
Abstract
Background:
Autistic people experience a higher rate of suicidal thoughts and behaviors (STBs) than the general population and the autism community has identified suicide prevention research, including risk factors, as a priority. One risk factor may be experiencing invalidation (i.e., dismissal or minimization of one’s thoughts, feelings, behaviors, or experiences). However, no studies have asked autistic people about the perceived impact of invalidation on their suicidality. As autistic people report widespread invalidation, including of their diagnosis and characteristics, the relationship between invalidation and STBs in this population deserves exploration.
Methods:
106 autistic adults (Mage = 38.8, SDage = 11.1) with a history of suicidality completed an online survey that asked if experiencing invalidation had contributed to STBs and, if yes, to describe the invalidation. Qualitative content analysis was used to summarize open-ended responses.
Results:
92% of respondents reported invalidation as a contributor to STBs. A range of sources were reported, most frequently parents or other family members (50%), health care providers (32%), and friends or peers (24%). The most common content was invalidation of mental health challenges (43%) and autistic traits (20%). For example, participants reported experiences of being told they were “mak[ing] things up for attention,” not believed or taken seriously, and having their sensory needs and communication differences dismissed. Some respondents reflected on historical invalidation (i.e., experienced years ago; 12%) and others shared that it was overwhelming to summarize due to the extent or frequency (11%).
Conclusion:
Most autistic adult respondents endorsed that invalidation contributed to STBs. The invalidation reported was pervasive, spanning many sources and relating to deeply personal experiences across the lifespan. These findings support the need for more research on this relationship in addition to a shift toward neuro-affirming conceptualizations of autism and mental health in community and health care settings to prevent invalidation.
Community Brief
Why is this an important issue?
Suicide prevention has been ranked as a top research priority by the autism community because autistic people are more likely to experience suicidal thoughts and behaviors (STBs) and to die by suicide. Invalidation, or having your feelings, thoughts, or experiences not believed or dismissed, is a common experience for autistic people. Some research with non-autistic people suggests that invalidation may contribute to STBs, but this has not been explored for autistic people.
What was the purpose of this study?
We wanted to learn whether autistic adults believe that experiences of invalidation contributed to STBs and, if so, more information about the invalidation.
What did the researchers do?
Our study co-lead author, an autistic woman, identified invalidation as critical to ask about in our anonymous online survey on autistic adults’ experiences with STBs. We asked 106 autistic adults if experiencing invalidation had contributed to STBs and, if yes, what was said and by whom. We used qualitative data analysis techniques to summarize responses.
What were the results and conclusions of the study?
Overall, 92% of participants responded that invalidation contributed to STBs. Participants described a range of sources and invalidation related to a variety of personal experiences. The sources mentioned most were parents or other family, health care providers, and friends or peers. Other sources included people in work, school, and community settings. The most common content was invalidation of mental health challenges and autistic traits. For example, not being believed when reporting distress, being accused of attention-seeking, having their sensory needs dismissed, and having their communication differences misunderstood. Some participants shared that responding was overwhelming because of the extent or frequency of invalidation, and some wrote about invalidation that occurred years ago.
What is new or controversial about these findings?
This is the first study that asks autistic adults whether experiences of invalidation contribute to STBs. These results tell us that invalidation is common, that it comes from multiple sources, and often relates to deeply personal experiences such as mental health challenges and autistic traits.
What are potential weaknesses in the study?
The way the questions were worded may have led participants to the answers our team was interested in. We also could not ask participants to clarify because it was anonymous. In addition, our participants do not represent the entire autism community because they had to access the internet and be able to write in English, and most were White, female, late-diagnosed, and highly educated. Since many participants found the study through the research team members’ social media, they may already have been engaged in research and advocacy.
How will these findings help autistic adults now or in the future?
We hope our findings integrate autism community knowledge into scientific evidence and affirm the invalidation experienced by autistic people as real and deeply impactful. Our results reinforce the idea that efforts to increase acceptance and understanding of autistic people must center their perspectives and lived experiences to decrease invalidation. These efforts are needed for both community members and professionals.
