
Abstract
Introduction:
This systematic review evaluated randomized controlled trials (RCTs) conducted specifically in participants with diabetes and painful peripheral neuropathy to assess the effectiveness and safety of medical cannabis, isolated cannabinoids, or nationally approved cannabis-based medicines as adjuvant treatment, compared with placebo or baseline.
Materials and Methods:
Controlled clinical studies and RCTs in adults with diabetic peripheral neuropathy were eligible. Animal and in vitro studies were excluded. We searched PubMed, Google Scholar, Cochrane Library, and Scopus and screened 15,377 records; 35 full-text articles were assessed for eligibility, and 4 RCTs were included in the qualitative synthesis.
Results:
Three of four studies reported statistically significant reductions in neuropathic pain with cannabinoid-based interventions compared with placebo, whereas one trial did not demonstrate superiority. In two trials using vaporized or sublingual Δ9-tetrahydrocannabinol (THC), doses in the range of approximately 16–18 mg were associated with clinically meaningful pain relief in participants. Adverse effects, including dizziness and cognitive symptoms, were common but generally mild-to-moderate, and discontinuations due to adverse effects varied across studies.
Discussion/Conclusion:
Evidence from four small, heterogeneous RCTs suggests that cannabinoid-based therapies may reduce pain in some patients with diabetic peripheral neuropathy; however, the limited number of studies, variability in formulations and comparators, and risk of bias preclude firm conclusions regarding efficacy. Observed THC doses around 16–18 mg/day delivered via vaporized or sublingual routes should be viewed as preliminary, hypothesis-generating ranges rather than definitive recommendations. Larger, contemporary RCTs with rigorous risk-of-bias control, standardized outcomes, and detailed safety reporting are needed.
Introduction
Neuropathic pain affects an estimated 20 million people in the United States, and over 50% of patients with diabetes will develop some form of peripheral neuropathy during their lifetime. 1 The mechanism is complex and largely idiopathic, causing pain through a combination of nerve damage, altered pain signaling pathways, inflammation, and central nervous system (CNS) changes. 2 Damaged sensory nerves can become hypersensitive and lead to abnormal pain signaling to the brain. In addition, changes in the CNS can lead to perceived amplification of pain. Peripheral neuropathy is characterized by weakness, pain, and paresthesia, typically in the hands and feet. While metabolic disorders such as diabetes can lead to peripheral neuropathy, other common causes include viral infections (e.g., postherpetic neuralgia), autoimmune disorders (e.g., multiple sclerosis or rheumatoid arthritis), trauma (e.g., spinal cord injury), and cancer treatments (e.g., chemotherapy, radiation, or surgery). 3
Traditional treatment options aim to manage pain and improve function, including anticonvulsants, tricyclic antidepressants, and serotonin–norepinephrine reuptake inhibitors. The three oral medications approved by the Food and Drug Administration (FDA) for peripheral neuropathy are duloxetine, pregabalin, and tapentadol. 4 These medications are limited by sometimes significant adverse effects and insufficient pain relief. This can often result in a worsening quality of life and lead to emotional, cognitive, and functional impairment. Despite the significant morbidity involved with peripheral neuropathy, it often remains undertreated; also, historically, only 50% of patients have responded to traditional medication treatments.1,4 Thus, patients are seeking other tools, including complementary and alternative treatments, to assist with providing relief for peripheral neuropathy.
When discussing medical cannabis, the main cannabinoids are Δ9-tetrahydrocannabinol (THC) and cannabidiol (CBD). 5 THC acts as a partial agonist at cannabinoid (CB1 and CB2) receptors and can produce euphoria and psychotropic effects, especially in higher doses. The CB1 receptors are located in the basal ganglia and cerebellum, and in the dorsal horn of the spinal cord, which conducts and modulates pain signals. The CB2 receptors, located in peripheral tissues and organs, are thought to help regulate inflammation, allodynia, and hyperalgesia. The cannabinoid CBD is not psychoactive. It has anti-inflammatory properties and may reduce pain and inflammation. Also, when used in combination with THC, CBD may attenuate the psychoactive effects of THC. 5 Both CBD and THC display activity on transient receptor potential (TRP) channels, which detect pain stimuli. 6 Some TRP channels that may have roles in modulating neuropathic pain include TRPV1 and TRPV4 (vanilloid) and TRPM8 (melastatin). Given the contribution of inflammation and altered nociceptive processing to diabetic peripheral neuropathy, modulation of CB1 and CB2 receptors and TRP channels provides a biological rationale for exploring cannabinoids as adjuvant analgesics.5,6
Chronic pain is the most common qualifying condition for states who have medical cannabis programs, and nine states specify neuropathy as a qualifying condition. 7 A few systematic reviews have been published regarding the effect of medical cannabis for treating chronic pain and/or neuropathic pain. These reviews included from 16 to 35 randomized controlled trials (RCTs). Three of these reviews reported pain reduction as being significant (e.g., ≥30% pain reduction) in comparison with placebo.8–10 The Whiting et al. review recommended that moderate quality evidence supports the use of cannabinoids for chronic pain. 8 The Nugent et al. review stated that limited evidence suggested that cannabis may alleviate neuropathic pain in some participants. 9 Conclusive or substantial evidence that cannabis or cannabinoids are effective for treating chronic pain was suggested by the National Academies of Sciences, Engineering, and Medicine. 10
For the treatment of chronic neuropathic pain, the Cochrane Database of Systematic Reviews found that cannabis-based medicines were better than placebo. 11 Due to the variability in individual responses and adverse effects, however, the authors stated that benefits may be outweighed by harms. A review from the American Society of Pain and Neuroscience published in 2023 gave use of medical cannabis for neuropathic pain evidence a level 1 with a grade of C. 12 They stated that while several RCTs support the use of medical cannabis for neuropathic pain, more large-scale RCTs are needed.
