
Abstract
Background:
Fibromyalgia (FM) is a chronic pain condition characterized by widespread pain, fatigue, and functional impairment. Current pharmacological treatments show limited efficacy and poor tolerability. Cannabidiol (CBD) has demonstrated analgesic and anti-inflammatory properties, but evidence regarding CBD-containing topical formulations in FM remains scarce.
Objectives:
To evaluate the feasibility, safety, and preliminary efficacy of a CBD-containing topical formulation for localized pain in patients with FM and to explore its potential impact on broader symptom domains.
Material and Methods:
This single-arm pilot study included 30 women with FM and clinically relevant localized pain due to musculoskeletal, neuropathic, or cutaneous comorbidities. Participants self-applied a commercially available CBD-containing topical formulation to a painful area every 8 h for 12 weeks. Outcomes were assessed at baseline, 4 weeks, and 12 weeks. Nonparametric repeated-measures analyses, Monte Carlo resampling, effect sizes, and minimal clinically important difference (MCID) thresholds were applied.
Results:
At the 4- and 12-week follow-up visits, all participants reported full adherence to the prescribed application schedule. No adverse events or side effects were reported. Localized pain showed a significant and clinically meaningful reduction at 4 weeks, sustained at 12 weeks (60% achieving MCID). Functional capacity improved significantly, with 50% of participants exceeding the MCID at 4 weeks. Widespread Pain Index (WPI) and Symptom Severity Scale (SSS) scores decreased progressively, and a lower proportion of participants met the 2010 American College of Rheumatology (ACR) diagnostic criteria for FM at 12 weeks, while generalized pain, fatigue, anxiety, and depression did not show significant changes.
Conclusions:
Topical application of a CBD-containing formulation was feasible and was associated with improvements in localized pain and functionality in this exploratory single-arm study. Changes observed in WPI and SSS, and in the proportion of participants meeting the 2010 ACR criteria at follow-up, should be interpreted cautiously and considered exploratory and hypothesis-generating, given the uncontrolled design (precluding causal inference), the symptom-based and fluctuating nature of FM, and the multicomponent composition of the product. Although limited by its uncontrolled design, this pilot study provides effect size estimates and methodological guidance to support future randomized controlled trials of topical cannabinoids in FM.
Keywords
Introduction
Fibromyalgia (FM) is a chronic disorder mainly characterized by widespread musculoskeletal pain and substantial functional burden. Despite advances in understanding its pathophysiology, effective pain management remains challenging. Current treatments often show limited efficacy and poor tolerability, 1 prompting patients’ interest in alternative approaches. 2 Oral cannabinoids have gained attention for pain modulation, although results remain mixed.3,4 Evidence has been reported in neuropathic, inflammatory, cancer-related, and postoperative pain conditions.5–9 Cannabidiol (CBD), a nonpsychotropic component of Cannabis sativa, has emerged as a promising option because of its analgesic and anti-inflammatory properties. 10
Peripheral sensitization has been implicated in FM pain, with increased excitability and reduced activation thresholds in nociceptive fibers. 11 This process involves the release of inflammatory mediators and changes in peripheral sensory receptors, perpetuating localized hyperalgesia. Addressing peripheral inflammation and nociceptor activation to reduce peripheral sensitization might influence pain perception, although its impact on generalized symptoms remains uncertain.12,13 CBD is postulated to modulate peripheral sensitization through anti-inflammatory effects and receptor interactions relevant to pain transmission. 14 However, FM is a symptom-based syndrome with fluctuating pain distribution and symptom burden, so interventions targeting localized pain may not necessarily translate into changes in overall clinical status.
Concerns about adverse effects may limit acceptance of cannabis-based therapies for chronic pain.15,16 Topical administration of CBD-containing formulations might allow localized treatment with lower systemic exposure and side effects.17,18 Clinical studies suggest potential benefit in recurrent aphthous ulcers, 19 orofacial myofascial pain, 20 and thumb basal joint arthritis. 21 However, evidence regarding cannabinoids in FM remains limited and inconclusive,22–24 and studies specifically evaluating CBD-containing topical formulations in this population are scarce.
