
Abstract
Background:
Photobiomodulation Valeda (PBM-Valeda) is a novel therapeutic approach for dry age-related macular degeneration (AMD). The primary objective of this short-term study was to conduct an analysis of best-corrected visual acuity (BCVA) and evaluate of biomarkers using state-of-the-art high-resolution imaging with swept-source optical coherence tomography OCT (SS-OCT) and OCT angiography (SS-OCTA) in dry AMD patients treated with PBM.
Materials and Methods:
This prospective, noncomparative, interventional case series pilot study examined the following biomarkers before and after PBM treatment: BCVA, central macular thickness (CMT), subfoveal choroidal thickness (SCT), capillary density (CD), avascular area of the superficial plexus (AASP), and avascular area of the deep plexus (AADP). All parameters were assessed at baseline and 1 week after treatment. A questionnaire (exploratory, not a validated endpoint) was carried out at the end of the treatment.
Results:
The study included 25 eyes (19 patients), predominantly in the Age-Related Eye Disease Study category II. A statistically significant change in BCVA was observed (p = 0.001). No statistically significant changes were observed in CMT, SCT, CD, AASP, or AADP (p > 0.05). The treatment was well tolerated, with few mild side effects, and no patient developed wet AMD.
Conclusion:
PBM-Valeda therapy demonstrated a favorable short-term safety profile in patients with dry AMD. The key finding of this study was the stability of SS-OCT and SS-OCTA biomarkers (CMT, SCT, CD, AASP, and AADP), with no adverse changes observed. These results reinforce the short-term safety of PBM. Reported side effects were minimal, with no evidence of retinotoxicity. This is the first prospective study to explore SS-OCT and SS-OCTA biomarkers in patients with dry AMD undergoing PBM therapy, providing preliminary safety data for future controlled trials.
Keywords
Introduction
Age-related macular degeneration (AMD) impairs central vision in individuals over 50 years of age and remains a leading cause of irreversible visual loss in Western countries. 1 The number of cases in the United States is expected to reach approximately 7.5 million by 2030. 2 In Brazil, approximately three million adults are affected. 3 AMD presents as atrophic (dry) or neovascular (wet) forms, with the latter causing 80% of AMD-related legal blindness despite representing only 10% of cases.4,5
The Age-Related Eye Disease Study (AREDS) staging system categorizes progression from microdrusen to geographic atrophy (GA) or neovascularization with visual acuity (VA) worse than 20/32. 6 Antivascular endothelial growth factor (anti-VEGF) injections have transformed wet AMD management, 7 and the dry form of AMD shows disruption in retinal pigment epithelium (RPE) and outer retinal atrophy, 8 and antioxidant supplementation, which only delays progression in 20%–25% of eyes. 9 In 2024, the FDA approved the Valeda photobiomodulation (PBM-Valeda) system for dry AMD, following earlier approvals by European agencies and ANVISA.9,10
PBM uses light with wavelengths between 500 and 1000 nanometers (nm) to modulate mitochondrial function and cellular repair mechanisms.11–13 Cytochrome c oxidase (CcO) serves as the primary chromophore, with photon absorption accelerating electron flow and ATP synthesis.12,13 PBM-Valeda delivers multiwavelength beams (590 nm, 660 nm, and 850 nm) target specific cellular mechanisms: 590 nm light suppresses VEGF expression,11,14 whereas 660 nm and 850 nm light interact with different CcO sites to increase oxygen binding and electron transfer.12,13 Clinical studies have confirmed Valeda’s safety and efficacy in slowing functional decline in early/intermediate dry AMD.8,9,15
Multiple trials, including LIGHTSITE I 15 and subsequent LIGHTSITE II 8 and III 9 multicentre investigations, have demonstrated that PBM-Valeda treatment can improve VA, reduce drusen load, and enhance contrast sensitivity.8,9,15
Swept-source optical coherence tomography (SS-OCT) provides superior choroidal imaging with 8 µm axial resolution and 100,000 A-scans per second at 1050 nm, enabling precise choroidal thickness measurements.11,12 SS-OCT angiography (SS-OCTA) captures erythrocyte flow to visualize the retinal microvasculature without dye injection, allowing assessment of deep plexuses and subtle vascular changes. 13
The primary objective of this study was to evaluate between pre- and post-treatment periods with PBM-Valeda: a) best-corrected visual acuity (BCVA); b) biomarkers obtained by SS-OCT and SS-OCTA. The biomarkers were: central macular thickness (CMT), subfoveal choroidal thickness (SCT), capillary density (CD), avascular area of the superficial plexus (AASP), and avascular area of the deep plexus (AADP). As a secondary outcome, a subjective assessment of visual function was performed using a structured questionnaire administered to patients at the end of treatment.
Methods
A prospective, noncomparative, interventional pilot case series study was conducted involving 19 patients (25 eyes) diagnosed with dry AMD who were treatment-naïve except for AREDS-2 vitamin supplementation. Participants were recruited from the Retina Department at the Instituto de Oftalmologia de Presidente Prudente, SP, Brazil.
Inclusion criteria
Participants were eligible if they met the following requirements:
Aged 50 years or older. Diagnosis of dry AMD characterized by drusen presence. Current use of AREDS-2 mineral and antioxidant supplements. Noncenter-involving GA. BCVA between 20/25 and 20/200 using Early Treatment Diabetic Retinopathy Study (ETDRS) and Snellen charts. Complete medical records including demographics, medications, intraocular pressure (IOP) measurements, BCVA assessments, and SS-OCT/SS-OCTA results. Signed informed consent.
Exclusion criteria
Exclusion criteria were as follows:
History of choroidal neovascularization. Centre-involving GA. Other major retinal conditions (e.g., diabetic retinopathy, epiretinal membrane, macular hole, retinal dystrophies). Other ophthalmological conditions (e.g., glaucoma). Previous ocular surgeries (e.g., retinal detachment repair, glaucoma surgery). Inability to complete the treatment protocol.
Ethics approval
This study was conducted in accordance with Resolution 466/12 of the National Health Council of Brazil. The research protocol received approval from the Ethics Committee of Universidade do Oeste Paulista (UNOESTE), Presidente Prudente, SP, Brazil (approval date: September 28, 2023; CAAE: 70635623.5.0000.5515). All participants provided written informed consent before enrollment.
Study design
Patients who met the inclusion criteria and provided written informed consent between September 2023 and January 2025 were enrolled in the study. After the diagnosis of dry AMD, participants were evaluated for age, sex, medical and ocular history, and AREDS score.
Baseline assessments included medical history, BCVA, IOP, slit-lamp biomicroscopy, dilated fundus examination, color fundus photography, red-free imaging, fundus autofluorescence (FAF), fluorescein angiography (FA), SS-OCT, and SS-OCTA. These tests were repeated 4 weeks after treatment initiation (baseline).
