
Abstract
Background:
Autistic adolescents and young adults experience high rates of co-occurring physical health challenges, particularly sleep disturbances and gastrointestinal (GI) symptoms, which likely reflect underlying structural barriers to timely and appropriate healthcare. In countries with urban and remote service gaps, such as Saudi Arabia, these inequities are more visible in the post-pandemic context. Neurodiversity-affirming approaches emphasize modifiable systems, accessibility, and supportive environments that can promote more equitable healthcare experiences; however, evidence applying this lens to physical health inequities in the Arab region remains limited.
Methods:
We conducted a cross-sectional survey of 198 primary caregivers of autistic adolescents and young adults (aged 13–25 years) living in urban (61%) and remote (39%) regions of Saudi Arabia. Caregivers completed measures of sleep disturbance (using age-specific instruments), GI symptom severity, healthcare access barriers, autism traits, neurodiversity-affirming practices, and digital health utilization. Analyses included group comparisons, hierarchical and multivariate regression, and mediation and moderation models using PROCESS.
Results:
Remote residence was associated with greater sleep disturbance and higher GI symptom severity compared with urban residence. Caregivers in remote regions reported substantially higher healthcare access barriers and lower neurodiversity-affirming practices, while telehealth utilization did not significantly differ by geographic region. Healthcare access barriers significantly mediated the association between geographic region and sleep outcomes. Neurodiversity-affirming practices were independently associated with better physical health and attenuated the negative impact of access barriers on sleep outcomes.
Conclusions:
Physical health inequities among autistic adolescents and young adults in Saudi Arabia were more strongly associated with modifiable structural barriers, including healthcare access barriers and regional inequities in service availability. Strengthening neurodiversity-affirming practices and embedding affirming principles across in-person and digital services may support more equitable and context-sensitive care.
Community Brief
Why is this issue important?
Many autistic people experience health problems, especially difficulties with sleep and stomach or digestion problems. In Saudi Arabia, many autism-related services are mainly available in major cities. This can make it harder for autistic young people living far from cities to get the healthcare and support they need. This study looked at how location may affect health and used an approach that respects autistic ways of thinking, communicating, and experiencing the world.
What was the purpose of this study?
This study had three main goals. First, we compared sleep and digestion-related health problems among autistic young people living in major cities and those living farther from cities. Second, we examined the difficulties families face when trying to access healthcare services. Third, we explored whether supportive and respectful practices at home may help improve health and well-being.
What did the researchers do?
We recruited 198 families from across Saudi Arabia, including 120 families living in major cities and 78 living in areas farther from cities. Caregivers, most of whom were mothers, answered questions about health, access to healthcare, and the daily support practices they used with their autistic family member.
What are the results and conclusions of the study?
We found three main results. First, autistic young people living farther from cities experienced more sleep and digestion problems than those living in major cities. Second, these differences were strongly linked to difficulties in getting healthcare. Families living farther from cities often had to travel longer distances, pay higher costs, and had fewer opportunities to access autism specialists. Third, supportive and respectful practices at home were linked to better health and appeared to reduce some of the negative effects of these challenges, especially for sleep.
What is new or controversial about these findings?
The study suggests that poorer health outcomes in areas farther from cities were more strongly associated with healthcare access barriers and regional inequities in service availability. The findings also suggest that telehealth alone may not fully address disparities if services are not designed in ways that are accessible, respectful, and responsive to autistic needs.
What are the potential weaknesses of the study?
We collected information from caregivers at one point in time only. The study did not directly include autistic individuals’ own views in the main analyses, which remains an important goal for future research. In addition, many participating families were already connected to healthcare or support services, so the findings may not fully reflect the experiences of more isolated families.
How will these results help autistic people now or in the future?
These findings show how healthcare systems can provide fairer and more supportive care for autistic people across different regions. Policymakers can improve services in areas farther from cities and provide better training for healthcare professionals. Healthcare planners can also work together with autistic people and families to improve telehealth services. Families may also benefit from supportive practices at home when access to services is limited. Overall, improving health requires reducing barriers and providing respectful and supportive care across all regions.
Keywords
Background
Autism is a neurodevelopmental condition commonly characterized in diagnostic frameworks by differences in social communication and interaction, alongside restricted or repetitive patterns of behavior. 1 However, autism is also increasingly understood as a form of neurodivergence shaped by relational, environmental, and sociocultural factors.2,3 This perspective aligns with relational accounts of autism, including the Double Empathy Problem, 4 which emphasizes that communication differences between autistic and non-autistic individuals are mutual rather than one-sided deficits.
Beyond these core characteristics, autistic individuals experience a substantially higher prevalence of co-occurring physical health conditions compared with non-autistic populations. Commonly reported conditions include sleep disturbances, gastrointestinal disorders, immune-related conditions, and musculoskeletal differences.5,6 We selected sleep disturbances and gastrointestinal symptoms as the primary outcomes in the present study because they are among the most prevalent and clinically significant health concerns reported in autism.5,6 These outcomes are closely linked to healthcare access, continuity of care, and overall quality of life. 7
A growing body of evidence indicates that while some co-occurring health conditions may have biological underpinnings more common among autistic individuals, the extent to which these conditions become disabling or remain unaddressed is substantially influenced by systemic and structural barriers within healthcare systems.8,9 Consequently, autistic adolescents and adults face elevated risks of multimorbidity, delayed diagnosis, and unmet physical health needs, contributing to persistent and largely preventable health inequities.7,10 Thus, health disparities among autistic individuals likely reflect interactions between biological and modifiable system-level factors. 11
The neurodiversity movement provides a critical framework for reexamining autism and related health disparities. It conceptualizes autism as a natural form of human variation rather than a disorder to be normalized, and emphasizes the role of social, environmental, and systemic factors in shaping outcomes.2,3 Within this framework, neurodiversity-affirming healthcare emphasizes respect for autistic identity, accommodation of sensory and communication differences, shared decision-making, and the promotion of autonomy and quality of life, without seeking to suppress or normalize autistic traits.12–14 The emergence of profession-specific guides highlights the translational potential of these principles across service sectors. In healthcare specifically, practical adaptations include sensory-friendly clinical environments, flexible communication approaches, shared decision-making processes, and caregiver–provider collaboration that respects autistic preferences and autonomy. The adoption of such neurodiversity-affirming practices is critical not only for communication and sensory accommodation but also for addressing systemic barriers linked to sleep disturbance, gastrointestinal symptom severity, and broader physical health inequities.
Sensory sensitivities, including auditory or tactile hypersensitivity, are closely linked to physical health experiences among autistic individuals and may contribute to differences in sleep quality (e.g., through sensory overload at bedtime) 15 and gastrointestinal comfort (e.g., through stress responses to unfamiliar environments). Within a neurodiversity-affirming framework, accommodating these sensory differences in healthcare settings is essential for promoting comfort, trust, and accurate assessment of physical health needs. 16 When such accommodations are lacking, autistic individuals may avoid or delay seeking care, potentially compounding existing geographic barriers to healthcare access. 16
Geographic location constitutes a major structural determinant of health and plays a central role in shaping access to neurodiversity-affirming care. Urban and remote disparities in healthcare access are well documented internationally, with families in rural and remote regions facing shortages of specialized providers, long travel distances, fragmented care pathways, and limited continuity of services.17,18 These challenges are especially consequential for autistic individuals, whose healthcare needs often require coordinated, specialized, and sensory-informed approaches.