The aforementioned systematic reviews and RCTs compare the effect of medical cannabis versus placebo in patients with chronic pain and/or neuropathic pain. However, neuropathic pain in patients with diabetes can differ significantly from neuropathic pain arising from other modalities. 13 Existing systematic reviews of medical cannabis for chronic or neuropathic pain have largely combined heterogeneous etiologies and typically include few participants with diabetic peripheral neuropathy specifically.8–12 Diabetic neuropathic pain may differ in pathophysiology, comorbidities, and treatment response from other neuropathic conditions. 13 Therefore, a focused synthesis of RCTs and randomized studies conducted exclusively in patients with diabetes and peripheral neuropathy is needed to better inform clinicians about potential benefits, risks, and practical dosing considerations for this population.
Materials and Methods
This systematic review was conducted and reported in accordance with the PICOTS framework and was prospectively registered in PROSPERO (CRD42024577694). The review addressed the following primary question:
What RCTs or controlled studies have evaluated medical cannabis, isolated cannabinoids (alone or in combination), or nationally approved cannabinoid formulations versus placebo, a traditional comparator medication, or versus baseline in participants with peripheral neuropathy associated with diabetes?
The specific aims were to determine:
Which formulation(s) and/or dosing regimens of medical cannabis have been shown to be effective for pain management of peripheral neuropathy in persons with diabetes? Which formulation(s) and/or dosing regimens of isolated cannabinoids, alone or in combination, have been shown to be effective for pain management of peripheral neuropathy in persons with diabetes? Which formulation(s) and/or dosing regimens of nationally approved cannabinoid products (e.g., Sativex®/nabiximols, Epidiolex®/cannabidiol oil, Marinol®/dronabinol, Cesamet®/nabilone) have been shown to be effective for pain management of peripheral neuropathy in persons with diabetes?
Search strategy
A systematic literature search was conducted in PubMed, Google Scholar, Cochrane Library, and Scopus from database inception to December 31, 2024. The following Boolean search strategy was used and adapted as appropriate for each database:
(Neuropathy OR “peripheral neuropathy”) AND diabetes AND (cannabis OR marijuana OR “Δ9-tetrahydrocannabinol” OR THC OR cannabidiol OR CBD OR nabiximols OR Sativex OR nabilone OR dronabinol OR Marinol OR Epidiolex).
Reference lists of included studies and relevant reviews were manually screened to identify additional eligible trials. Only articles published in English were considered.
Inclusion/Exclusion criteria
Studies were eligible if they met all of the following criteria:
Population: Adults with peripheral neuropathy attributable to diabetes. Intervention: Any formulation, route, or dose of medical cannabis or cannabinoid (e.g., plant-derived products, synthetic cannabinoids, or approved pharmaceutical preparations). Comparator: Placebo, an active comparator, or within-subject comparison to baseline. Outcomes: Quantitative assessment of neuropathic pain (e.g., visual analog scale [VAS], numerical rating scale, neuropathic pain scale). Timing: No time limits were set. Study design: RCTs or controlled clinical trials. Language: English.
Exclusion criteria were as follows:
Animal or in vitro studies. Observational designs without a controlled comparator (e.g., case reports, case series, uncontrolled cohorts). Studies in which the neuropathy was not attributable to diabetes or where diabetic neuropathy outcomes could not be analyzed separately.
The focus on RCTs and controlled clinical trials was selected because they provide the highest level of evidence for assessing treatment efficacy.
Study selection, data extraction, and risk of bias assessment
The search identified 15,377 records. After removal of duplicates, 6,460 records were screened by title and abstract for potential eligibility (Fig. 1). Thirty-five full-text articles were retrieved and assessed for inclusion. Two reviewers independently screened titles/abstracts and full texts. Discrepancies were resolved by discussion and, when needed, by consultation with a third reviewer until consensus was reached.