Background
Autistic people are a particularly high-risk group for suicidal thoughts and behaviors (STBs).1,2 While prevalence estimates vary, studies have found that they are up to nine times more likely to experience suicidal ideation (SI) and up to eight times more likely to die by suicide compared with the general population.1,3 For this reason, the autism community has identified suicide prevention research as a top priority, including risk factors, barriers to seeking help, and experiences of not being believed when reporting distress.4,5
As research has begun to center autistic perspectives, invalidation (i.e., dismissal or minimization of one’s thoughts, feelings, behaviors, or experiences) is increasingly highlighted as a salient experience of autistic people. A growing body of literature shows that autistic people experience invalidation of abusive relationships6,7; sensory experiences6,8; autism diagnosis, including the diagnostic process 9 ; and when seeking help for co-occurring mental health challenges, including suicidality.10,11 Notably, this empirical evidence of invalidation supports community perspectives that autistic people continue to not be believed when recounting their own lived experiences and are dismissed in a multitude of settings by family members, professionals, peers, and others.
In fact, community and academic perspectives have historically been misaligned, and invalidation has been inherent within persisting conceptualizations of autism. The academic and medical fields of autism have largely been shaped by the medical model of disability, a framework that positions autism as a pathology within an individual rather than a natural neurological difference with both strengths and challenges. 12 Furthermore, it ignores the ways that societal expectations and structures may interact with autistic traits to shape a person’s experiences and instead focuses solely on individual impairment. The impact of this deficit-based framing can be seen in the systemic invalidation of autism community knowledge and expertise and in the historical denial of autistic people’s epistemic authority, the ability to provide reliable information about autism and their own experiences. 13 This is evident in the way that medical professionals, rather than autistic people, are considered autism experts.12,14
Recent community discourse has also criticized Applied Behavior Analysis, a common autism intervention, particularly for young children, as being inherently invalidating due to its prioritization of societal conformity over the autonomy, comfort, and well-being of the autistic person. 15 This emphasis on conformity and eliminating behaviors that are different from neurotypical behaviors (e.g., stimming) has been criticized as leading to masking or camouflaging (i.e., the suppression of autistic traits). Masking behaviors have been shown to relate to invalidation and have long-term negative consequences for mental health.10,16–19 Unfortunately, it is unclear how invalidation contributes to STBs, even in non-autistic samples. Limited research has explored invalidation as it relates to mental health and suicidality, with varied findings that are not specific to autism. For example, research in adolescents has shown an association between parental invalidation and self-harm, including suicide attempts, and peer invalidation as predictive of self-mutilation.20,21 In another study, parental invalidation of gender identity was associated with more severe passive SI (i.e., weakened desire to live) for transgender and gender-diverse adolescents. 22 Despite the historical and continued experiences of invalidation in the autistic community and the higher risk for STBs, no studies, to our knowledge, have explored the self-reported impact of invalidation on suicidality in this population. Thus, in this study, we aimed to ask autistic people with a history of STBs whether experiences of invalidation were a contributor, and if so, what those experiences were.
Methods
This study was approved by the University of North Carolina at Chapel Hill Institutional Review Board (IRB #22-1216). To guide the presentation of our positionality, methods and analytical approach, and study results and interpretation, we used the 21-item Standards for Reporting Qualitative Research, which aims to facilitate complete and transparent qualitative research reporting. 23
Researcher positionality
The study team included (1) an autistic study co-lead and founder and co-lead of the Autism and Suicide Prevention Workgroup; (2) a neurodivergent study co-lead and assistant clinical research coordinator passionate about supporting research that authentically engages autistic people as full members of the research team; (3) an autistic assistant clinical research coordinator; (4) a research project manager; and (5) a researcher in the field of autism with over 15 years’ experience working, predominately, with autistic girls and women.
Participants
Participants were 106 autistic adults aged 18–67 (M = 38.8 years, SD = 11.1 years) who either reported having a formal diagnosis of autism (74%), self-identified as autistic (17%), were seeking a diagnosis (7%), or preferred not to provide information about their diagnostic status (3%). The sample was 53% female (including transgender women), 18% male (including transgender men), and 29% nonbinary or another gender identity. The sample was 78% White, 6% Asian, 15% multiracial or other, and 1% American Indian or Alaska Native. All participants had a history of suicidality, reporting they first experienced suicidal thoughts as young as 5 years of age (M = 14.7 years, SD = 7.8 years), and 56% had previously made at least one suicide attempt. See Table 1 for participant demographic information.