Recognizing the unmet need for new FM pain treatments and the scarcity of data on CBD-containing topical formulations, we designed a pilot study to evaluate such a formulation for localized and generalized pain in FM. The study was intended to inform future randomized clinical trials by generating preliminary data on feasibility, acceptability, safety, and effect sizes, while identifying logistical issues relevant to protocol optimization. 25 We anticipated that it would be feasible, safe, and well accepted, with meaningful effects on localized pain, while potential effects on generalized pain remained uncertain.
Materials and Methods
Participants
This study included 30 participants (consistent with recommendations for pilot studies assessing feasibility and study design 26 ) referred to the Interdisciplinary Primary Chronic Pain Unit of the Hospital Clinic of Barcelona for specialized evaluation of suspected FM.
The study was approved by the Research Ethics Committee of the Hospital Clinic of Barcelona; approval number HCB/2023/0622. The study was conducted in compliance with the Declaration of Helsinki (Fortaleza, Brazil, October 2013) and in accordance with the legal requirements of the Spanish Law 14/2007 of July 3 on biomedical research. All patients signed a written informed consent before entering the study.
To ensure the reliability and validity of the study outcomes while safeguarding participant safety, participants were eligible for inclusion if they met the following criteria:
Aged 18 years or older. Confirmation by the Unit’s Rheumatologists of suspected FM diagnosis following the diagnostic criteria established by the American College of Rheumatology (ACR).27,28 Meet diagnostic criteria for at least one comorbidity causing localized pain of musculoskeletal, neuropathic, or cutaneous origin (e.g., scar tissue). Scored ≥4 on a 0–10 cm Visual Analog Scale (VAS) for both generalized pain and fatigue. Scored ≥4 on the VAS for localized pain secondary to comorbidity. No initiation or dose changes of psychotropic drugs or opioid analgesics during the four weeks prior to study entry (paracetamol, tramadol, nonsteroidal anti-inflammatory drugs, and metamizole were permitted if maintained on a stable regimen).
Participants were excluded if they met any of the following conditions:
Presence of psychiatric conditions that could interfere with the reliability of self-reported outcomes or require immediate clinical attention. This included, but was not limited to, dementia, severe suicide risk, unstable schizophrenia, other psychotic or bipolar disorders, severe personality disorders, or active drug dependence or abuse. Use of other topical products that might confuse results, such as topical lidocaine or capsaicin creams. Participation in, or planned participation in, another clinical trial during this study. Patients actively applying for disability status.
Procedure
The intervention consisted of a commercially available CBD-containing multicomponent topical formulation (BlissCBD® Cream;
For study purposes, each participant was categorized according to one index localized pain region, classified into a single anatomical region, and the intervention focused on that index painful site.
Patients were assessed before starting treatment and at 4 and 12 weeks using the following standardized evaluation protocol:
Pain and fatigue
Generalized pain, localized pain, and fatigue intensities were assessed separately using 10-cm VASs. Widespread pain was quantified using the Widespread Pain Index (WPI), and symptom severity was assessed using the Symptom Severity Scale (SSS). 27
Clinical Global Impression scale
The Clinical Global Impression (CGI) scale was used to assess the improvement of the condition over time in response to treatment according to the investigator’s impression. 29
Patient Global Impression of Change
The Patient Global Impression of Change (PGIC) scale was used as an indicator of meaningful change after treatment from patients’ point of view.
Both the PGIC and the CGI assess the change in health on a six-point symmetrical scale ranging from 1 = Very much improved to 6 = Very much worse. 30
Functional capacity
Functional capacity was evaluated using the 10-item Spanish version of the FM Impact Questionnaire (s-FIQ). 31 The s-FIQ assesses the extent to which FM interferes with the patient’s functional capacity over the preceding week.
