codes in the table were replaced by a selection of the condensed sentences to improve the readability and transparency of the analysis, and to ensure that the voices of the participants were made heard in the final report. Thus, the qualitative results table depicts level 3 (themes), level 2 (categories), and excerpts from participants’ comments, while excluding level 1 (codes).
Results
Participants, attrition, and treatment completion
There were no significant differences between the two groups (MBSR vs. TAU) at baseline regarding sociodemographic or clinical variables. The participants (52% female) were an average of 40 years. Despite a similar education level to the general population of Sweden, 65% of the study participants were not studying or working at study inclusion, and 87% had at least one additional psychiatric diagnosis (details depicted in Table 1).
Sociodemographic and Clinical Characteristics Among the Study Participants
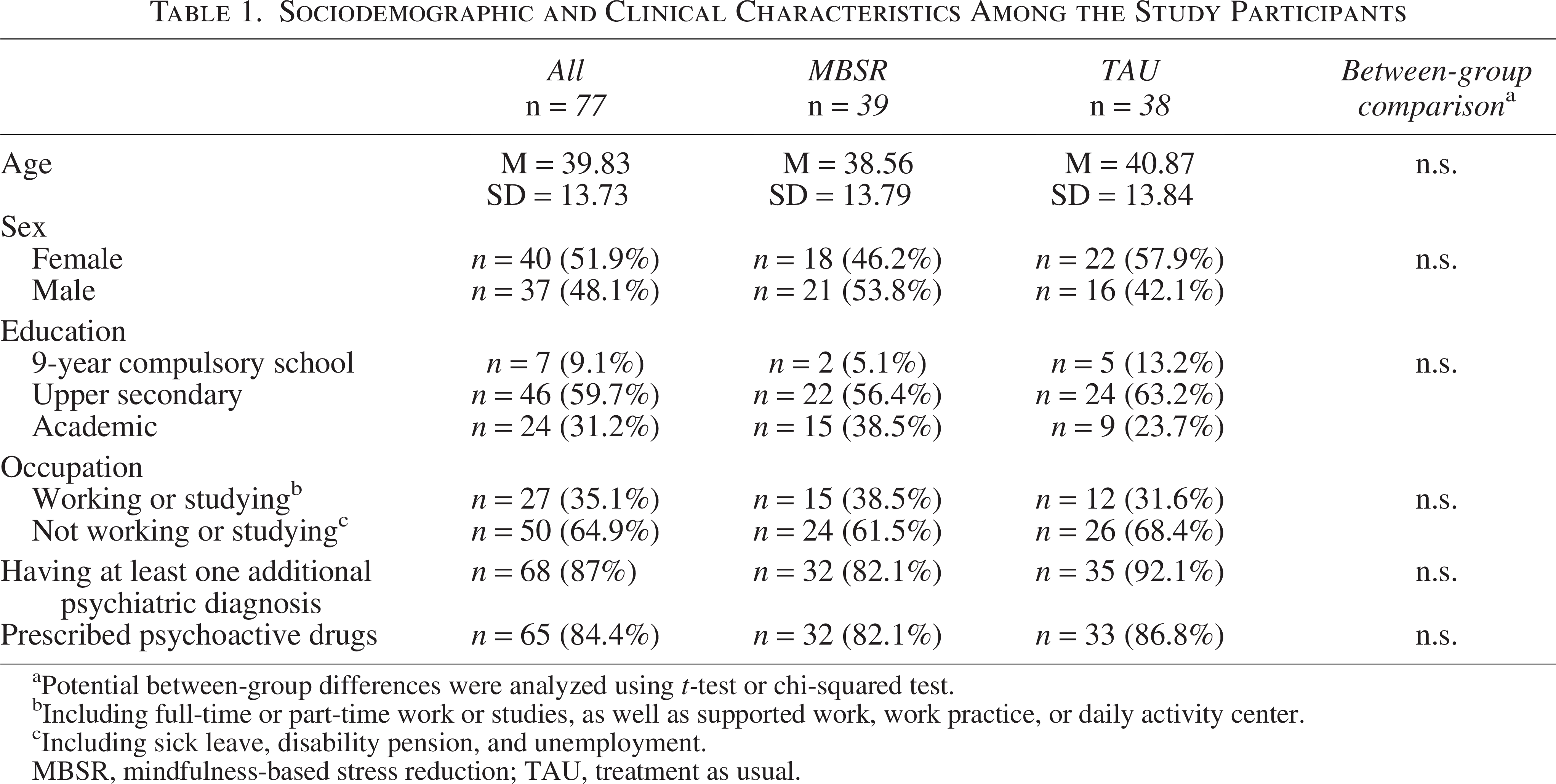
Potential between-group differences were analyzed using t-test or chi-squared test.