In the Kingdom of Saudi Arabia, geographic inequities in healthcare access are particularly salient due to the country’s vast land area and uneven distribution of specialized services. Existing research indicates that families residing in remote regions frequently encounter delayed autism diagnoses, limited access to multidisciplinary care, and a heavy reliance on major urban centers for specialized services.19,20
However, access alone does not guarantee the quality of care. Increased geographic access to healthcare services does not necessarily equate to neurodiversity-affirming care. Services may be physically available yet fail to meet the needs of autistic individuals if providers lack appropriate training or do not accommodate sensory and communication differences. Recent consensus-based work integrating psychologist and autistic client perspectives has further clarified the defining features of neurodiversity-affirming psychological practice. 21 These include respect for autistic identity, autonomy, sensory needs, and collaborative decision-making.
Recent work has also highlighted the relevance of the neurodiversity framework within medicine, calling for its broader integration into clinical practice rather than its traditional confinement to psychological or educational domains. 22 Emerging evidence highlights distinct and often unmet health needs among neurodivergent emerging adults, indicating challenges during the transition to adult-oriented healthcare services. 23
Furthermore, emerging evidence indicates that geographic barriers are associated not only with reduced service utilization but also with poorer physical health outcomes and diminished quality of life among autistic adults, with healthcare access barriers identified as a key predictor of reduced physical health-related quality of life. 7
Although recent national initiatives and clinical guidelines have sought to strengthen services for autistic individuals and improve care coordination across regions,24,25 the extent to which these efforts translate into equitable, neurodiversity-affirming physical healthcare, particularly for adolescents and young adults, remains insufficiently examined.
While the neurodiversity movement has been more extensively developed in Western contexts, its principles are increasingly relevant within the Saudi Arabian healthcare landscape. Recent efforts to expand autism services and improve care coordination nationally have begun to incorporate more holistic and person-centered approaches,19,20,26 creating opportunities for the integration of neurodiversity-affirming practices. However, the extent to which these perspectives are systematically reflected in service design and delivery remains limited, particularly in remote and underresourced areas.
Autism research in Saudi Arabia has grown considerably over the past decade. Prior studies have primarily focused on prevalence estimates, diagnostic practices, and family experiences, including parental stress and coping.27–29 A recent systematic review confirmed that ADHD and autism are the most studied neurodevelopmental disorders in Saudi Arabia, revealing that various societal groups, including healthcare professionals and the general public, lack knowledge about these conditions, which often leads to stigmatized attitudes toward autistic individuals. 30 Research has also documented the experiences of stigma among family members of autistic children in Saudi Arabia, including feelings of guilt, sadness, and instances of discrimination and social exclusion. 31 However, research examining sleep disturbance, gastrointestinal symptom severity, and the application of neurodiversity-affirming frameworks remains limited, particularly among adolescents and young adults. This study addresses these gaps by examining geographic disparities in physical health and neurodiversity-affirming practices within the Saudi context.
The COVID-19 pandemic further exposed and intensified preexisting structural vulnerabilities within healthcare systems. 32 Disruptions to in-person healthcare and the rapid shift toward telehealth highlighted longstanding inequities in service availability, coordination, and continuity, particularly in remote and underresourced regions. These broader disruptions also affected access to essential services for children and adolescents, particularly in contexts shaped by socioeconomic disadvantage and limited resources. 33 Emerging evidence, including a recent scoping review, suggests that autistic individuals and their families, especially in underresourced areas, experienced worsened mental and physical health outcomes during this period, including heightened anxiety, disrupted routines, and increased sleep and gastrointestinal difficulties.27,34–36
At the same time, the accelerated adoption of digital health tools and remote care modalities raised important concerns about whether such innovations reduce access inequities or instead risk reproducing, and in some cases amplifying, geographic disparities in the post-pandemic context, particularly when services are not designed to be autism and neurodiversity-affirming.14,37–39
These global patterns are particularly relevant to the Saudi Arabian context, where geographic disparities in access to specialized healthcare services are well documented.19,20,26 Accordingly, the present study examines whether post-pandemic shifts in healthcare delivery have addressed or sustained these inequities in sleep disturbance and gastrointestinal symptom severity among autistic adolescents and young adults.
Despite these converging issues, empirical research examining the intersection of geography, physical health, and neurodiversity-affirming practices remains scarce in the Arab region, and in Saudi Arabia in particular.27,28 Prior studies conducted in Saudi Arabia have largely focused on parental stress, educational challenges, or general service availability, with limited attention to sleep disturbance, gastrointestinal symptom severity, or to adolescents and young adults navigating the transition to adult-oriented healthcare systems.27,28 Moreover, few investigations have explicitly applied a neurodiversity-affirming framework to examine how systemic and geographic factors shape physical health equity.2,3,14
Against this backdrop, the present study examines geographic disparities in sleep disturbance, gastrointestinal symptom severity, healthcare access, and neurodiversity-affirming practices among autistic adolescents and young adults in Saudi Arabia.7,14,19 By centering sleep disturbance and gastrointestinal symptom severity as key dimensions of physical health equity, and shifting the analytic focus from individual-level characteristics to modifiable structural determinants, including healthcare access barriers and neurodiversity-affirming practices, this research seeks to inform the development of equitable, context-sensitive, and affirming healthcare models capable of supporting autistic individuals across diverse geographic settings.7,14
In this conceptual framework, geographic region is treated as the primary independent variable representing a structural determinant of healthcare access. Healthcare access barriers are examined as a mediator linking geographic disparities to sleep disturbance and gastrointestinal symptom severity, while neurodiversity-affirming practices are examined as a moderator that may buffer the impact of these barriers on outcomes.
This study focuses on autistic adolescents and young adults, a developmental period characterized by the transition from pediatric to adult healthcare systems, during which risks of service discontinuity and unmet healthcare needs are heightened.23,29
Present study
The present study examined geographic disparities in sleep disturbance and gastrointestinal symptom severity among autistic adolescents and young adults in Saudi Arabia, alongside differences in healthcare access barriers, neurodiversity-affirming practices, and digital health utilization. The study also tested whether healthcare access barriers mediated the relationship between geographic location and sleep disturbance and gastrointestinal symptom severity, and whether neurodiversity-affirming practices moderated these associations.
The study addressed the following research questions:
Are there differences in sleep disturbance and gastrointestinal symptom severity between autistic individuals living in urban versus remote areas? Do healthcare access barriers mediate the relationship between geographic location and sleep and gastrointestinal outcomes? Do neurodiversity-affirming caregiving practices moderate the relationship between healthcare access barriers and sleep disturbance and gastrointestinal outcomes?
Methods
Design and procedure
Ethics approval and consent to participate
We obtained ethical approval from the University Research Ethics Committee at the Deanship of Scientific Research, University of Jeddah (Application Number: U-REC-085). All participants provided informed consent electronically prior to participation.
The study recruited primary caregivers of autistic adolescents and young adults residing in Saudi Arabia. We recruited participants using a nonprobability convenience sampling approach through autism service providers, rehabilitation centers, educational institutions, and community networks that serve families of autistic individuals across both urban and remote regions of Saudi Arabia. Eligible caregivers received an electronic survey link through collaborating centers and professional networks. The first page of the survey included an informed consent statement outlining the purpose of the study, confidentiality assurances, voluntary participation, and the right to withdraw at any time without consequence. Participants did not receive financial or material compensation for participation in the study.
We collected data using a structured, self-administered electronic questionnaire. The survey assessed caregiver and family demographics, physical health challenges experienced by the autistic individual during the post-pandemic period, access to healthcare services (including telehealth), and the extent to which families adopted neurodiversity-informed health and daily living practices. The final analytic sample included 198 respondents. We determined a minimum sample size of 180 to achieve adequate statistical power (>0.80) for detecting medium effects in regression analyses using G*Power.