Emotional distress
Emotional distress was assessed using the 14-item Hospital Anxiety and Depression Scale (HADS). 32 The HADS evaluates symptoms of anxiety and depression while minimizing contamination from somatic symptoms, which is a limitation of other psychopathology questionnaires. 33
Adverse events and adherence
Participants were provided with a symptom diary to record skin changes and any other noted adverse events or side effects; diaries were reviewed at the 4- and 12-week follow-up visits. Adherence was assessed at the same visits by open questioning regarding whether the formulation had been applied according to the prescribed schedule.
Statistical analyses
Descriptive analyses were conducted by calculating the mean and standard deviation for quantitative variables, and frequency and percentage for qualitative variables. Comparisons of the outcome variable means across the three time points were performed using nonparametric tests for repeated measures, specifically the Friedman test or the Wilcoxon signed-rank test, as appropriate. Given the single-arm design and the sample size, the observation of significant differences was reanalyzed using the Monte Carlo repeated random sampling method (99% confidence level, sample size = 1000). This approach enables a more robust empirical estimation of the distribution of the mean difference, the standard error, and the confidence intervals, thereby enhancing the reliability of the results in contexts where normality or homoscedasticity cannot be fully assured. In addition, effect sizes were calculated, and the number of participants who achieved a minimal clinically important difference (MCID) by the end of the study was determined for those variables for which an MCID has been established.