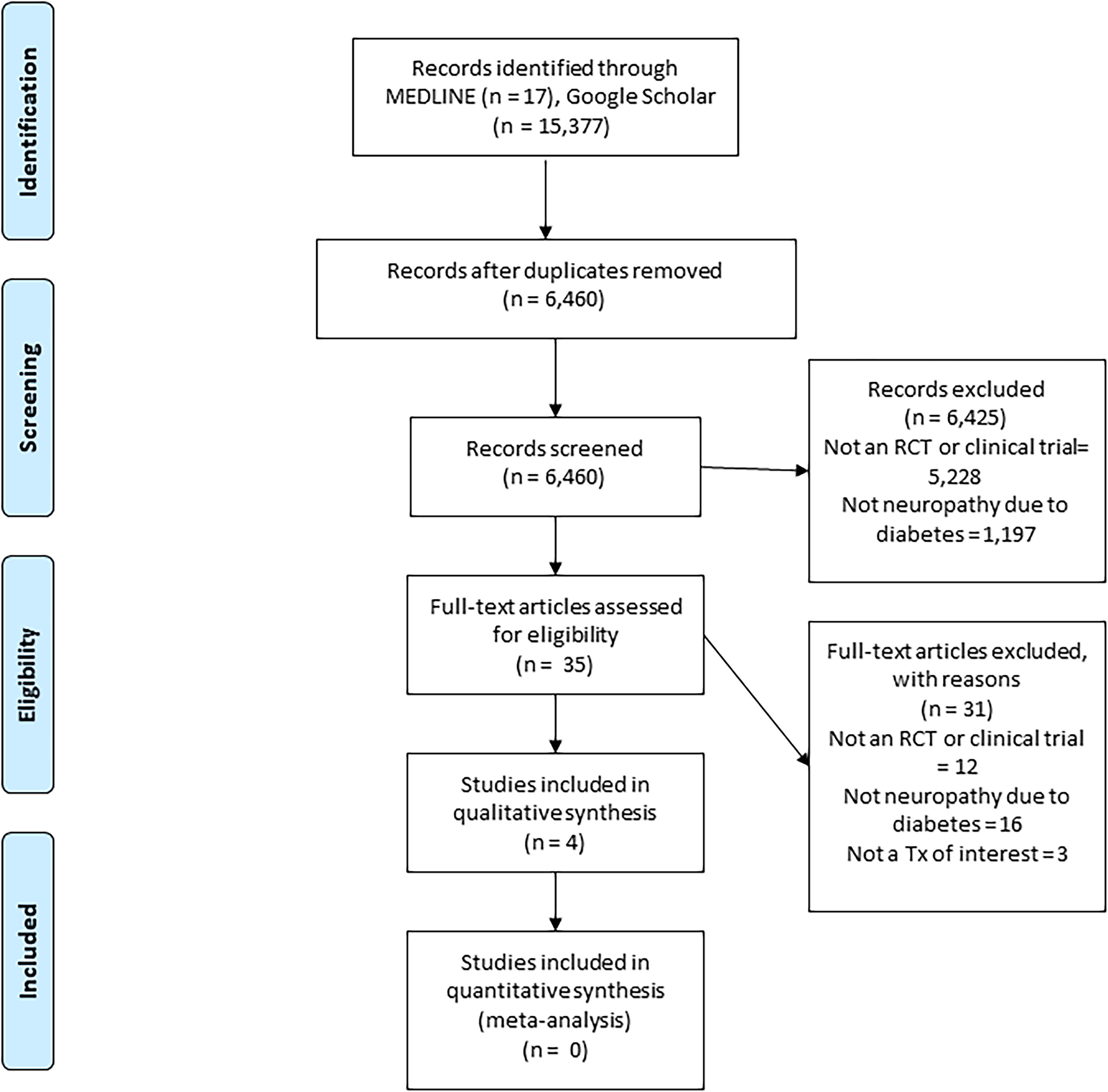
PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analyses; RCT, randomized controlled trial; Tx, treatment.
Four studies met the inclusion criteria and were included in the qualitative synthesis (Table 1). One additional trial was identified on ClinicalTrials.gov that would have met criteria; because results were never published, it was not included in this review. 18
Description of the Studies
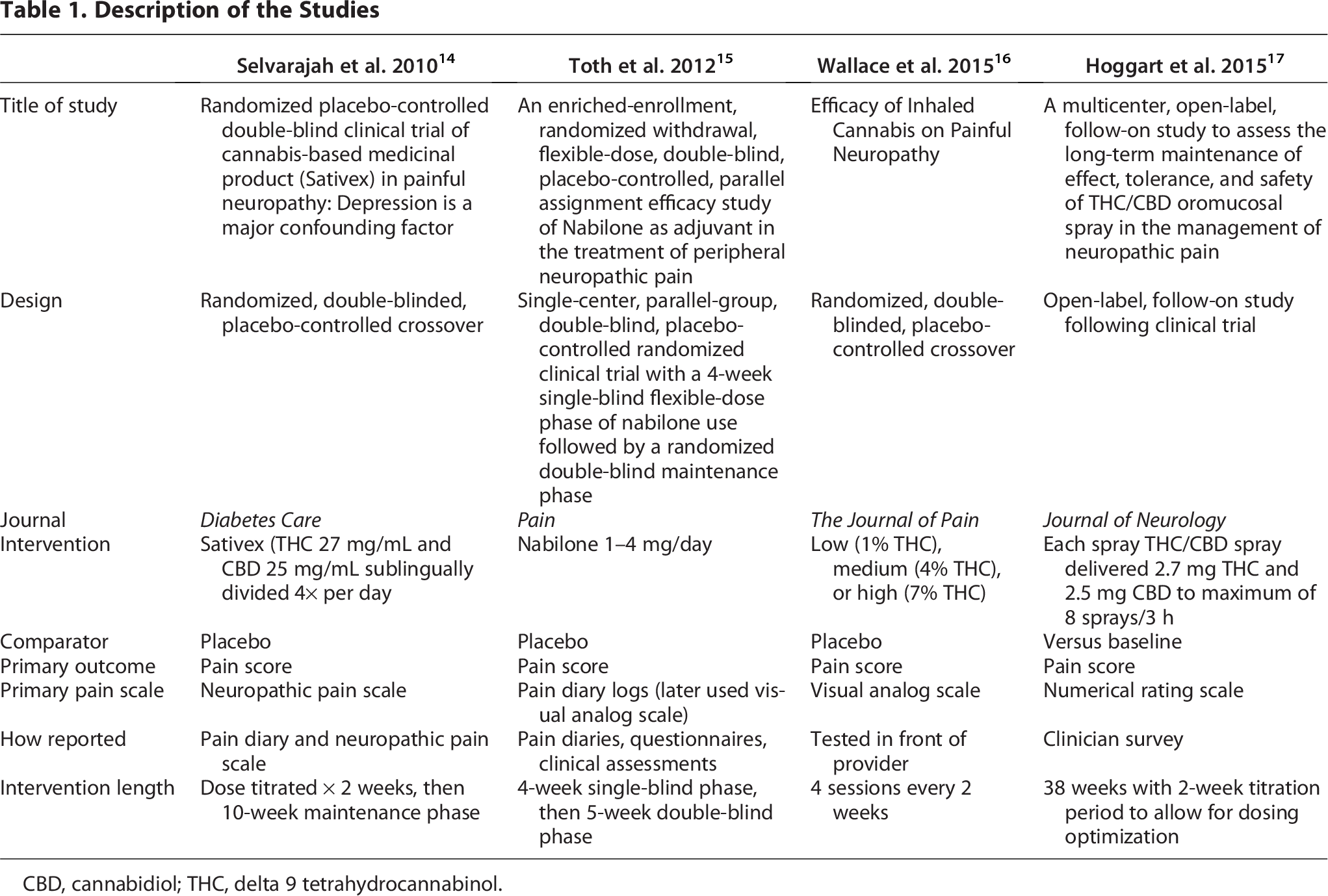
CBD, cannabidiol; THC, delta 9 tetrahydrocannabinol.
A standardized data extraction form was used to collect information on study characteristics (country, setting, design, sample size), participant characteristics (age, diabetes type and duration, neuropathy characteristics), intervention details (formulation, route, dosing, titration schedule), comparator, duration of follow-up, outcome measures, and efficacy and safety results. Data were extracted independently by two reviewers, with disagreements resolved by consensus.
Risk of bias for each included RCT was assessed using the Cochrane Risk of Bias 2.0 tool, evaluating domains including randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. For the Hoggart et al. study, a narrative assessment was done due to it being nonrandomized with high risk of bias for efficacy. Risk of bias judgments are summarized in Table 2.
Risk of Bias Analysis
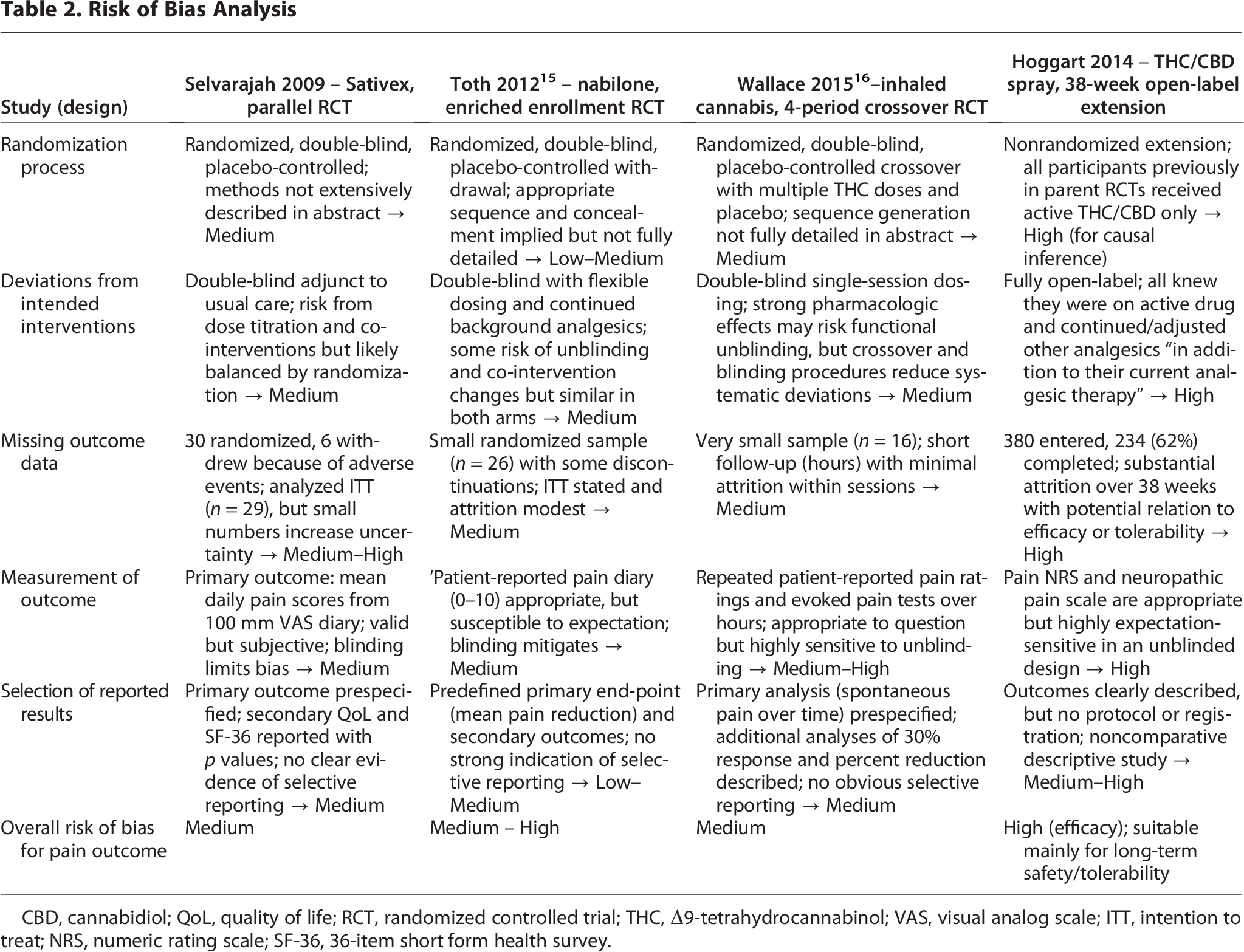