Participants
Based on a priori considerations to support robust geographic comparisons and adequate statistical power, the final sample included 198 primary caregivers of autistic adolescents and young adults aged 13–25 years. All participants were Saudi nationals. Eligible participants were primary caregivers of an autistic adolescent or young adult aged 13–25 years residing in Saudi Arabia and able to complete the survey in Arabic. We excluded respondents who did not complete the core sections of the survey or who did not meet the age criteria.
The majority of respondents were mothers (82%), with fathers comprising the remaining 18%. Participants were drawn from both urban (61%) and remote (39%) regions of Saudi Arabia. Detailed demographic, socioeconomic, physical health, and practice-related characteristics of the sample are presented in Table 1.
Demographic, Socioeconomic, Physical Health, and Neurodiversity-Affirming Practice Characteristics of Autistic Adolescents/Young Adults and Their Caregivers (N = 198)
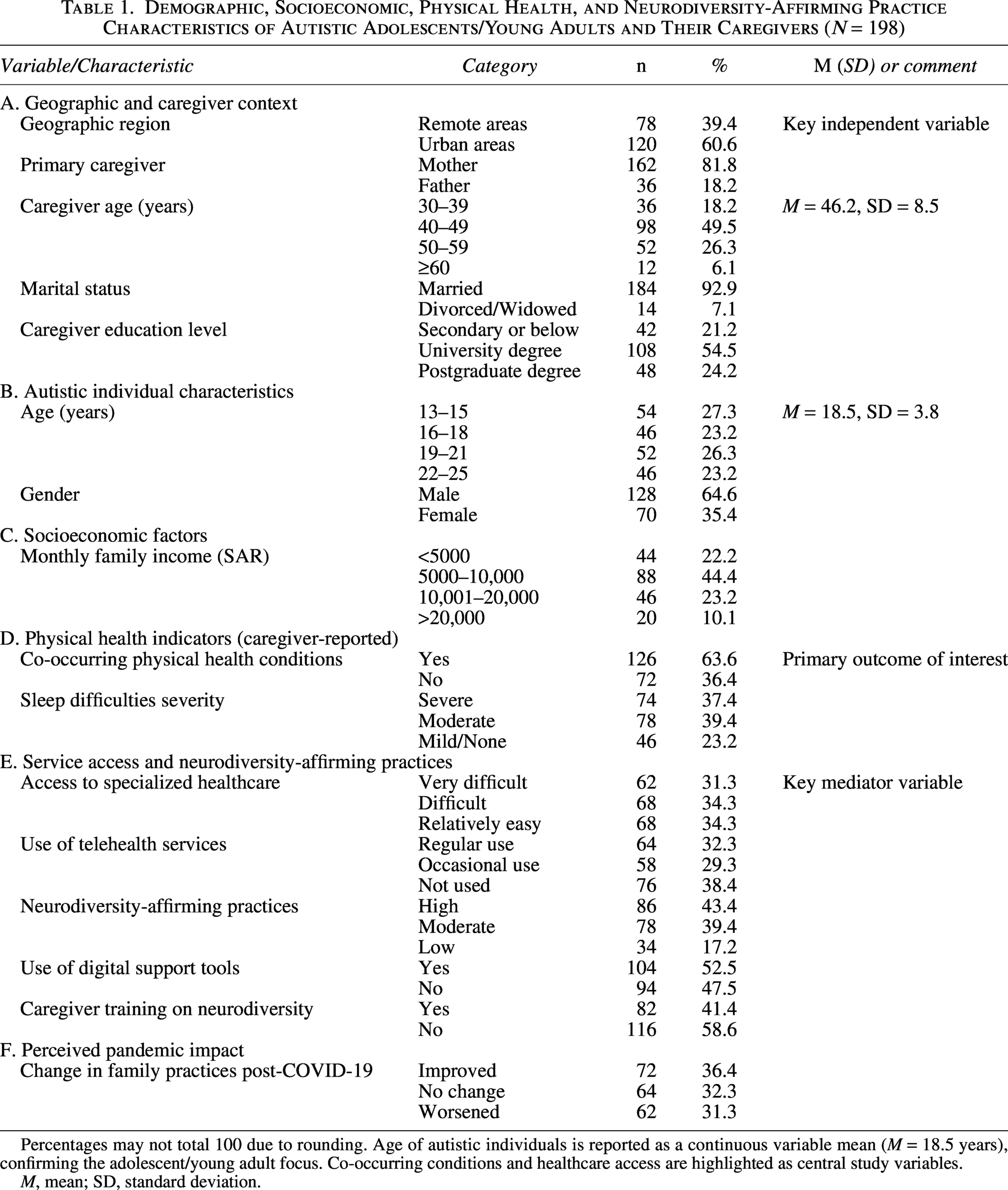
Percentages may not total 100 due to rounding. Age of autistic individuals is reported as a continuous variable mean (M = 18.5 years), confirming the adolescent/young adult focus. Co-occurring conditions and healthcare access are highlighted as central study variables.
M, mean; SD, standard deviation.
Among eligible caregivers successfully reached through collaborating centers and community networks, 68% completed the survey (n = 198). We excluded participants who did not meet inclusion criteria or submitted incomplete responses prior to analysis.
We classified participants’ residence as urban versus remote based on caregiver-reported location and cross-checked administrative region designations against national statistical definitions from the General Authority for Statistics. 33 Consistent with these standards, “urban” referred to major metropolitan centers (e.g., Riyadh, Jeddah, Dammam) with comparatively greater specialist availability, whereas “remote” referred to non-metropolitan localities, including smaller towns and rural settlements, typically characterized by limited local services and greater travel distances (e.g., >100 km) to tertiary healthcare centers.19,40
Instruments
The study employed a multicomponent measurement battery combining internationally standardized, psychometrically validated instruments with a limited set of context-specific items to ensure relevance to the Saudi Arabian healthcare setting and alignment with a neurodiversity-affirming framework.
Translation, cultural adaptation, and piloting
We administered all measures in Arabic following rigorous translation and cultural adaptation procedures. We used previously validated Arabic versions of the Social Responsiveness Scale–Second Edition (SRS-2), the Pittsburgh Sleep Quality Index (PSQI), and the abbreviated caregiver-report version of the Children’s Sleep Habits Questionnaire (CSHQ). Bilingual experts in autism and health research conducted forward and backward translation procedures for the Gastrointestinal Severity Index (6-GSI) and the adapted Barriers to Care Questionnaire (BCQ), with discrepancies resolved through panel consensus. The expert panel included researchers in autism and neurodiversity, bilingual specialists in health measurement, and autistic self-advocates, who collaboratively reviewed the translated instruments to ensure conceptual equivalence, cultural relevance, and linguistic clarity.
In addition to translation, we contextually adapted selected instruments to reflect the Saudi healthcare context. For example, we modified items in the BCQ to capture autism-specific services and locally relevant access barriers, including transportation distance, referral processes, service availability, and access to trained specialists.
We piloted the full battery with 30 caregivers representing diverse urban and remote regions to assess cultural appropriateness, comprehension, administration time, and feasibility. Piloting was conducted with caregivers only. We revised several items based on feedback, including clarifying the wording of selected sleep-related items to improve cultural clarity and comprehension. The full survey required ∼20–25 minutes to complete on average. Additional details regarding translation procedures, adapted instruments, and study-developed measures are provided in the Supplementary Data.
Caregiver-reported measurement approach
All primary outcome measures relied on caregiver report. We selected this approach because participants varied in communication abilities and levels of independence, which may limit the feasibility and reliability of self-report for some individuals. Caregiver-reported measures are widely used in autism health research, particularly when assessing observable health-related outcomes such as sleep and gastrointestinal symptoms.