Given the exploratory nature of this pilot study, no correction for multiple comparisons was applied. Therefore, the results should be interpreted with caution, particularly with respect to the risk of type I error.
Results
Thirty-one patients were invited to participate, and all agreed. One patient was lost before the first follow-up, and two additional participants were lost before week 12; thus, 30 initiated the intervention, and 28 completed the study.
All participants were female, with a mean age of 54 years and a mean generalized pain duration of 17 years. Localized pain was evenly distributed across anatomical regions. Most were receiving pharmacological treatment, mainly antidepressants and analgesics, and two-thirds had a diagnosed psychiatric disorder, predominantly adjustment disorders associated with persistent somatic symptoms and disability (Table 1).
Demographic and Clinical Variables
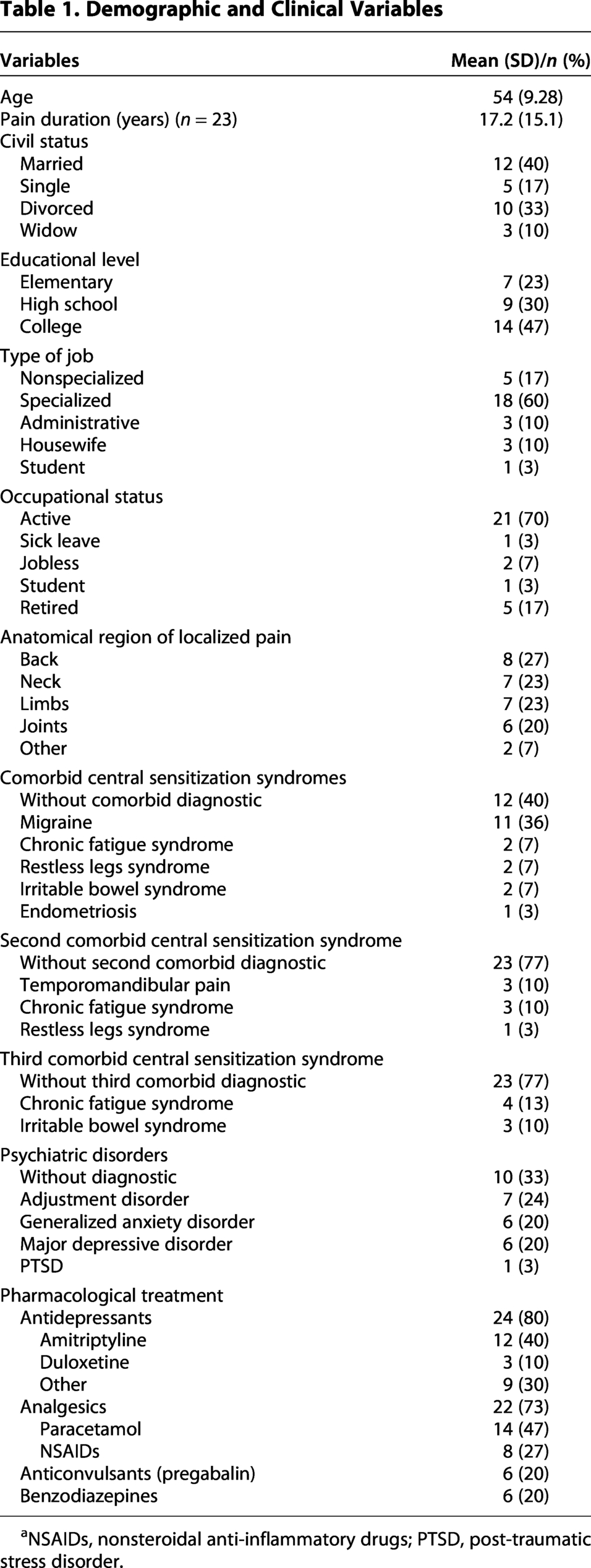
NSAIDs, nonsteroidal anti-inflammatory drugs; PTSD, post-traumatic stress disorder.
Clinical Change after 12 Weeks of BlissCBD Self-Application
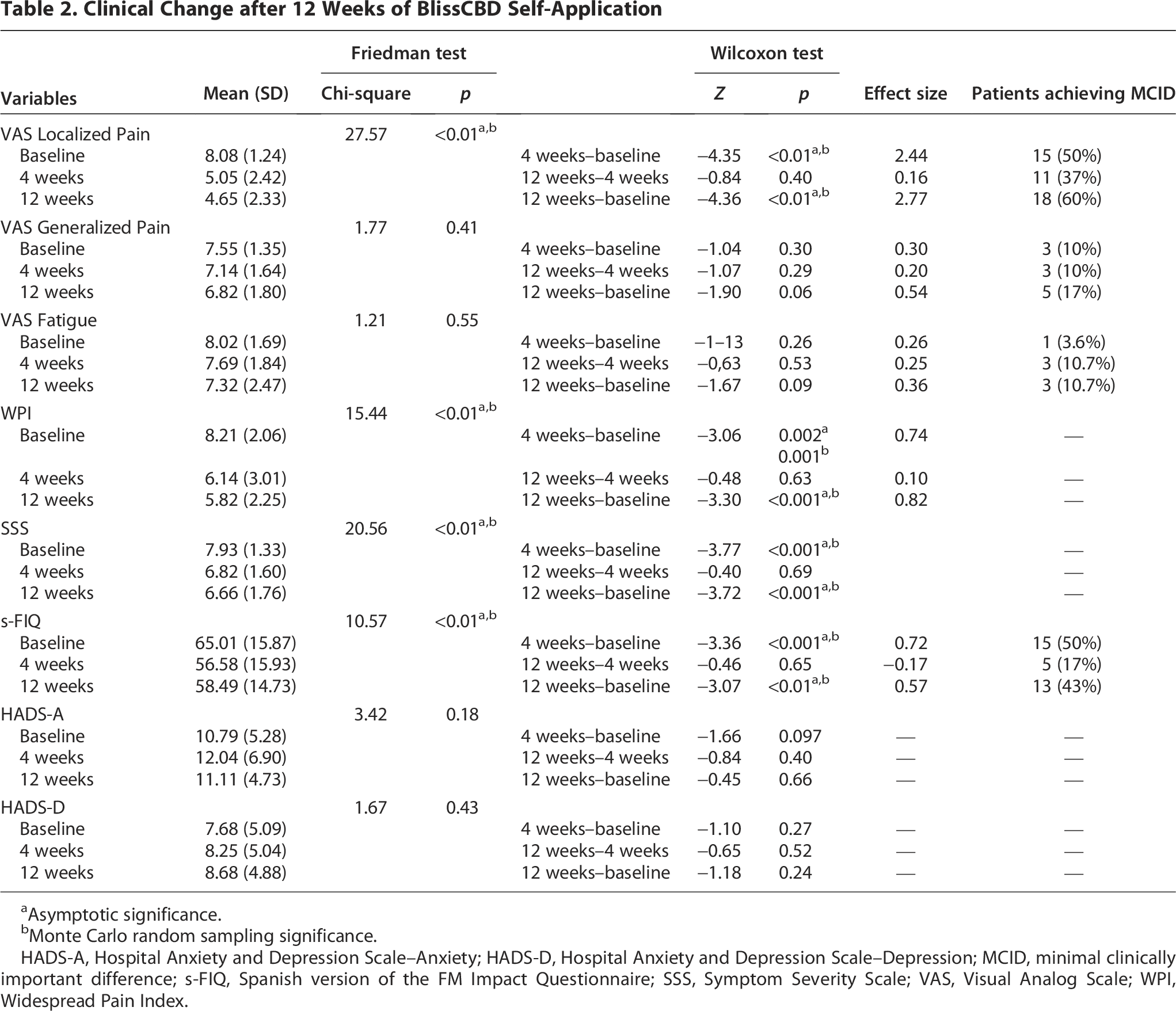
Asymptotic significance.
Monte Carlo random sampling significance.
HADS-A, Hospital Anxiety and Depression Scale–Anxiety; HADS-D, Hospital Anxiety and Depression Scale–Depression; MCID, minimal clinically important difference; s-FIQ, Spanish version of the FM Impact Questionnaire; SSS, Symptom Severity Scale; VAS, Visual Analog Scale; WPI, Widespread Pain Index.
At both follow-up visits, all participants self-reported full adherence to the prescribed schedule, and no adverse events or side effects were reported.