Participant Demographics (N = 106)
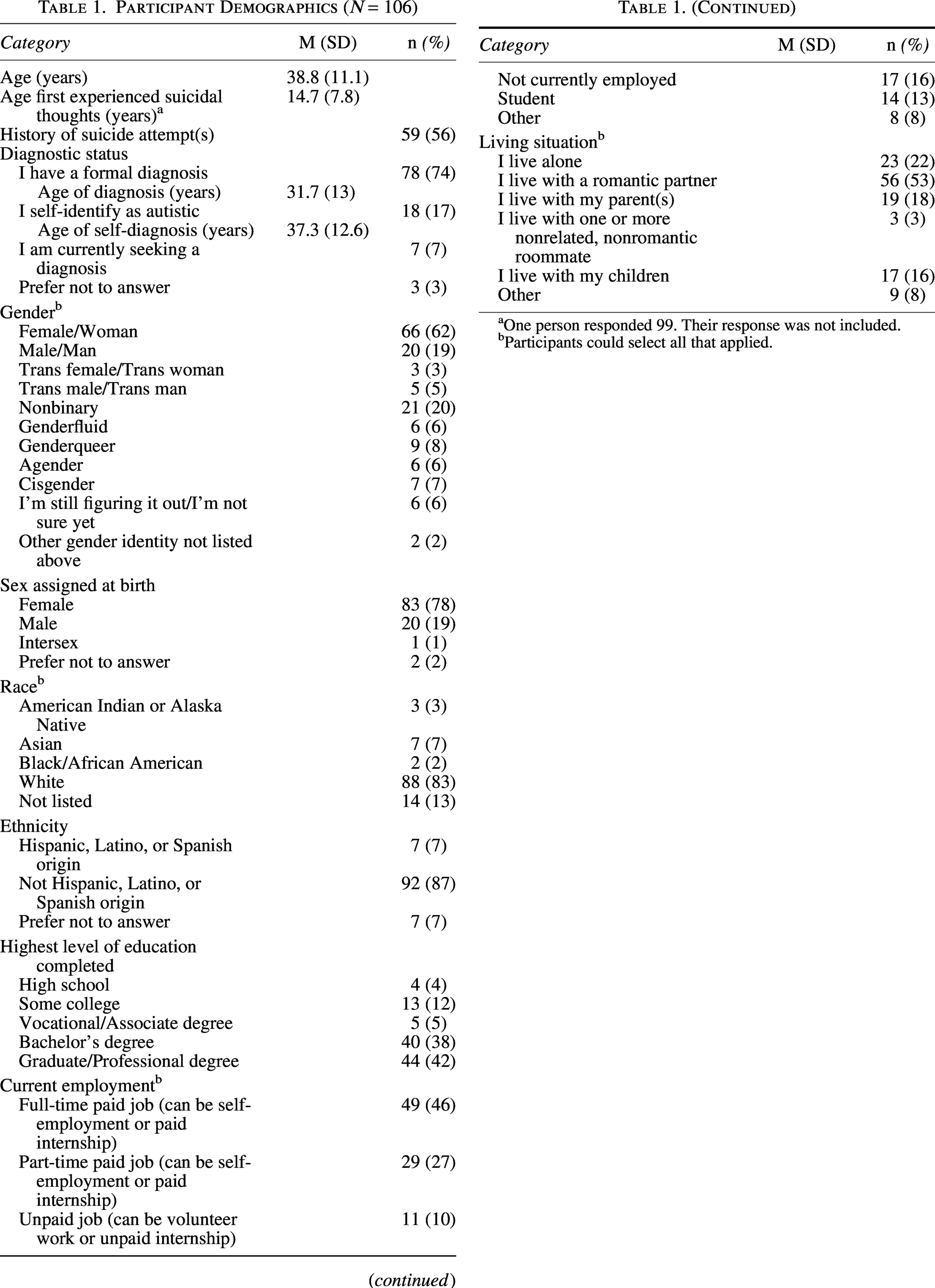
One person responded 99. Their response was not included.
Participants could select all that applied.
Procedures
The autistic co-lead of this study identified priority research questions based on her personal and professional expertise in autism community experiences of suicidality. Our team then finalized the survey (see Supplementary Table S1), which asked autistic adults about their experiences with STBs, including contributing factors and coping strategies, and demographic characteristics. A recruitment graphic and Qualtrics survey link were posted to one of the project leads’ LinkedIn and X accounts. Additional recruitment materials were distributed via email to other researchers in the field who had existing relationships with team members with a request to distribute to their channels. Survey responses were gathered between May 2024 and January 2025.