BCVA was assessed using Snellen visual charts and converted to logarithm of the minimum angle of resolution (logMAR) units for statistical analysis. Retinal and choroidal images were obtained using SS-OCT and SS-OCTA (DRI-OCT Triton; Topcon, Tokyo, Japan). The images were analyzed using automated layer segmentation software. Scans measuring 7 × 7 mm were used for SS-OCT and 4.5 × 4.5 mm for SS-OCTA. Retinal thickness was defined as the distance between the vitreoretinal interface and the RPE. Choroidal thickness was measured as the distance from the outer edge of the RPE to the choroidoscleral border. The automated calibration software of the SS-OCT system calculated the distances between these layers.
CMT and SCT were defined as the average thickness within the central 1000 µm diameter of the ETDRS grid, as calculated by the SS-OCT software’s macular and choroidal thickness maps.
Imaging examinations were performed in a masked fashion to minimize potential bias. All SS-OCT and SS-OCTA exams were conducted by a trained technician who was blinded to the study protocol and patient treatment status. Two independent ophthalmologist investigators analyzed the images. Any discrepancies in measurements were resolved by a third reviewer to ensure accuracy and objectivity. Each layer of the vitreoretinal interface, RPE, and choroidoscleral boundary was carefully examined to verify segmentation accuracy, with manual adjustments performed when necessary.
The SS-OCTA images included two primary measurements: (A) CD: automatically calculated by the OCTA software (Imaginet 6), which in this system, reflects the total vessel density of the retina by combining the superficial capillary plexus and deep capillary plexus.
(B) Foveal avascular zone (FAZ) areas in the superficial and deep capillary plexuses. One of the advantages of this imaging technology is its ability to segment the retinal vascular layers. The FAZ area of the superficial plexus was labeled as AASP and that of the deep plexus as AADP. These areas were measured manually by an experienced ophthalmologist and confirmed by a second specialist, since the software does not provide this measurement automatically. In cases of discrepancy, a third expert was consulted to ensure accuracy and eliminate measurement bias.
After confirmation of dry AMD and determination of treatment indication, patients were thoroughly informed about the procedure, including associated risks, potential benefits, and expected visual outcomes. SS-OCT and SS-OCTA evaluations were performed at baseline and at follow-up visits to assess structural and functional changes. All PBM-Valeda treatments were administered by the same ophthalmologist. At the final visit, patients completed a brief subjective questionnaire developed by the investigators to evaluate perceived changes in visual function. They were asked to respond whether VA and contrast sensitivity were “improved,” “stable,” or “worsened,” and whether any side effects occurred. This qualitative tool was used to supplement the objective imaging and functional data (as an exploratory tool, not as a validated functional endpoint).
PBM protocol
The PBM-Valeda delivered three wavelengths: 590 nm (4 mW/cm2, 2 × 35 sec), 660 nm (65 mW/cm2, 2 × 90 sec), and 850 nm (0.6 mW/cm2, 2 × 35 sec). Treatment with PBM-Valeda was performed three times a week for 3 weeks (totaling 9 sessions).
The study design is illustrated in Figure 1.
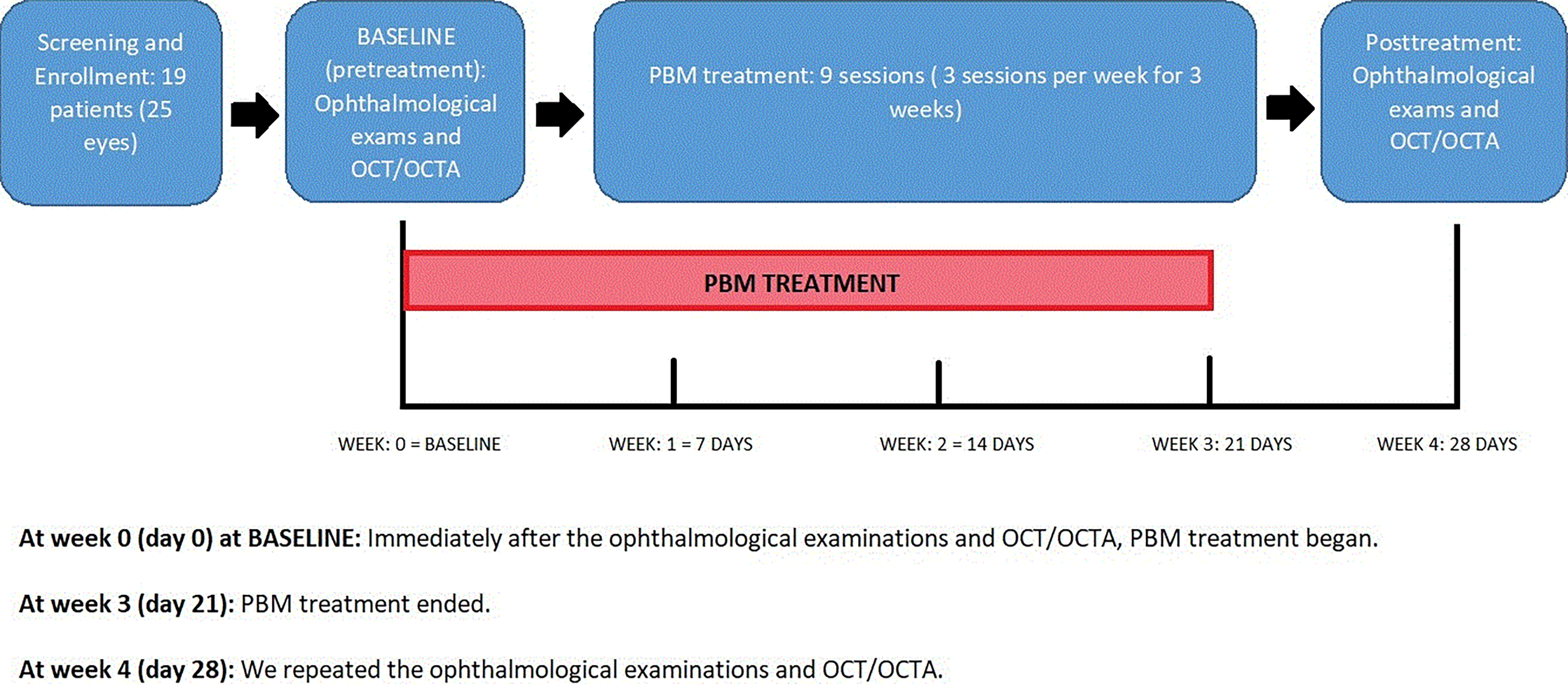
Study design and timeline of interventions and assessments. This prospective pilot study included 19 patients (25 eyes) with dry age-related macular degeneration (AMD) treated with photobiomodulation (PBM) using the Valeda® device. Following screening and baseline ophthalmological assessment, each patient underwent a series of 9 PBM sessions over a 3-week period (3 sessions/week). Structural and vascular biomarkers were evaluated using swept-source optical coherence tomography (SS-OCT) and OCT-angiography (SS-OCTA) both before (baseline, day 0) and after treatment (day 28). A subjective visual function questionnaire was also applied post-treatment. The diagram outlines the enrollment, treatment, and follow-up phases along with key timepoints.