After 12 weeks of self-application of the formulation every 8 h, several variables changed (Table 2). Localized pain improved at 4 weeks with a large effect size, with no further improvement at 12 weeks. Monte Carlo random sampling confirmed the statistical significance of these differences, enhancing confidence in interpreting the follow-up changes as meaningful. At the end of the study, 60% of patients reported an improvement exceeding the 30% threshold established as the MCID. 34
Neither generalized pain nor fatigue showed significant improvement at any follow-up. However, both the WPI and the SSS improved progressively at 4 and 12 weeks. At 4 weeks, 10 patients (33.3%) no longer met the 2010 ACR diagnostic criteria for FM (WPI ≥7 and SSS ≥5, or WPI 3–6 and SSS ≥9). 27 By 12 weeks, an additional 7 (23.3%) no longer met criteria, whereas 3 relapsed.
At 4 weeks, 60% of participants reported improvement on the PGIC, increasing to 71% at 12 weeks. Clinician ratings on the CGI indicated improvement in 97% and 93% of participants at 4 and 12 weeks, respectively.
The interference of FM with the participants’ functional capacity according to the sFIQ improved at 4 weeks, with 15 patients (50%) showing a reduction exceeding the 14% threshold for the MCID. 35 Results were sustained at the 12-week follow-up, with nonsignificant changes between weeks 4 and 12.
Despite improvements in localized pain and functional capacity, neither anxiety nor depression improved at any follow-up.
Discussion
This pilot study explored the feasibility, safety, and preliminary clinical signal of a CBD-containing multicomponent topical formulation in patients with FM and localized comorbid pain. Over 12 weeks, its use was associated with improvements in localized pain, WPI, SSS, and functional capacity, with no reported adverse events. These findings suggest that such a formulation may be a feasible and well-tolerated approach for localized comorbid pain in FM.