In the Saudi Arabian context, caregiving is typically family-centered, with caregivers playing a central role in health-related decision-making and daily management. This cultural context further supports the use of caregiver-reported measures as a valid and appropriate source of information.19,20
Psychometric evaluation
Unless otherwise specified, higher scores indicate greater symptom severity, greater perceived barriers, or greater use of the measured construct. For all multi-item scales, we evaluated internal consistency reliability in the current sample using Cronbach’s alpha (α). We examined construct validity using item-total correlations and exploratory factor-analytic checks where appropriate, and we assessed convergent validity by testing theoretically expected associations between healthcare access barriers, neurodiversity-affirming practices, sleep disturbance, and gastrointestinal symptom severity.
Prior to hypothesis testing, we evaluated the psychometric performance of all key measures within the current Saudi Arabian sample. All adapted and newly developed scales demonstrated acceptable to excellent internal consistency. Specifically, the CSHQ showed excellent reliability (α = 0.89), as did the adapted BCQ (α = 0.91) and the Social Responsiveness Scale, Second Edition (SRS-2; α = 0.94). The PSQI (α = 0.82), the GSI (modified 6-item version; 6-GSI; α = 0.84), and the Neurodiversity-Affirming Practices Scale (NAPS) developed for this study (α = 0.88) demonstrated good to very good reliability. The context-specific Digital Health Utilization subscale showed acceptable reliability (α = 0.79).
We found that intercorrelations among study variables supported convergent validity. As hypothesized, healthcare access barriers were positively correlated with sleep disturbance severity (r = 0.45, p < 0.001) and gastrointestinal symptom severity (r = 0.38, p < 0.001). In contrast, neurodiversity-affirming practices were negatively correlated with sleep disturbance (r = −0.31, p < 0.001) and gastrointestinal severity (r = −0.28, p < 0.01). Digital health utilization was positively associated with neurodiversity-affirming practices (r = 0.25, p < 0.01) but not directly with physical health outcomes. Together, these findings indicate that the instruments functioned as theoretically expected within this context, supporting their suitability for subsequent analyses.
Physical health outcomes
Children’s Sleep Habits Questionnaire
We assessed sleep disturbances among autistic adolescents under 18 years using the CSHQ, 41 a caregiver-reported, norm-referenced instrument designed to assess common sleep behaviors in school-aged children. The CSHQ comprises 33 items organized into eight subscales (e.g., Bedtime Resistance, Sleep Onset Delay, Sleep Duration, Sleep Anxiety, Night Wakings, Parasomnias, Sleep-Disordered Breathing, and Daytime Sleepiness). Participants rated items on a 3-point frequency scale (rarely, sometimes, usually). Total and subscale scores are computed, with higher scores indicating greater sleep disturbance.
Pittsburgh Sleep Quality Index
For participants aged 18 years or older, we measured sleep quality using the PSQI. 42 The PSQI assesses sleep quality and disturbances over the previous month using 19 items, which yield seven component scores and a global score ranging from 0 to 21. Higher scores indicate poorer sleep quality, with scores >5 commonly reflecting clinically significant sleep problems. Participants completed the PSQI when feasible; otherwise, caregivers provided proxy reports. Prior autism health research has used proxy reports when self-report was not feasible.
Gastrointestinal Severity Index
We assessed gastrointestinal symptom severity using a caregiver-reported GSI, operationalized as the modified 6-item GSI (6-GSI) widely used in autism research. 43 The 6-GSI assesses the frequency and severity of core gastrointestinal symptoms, including constipation, diarrhea, abdominal pain, stool consistency, stool odor, and flatulence/gas. Caregivers rated each item on a 4-point scale (0 = none/not a problem, 1 = mild, 2 = moderate, 3 = severe), yielding a total severity score ranging from 0 to 18. Higher scores indicate greater gastrointestinal symptom burden. In the current sample, the scale demonstrated good internal consistency (Cronbach’s α = 0.84).
Co-occurring Physical Health Conditions Checklist.
Caregivers completed a brief checklist of co-occurring physical health conditions (e.g., epilepsy, allergies, asthma). We adapted these items from domains commonly used in autism clinical registries such as the Autism Treatment Network. We analyzed these items descriptively and did not combine them into a single psychometric scale.
Healthcare access barriers
Barriers to Care Questionnaire
We reviewed item wording to avoid ableist language, consistent with recent guidance for autism research. 44 We measured perceived barriers to healthcare access using an adapted version of the BCQ. 45 The BCQ is designed to assess experiences and circumstances that interfere with obtaining timely and appropriate care for children with special healthcare needs.
For this study, we contextually adapted items to reflect autism-related services and capture structural, logistical, financial, informational, and provider-related barriers relevant to urban versus remote settings (e.g., transportation distance, service availability, costs, referral procedures, stigma). For example, we modified general items referring to healthcare services to explicitly reference autism-specific diagnostic and therapy services for autistic individuals, and we expanded items addressing access barriers to reflect locally relevant challenges such as long travel distances to specialized centers, delays in referral pathways, and limited availability of trained autism specialists. We summed responses to all items to yield a total barrier score. Higher total scores reflect greater perceived barriers to care.
Neurodiversity-affirming practices
Neurodiversity-Affirming Practices Scale
We developed the NAPS specifically for the present study to assess caregiver practices that support autistic individuals’ autonomy, communication preferences, and sensory needs within everyday health-related contexts. The scale captures caregiver behaviors and attitudes, rather than system-level practices. We based the scale on contemporary neurodiversity scholarship and existing literature on affirming autism support practices,14,46 and aligned it with the study’s conceptual framework, which examines neurodiversity-affirming practices as a potential moderating factor in sleep disturbance and gastrointestinal symptom severity.
We generated an initial pool of items based on key domains identified in the literature.14,46 These domains included sensory accommodation, respect for communication styles, support for autonomy in health-related decisions, and validation of autistic identity. A panel of bilingual experts in autism and neurodiversity research reviewed the items to ensure content validity and cultural relevance within the Saudi context. We further refined the items through expert review by three autism and neurodiversity researchers and through feedback from a panel of autistic self-advocates and caregivers in Saudi Arabia to enhance clarity and contextual relevance.
The scale consists of 15 caregiver-reported items rated on a 5-point Likert scale (1 = never, 5 = always), with total scores ranging from 15 to 75. Higher scores indicate greater use of neurodiversity-affirming practices. We designed the items to reflect key principles of neurodiversity-affirming care, including autonomy, sensory accommodation, and respect for autistic identity.
We conducted exploratory factor analysis, which supported a unidimensional structure, with a single factor explaining 52.8% of the variance and item loadings ranging from 0.52 to 0.81. The scale demonstrated good internal consistency in the current sample (Cronbach’s α = 0.88). We found evidence of construct validity through expected associations with key study variables, including negative correlations with sleep disturbance and gastrointestinal symptom severity, and positive associations with supportive caregiving practices. We provide the full-scale items, scoring procedures, and detailed descriptions in the Supplementary Data (Section S1).
Digital health utilization
Digital Health Utilization Subscale
We assessed digital health utilization using a brief, context-specific subscale developed for this study to capture the frequency and perceived usefulness of telehealth consultations, mobile health applications, and online caregiver support networks.37–39 The expert panel reviewed the items, and we averaged them to yield a mean utilization score, with higher scores indicating greater digital health utilization. Caregivers rated the items on a 5-point Likert scale (1 = never/not useful, 5 = very frequent/very useful).