CBD, cannabidiol; QoL, quality of life; RCT, randomized controlled trial; THC, Δ9-tetrahydrocannabinol; VAS, visual analog scale; ITT, intention to treat; NRS, numeric rating scale; SF-36, 36-item short form health survey.
Due to substantial clinical and methodological heterogeneity across the four included studies—particularly differences in cannabinoid formulation, dosing, routes of administration, comparators, and outcome measures—and the small number of trials, the research team determined that a quantitative synthesis (meta-analysis) would not be appropriate. Therefore, a narrative synthesis was conducted.
Study characteristics
Four clinical trials evaluated medical cannabis or cannabinoid-based therapies for the treatment of peripheral neuropathy specifically in participants with diabetes.14–17 Publication years ranged from 2010 to 2015. Journal impact factors ranged from 4.6 to 16.2 at the time of publication.
Three studies were randomized, double-blind, placebo-controlled trials, two of which used a crossover design. One study used an open-label design as a follow-up to an unpublished RCT listed on ClinicalTrials.gov One trial was conducted in the United States, one in the United Kingdom, and one in Canada.14–16 The multicenter trial by Hoggart et al. was conducted in the United Kingdom, Czech Republic, Romania, Belgium, and Canada.
All studies used pain intensity as the primary outcome (Table 1). Two used VAS, one used a numerical rating scale, and one used a neuropathic pain scale with a broader scoring range. Two studies required participants to maintain pain diaries.14,15 Three studies included a placebo comparator group, whereas one compared pain scores to baseline. Study durations ranged from less than 10 weeks to 38 weeks, with the longest study incorporating a 2-week titration period.
Interventions varied widely. One study used inhaled (vaporized) THC at low, medium, and high concentrations (1%, 4%, and 7% THC, respectively). Two studies used nabiximols (a 1:1 THC:CBD oromucosal spray).14,17 One study compared three fixed doses of nabilone (1 mg/day, 2 mg/day, and 4 mg/day after titration) with placebo. Concomitant analgesic medications for peripheral neuropathy were permitted in all studies; only Hoggart et al. systematically recorded concomitant analgesic use and dosing, with anticonvulsants, tricyclic antidepressants, opioids, and nonsteroidal anti-inflammatory drugs being most common.
Data and resource availability
The datasets generated and analyzed during the current systematic review are available from the corresponding author upon reasonable request.
Results
Participants and demographics
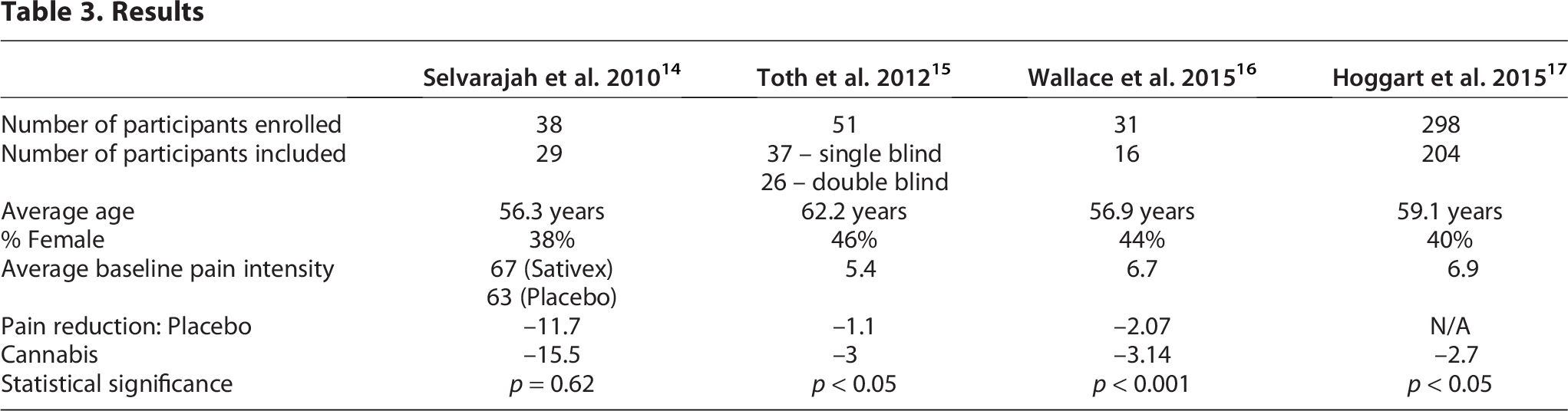
Across the four included trials, 416 participants were enrolled, and 275 completed the studies (Table 3). Hoggart et al. enrolled the largest sample but also had the highest withdrawal rate (31.5%). Mean age at enrollment ranged from 56.3 to 62.2 years. Most participants were male, with proportions ranging from 54% to 62%.