Potential mechanisms underlying the effects of CBD remain incompletely understood. Pre-clinical and experimental studies suggest that CBD may interact with multiple targets involved in nociception and inflammation, including transient receptor potential vanilloid 1 channels, modulation of pro-inflammatory cytokines, and components of the endocannabinoid system. 14 However, the present study was not designed to investigate mechanistic pathways, and no causal inferences can be drawn.
CBD-containing multicomponent topical formulations remain relatively underexplored compared with oral or inhaled routes. Emerging evidence suggests potential benefits in peripheral neuropathy and thumb basal joint arthritis, with more heterogeneous evidence in orofacial pain conditions.18,20,21 Our findings are consistent with these reports and suggest that similar approaches might be feasible in FM, a condition involving both central and peripheral pain components. Self-reported adherence and the absence of reported adverse events support the short-term practicality and acceptability of this formulation; however, confirmation in controlled studies with more rigorous monitoring of adherence and adverse events remains necessary.
Localized pain intensity showed marked improvement by week 4, which was sustained through week 12. These benefits translated into functional improvements, with half of the participants demonstrating significant reductions in s-FIQ scores that exceeded the MCID. 35 Such findings may coincide with changes in other reported outcomes. However, the present study did not include objective measures of peripheral nociception, inflammatory activity, or neurophysiological processes, and therefore, no conclusions can be drawn regarding the involvement of specific peripheral mechanisms. Although these observations may be considered in the context of models of FM pathophysiology describing interactions between peripheral and central sensitization, it is important to note that central sensitization in chronic widespread pain conditions may become self-sustaining and relatively independent of peripheral input. 12 This consideration raises further uncertainty regarding the plausibility of a predominantly peripheral pathway. Accordingly, these findings should be interpreted as hypothesis-generating rather than mechanistic evidence. 12
In this sense, the progressive decline in WPI and SSS scores over the 12 weeks of intervention might be of interest. Notably, a lower proportion of participants met the 2010 ACR diagnostic criteria for FM at the end of the study. Previous research suggests that peripheral nociceptive input may contribute to the maintenance of central sensitization and widespread pain.11,13 However, these findings should be interpreted with caution. The present data do not allow conclusions regarding effects beyond the localized site of application, and improvement in localized pain should not be interpreted as evidence of modification of the underlying FM condition. FM is a dynamic and symptom-based syndrome characterized by fluctuating pain distribution and symptom burden. Accordingly, changes in composite measures such as WPI and SSS may reflect temporary modulation of symptom expression rather than sustained modification of the underlying condition.
Despite these improvements, no statistically significant changes were observed in generalized pain or fatigue VAS scores. This apparent dissociation between outcomes may be explained by the fact that these instruments capture different dimensions of the pain experience. The WPI reflects the spatial distribution of pain, whereas the VAS assesses the perceived intensity of overall pain. Accordingly, a reduction in the number of painful regions may occur without a corresponding change in global pain intensity. Several additional interpretations are possible. Generalized pain and fatigue may be more resistant to change over short periods or may require interventions that more directly address central nervous system mechanisms. In addition, the VAS measures used may not fully capture subtle changes in symptom burden. In contrast, the WPI and SSS, as structured composite indices, may reflect variations in symptom reporting over time. Finally, psychological or lifestyle factors influencing fatigue and widespread pain may not have been impacted by the localized CBD application. This dissociation further supports that changes in WPI and SSS should not be interpreted as evidence of generalized improvement in FM.
No significant improvements were observed in anxiety or depression. This may reflect the somatic focus of the intervention, the absence of systemic CBD absorption, and the modest baseline severity of emotional symptoms in this cohort. Prior reviews of systemic cannabinoids have reported modest effects on mood and sleep,6,10 which may be less likely with topical administration.