Covariates
Social Responsiveness Scale, Second Edition (SRS-2)
We controlled for autism-related characteristics using the Social Responsiveness Scale, Second Edition. 47 The parent-reported form includes 65 items assessing social awareness, social cognition, social communication, social motivation, and restricted and repetitive behaviors. We used the total T-score as a covariate to adjust for variation in core autism trait severity. Additional covariates included caregiver education, household income, family structure, and geographic region (urban vs. remote).
Data analysis
We analyzed cohort data (N = 198) using IBM SPSS Statistics (version 29). We conducted mediation and moderation analyses using the PROCESS macro. 48 We computed descriptive statistics to summarize participant characteristics and key study variables. We then performed bivariate analyses to examine urban and remote differences in sleep disturbance severity, gastrointestinal symptom severity, healthcare access barriers, digital health utilization, and neurodiversity-affirming practice scores, using independent-samples t-tests for continuous variables and chi-square tests for categorical variables.
To identify predictors of sleep disturbance severity and gastrointestinal symptom severity, we conducted hierarchical multiple regression analyses. We entered demographic covariates in Block 1, followed by geographic region in Block 2. We then entered healthcare access barriers and neurodiversity-affirming practice scores in the final block to evaluate their incremental explanatory contribution and their roles in the hypothesized pathways.
We tested mediation and moderation models using PROCESS Models 4 and 1 with 5000 bootstrap resamples. These analyses evaluated whether healthcare access barriers mediated the association between geographic region and sleep disturbance and gastrointestinal symptom severity, and whether neurodiversity-affirming practices moderated (i.e., buffered) the effects of these barriers on outcomes. We considered indirect effects statistically significant when the 95% bootstrap confidence intervals did not include zero.
We observed minimal missing data, affecting <2% of responses across all variables. Given this very low rate of missingness, we considered listwise deletion appropriate and excluded participants with missing data on variables required for specific analyses from those analyses. We further supported this approach by confirming the absence of systematic patterns in missingness. Sensitivity analyses using pairwise deletion produced substantively identical results, supporting the robustness of the findings. We set statistical significance at p < 0.05 for all analyses.
Results
Sample characteristics and preliminary descriptives
The sample included 198 caregivers of autistic adolescents and young adults aged 13–25 years (M = 18.5, SD = 3.8). Table 1 presents the sample characteristics and geographic distribution of participants, with 39% (n = 78) residing in remote areas and 61% (n = 120) in urban areas. Most caregivers were mothers (82%) and had attained a university-level education or higher (79.7%). Notably, 63.6% of autistic individuals had at least one co-occurring physical health condition, and 76.8% experienced moderate to severe sleep difficulties.
We first examined the direct association between geographic region and sleep disturbance and gastrointestinal symptom severity. We then tested whether healthcare access barriers mediated these relationships. Finally, we tested whether neurodiversity-affirming practices moderated the relationship between healthcare access barriers and sleep disturbance and gastrointestinal symptom severity.
Urban and remote disparities in sleep disturbance and gastrointestinal symptom severity
We conducted independent-samples t-tests and found significant geographic disparities in physical health outcomes. Autistic individuals residing in remote areas exhibited significantly greater sleep disturbances and gastrointestinal symptom severity than those in urban areas. Table 2 presents these differences. Specifically, sleep disturbance scores (CSHQ/PSQI) were significantly higher in remote regions (M = 48.2, SD = 5.1) than in urban areas (M = 41.5, SD = 4.8), t(196) = 4.87, p < 0.001, Cohen’s d = 0.69. Likewise, gastrointestinal symptom severity (GSI) was higher in the remote group (M = 15.8, SD = 3.9) than in the urban group (M = 12.1, SD = 3.5), t(196) = 3.42, p = 0.001, Cohen’s d = 0.51. These effect sizes ranged from moderate to large.
Urban–Remote Differences in Physical Health Outcomes
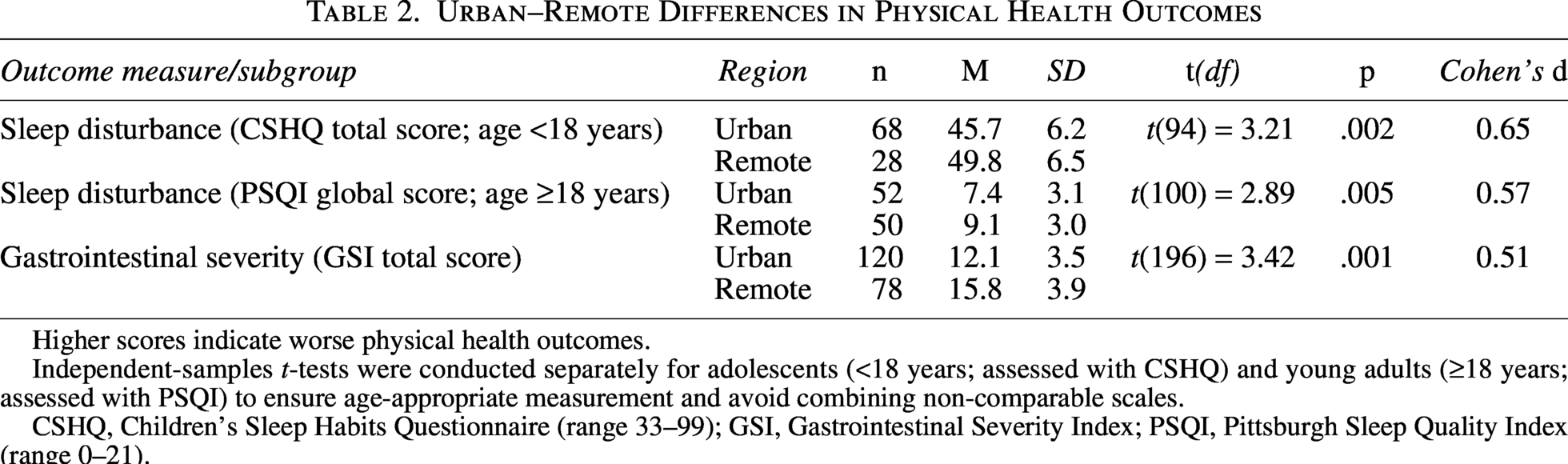
Higher scores indicate worse physical health outcomes.
Independent-samples t-tests were conducted separately for adolescents (<18 years; assessed with CSHQ) and young adults (≥18 years; assessed with PSQI) to ensure age-appropriate measurement and avoid combining non-comparable scales.
CSHQ, Children’s Sleep Habits Questionnaire (range 33–99); GSI, Gastrointestinal Severity Index; PSQI, Pittsburgh Sleep Quality Index (range 0–21).
Geographic differences in healthcare access and neurodiversity-affirming practices
We found significant geographic disparities in access to care and caregiving approaches. Table 3 shows that caregivers in remote regions reported significantly greater barriers to accessing healthcare services on the BCQ (M = 38.4, SD = 6.7) compared with urban caregivers (M = 29.1, SD = 5.9), t(196) = 5.91, p < 0.001, Cohen’s d = 0.84. Conversely, scores on the NAPS were significantly lower in remote areas (M = 32.1, SD = 7.2) than in urban areas (M = 38.5, SD = 6.4), t(196) = −3.88, p < 0.001, Cohen’s d = 0.63. These results reflect higher reported barriers to care alongside lower levels of neurodiversity-affirming practices in remote regions. We found no significant geographic difference in telehealth utilization scores (p = 0.12).