Including full-time or part-time work or studies, as well as supported work, work practice, or daily activity center.
Including sick leave, disability pension, and unemployment.
MBSR, mindfulness-based stress reduction; TAU, treatment as usual.
Of the 32 participants who started the MBSR treatment, 26 participants completed at least five of the ordinary eight group sessions, yielding a completion rate of 81% (Fig. 1. flowchart). Four participants missed at least four sessions due to illness, work obligations, travel, or similar reasons, and were categorized as noncompleters in the analysis. Additional two participants dropped out in the beginning of the program after one or two sessions; one because of work obligations while the reasons for the other one were not known.
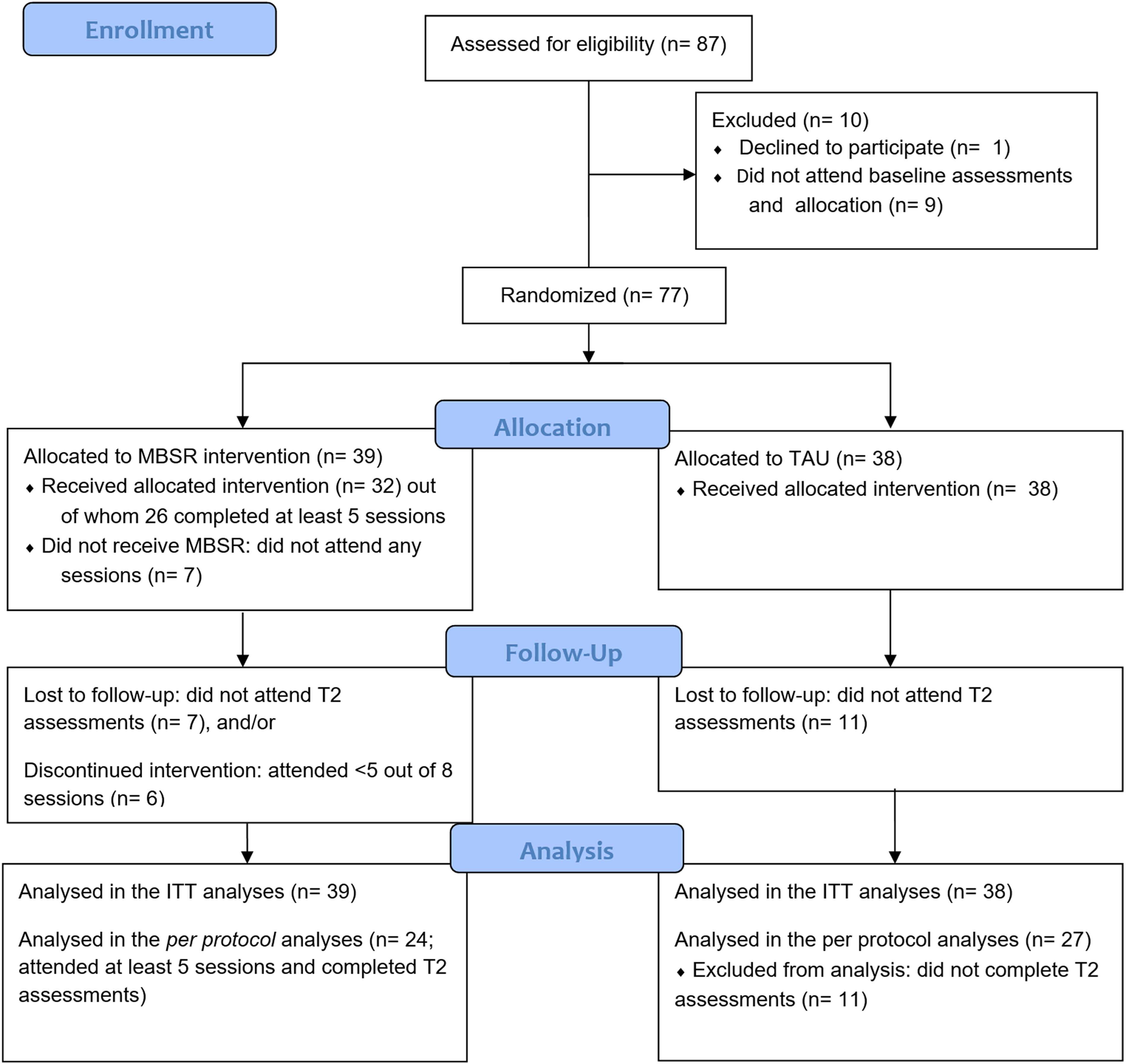
CONSORT flow diagram of the study participants.
Primary outcome
The details from the mixed linear models are depicted in Table 2. For the PSS, an interaction effect indicated group differences over time in the slopes of the two groups (MBSR vs. TAU). More specifically, the MBSR group reported greater reduction in PSS total (d = 0.55 [0.20–0.90], p = 0.003 at