Statistical analysis
Statistical analysis was performed using Stata, version 17 (StataCorp LLC) and SPSS, version 20 (IBM Corp). The data were expressed as the mean ± SD and median (interquartile range) or frequencies according to the nature of the characteristic evaluated. The means of measurements between two moments were evaluated using linear random effects models (linear mixed models) with unstructured covariance structure to accommodate possible dependence between eyes of the same patient. The normality of distribution was assessed by the Kolmogorov–Smirnov test. Since we are conducting multiple tests and mitigating the risk of type I error, the p-values were corrected using Benjamini–Hochberg procedure. The tests were two-sided, and p-values of <0.05 were considered significant.
Results
The study included 25 eyes from 19 patients. As shown in Table 1, 9 patients were female (47.4%) and 10 were male (52.6%). The mean age was 72.6 years (SD = 11.2 years), ranging from 56 years to 94 years. Of the 19 patients, 6 had both eyes treated (31.6%) and 13 were treated in just one eye (68.4%). Among the 13 patients whose contralateral eye was not treated, 6 (46.15%) had exudative AMD (treated with intravitreal aflibercept 40 mg/mL), and 7 (53.85%) were diagnosed with dry AMD. These untreated eyes either did not meet the inclusion criteria or met the exclusion criteria. A total of 48% of the treated eyes (12 eyes) were on the right side and 52% (13 eyes) were on the left. Regarding the AREDS classification of the 25 eyes, none of the eyes (0%) were Category I or IV, 16 eyes (64%) were Category II, and 9 eyes (36%) were Category III.
Demographic and Ocular Characteristics
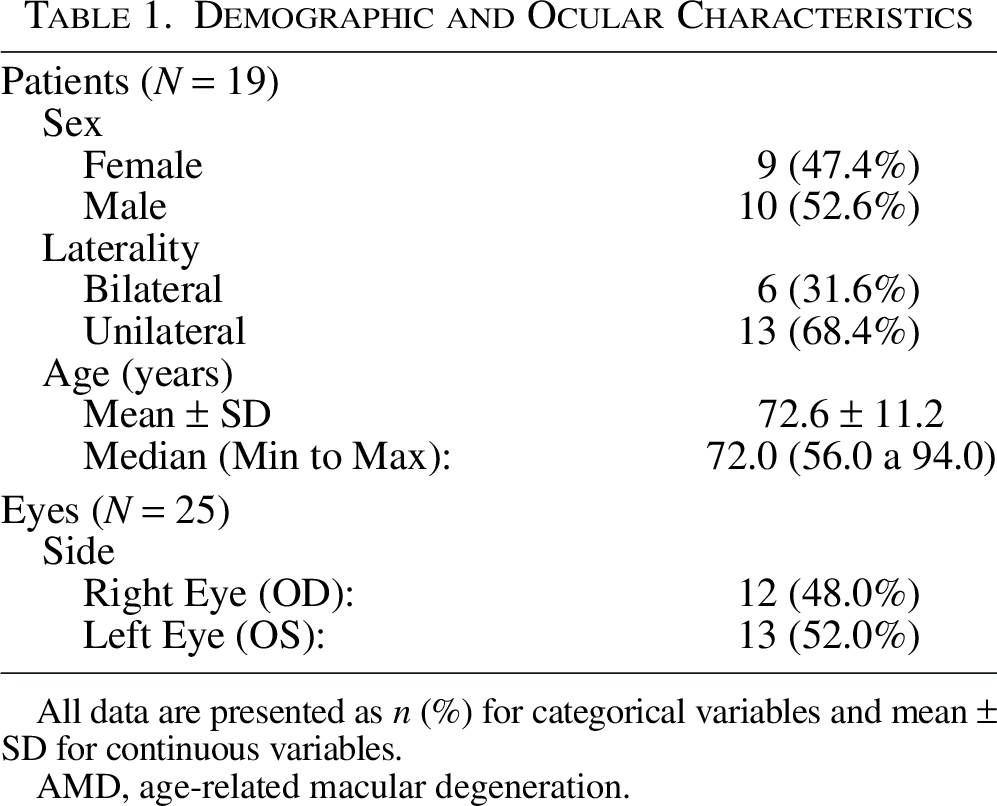
All data are presented as n (%) for categorical variables and mean ± SD for continuous variables.
AMD, age-related macular degeneration.
Table 2 summarizes the biomarkers evaluated. Mean BCVA changed from 0.38 (20/48 Snellen) to 0.32 (20/42), with a statistically significant difference of p = 0.001 (Fig. 2) (Fig. 4). No statistically significant changes were observed in CMT, SCT, CD, AASP, or AADP (Fig. 3 to 7) (Fig. 5 to 9). The mean CMT varied from 234.56 µm at baseline to 236.08 µm post-treatment (p = 0.198). The mean SCT varied from 163.00 µm at baseline to 161.8 µm post-treatment (p = 0.546). CD varied from 15.08 to 15.62 (p = 0.567), AASP from 187,644.80 µm2 to 177,198.24 µm2 (p = 0.466), and AADP from 268,296.72 µm2 to 270,879.44 µm2 (p = 0.865). Figures 8 and 9 Figures 2 and 3 illustrate a multimodal SS-OCT and SS-OCTA case of a 60-year-old patient with dry AMD in the left eye, showing pre- and post-treatment measurements of CMT and SCT in µm (Fig. 8: Fig. 2: structural biomarkers), AASP and AADP in µm2 and CD (Fig. 9: Fig. 3: vascular biomarkers).
Summary Measurements and Linear Random Effects Model Results of BCVA and Biomakers
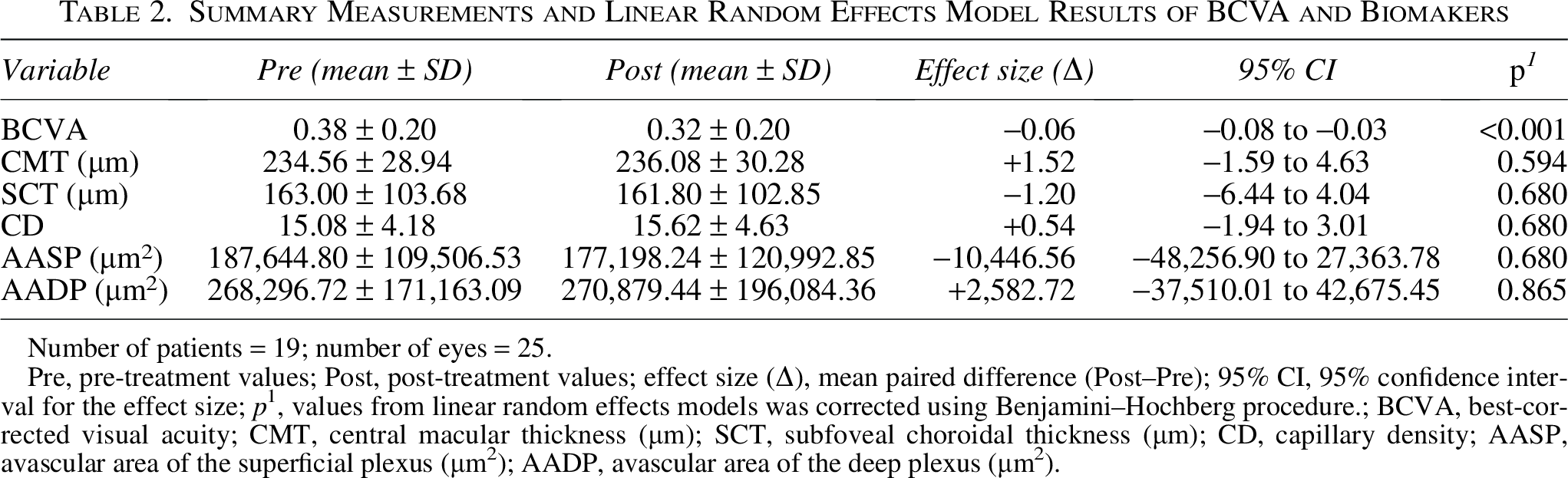
Number of patients = 19; number of eyes = 25.