Interested people had to confirm they were at least 18, identified as autistic or on the autism spectrum, had experienced STBs, could write in English, understood they would not be compensated, did not have any unanswered questions, and provide consent. Our team felt strongly about including self-identified people (i.e., without formal autism diagnosis) given the known barriers to diagnosis, especially for those from other marginalized communities, and the unique experiences of invalidation faced by this group. 9 The survey was expected to take about 25 minutes to complete. The present study focuses on a subset of survey questions about autistic adults’ self-reported experience of invalidation as a contributor to their STBs. Respondents were asked, “Has experiencing invalidation (i.e., having your thoughts, feelings, behaviors, or experiences dismissed or minimized) contributed to suicidal thoughts and/or behaviors for you?” If they responded yes, they were asked to “Please describe what was said and the source(s) of invalidation (e.g., health care provider, parent, peer, teacher).”
The team relied on survey security measures in Qualtrics, in addition to validation questions, to detect duplicate or inconsistent responses and used a consensus-based, case-by-case approach for evaluating each flagged response. The lack of compensation likely prevented bot and “scammer participants” who have threatened data integrity for other qualitative autism research conducted online. 24
Qualitative research paradigm and analysis
Our research team’s views and approach to analysis were guided by the interpretivist paradigm of qualitative research, such that we honor each person’s subjective experiences as a unique reality. We feel that this is particularly important when considering feelings of invalidation, as harm can occur regardless of intention. The present study used a combination of directed and conventional qualitative content analysis to analyze participants’ open-ended responses. 25 Two coding team members independently familiarized themselves with participants’ responses. A preliminary coding scheme was developed from the personal and professional expertise of members of the research team (i.e., directed qualitative content analysis). Both coders then independently applied code labels to participant responses. Conventional qualitative content analysis was used to identify inductive codes that the original coding scheme had not captured but were relevant to the research questions. Following a second round of coding, discrepancies were discussed, and consensus was established among all team members. Throughout the analysis, we actively engaged in reflexivity, striving to understand how our own perspectives and experiences influenced our interpretations, and team members were empowered to offer alternative interpretations of the data. Investigator triangulation facilitated a more complete, nuanced perspective of the results.
Results
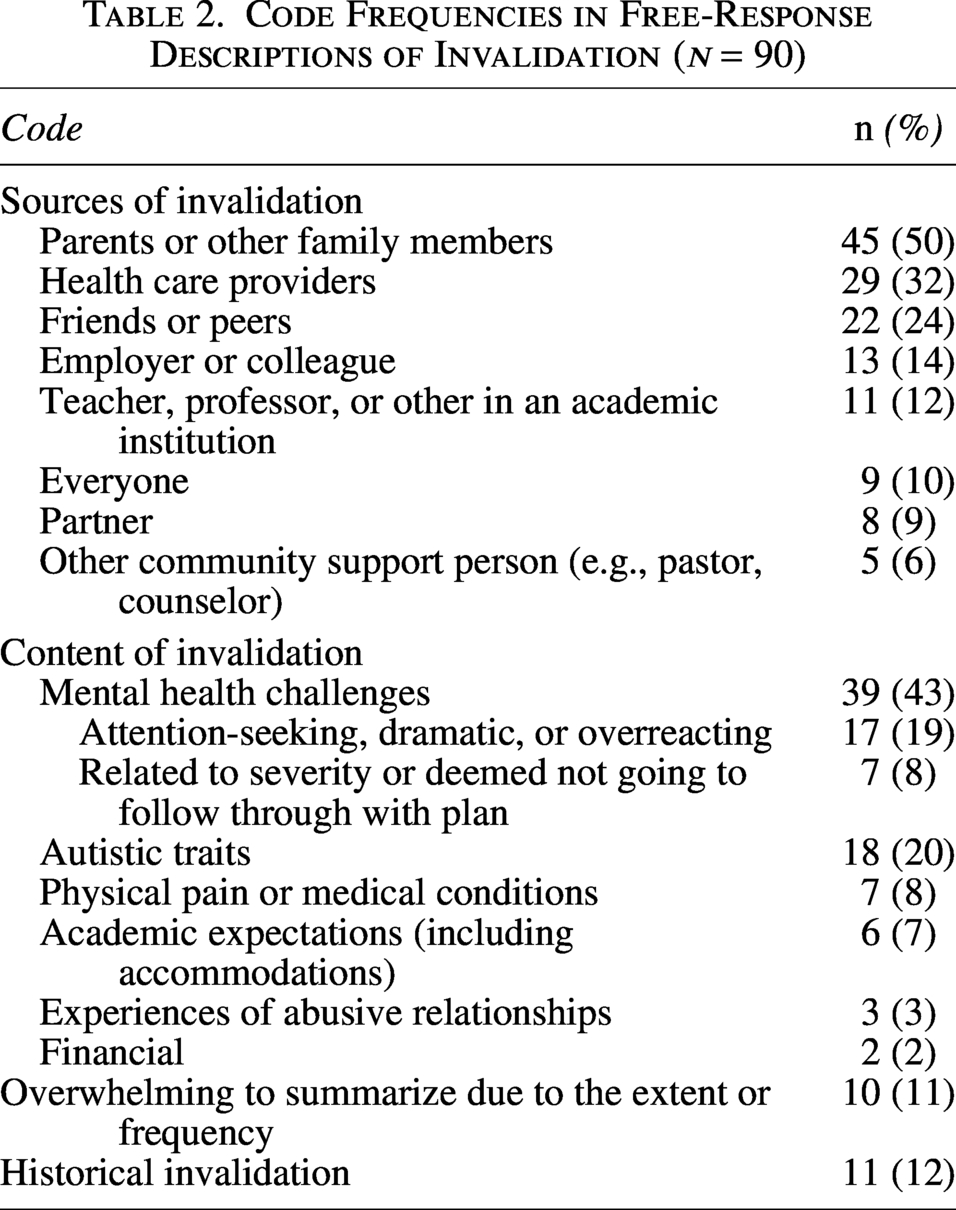