The primary methodological limitation of this study is its single-arm, uncontrolled design. Without a control or placebo group, the possibility that observed improvements were influenced by placebo effects, regression to the mean, natural symptom fluctuations, or other nonspecific factors cannot be excluded, particularly in composite diagnostic measures. In addition, expectation bias represents a particularly relevant limitation in this context. Participants were unblinded to treatment, all outcomes were self-reported, and the study population had long-standing chronic pain, which may have been associated with heightened expectations of benefit. Furthermore, clinicians were aware of treatment allocation and were also involved in the study, limiting the independence of clinician-rated outcomes such as the CGI. Accordingly, both patient-reported and clinician-rated measures may have been influenced by expectation effects. In this context, expectation effects may more appropriately capture these influences than placebo alone. In addition, multiple outcomes were evaluated without adjustment for multiple comparisons, which increases the risk of type I error. The findings should therefore be considered exploratory and hypothesis-generating.
An additional limitation is that the intervention consisted of a CBD-containing multicomponent topical formulation rather than isolated CBD. In addition to CBD, the product included several components that may have independent soothing, counterirritant, or analgesic properties. Therefore, the observed effects cannot be attributed specifically to CBD. Future randomized controlled trials should aim to better isolate the specific contribution of CBD within topical multicomponent formulations.
Adherence was based on self-report and was not objectively verified. Likewise, adverse event ascertainment relied on participant-completed symptom diaries and review at follow-up visits, which may have underestimated minor, transient, or unrelated events. Accordingly, reporting bias cannot be excluded. The absence of reported adverse events in the present study is consistent with some human trials of CBD-containing topical formulations (e.g., randomized studies in thumb basal joint arthritis 21 ), which also reported no adverse events or no side effects. However, other topical CBD studies have reported mild local adverse effects, particularly transient skin dryness or rash. 36 Therefore, our findings should be interpreted as suggesting short-term tolerability rather than establishing the absence of adverse effects.
Despite the magnitude and consistency of the observed benefits—improvement of localized pain, WPI, and SSS scores and nonimprovement of generalized pain and fatigue—concerns about causality are valid, and future research must incorporate rigorous randomized, double-blind, placebo-controlled designs to confirm these preliminary findings. Future research should prioritize well-powered RCTs comparing topical CBD to placebo and to standard topical analgesics such as lidocaine or capsaicin. Stratification by pain phenotype, comorbidity profile, and endocannabinoid system markers may identify responders more accurately.
Consistent with methodological frameworks,25,26 this study was designed to generate preliminary effect sizes, safety and tolerability data, and information relevant to the planning of larger randomized trials.
Conclusion
This pilot study supports the feasibility and preliminary clinical signal of a CBD-containing multicomponent topical formulation for localized pain in FM. Improvements in localized pain, functional capacity, and diagnostic criteria fulfillment should be interpreted cautiously and do not demonstrate modification of the underlying FM condition. These findings support future randomized controlled trials and suggest that this approach may be a feasible adjunctive option for patients with prominent localized pain who prefer to avoid systemic medications.
Authors’ Contributions
All authors meet the International Committee of Medical Journal Editors criteria for authorship and have approved the final version of the article. Using the CRediT (Contributor Roles Taxonomy), the authors’ contributions were as follows: Conceptualization—T.L.R., A.A., X.T., and L.P.; Methodology—X.T., A.A., and T.L.R.; Investigation—T.L.R., A.A., X.T., L.P., E.H., G.O.; Data curation—X.T., E.H., and G.O.; Formal analysis—X.T.; Writing—original draft—X.T., T.L.R., and A.A.; Writing—review and editing—all authors; and Supervision—A.A. and T.L.R.
Footnotes
Consent to Participate
All patients signed a written informed consent before entering the study.
Data Availability
Data that support the findings of this study are available on reasonable request from T.L.R.
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
This study received financial support from industry sources. The funding entity had no role in the study design; data collection, analysis, or interpretation; article preparation; or the decision to submit the article for publication.