Pre, pre-treatment values; Post, post-treatment values; effect size (Δ), mean paired difference (Post–Pre); 95% CI, 95% confidence interval for the effect size; p1, values from linear random effects models was corrected using Benjamini–Hochberg procedure.; BCVA, best-corrected visual acuity; CMT, central macular thickness (µm); SCT, subfoveal choroidal thickness (µm); CD, capillary density; AASP, avascular area of the superficial plexus (µm²); AADP, avascular area of the deep plexus (µm²).
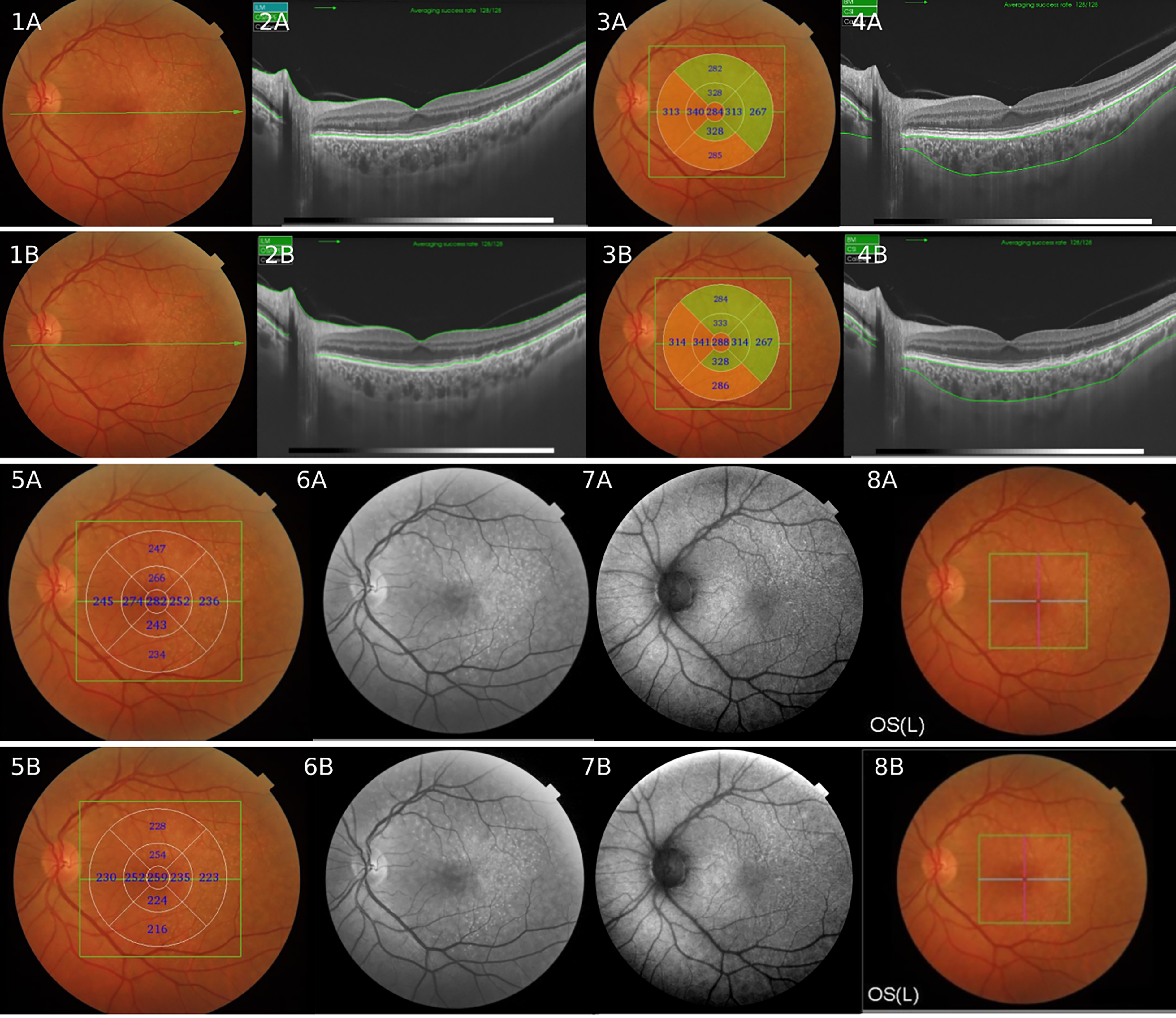
Images obtained using SS-OCT showing structural biomarkers of a 60-year-old female patient with dry age-related macular degeneration, treated with nine sessions of PBM-Valeda. Retinography (1A: pre-treatment and 1B: post-treatment) shows yellowish-white dots corresponding to hard drusen in the macular area. SS-OCT B-Scan: Pre (2A) and post (2B) images with macular thickness delineation. Macular thickness maps (ETDRS) are shown in 3A (pre: CMT: 284 µm) and 3B (post: CMT: 288 µm). Images 4A (pre) and 4B (post) are SS-OCT B-scans with choroidal thickness delineation, while 5A (pre: SCT: 282 µm) and 5B (post: SCT: 258 µm) are choroidal thickness maps. Images 6A (pre) and 6B (post) correspond to red-free imaging, while 7A and 7B correspond to autofluorescence imaging before and after treatment, highlighting hyperautofluorescent lesions corresponding to hard drusen. Image 8A shows retinography with drusen and the scan delimitation of the 4.5 × 4.5 mm SS-OCT angiography (green central square); 8B shows the post-treatment scan. All biomarker analyses presented in this figure yielded p values > 0.05. CMT, Central Macular Thickness; SCT, Subfoveal Choroidal Thickness.