Results
Pain reduction
Three of the four studies reported statistically significant reductions in neuropathic pain with cannabinoid-based interventions compared with placebo or baseline (p < 0.05), whereas Selvarajah et al. did not observe a significant treatment effect. In post hoc analyses, Selvarajah et al. suggested that comorbid depression and an unexpectedly large placebo response may have contributed to the lack of between-group differences: participants with depression in both the 1:1 THC:CBD and placebo groups had higher baseline neuropathic pain scale scores and exhibited greater pain reduction than those without depression, and the placebo group overall improved more than anticipated.
In the Toth et al. trial, all three nabilone dose groups (1 mg/day, 2 mg/day, and 4 mg/day) achieved at least a 30% reduction in pain scores versus placebo. Analgesic effects favoring nabilone were evident at week 6 and were maintained through week 9. Notably, all participants randomized to the highest dose (4 mg/day) achieved ≥30% pain reduction compared with placebo.
Wallace et al. evaluated inhaled (vaporized) THC and found that the 4% THC concentration significantly reduced pain scores compared with placebo, whereas the 1% concentration did not differ from placebo, and the 7% concentration was associated with higher pain scores than placebo. These findings are consistent with a potential U-shaped dose–response relationship for vaporized THC, in which higher doses do not confer additional benefit and may worsen pain.
Hoggart et al., the largest and longest trial, investigated a 1:1 THC:CBD oromucosal spray. Participants experienced a reduction in numerical rating scale pain scores from baseline after the first month, which was maintained over the 10-month study. There was no evidence of tolerance: the mean daily dose remained stable at approximately 6.6 sprays/day, despite a protocol-defined maximum of 8 sprays every 3 h (24 sprays/day). Concomitant analgesic use (number of agents and dosing regimens) did not increase over the course of the study.
Adverse effects
Adverse effects were reported in three of the four trials (Wallace et al., Toth et al., and Hoggart et al.). In Wallace et al., impaired performance on two of three neuropsychological tests was observed in the high-dose (7%) vaporized THC group. All participants in the 7% THC group reported euphoria, although 60% of participants receiving placebo also reported euphoria. Somnolence was also more frequent with 7% THC than with placebo.
Selvarajah et al. did not provide detailed adverse event data, reporting only that six participants withdrew due to adverse effects.
In Toth et al., commonly reported mild-to-moderate adverse effects with nabilone included dizziness, dry mouth, confusion or impaired memory, lethargy, drowsiness, euphoria, headache, and increased appetite. Two participants discontinued because of intolerable confusion.
In Hoggart et al., a large proportion of participants reported at least one adverse event, most frequently dizziness, nausea, dry mouth, dysgeusia, fatigue, somnolence, and feeling drunk. Among the 31.5% of participants who withdrew from the study, 23% of withdrawals were attributed to adverse effects.
Discussion and Clinical Implications
In comparison with other qualifying conditions for medical cannabis, the majority of evidence for its use in patients with chronic and neuropathic pain is significant.9,19 Pain presentation and management can differ widely due to etiology and underlying pathology. Thus, a systematic review, including only RCTs and controlled clinical trials with participants who experience peripheral neuropathy solely due to diabetes, is relevant and unique to the literature. Of the four published studies herein, three of them had significant improvement in pain scales that should be discussed in context with existing neuropathic pain reviews and future research implications.
Multiple systematic reviews and meta-analyses across mixed neuropathic etiologies (HIV, multiple sclerosis [MS], spinal cord injury, postherpetic neuralgia, chemotherapy-induced neuropathy, diabetic neuropathy, etc.) generally find that cannabis-based medicines provide, at best, modest analgesia with low-moderate quality evidence and frequent adverse effects. For example, a Cochrane review (16 RCTs, 1750 participants) concluded that cannabis-based medicines may increase the proportion achieving ≥30% pain relief (number needed to treat [NNT] ≈ 11), but with very-low to moderate-quality evidence and substantially increased nervous system and psychiatric adverse events. 11 Other meta-analyses and recent systematic reviews similarly report small effect sizes (standardized mean difference around −0.2 to −0.3 or mean differences ≈ 6–9 points on a 0–100 scale) and highlight small samples, short duration, heterogeneous products/routes, and high placebo responses.20,21 An individual patient-data meta-analysis of five inhaled-cannabis RCTs in chronic neuropathic pain estimated an NNT of 5–6 for ≥30% pain relief, but emphasized the very short follow-up (days to weeks) and similar limitations as other meta-analyses already described. 22 Within this context, our findings that only four small RCTs/controlled trials exist specifically for painful diabetic peripheral neuropathy, with three showing statistically significant pain reduction, fit this broader pattern: a suggestion of benefit, but on a heterogeneous evidence base. Our focus on study participants only including those with diabetic peripheral neuropathy is novel, but still a narrow slice of an uncertain field.