About 92% (n = 97) of respondents reported invalidation as a contributor to their STBs. Of those 97 respondents, 90 provided free-response descriptions of the invalidation. Table 2 details the occurrence of codes in the descriptions. Additional examples of responses are presented by code label in Supplementary Table S2.
Code Frequencies in Free-Response Descriptions of Invalidation (n = 90)
Sources of invalidation
Participants’ responses revealed a range of sources of invalidation; most frequently mentioned were parents or other family members (50%), health care providers (32%), and friends or peers (24%). Other sources included an employer or colleague (14%); teacher, professor, or other in an academic institution (12%); partner (9%); or other community support person (e.g., pastor, holistic counselor, occupational vocational rehabilitation coach; 6%). Many participants reported that the invalidation came from multiple sources, with some expressing that it felt like it came from “basically everyone in [their] life” (10%).
Content of invalidation
Several categories emerged in the content of invalidation reported. The most common was invalidation of mental health challenges (41%). One participant paraphrased: “Have you considered spending more time in the sun and getting more vitamin D? It should be able to decrease your depression.” The subcategory of being perceived as attention-seeking, dramatic, or overreacting (19%) was common in responses. A participant wrote, “One teacher told me I did not cut deeply enough to ‘do any real harm’ (aged 14) and implied it was attention-seeking behaviour.” Another subcategory, related to severity or deemed not going to follow through with plan (8%), revealed that participants did not feel their experiences were taken seriously. One participant shared that they were told that “their attempts weren’t real attempts (just being impulsive and [they] didn’t really want to die).” Another participant paraphrased a health care provider telling them, “You’re not actually going to do anything” and added that “… ironically, being told that was NOT comforting; it felt like a challenge.”
The second most common category was invalidation of autistic traits (20%), revealing a lack of a nuanced understanding of autism; for example, someone saying, “You don’t look Autistic” to them. Some participants shared that others “dismissing [their] sensory needs” was invalidating, with one participant recalling the following experience with a psychiatrist: “He also was saying that I can always control my body even though multiple times I explained during a sensory overload meltdown I have no control of my body and can bang my head for an hour. The whole thing really upset me and then I got really angry and disregulated [sic] that lead to hours of crying and then some suicidal thoughts.” Other participants shared experiences that highlighted others’ “lack of understanding of communication differences”: “Invalidation happens often because it’s hard for me to express thoughts and ideas clearly, especially in conversation.”