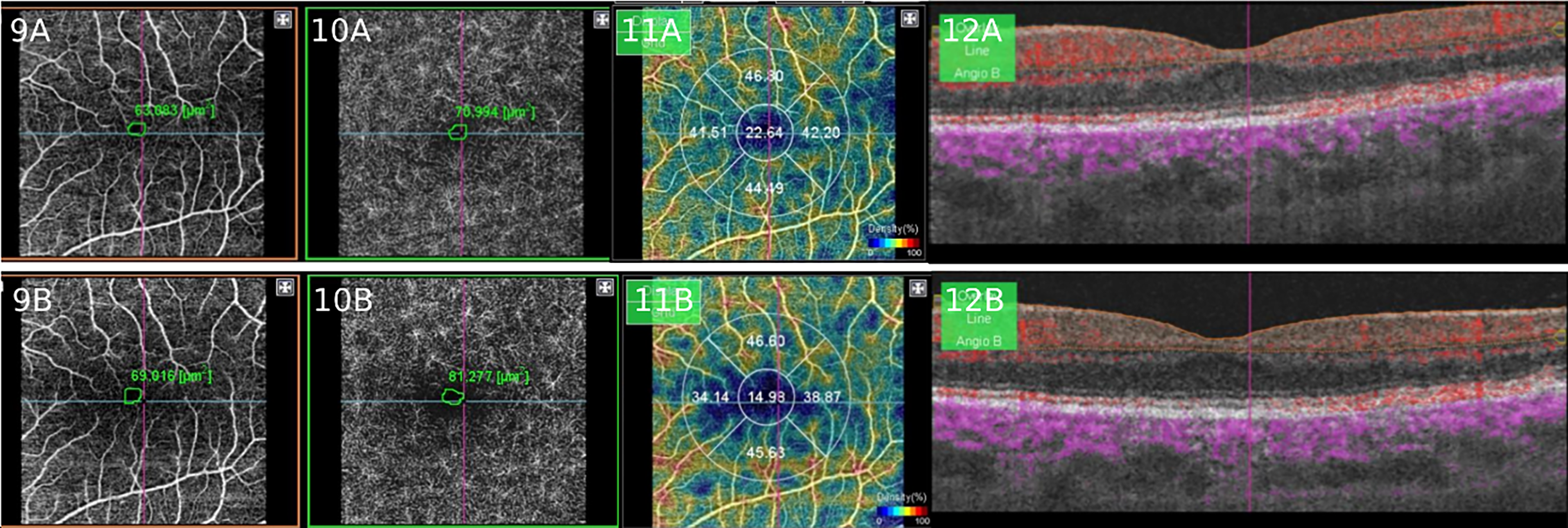
Images (of the same paciente in the figure 2) obtained using SS-OCT Angiography showing vascular biomarkers. Images 9A (pre) and 9B (post) display the AASP (9A = 63.083 µm² and 9B = 69.016 µm²). Images 10A (pre) and 10B (post) show the avascular area of the deep plexus (10A = 70.994 µm² and 10B = 81.277 µm²). Images 11A (pre) and 11B (post) represent the capillary density map, with 11A = 22.64 and 11B = 14.93 in the central foveolar region. Images 12A (pre) and 12B (post) are B-scans, with red areas corresponding to blood flow, as analysed by the device's software. All biomarker analyses presented in this figure yielded p values > 0.05. AASP, Avascular Area of the Superficial Plexus; AADP, Avascular Area of the Deep Plexus; CD, Capillary Density.
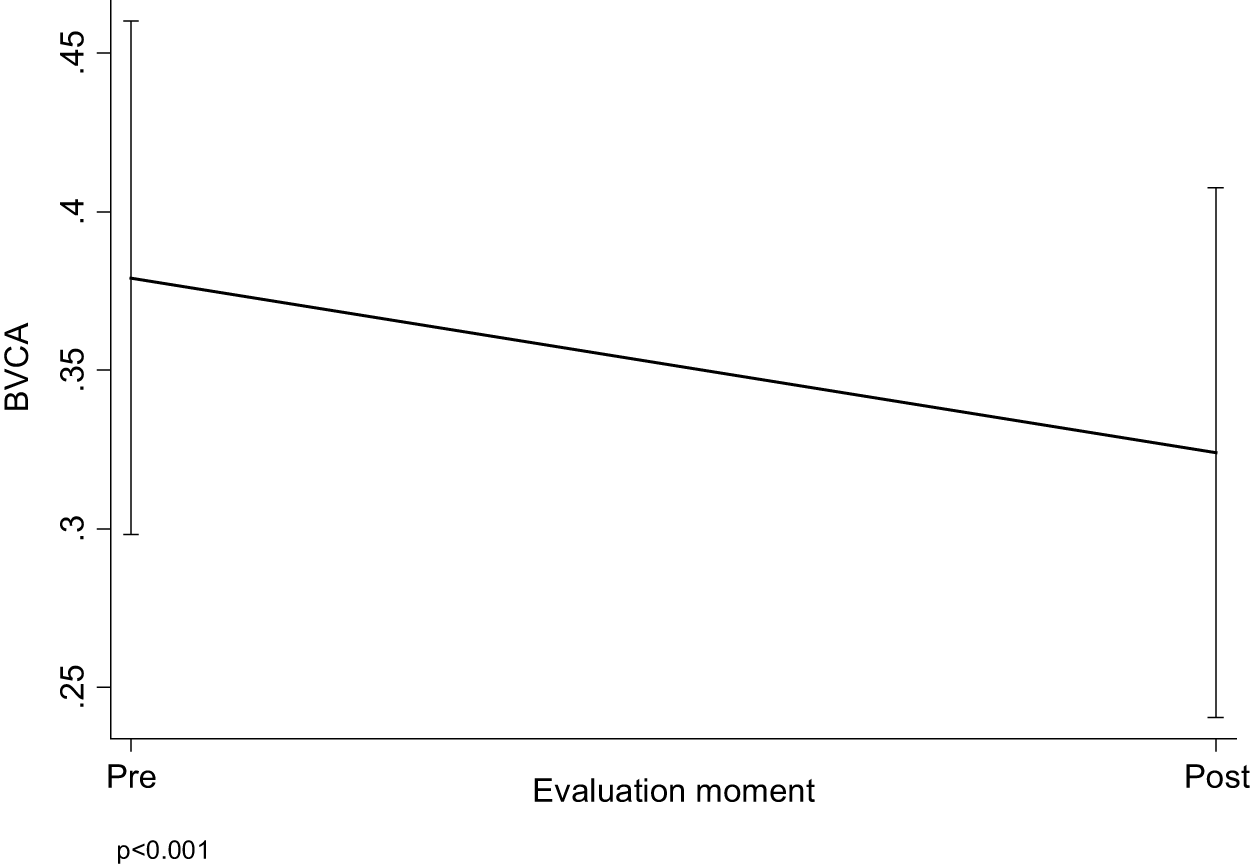
Mean and 95% Confidence Interval of BCVA by Evaluation Moment.