There is a patient preference toward inhalation delivery (including vaporized) of medical cannabis. 23 According to the American Lung Association, smoking cannabis cigarettes can damage the lungs with chronic cough and acute bronchitis. 24 It is known that people with diabetes who smoke traditional cigarettes have an increased risk for microvascular and macrovascular complications, including increased mortality. 25 Thus, using cigarettes would not be an optimal delivery method for medical cannabis, especially for those with diabetes or reactive airway diseases (e.g., asthma or chronic obstructive pulmonary disease). Little is known, however, regarding the harms of inhalation in an electronic vaporized form, such as in the Wallace et al. study. Vaporization of medical cannabis without the carcinogens found in traditional smoking appears to be a useful delivery method for research.
Selvarajah et al. was the only study without a significant primary outcome for pain in the available literature. 14 Depression was the main confounding factor, which is also consistent with other literature. Diabetes and depression have a bidirectional link and should be treated concomitantly. Treatment of depression can lead to better diabetes outcomes, and treatment of diabetes can alleviate depressive symptoms. 26 Likewise, a possible bidirectional relationship may exist between depression and neuropathy in patients with diabetes. 27 For future studies examining the effect of medical cannabis on peripheral neuropathy in patients with diabetes, it would be feasible to use depression as an exclusion criterion or include antidepressive pharmacotherapy in the methodology.
Clinically meaningful pain reduction is widely recognized as at least a reduction of 2 points on a 0–10 numerical pain scale. 28 A VAS was used in the Wallace et al. and Toth et al. studies, and a numerical rating scale was used in the Hoggart et al. study. At least a 30% reduction or greater in pain intensity is also considered clinically meaningful. While the Hoggart et al. study showed at least a 2-point reduction in pain versus baseline, the Toth et al. study found at least a 30% or better reduction of pain intensity with nabilone versus placebo.15,17 As stated in the Results section, the highest dose regimen (i.e., 4 mg/day) of nabilone achieved at least 30% pain reduction in 100% of the participants in this dosing arm. Overall, this was achieved in 85% of participants in the entire study. 17 Nabilone, at least in the United States, is more expensive than another synthetic THC that is approved by FDA—dronabinol (Marinol®). Nabilone is only available in its brand form, Cesamet®, in the United States. From a practical standpoint, it is unknown as to whether the results of this study could be extrapolated for use of dronabinol. Therefore, using dronabinol as a treatment arm in future studies would be feasible. Also, clinicians who are not as accustomed to recommending medical cannabis may be more amenable to prescribing an FDA-approved medication for an off-label use.
The possible U-shaped dose–response curve, also known as a biphasic effect, found in the Wallace et al. study has interesting implications. The authors of that study state that the placebo, 1%, 4%, and 7% THC yielded 0 mg, 4 mg, 16 mg, and 28 mg, respectively, as per dosing session. 16 This seems to indicate that while 16 mg may have been effective for neuropathic pain relief versus placebo, higher dose regimens (i.e., 28 mg) may cause increased neuropathic pain. This is consistent with findings in the literature regarding biphasic effects, where a lower dose of a medical cannabis formulation is effective, whereas a higher dose produces adverse effects and/or opposite of the intended effect. Such biphasic effects have been found with medical cannabis for pain and anxiety.29–31
Compared with FDA-approved agents for diabetic peripheral neuropathy (duloxetine, pregabalin, tapentadol), the limited RCT data suggest that dropout from adverse effects with cannabinoid therapies is generally in the same range or lower, but based on much smaller samples and shorter exposure. Longer and larger RCTs of standardized medications for diabetic peripheral neuropathy typically show adverse-event–related discontinuation in the ∼10–20% range, with much higher overall adverse effect rates than reported in these small cannabinoid studies. Clinically, this suggests that cannabinoids do not cause more adverse effect-related dropout than standard agents and in some contexts may cause less, but the evidence base is weak.
At 40 weeks duration, Hoggart et al. exhibited the design most likely to demonstrate long-term efficacy for peripheral neuropathy. 17 Significant improvement in pain for a 1:1 THC:CBD was demonstrated versus baseline at 1 month, and this was maintained for the remainder of the study. Maintaining effective pain relief without increasing doses suggests that the participants did not develop tolerance, as per the study authors. As stated in the Results, they also tracked concomitant analgesics and found no increased dose regimens or increase in number of analgesics. This also reinforces that the study agent led to no increased need for adjunct pain relief.