postintervention, and d = 0.61 [0.13–1.10], p = 0.013 at the 3-month follow-up), PSS coping difficulties (d = 0.50 [0.08–0.93], p = 0.02 at postintervention, and d = 0.90 [0.32–1.49], p = 0.003 at the 3-month follow-up), and in PSS distress (d = 0.53 [0.15–0.91], p = 0.007, n.s. at the 3-month follow-up).
The Between-Group Difference at Postintervention as Expressed by the Group a Time Parameter Estimates
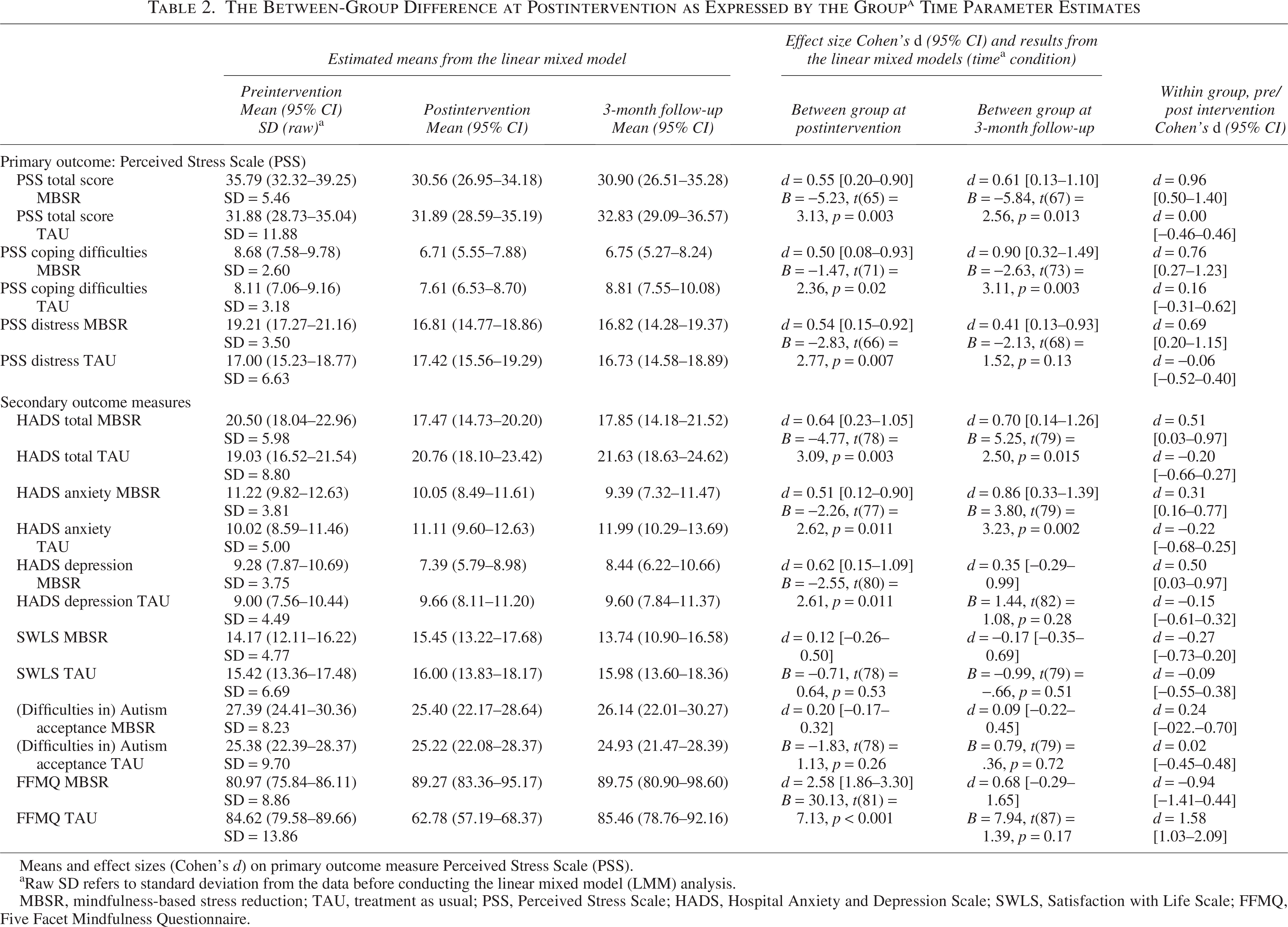
Means and effect sizes (Cohen’s d) on primary outcome measure Perceived Stress Scale (PSS).
Raw SD refers to standard deviation from the data before conducting the linear mixed model (LMM) analysis.
MBSR, mindfulness-based stress reduction; TAU, treatment as usual; PSS, Perceived Stress Scale; HADS, Hospital Anxiety and Depression Scale; SWLS, Satisfaction with Life Scale; FFMQ, Five Facet Mindfulness Questionnaire.
Secondary outcomes
Interaction effects indicated a greater reduction in mental health problems in the MBSR group than in the TAU group, as reflected by the HADS total score (d = 0.64 [0.23–1.05], p = 0.003 at postintervention, and d = 0.70 [0.14–1.26], p = 0.015 at the 3-month follow-up), HADS Anxiety subscale (d = 0.51 [0.12–0.90], p = 0.011 at postintervention, and d = 0.86 [0.33–1.39], p = 0.002 at the 3-month follow-up), as well as HADS depression subscale (d = 0.62 [0.15–1.09], p = 0.011 at postintervention, but n.s. at the 3-month follow-up). There were no between-group differences in change of quality of life or autism acceptance. Finally, the participants’ perception of their mindfulness skills showed larger improvements in the MBSR group at postintervention (d = 2.58 [1.86–3.30], p < 0.001). However, this difference did not remain at the 3-month follow-up.
Secondary additional outcomes: Adverse events and participants’ lived experiences
Adverse events
In total, eight adverse events were reported. Two adverse events were related to a somatic disease, two were related to other ongoing interventions, two to stressful life events, and two to study participation. Of the two who reported stress related to study participation, one participant described experiences of anxiety when completing the questionnaires at baseline and one after an MBSR intervention session. Both participants could continue after a short break and individual support provided by an MBSR teacher.