Other categories of invalidation included physical pain or medical conditions (8%), academic expectations (7%) (sometimes related to accommodations), experiences of abusive relationships (3%), and financial (2%) invalidation.
Some participants shared that it was overwhelming to summarize due to the extent or frequency (11%) of invalidation experienced, with participants noting things like, “It’s difficult to summarise [sic] decades of history,” “I don’t even know where to begin!” and “There is not enough space here to list 36 years of invalidation from almost everywhere and everyone.”
Finally, 11 respondents (12%) reflected on what we were able to infer was historical invalidation (i.e., experienced many years ago). For example, one participant, age 37, paraphrased a statement made by her pediatrician: “I don’t like to prescribe antidepressants to children but if it’s very important to you I guess I will consider it.” Another, age 57, responded, “There are thousands of instances from my earliest memories. I was diagnosed last year and people still insist I’m not autistic.”
Discussion
The goal of this study was to examine the sources and content of invalidation reported by autistic adults as contributing to STBs. We found that the majority of autistic adult respondents reported that invalidation contributed to their STBs. The invalidation experienced was seemingly ubiquitous, spanning many sources, relating to a breadth of deeply personal experiences, and leaving long-lasting impressions. Though this study is the first to our knowledge to directly ask autistic people about experiences of invalidation as a contributor to suicidality, our findings of widespread invalidation are supported by prior literature.6–11 Taken together, it is likely that these are not one-off moments of interpersonal misunderstanding but instead reflective of systemic breakdowns in non-autistic peoples’ perceptions of autistic experiences. These findings support a pivot away from traditional conceptualizations of autism, which may promote these communication breakdowns and focus on a person’s challenges or differences (e.g., the medical model), and toward neurodiversity-affirming models, which prioritize autistic people as experts in their own lived experiences. In addition, our participants reported that invalidation came from their personal communities in addition to health care and mental health professionals, illuminating the need for comprehensive, community-wide education informed by lived experience to increase awareness and acceptance of autistic people.
This study, while the first, to our knowledge, to address the experience of invalidation and its reported contribution to STBs in autistic adults, also has several limitations. First and foremost, given that it was a cross-sectional survey, we cannot infer causality. Furthermore, the wording of our survey questions could have led participants to provide answers related to invalidation when they may not have previously considered invalidation as contributing to STBs. Third, we used convenience sampling to recruit our participants; thus, the majority were already engaged with related work or following social media pages that share information about autism and suicide. In addition, as our sample had to have internet access and the ability to write in English and was largely White, female, late-diagnosed, and highly educated, our findings may not generalize to the broader autistic community. Finally, as the study was conducted as an online survey rather than synchronous interviews, we were unable to ask follow-up questions about participants’ responses. To this end, future work should seek to examine the effects of invalidation on suicidality with a more diverse population of autistic people and to utilize multiple research modalities that allow for increased nuance. For example, it is important to distinguish perceived contribution based on the type of suicidality (i.e., SI vs. suicidal behavior and attempts) and, in measuring the association, identify any differential effects based on the source, context, or experiences and identities implicated (e.g., mental health, autistic identity, other cultural identities).
Though this study is relatively novel within the scientific community, the findings may not be ground-breaking to the broader autism community. Instead, we hope that our work bridges the gap between autism community knowledge and experience and the academic autism field. Our work is grounded in the expertise of our autistic co-lead and neurodivergent research team members, without whom this study may never have been conceptualized or conducted, and illustrates the importance of prioritizing autistic perspectives. Ultimately, autistic people need to be accepted for who they are, believed when sharing lived experience, and sincerely understood by the people supporting them.
Authorship Confirmation Statement
L.M. contributed to conceptualization and article preparation. J.H. contributed to conceptualization, formal analysis, and article preparation. E.V. contributed to formal analysis and article preparation. S.B. contributed to supervision and article review. C.H. contributed to supervision and article review. The article has been submitted solely to Autism in Adulthood.
Footnotes
Acknowledgments
The authors would like to thank the autistic participants who made this work possible. They are grateful for their willingness to share their experiences with STBs.
Author Disclosure Statement
L.M. receives fees for speaking engagements and workshops on this topic. The authors report no other potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
No funding was received for this article.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.