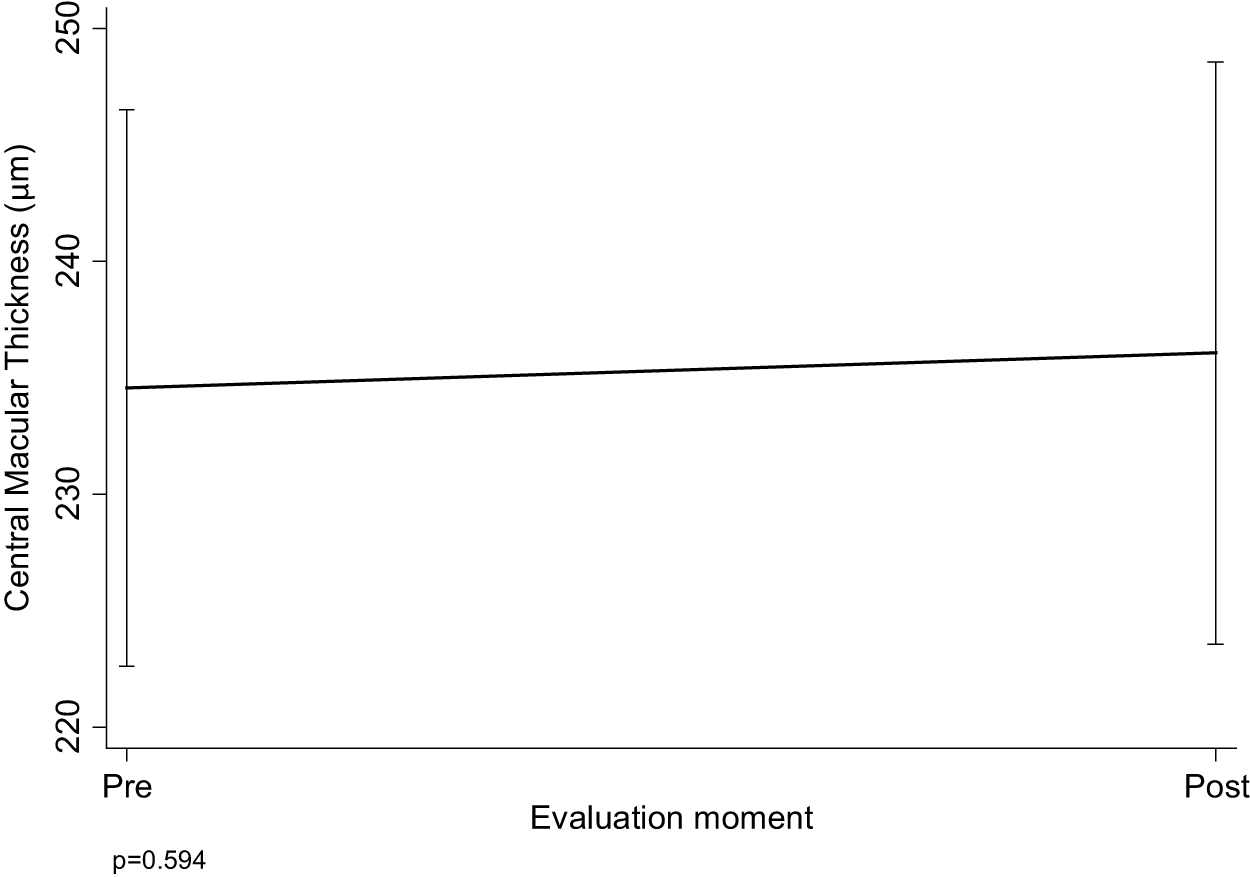
Mean and 95% Confidence Interval of CMT by Evaluation Moment.
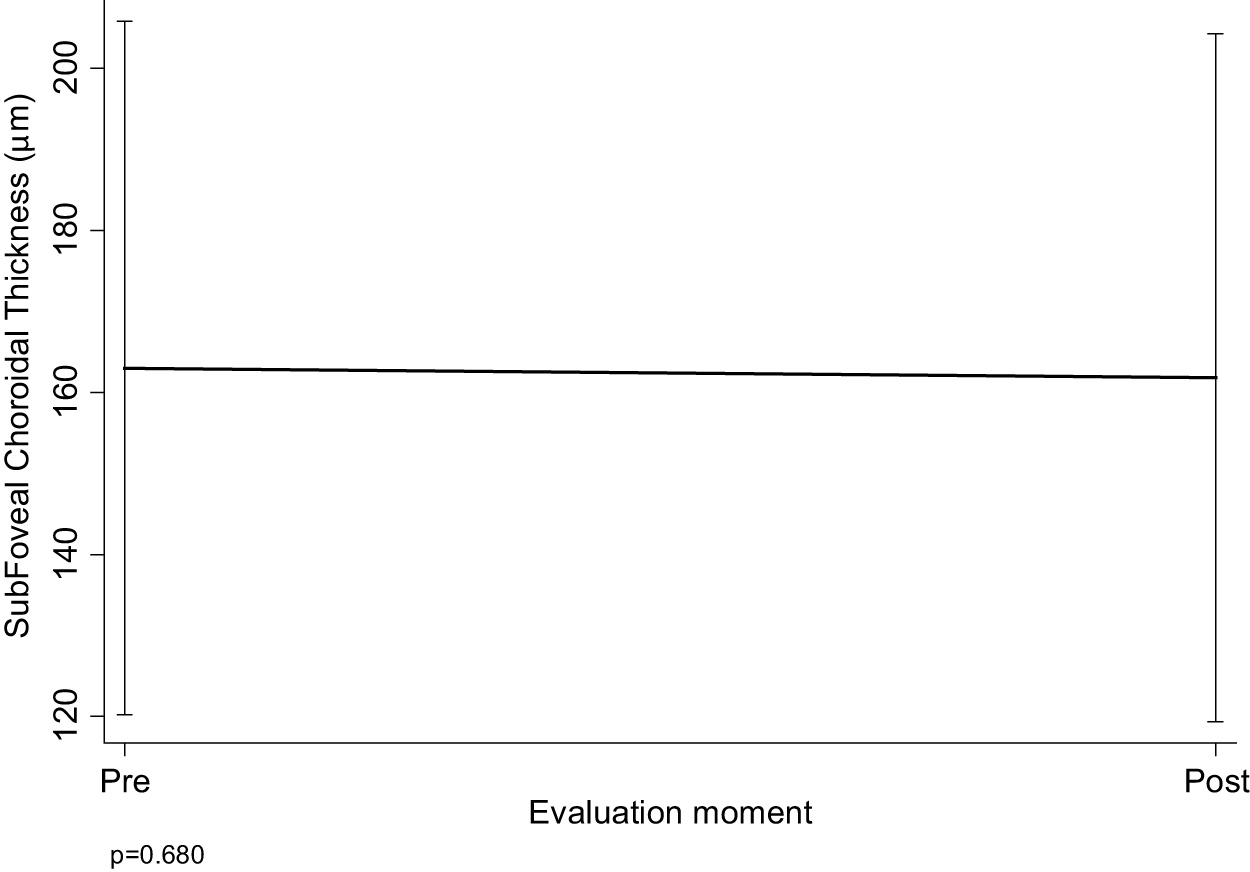
Mean and 95% Confidence Interval of SCT by Evaluation Moment.