Geographic Differences in Healthcare Access, Neurodiversity-Affirming Practices, and Digital Health Utilization
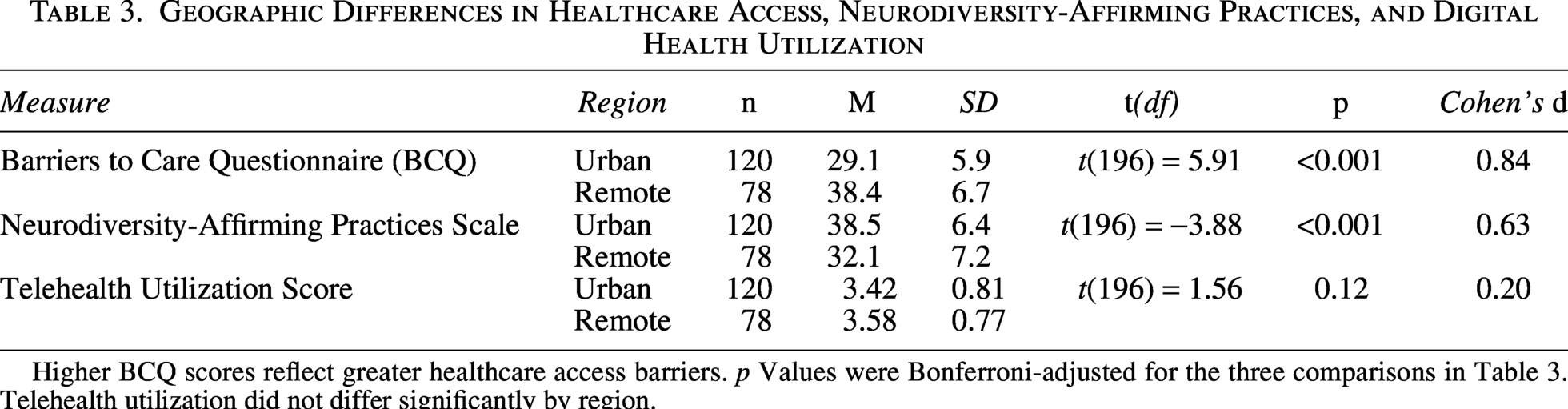
Higher BCQ scores reflect greater healthcare access barriers. p Values were Bonferroni-adjusted for the three comparisons in Table 3. Telehealth utilization did not differ significantly by region.
Structural pathways linking geography to sleep disturbance and gastrointestinal symptom severity
Hierarchical regression analysis
Table 4 presents multivariate regression models examining sleep disturbance severity. We found that healthcare access barriers were independently associated with worse sleep outcomes, whereas neurodiversity-affirming practices were associated with better sleep outcomes. Table 4 (Part A) shows these results. To examine whether structural factors help explain the geographic disparity in sleep disturbance, we conducted a hierarchical multiple regression (Table 4). After controlling for autism symptom severity (SRS-2 total T-score) and age in Model 1 (R2 = 0.18, p < 0.01), adding geographic region in Model 2 significantly improved model fit (ΔR2 = 0.12, p < 0.001), with remote residence associated with greater sleep disturbance (β = 0.34, p < 0.001). In Model 3, we found that healthcare access barriers (β = 0.29, p < 0.001) and neurodiversity-affirming practices (β = −0.22, p = 0.001) significantly predicted sleep outcomes. We also found that the direct effect of geographic region decreased and became non-significant (β = 0.11, p = 0.08).
Multivariate Regression and Mediation/Moderation Results Predicting Physical Health Outcomes
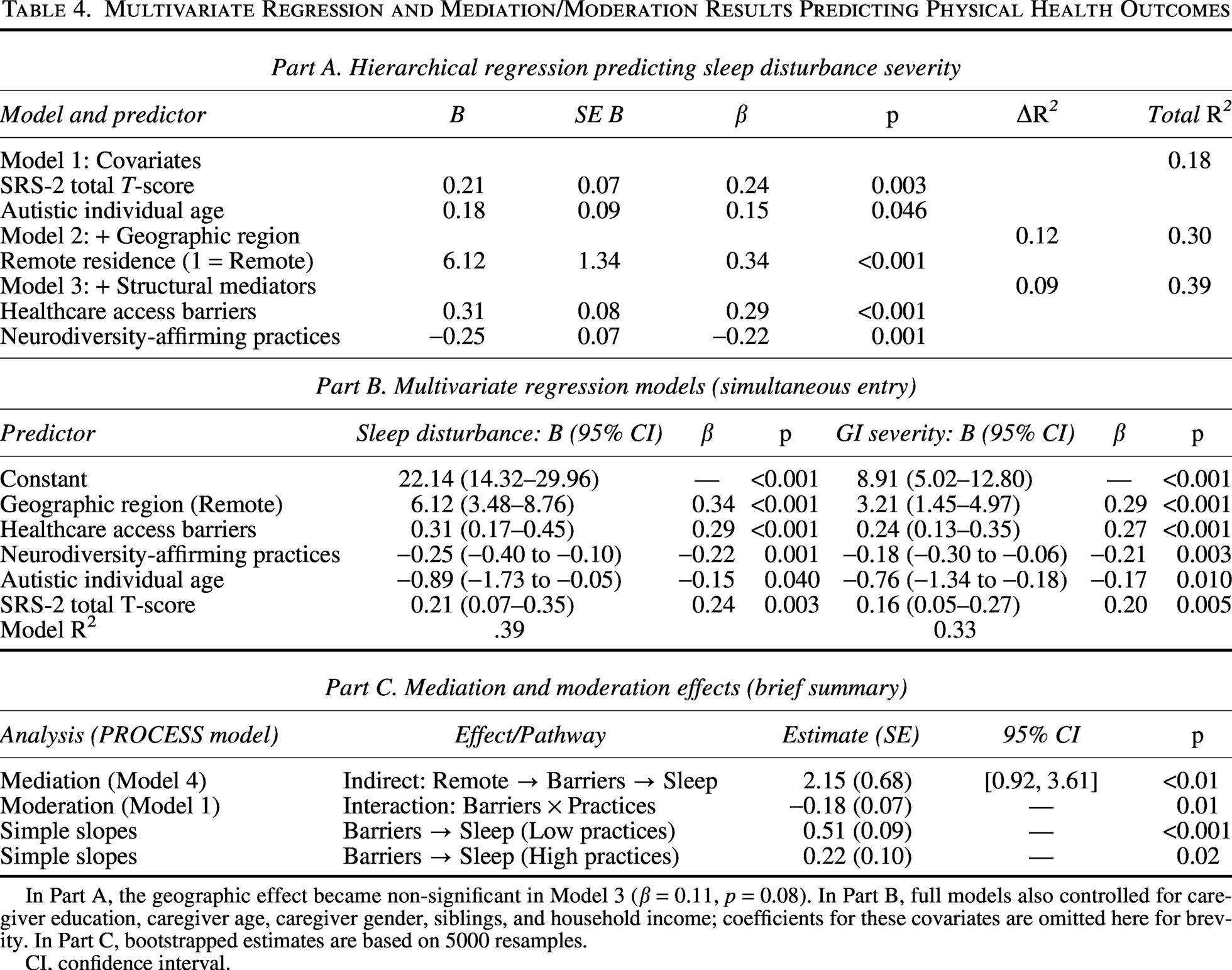
In Part A, the geographic effect became non-significant in Model 3 (β = 0.11, p = 0.08). In Part B, full models also controlled for caregiver education, caregiver age, caregiver gender, siblings, and household income; coefficients for these covariates are omitted here for brevity. In Part C, bootstrapped estimates are based on 5000 resamples.
CI, confidence interval.