Qualitative data—thematic content analysis
The thematic content analysis of the exit group discussions in the MBSR groups resulted in three major themes, as described below. The themes, underlying categories, and a selection of excerpts from the participants’ comments are depicted in Table 3.
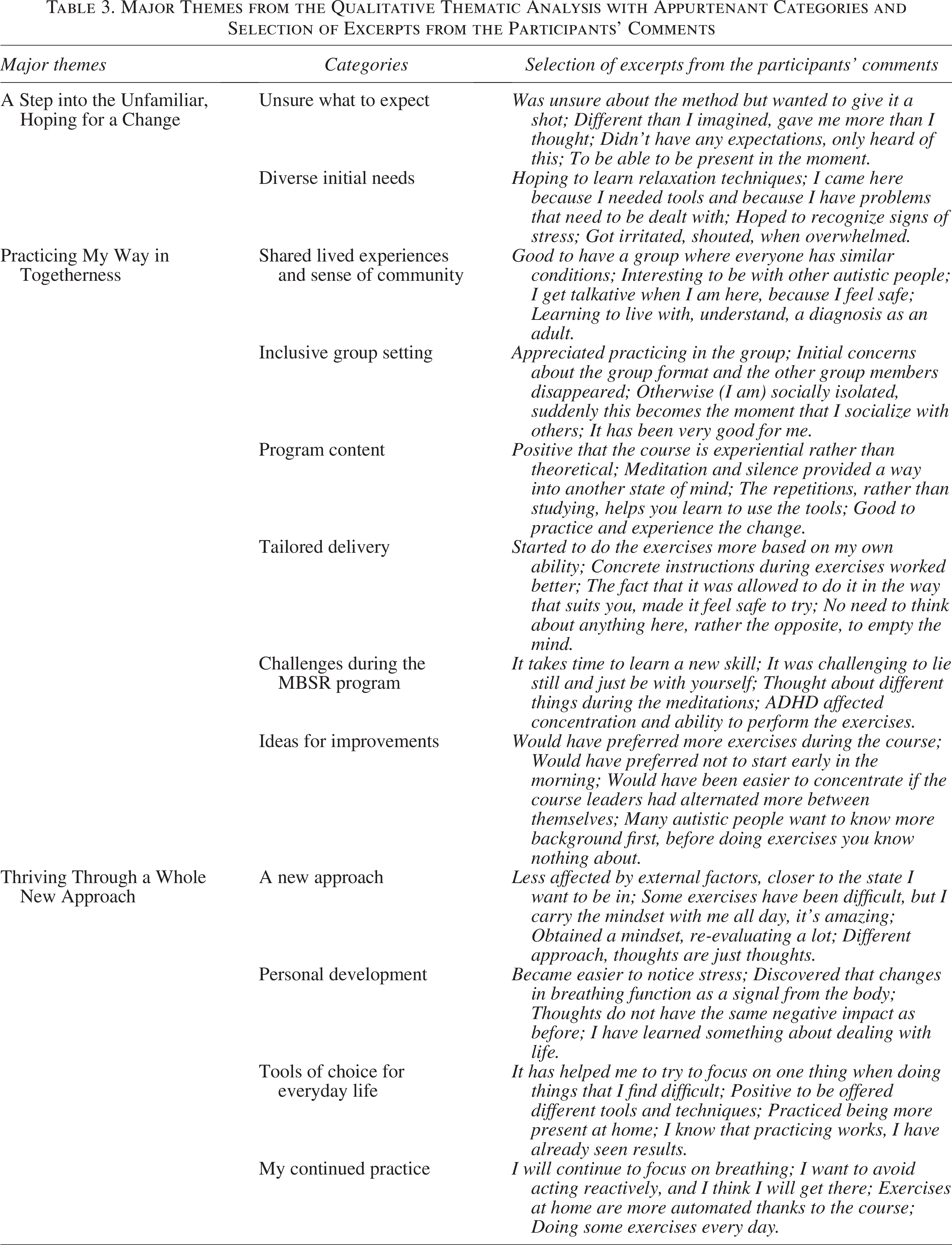
The first theme, A Step into the Unfamiliar, Hoping for a Change, describes the participants’ initial thoughts about the MBSR intervention. Many of the participants were referred to the program by a clinician based on their needs profile (e.g., overwhelmed by daily stressors, difficulties with emotion regulation), while they themselves did not always have clear expectations regarding the intervention’s contents. This is reasonable since the MBSR program is based on experiential learning and as such it is not possible to be learned by didactics (such as lectures) but through lived experiences of focusing attention to the present-moment in a nonreactive manner.