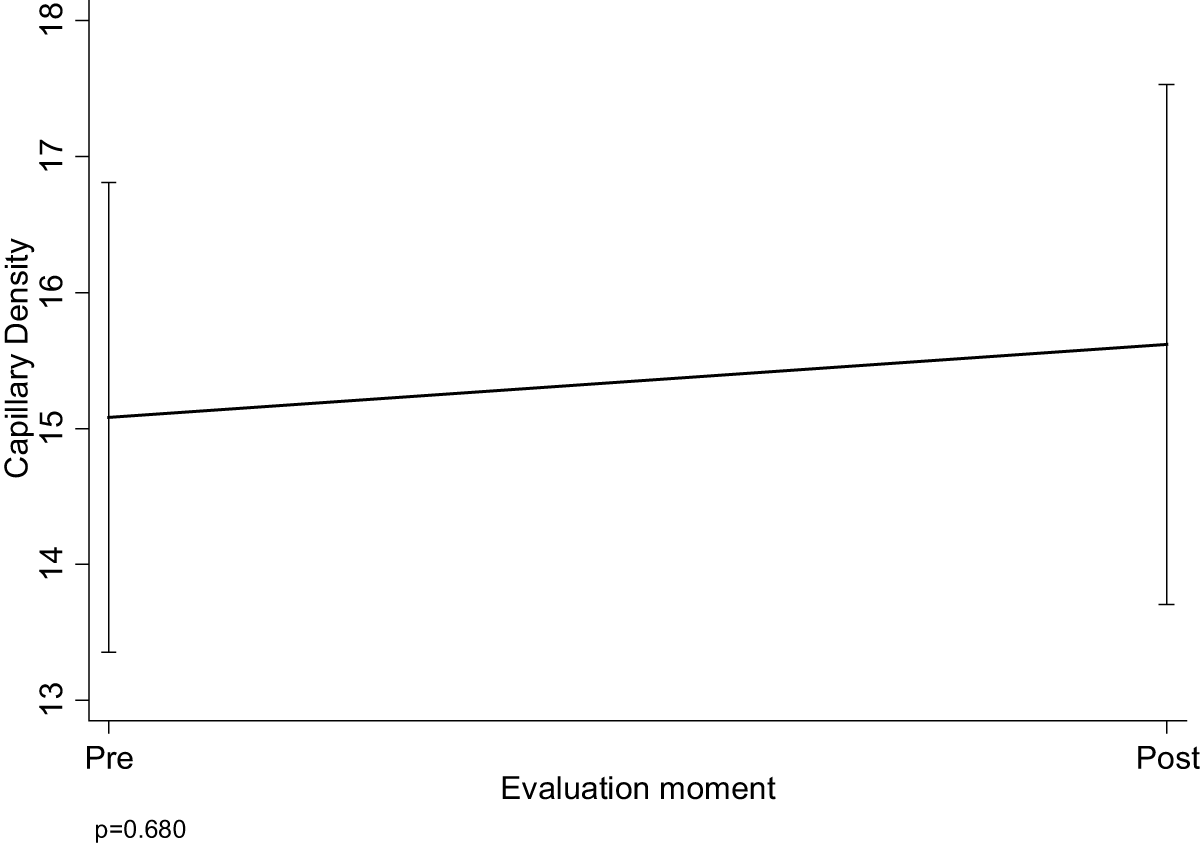
Mean and 95% Confidence Interval of CD by Evaluation Moment.
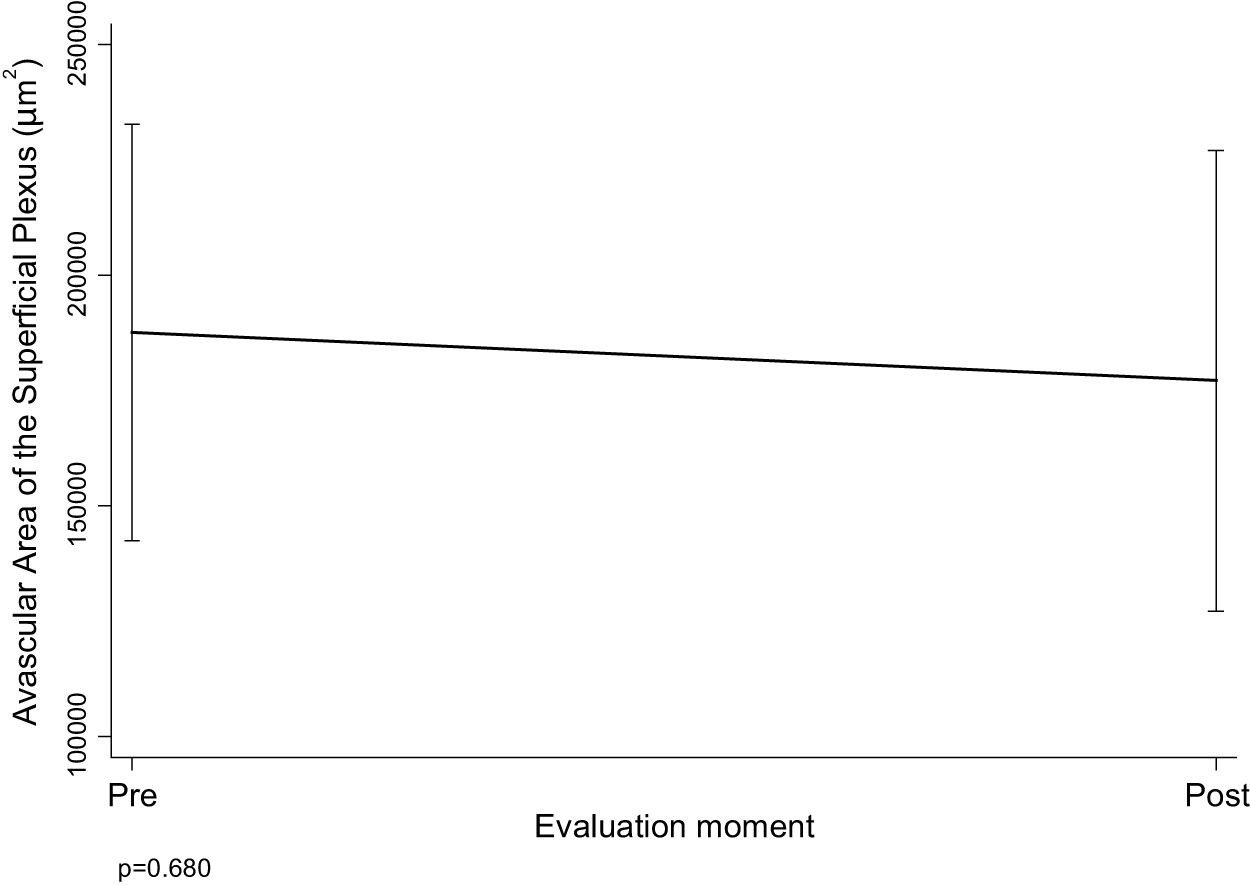
Mean and 95% Confidence Interval of AASP by Evaluation Moment.