Neuropathic pain reviews emphasize that optimal THC dosing remains unresolved, citing: small, short RCTs; divergent formulations and delivery routes; variable titration schemes; and substantial between-study heterogeneity.20,21 However, an analysis of the Hoggart et al. and Wallace et al. studies regarding effective dosing leads to an interesting finding. While the Hoggart et al. study protocol allowed 8 sprays every 3 h, the authors stated that participants who had reduced pain scores maintained an average of 6.6 sprays per day during the final treatment month. Of note, this would be approximately 18 mg THC per day, which is similar to the effective dose in the Wallace et al. study. This leads to a hypothesis-generating range, but should be tempered as suggestions from two small diabetic peripheral neuropathy trials. Taken together, the Hoggart et al. and Wallace et al. studies suggest a potential therapeutic window in the range of approximately 16–18 mg THC per day for diabetic peripheral neuropathy. However, this dosing range should be considered preliminary and requires confirmation in larger, longer, head-to-head studies that systematically explore possible dose–response curves.
Limitations
Conducting a meta-analysis for studies using medical cannabis solely in participants with diabetes experiencing peripheral neuropathy would have been optimal; however, heterogeneity and number of patients limited the quantitative analysis that a meta-analysis could provide. Standardized THC products are inconsistent across different studies; strains and batches can vary with a wide range of cannabinoid concentrations. There has been a lack of knowledge regarding appropriate dose regimens to use, including routes of administration. 32 Three of the four studies used commercially available products (i.e., nabiximols and nabilone). The authors of the four studies suggested other limitations, such as difficulty in blinding due to the psychoactive properties of THC-containing products. Particularly, studies with crossover designs (i.e., Toth et al. and Wallace et al.) could suffer from this limitation. Although Hoggart et al. was the longest study, it compared outcomes versus baseline rather than versus placebo. None of the studies included a treatment group consisting of traditional therapies for peripheral neuropathy. While all studies included concomitant treatments, only Hoggart et al. reported medication specifics. All of the studies used pain scores as the outcome; functional improvement would also be a relevant outcome. These limitations mirror those highlighted in broader neuropathic pain reviews, which also conclude that the overall evidence for cannabis-based medicines is of low-to-moderate quality, with modest average effect sizes and uncertain generalizability across neuropathic subtypes.20,21
Conclusions
This systematic review summarizes randomized and RCTs that enrolled only participants with painful peripheral neuropathy due to diabetes and evaluated medical cannabis or nationally approved cannabis-based medicines. Within this narrowly defined population, three of four identified studies demonstrated statistically significant reductions in pain compared with placebo or baseline, suggesting that cannabinoid-based interventions may offer analgesic benefit for some patients with diabetic peripheral neuropathy. However, these findings must be interpreted in the context of a small number of heterogeneous, generally short-duration trials, consistent with broader neuropathic-pain reviews that describe only modest average benefits and low-to-moderate quality evidence for cannabis-based medicines overall.
Due to the fact that the most recent RCT was published in 2015, newer studies are urgently needed. Future RCTs restricted to participants with painful diabetic peripheral neuropathy should be adequately powered, of at least 12 months’ duration, and include both an optimized traditional pharmacologic comparator and a placebo group. Trials should also use standardized products with clearly defined cannabinoid content, systematically explore dose–response relationships, and incorporate functional and patient-centered outcomes, in addition to pain scores. Such studies would also most likely not have as much possible bias as was determined in the currently discussed RCTs.
In two of the reviewed studies, a preliminary signal emerged that intermediate THC exposure may be associated with analgesic benefit. In one study, a vaporized 4% THC condition (approximately 16 mg per session) improved pain relative to placebo, whereas a higher 7% condition (approximately 28 mg) worsened pain. In the other study, a 1:1 THC:CBD oromucosal spray produced sustained benefit at an average daily use approximating 18 mg THC without evidence of dose escalation. On this basis, THC exposure in the range of roughly 16–18 mg, delivered via vaporized or sublingual/oromucosal routes, should be viewed as a hypothesis-generating therapeutic window rather than a definitive dosing recommendation and requires confirmation in larger, long-term dose-finding trials.
Overall, this review may assist clinicians and researchers by (1) delineating the limited RCT evidence specific to painful diabetic peripheral neuropathy, (2) highlighting promising formulations and routes of administration, and (3) outlining plausible, but as yet unconfirmed, target dose ranges. Given the modest and uncertain benefits, frequent adverse effects, and substantial gaps in the evidence base, cannabis-based medicines for painful diabetic neuropathy should currently be considered only as experimental or adjunctive options, ideally within research settings or carefully monitored clinical practice.
Authors’ Contributions
J.J.S. researched data, contributed to discussion, and wrote the first draft of the article. D.M.R. reviewed and edited the article and contributed to all discussions. All the authors approved the final version of this article.
Footnotes
Acknowledgments
The authors would like to thank Dr. William Baker, faculty at the University of Connecticut, who provided helpful discussions regarding the potential for a meta-analysis versus a systematic review for these data. Also, the authors would like to thank Isaiah Brown, 4th year pharmacy student with the University of Mississippi, for his assistance in procuring data for this project.
Author Disclosure Statement
The authors have nothing to disclose that would serve as a conflict of interest relevant to this systematic review.
Funding Information
The authors have received no funding for this research.
Prior Presentation
Part of the data from this article was presented at the Association of Diabetes Care and Education Specialists Annual Conference, August 11, 2024.