The group setting including only autistic people was highly appreciated by the participants, as summarized in the second theme Practicing My Way in Togetherness. The group was perceived as supporting and as a safe setting for learning and exercising new skills. The possibility of choosing between several provided mindfulness and yoga exercises, based on their own needs (individualization of the program) was important for the participants.
In the third theme, Thriving Through a Whole New Approach, the participants described changes in their approach to stress, how they gained new perspectives and insights. A new mindset facilitated a nonjudgmental perspective to own thoughts (thoughts are just thoughts) and other internal experiences, thus enabling regulation of own reactions. In several of the themes, the participants stressed some challenges related to the exercises and to the continued training after completing the MBSR program (Table 3).
Discussion
The current study is the first RCT to evaluate the effectiveness of the MBSR in autistic adults regarding subjective stress (including both distress and coping difficulties) in a clinical setting. Compared with the TAU group, the MBSR participants reported a larger postintervention reduction in perceived stress, less coping difficulties, and improved use of mindfulness skills as well as improved mental well-being. However, the overall quality of life and autism acceptance remained unchanged in both groups. The program completion rate in the MBSR group (81%) was on par with a previous open feasibility study in a clinical setting. 20 In the qualitative analysis, the participants stressed the benefits of concrete techniques for coping with stress, as well as having been able to change their “mindset” or “approach” to stressors and own stress reactions. However, it was also clear that the MBSR group training was not always easy and to maintain the acquired gains, continuous practice is needed.
The MBSR program is based on experiential learning (learning primarily by experience rather than through didactic materials) and stresses the importance of incorporating mindfulness in an everyday life situation. 16 In line with this, we observed postintervention medium-sized to large effects, on perceived stress coping skills and capability in applying mindfulness skills in everyday life. Previous feasibility and pilot studies have shown ambiguous results for MBSR-based six-session virtual (videoconference) groups,29,48 while adjusted MBSR groups (similar to the one applied in this study) have shown medium-sized reductions in perceived stress. 20 The clinical importance of addressing these outcomes was stressed in our study by the high level of perceived distress and coping difficulties at baseline: the participants reported higher perceived stress than observed in the general outpatient psychiatric population using the same questionnaire. 33 However, given our short follow-up time (3 months postintervention), further studies on long-term skills maintenance and further skills development after the MBSR participation would be an important topic for future studies. Future studies should preferably compare MBSR with an active control condition rather than with TAU, as was done in the present study. In addition, the use of blinded assessors both before and after the intervention—rather than only at baseline, as in the current study—would help minimize potential placebo effects. Using an active control design would also help ensure a comparable frequency of health care appointments across study groups during the intervention period. For instance, although participants in our study (MBSR vs. TAU) had similar access to health care services at baseline, we did not analyze their continued or discontinued use of services throughout the study period. Furthermore, we did not collect detailed information on the contents of TAU, such as specific medication regimens or the nature of counseling sessions.
In addition, it would be intriguing to examine if acquired MBSR skills can sustain and support autistic adults in coping with more burdensome life events, such as breaking up with a partner or losing a job, 49 besides managing everyday stress, which was the focus of the current study. Moreover, possible effects on other outcomes such as health habits (e.g., physical activity, sleep), emotion regulation, resilience, or self-compassion remain to be evaluated. Studies on long-term skills maintenance may be especially crucial given that the MBSR program is viewed as a first step towards optimizing their health: a direct experience of the influence one can have on one’s own health and well-being 16 and a continued practice is needed to maintain and develop the skills. Accordingly, the importance of continued practice was also stressed by the participants in the qualitative exit group discussions, also in line with results from other qualitative studies. 48 Since this study did not track the participants’ continued mindfulness practice after completing the intervention, this topic remains an important subject for future research.