Multivariate regression models
We estimated multivariate linear regression models to quantify the relative contributions of demographic characteristics and modifiable structural factors to sleep disturbance severity and gastrointestinal symptom severity. We fit two comprehensive models in which we entered all predictors simultaneously and modeled sleep disturbance severity and gastrointestinal symptom severity (GSI) as separate dependent variables. Table 4 (Part B) shows these results. We adjusted all models for autism symptom severity (SRS-2 T-score).
We found that geographic region remained a significant independent predictor of both outcomes. Compared with urban residence, remote residence was associated with more severe sleep disturbance (β = 0.34, p < 0.001) and greater gastrointestinal severity (β = 0.29, p < 0.001). We found that healthcare access barriers were the strongest modifiable risk factor, showing robust positive associations with sleep (β = 0.29, p < 0.001) and gastrointestinal severity (β = 0.27, p < 0.001). In contrast, we found that neurodiversity-affirming practices were the strongest protective factor, independently predicting lower sleep disturbance (β = −0.22, p = 0.001) and lower gastrointestinal severity (β = −0.21, p = 0.003).
We found that autistic individual age was the only demographic variable that showed consistent associations, with older age linked to lower symptom severity for sleep (β = −0.15, p = 0.040) and gastrointestinal outcomes (β = −0.17, p = 0.010). Caregiver education, caregiver age, gender, number of siblings, and household income did not show reliable effects after accounting for the structural predictors. We found that overall model fit was strong (sleep: R2 = 0.39; gastrointestinal: R2 = 0.33).
Mediation and moderation analyses
We conducted formal analyses to test the pathways implied by the regression models. Using bootstrapped mediation (PROCESS Model 4; 5000 resamples), we found that healthcare access barriers significantly mediated the association between remote residence and worse sleep outcomes (indirect effect = 2.15, SE = 0.68, 95% CI [0.92, 3.61]) (see Table 4, Part C).
Moderation analysis (PROCESS Model 1) showed a significant protective role of neurodiversity-affirming practices. The interaction between healthcare access barriers and neurodiversity-affirming practices was significant (β = −0.18, SE = 0.07, p = 0.01). Simple slopes analysis showed that healthcare access barriers were strongly associated with poorer sleep among caregivers reporting low levels of neurodiversity-affirming practices (β = 0.51, SE = 0.09, p < 0.001). In contrast, this association was weaker among caregivers reporting high levels of neurodiversity-affirming practices (β = 0.22, SE = 0.10, p = 0.02), indicating a buffering effect of neurodiversity-affirming practices on the relationship between healthcare access barriers and sleep outcomes.
Discussion
This study yielded three central findings that directly address its aims. First, we observed significant urban and remote disparities in sleep disturbance and gastrointestinal symptom severity of autistic adolescents and young adults in Saudi Arabia, with those in remote areas experiencing more severe sleep disturbances and gastrointestinal symptoms. Second, these health disparities were accompanied by a compounded geographic disadvantage in structural determinants: families in remote areas reported greater barriers to healthcare access and lower levels of neurodiversity-affirming practices, despite comparable levels of telehealth use. Third, mediation and moderation analyses indicated that healthcare access barriers partially mediated the relationship between geographic region and sleep disturbance and gastrointestinal symptom severity, while neurodiversity-affirming practices moderated (i.e., buffered) the negative impact of these barriers.
Together, these findings indicate that geographic health inequities are shaped not only by location but also by modifiable systemic factors, particularly barriers to healthcare access and variation in the adoption of neurodiversity-affirming practices. The findings indicate that autistic individuals living in remote areas experience more severe sleep disturbance and gastrointestinal symptoms in part because they face greater structural barriers, and that these barriers are differentially mitigated by caregiver-level practices.
Guided by a neurodiversity-affirming framework, we examined structural determinants of sleep disturbance and gastrointestinal symptom severity among autistic adolescents and young adults in Saudi Arabia. Our findings indicate that geographic inequities are associated with worse sleep disturbance and gastrointestinal symptoms, in part through systemic barriers to healthcare access, as shown by the significant mediation effect. This suggests that remote residence is associated with worse outcomes not directly, but through increased barriers to accessing timely and appropriate care.
We found that neurodiversity-affirming practices acted as a protective factor, buffering the negative impact of these barriers. Together, these results align with international evidence on autism-related health inequities while offering context-specific insights relevant to service planning and policy in Saudi Arabia.8,9,18 Although rural and urban disparities have been documented primarily in Western settings, 6 our findings suggest similar patterns in a non-Western context characterized by centralized services and rapid post-pandemic digital expansion.
Geographic disparities as structural determinants of sleep and gastrointestinal health
The pronounced urban and remote disparities observed in sleep disturbance and gastrointestinal symptoms are consistent with the social model of disability and extend its relevance to sleep disturbance and gastrointestinal symptom severity within the Arab region.17,49 We found that remote residence was associated with more severe sleep disturbance and gastrointestinal symptoms, even after accounting for autism traits, age, and socioeconomic factors.
Our findings further support this interpretation: Telehealth utilization did not differ significantly across regions and was not associated with improved sleep and gastrointestinal outcomes. Together, these results indicate that access alone, whether physical or digital, is insufficient without attention to the quality and appropriateness of care.
The mediation findings provide further insight into the mechanisms underlying these disparities, indicating that structural barriers to healthcare access partially account for the relationship between geographic location and sleep outcomes. In other words, remote residence increases exposure to access barriers, which in turn contributes to worse sleep outcomes and gastrointestinal symptoms.
This finding aligns with international evidence describing a “postcode lottery,” in which access to appropriate healthcare is shaped more by geography than by clinical need.8,9 Importantly, increased service availability does not necessarily translate to neurodiversity-affirming care. Our findings suggest that the quality and orientation of services, rather than availability alone, are critical in shaping health outcomes, particularly in the context of telehealth.
In Saudi Arabia, these results empirically confirm longstanding concerns regarding the concentration of services for autistic individuals in major urban centers.19,20 Cultural factors, including stigma surrounding autism, may also influence healthcare access and the adoption of neurodiversity-affirming practices in the Saudi context.19,20
Recent research in Saudi Arabia has documented that families of autistic individuals experience profound emotional distress, including feelings of guilt, sadness, and self-blame, as well as instances of discrimination and social exclusion due to prevalent misconceptions about autism. 31 A systematic review further confirmed that lack of knowledge about neurodevelopmental disorders among healthcare professionals and the general public leads to stigmatized attitudes toward autistic individuals. 30 Such stigmatizing attitudes can discourage families from seeking appropriate care or disclosing their child’s diagnosis, thereby compounding the structural barriers already faced by those in remote areas.
Although mobile health initiatives offer partial mitigation, mediation analyses indicate that persistent structural barriers to care partially explain the association between remote residence and poorer sleep outcomes. 26 These disparities likely reflect system-level inequities linked to healthcare access, service distribution, and broader structural conditions, highlighting the relevance of neurodiversity-affirming frameworks that emphasize justice, accessibility, and equitable health opportunity.2,3
The protective role of neurodiversity-affirming practices
Neurodiversity-affirming practices can be viewed as a practical, strengths-based support that helps families navigate healthcare barriers by emphasizing accessibility, autonomy, and respectful communication. 50
Importantly, the moderation findings indicate that neurodiversity-affirming practices alter the strength of the relationship between healthcare access barriers and sleep outcomes. Specifically, the association between barriers and poorer sleep was weaker among caregivers reporting higher levels of neurodiversity-affirming practices, suggesting a buffering effect at the family level.