We also hypothesized that direct experiences of possibilities to influence own health would reduce the experience of autism as a hindrance in life (i.e., increase autism acceptance) and improve general satisfaction with life. However, in current study, we did not observe any significant changes in autism acceptance or quality of life from pre- to postintervention. This conflicts with previous feasibility and pilot studies indicating positive preliminary effects on satisfaction with life, quality of life, and health-related quality of life21,22 following MBSR participation. Due to our short follow-up time of 3 months only, we could not determine whether these outcomes could be affected by continued mindfulness practice over time.
Interestingly, in the qualitive analyses, the participants not only stressed the importance of individualized, tangible yoga and mindfulness-based exercises and techniques, but also a new “mindset” or “approach” to stressors and to own thoughts and stress reactions. How this new mindset affects everyday life and how it is maintained postintervention could not be analyzed in this study but would be an interesting focus of future qualitative and long-term studies. Another crucial topic to address in future qualitative studies could be the impact of context for mindfulness practice. Both in our data and in previous studies on MBSR-based virtual (videoconference) groups,29,48 participants stressed the importance of the group format. An accepting and inclusive social environment as such seems to be an important facilitator for mindfulness practice for autistic adults who otherwise may experience social exclusion and have narrow social networks.
Mindfulness-based interventions have been suggested as a promising option for reducing and preventing mental health problems in autistic people. 17 In our study, consistent with previous research applying MBSR and related mind–body interventions,20,22–26 we observed significant effects from pre- to postintervention in both anxiety and depression symptoms in the MBSR group but not in the TAU group. However, although reduced in the MBSR group, the symptoms were still in the clinical range (indicating mild mental health problems at group level) at postintervention both regarding anxiety and the total scale level. 36 On the contrary, even small- to medium-sized symptom reduction may be important in a group with a heavy burden of mental health problems. Our participants were recruited in an outpatient context and a large majority (around 85%) had at least one psychiatric diagnosis and an ongoing psychoactive pharmacotherapy. Given the heterogenous nature of autism, including sociodemographic and clinical characteristics, it would be interesting to analyze predictors of treatment outcome and attrition based on these and other background variables in future studies with larger sample sizes. Nevertheless, we believe that acting early in the process (before the mental health difficulties reach clinical dignity) by providing autistic people tools for self-care and promoting active participation in their own health could be a more efficacious approach than what is common today: providing treatment when the mental health problems have reached a severe level, if at all.
Limited access to health care, including mental health services, is a frequent problem for autistic people.50–53 Health care professionals report a lack of competence and training to meet autistic people’s needs, leading to lack of, delays in, or interrupted services for autistic people, as well as dependency on family and friends as support and advocates. 50 Therefore, manualized interventions (such as the MBSR program) with structured group leader education to ensure treatment fidelity and quality may be a good option for health care organizations to improve access to services and to promote autistic people’s active participation in their health situations. MBSR teacher education to level 1 (i.e., qualification to teach the 8-week course) is done in three steps including both courses and retreats, associated with costs for the clinic. However, compared with, for example, a psychotherapist education, it is still a shorter and more affordable option. Moreover, the feasibility of the MBSR program has shown to be good in an outpatient context when adjusted for autistic adults’ needs, 20 and the good completion rate observed in the current study (81%) further corroborated these results. Still, a few individuals drop out of the MBSR early in the program due to discomfort with the group setting (e.g., getting irritated with other participants) or the intervention itself. Therefore, a thorough MBSR orientation before the intervention is important to minimize this kind of attrition. The attrition observed in this study corresponds to previous studies on mindfulness-based interventions 54 that typically apply a lower benchmark for completion (50%–55% of sessions) than used in this study (63% of the sessions). These results were obtained with the involvement of experienced clinicians who possessed both formal MBSR teacher training and substantial autism-specific expertise, including several years of professional experience in the field. Based on our experience, we consider both competencies—autism expertise and MBSR training—essential for effectively facilitating MBSR groups for autistic individuals. This dual requirement may pose challenges for implementation in clinical settings, where many clinicians may lack sufficient autism-specific competence.
This study specifically evaluated the MBSR, a standardized and well-structured mind–body intervention. The results from this study may not be generalizable to other types of mindfulness-based interventions or mindfulness-informed interventions such as the acceptance and commitment therapy or dialectical behavior therapy that may be helpful in similar or other ways. To consider a mindfulness-based intervention to be evidence-based, it is important that clear standards define the adoption (e.g., manualization, standardization of the material, and definition of facilitator competence) and claims on evidence should reflect the evidence base of that specific intervention. 55 Moreover, others have emphasized that “utilization of diverse type of mindfulness interventions may diminish the possibility of drawing general conclusions about the overall effectiveness of these interventions.” 27 On the contrary, using standardized program frameworks, such as MBSR, provides a possibility to compare results across various studies, including autistic individuals or other groups (ibid.).
Limitations
The rating scales used in this study have in most cases not been psychometrically evaluated for autistic people. However, the Cronbach’s alphas indicated good reliability in terms of internal consistency of all outcome measures. Another limitation was that the data collection was interrupted by the COVID-19 pandemic and the sample size therefore was somewhat smaller than planned. A further limitation is a probable underreporting of adverse events: we only registered spontaneously reported adverse events, while using a systematic interview or questionnaire would probably result in better coverage of possible adverse events. 56 In addition, the qualitative exit group discussion only captured the voices and lived experiences of the MBSR intervention completers, while neither autistic people who discontinued the MBSR prematurely nor those in the TAU group were interviewed.
Bearing these limitations in mind, the results of this study indicated that the MBSR can be an effective option to alleviate stress and improve stress coping and well-being in everyday life for autistic adults without intellectual disability met in an outpatient context.
Footnotes
Acknowledgments
The authors express their sincere gratitude to all the participants in this study, as well as to all the clinicians who contributed in different ways from referrals to interviews and treatment. They would also like to thank the research assistants for support in the CRF and data management, especially Maj April Frostvittra, as well as psychologist student Anna Björkman, who transcribed the exit group interviews. Finally, the authors wish to thank the management of Habilitation & Health, in particular, the managers of the Habilitation Center Mörby and Habilitation Center Stockholm who enabled the cooperation with the participating clinics.
Author Disclosure Statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: H.A., G.W., A.-K.L., C.E., and T.H. are employed by Habilitation & Health, Region Stockholm. T.H. receives royalties for treatment manuals from Hogrefe, and for text books from the publisher Studentlitteratur, although not related to this study. S.B. discloses no conflict of interest related to this study. S.B. discloses that he has in the last 3 years acted as an author, consultant, or lecturer for Medice and LinusBio. He receives royalties for textbooks and diagnostic tools from Hogrefe, UTB, Ernst Reinhardt, Kohlhammer, and Liber. S.B. is a partner in NeuroSupportSolutions International AB. N.J.-L. has no conflicts of interest to declare.
Funding Information
This study was funded by grants from the Region Stockholm funds for clinical research (ALF: FoUI-954901; FoUI-960703), as well as from the Promobilia foundation.
Authorship Confirmation Statement
T.H.: Conceptualization, methodology, formal analysis (quantitative data), validation (qualitative data), resources, data curation, writing—original draft, supervision, and funding acquisition. H.A.: Formal analysis (qualitative data), data curation, writing—review and editing, and funding acquisition. G.W.: Validation (qualitative data), investigation, and writing—review and editing. C.E.: Validation (qualitative data), investigation, and writing—review and editing. A.-K.L.: Conceptualization, investigation, project administration, and writing—review. N.J.-L.: Writing—review and editing. S.B.: Writing—review and editing. This article has been given solely to this journal and is not published, in press, or submitted elsewhere.
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.