A key contribution of this study lies in its empirical integration of neurodiversity-affirming practices into a structural health disparities model. Caregivers in remote regions reported significantly lower adoption of neurodiversity-affirming practices, suggesting differential exposure to contemporary neurodiversity-aligned knowledge and training. This represents a form of compounded disadvantage, wherein geographic isolation restricts not only access to services but also access to evolving care paradigms increasingly endorsed in international autism research and practice.2,3,14
From a practical standpoint, these findings suggest that building neurodiversity-affirming competencies among caregivers and frontline providers may enhance adaptive coping at the family level while broader systemic reforms are pursued. In underresourced settings, affirming practices may partially compensate for limited specialist access by enabling caregivers to implement individualized, respectful adaptations that directly address sleep routines, sensory regulation, and gastrointestinal discomfort. Importantly, this does not shift responsibility onto families but highlights an immediately actionable lever for improving well-being within structurally constrained environments.2,3,14
Telehealth: An unrealized equitable tool in the Saudi context
International studies have documented similar patterns, where telehealth expansion has failed to reduce disparities when services are not autism-competent, culturally responsive, or aligned with neurodiversity-affirming principles.9,14,38,39 In the Saudi context, telehealth initiatives for autistic children have likewise highlighted that access depends not only on connectivity but also on service design and implementation tailored to families’ needs. 19 Evidence from rural and remote settings further indicates that digital expansion may leave inequities unchanged when accessibility needs and provider training are not adequately addressed. 51
In Saudi Arabia, recent evaluations highlight promising growth in digital health platforms and mobile health clinics, yet persistent concerns remain regarding their specialization, continuity, and autism-specific training.24,26 Consistent with these patterns, our findings indicate that telehealth use, in its current form, was not independently associated with improved sleep and gastrointestinal outcomes. These findings indicate that many digital and mobile services may reproduce existing systemic limitations rather than address them. Future studies should validate these findings across independent samples and cultural contexts, as their capacity to provide ongoing, specialized, and neurodiversity-informed care for autistic individuals remains uncertain.
Accordingly, these findings highlight the need to move beyond generic telehealth provision toward codesigned, neurodiversity-affirming digital care models. Such approaches may include asynchronous consultations, structured caregiver coaching, specialist support for primary care providers in remote regions, and accessible digital resource libraries developed in partnership with autistic individuals and families. Embedding affirming principles into both in-person and digital services is essential if telehealth is to function as an equity-enhancing tool rather than a neutral technological overlay.14,38,39,52
Limitations
We note several limitations when interpreting these findings. First, the cross-sectional design precludes causal inference regarding the relationships between geographic location, healthcare access barriers, and sleep disturbance and gastrointestinal symptom severity. Second, the primary quantitative data relied on caregiver reports, which limit direct insight into autistic individuals’ own perspectives. Third, while the sample size was adequate for the planned analyses and included families from multiple regions, it may not fully capture the heterogeneity of all remote and underserved areas within Saudi Arabia.
Recruitment via service networks may have underrepresented the most isolated remote families. Future longitudinal research should examine how changes in healthcare access and service models influence sleep and gastrointestinal health trajectories over time. Most importantly, participatory research approaches that actively involve autistic adults from diverse geographic backgrounds in the design, implementation, and evaluation of interventions represent a crucial next step to ensure that proposed solutions are genuinely neurodiversity-affirming, context-sensitive, and effective.8,9,18
Although caregiver reports were appropriate given the family-centered context of care, they may not fully capture the subjective experiences of autistic individuals, particularly those able to self-report.
In addition, the study focused on only two physical health domains (sleep disturbances and gastrointestinal symptoms). Although these are among the most commonly reported co-occurring conditions in autistic adolescents and young adults, future research should examine a broader range of physical health challenges, including immune-related, musculoskeletal, and other comorbidities.
Most importantly, although the newly developed NAPS demonstrated strong internal consistency (α = 0.88) and initial evidence of construct validity in this sample, researchers have not yet validated this novel measure in independent samples. It is also important to note that the NAPS assesses caregiver-reported practices (e.g., sensory accommodation, respect for communication styles, support for autonomy) rather than the practices of healthcare providers. While our findings indicate that caregiver practices play a protective role, they do not directly assess whether healthcare services themselves were neurodiversity-affirming. Future research should examine its psychometric properties across larger and more diverse populations, as well as investigate provider-level practices and how they interact with family-level strategies to shape health outcomes.
Finally, although we undertook substantial efforts to support translation accuracy and cultural adaptation, including expert review and pilot testing, we did not independently subject some translated and contextually adapted instruments to full psychometric validation within the present study. In addition, the relatively high proportion of highly educated caregivers in the sample may limit the generalizability of the findings to broader caregiver populations.
Conclusion and recommendations
This study demonstrates that the physical health disparities experienced by autistic adolescents and young adults in Saudi Arabia can be understood as issues of geographic justice, systemic design, and healthcare access inequities. By identifying an association between remote residence and more severe sleep disturbance and gastrointestinal symptoms, partly explained by healthcare access barriers, and by identifying neurodiversity-affirming practices as a modifiable protective factor, the findings offer a clear and actionable framework for change. Advancing the sleep, gastrointestinal health, and overall well-being of autistic individuals across Saudi Arabia requires a sustained commitment to reducing spatial inequities in service provision and to building a healthcare system that is not only geographically accessible but also authentically affirming of neurodivergent identities. Such efforts are both a practical necessity and an ethical imperative, aligning closely with the principles of neurodiversity and the objectives of Saudi Vision 2030 related to health equity and quality of life.
Future research should prioritize participatory approaches that directly involve autistic adolescents and young adults in study design and data collection, in keeping with the principle of “nothing about us without us.”2,3 While the present study relied on caregiver-reported quantitative data, meaningful inclusion of autistic voices, particularly from those able to self-report, remains a critical priority for advancing equitable and context-sensitive research in this area.
Implications for policy and practice in Saudi Arabia
Drawing on these findings, we identify several policy and practice priorities:
Decentralize and specialize
National autism policy should prioritize the development of autism-specific expertise within primary healthcare services in remote regions, alongside sustainable outreach and consultation models linked to tertiary centers.
Invest in neurodiversity-affirming capacity building
Systematic training programs for healthcare providers and caregivers in neurodiversity-affirming principles should be considered essential components of health system infrastructure for health equity, rather than optional enhancements. This directly supports Saudi Vision 2030 goals related to human capital development and quality of life.
Re-engineer tele-support models
The Ministry of Health and partner institutions should invest in the development and evaluation of national digital autism health platforms that are codesigned with autistic individuals and families, ensuring accessibility, sensory sensitivity, and practical clinical relevance.
Shift the public health narrative
Public health messaging should move away from frameworks emphasizing individual caregiver “burden” toward a rights-based perspective that centers systemic responsibility and affirms the right of every autistic person, regardless of geographic location, to respectful, accessible, and high-quality healthcare. This includes replacing terms like “burden on families” with language emphasizing shared societal responsibility and autistic self-advocacy.
Footnotes
Acknowledgments
The authors extend their appreciation to the Deanship of Postgraduate Studies and Scientific Research at Majmaah University for funding this research through project number (R-2026-238). They are grateful to the autistic individuals and families who participated in this study and shared their experiences. They also thank the autism service providers and community organizations across Saudi Arabia who assisted with participant recruitment, and the autistic self-advocates who provided valuable feedback on study materials.
Authorship Confirmation Statement
A.F.A.: Conceptualization, methodology, investigation, writing—original draft, visualization, supervision, and project administration. F.A.: Data curation, formal analysis, and writing—review and editing. The article has been submitted solely to Autism in Adulthood.
Data Availability
All data supporting the findings of this study are provided in the article and its appendices. Additional anonymized raw data are available from the corresponding author upon reasonable request due to institutional data protection policies.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors extend their appreciation to the Deanship of Postgraduate Studies and Scientific Research at
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.