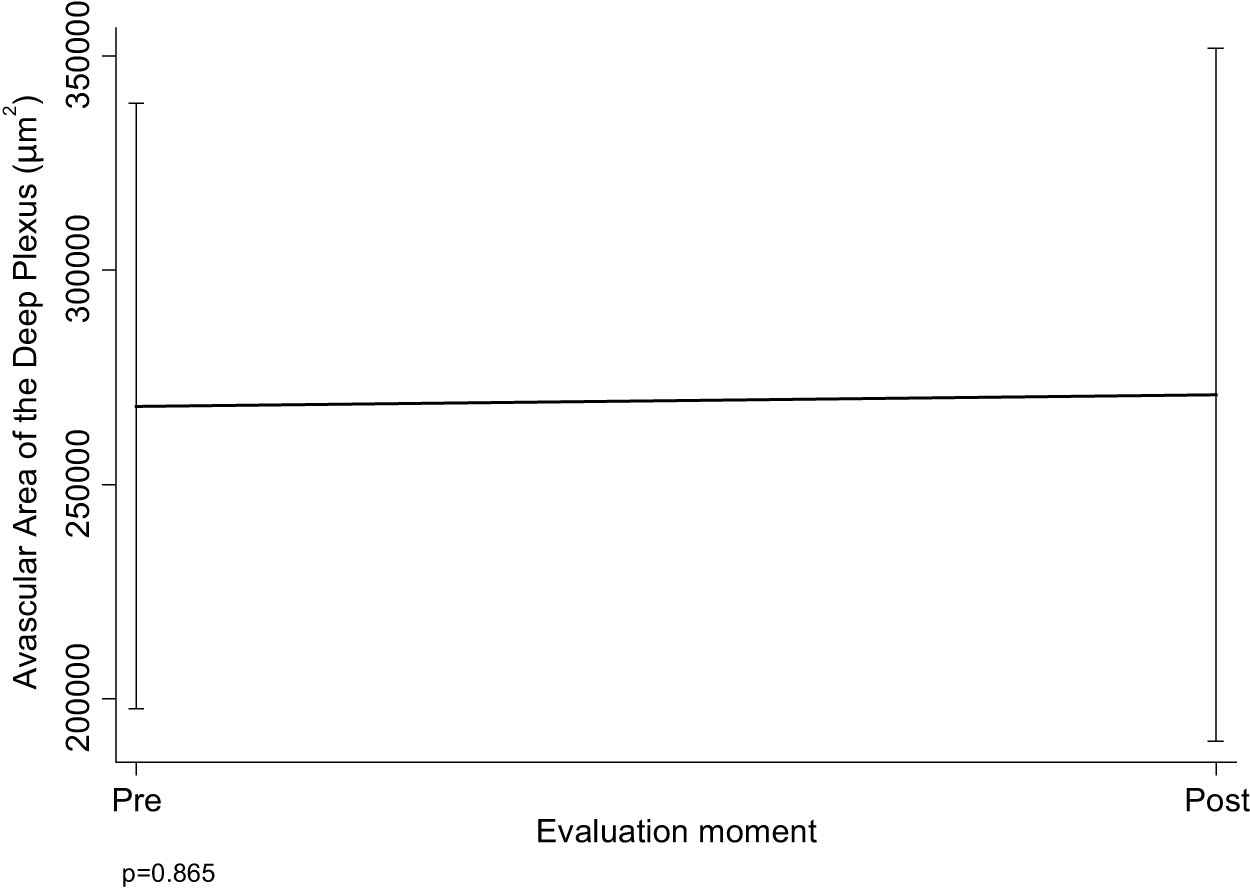
Mean and 95% Confidence Interval of AADP by Evaluation Moment.
No patient discontinued treatment due to adverse effects. The most common side effects were dry eye, reported by 3 of the 19 patients, and pruritus, reported by 2. Both conditions improved with lubricating eye drops. There were no serious side effects, and no patient progressed to the exudative form of AMD. An important subjective observation in this study, based on a structured exit questionnaire (an exploratory tool), was that 15 of the 19 patients reported a perceived change in VA and enhanced perception of color/contrast sensitivity. The remaining 4 patients reported stable VA. No patient reported worsening of VA following PBM-Valeda treatment. IOP did not show a notable difference, with values of 12.68 ± 1.30 pre-treatment and 12.79 ± 1.44 post-treatment (p = 0.641). Since dry AMD is a chronic disease, progression to GA was not evaluated in the present study.
Discussion
This study primarily provides evidence on the safety of PBM-Valeda therapy, supported by the stability of structural and vascular biomarkers assessed with SS-OCT and SS-OCTA. Importantly, the stability of biomarkers (CMT, SCT, CD, AASP, and AADP) remains the key finding of our study. This finding is unprecedented in the literature.
We observed a statistically significant change in BCVA following PBM therapy. However, this finding must be interpreted with caution due to the absence of a control group and the subjective nature of VA testing, which is subject to interindividual variability and influenced by external factors such as motivation, patient learning during the follow-up period, and examination conditions. Changes in BCVA have already been reported in previous studies, including LIGHTSITE I-III.16–18
PBM therapy in patients with dry AMD has multiple benefits: improved VA, enhanced contrast sensitivity, reduced central drusen volume, improved quality of life, and decreased progression of GA.18,19 In the study conducted by Merry et al., significant changes in BCVA was measured immediately after treatment (3 weeks) and at 3 months. 18 In our investigation, this change was verified 1 week after treatment ended (28 days after baseline). Similarly, Viggiano et al. and Nassisi et al. reported significant changes in BCVA over a short follow-up period.20,21
In this study, 16 eyes (64%) were AREDS Category II, 9 (36%) were Category III, and no eyes were Category I or IV. In contrast, Category III was the primary group observed in the LIGHTSITE III (86.9%) and LIGHTSITE II (64.70%) studies. In LIGHTSITE I, most patients were Category IV (67.4%) or Category III (30.4%).16–18
The CMT in healthy patients is approximately 230 µm. The average CMT in patients with dry AMD in our cohort was 234.56 µm, consistent with findings in the literature. 8 Studies have shown that CMT tends to decrease with disease progression, particularly as the condition advances toward GA. As Giani et al. demonstrated, the average CMT in patients affected by dry AMD was 220 µm. 22
This study did not include a control group, as our primary objective was not to evaluate treatment efficacy but to analyze the behavior of biomarkers and the safety of the intervention (side effects). All patients in our study were taking vitamin supplementation according to the AREDS 2 study. Antioxidant and mineral supplementation can delay nonexudative AMD progression to exudative AMD. For many years, the only proven supplement for nonexudative AMD was based on the findings of the AREDS formulation, consisting of vitamin C, vitamin E, beta-carotene, zinc, and copper, which demonstrated a 25% reduced risk of severe vision loss in individuals with intermediate-sized drusen, at least one large druse, noncentral GA, or advanced AMD over 5 years. Subsequent supplementation trials included the AREDS 2 formula, which modified the compound by replacing beta-carotene with lutein and zeaxanthin. 23
Based on the exploratory exit questionnaire, there was subjective change in both VA and color/contrast sensitivity, and few side effects of low clinical significance. Although qualitative in nature, these findings corroborate the functional relevance of PBM and align with previous reports suggesting improved visual performance after treatment.8,9,15,18
In this study, PBM-Valeda treatment was well tolerated, with a low occurrence of side effects, all of which were mild. This aligns with previous research demonstrating a favorable risk–benefit profile, a low occurrence of adverse events, and no evidence of retinal toxicity, reinforcing that it is a safe and well-tolerated therapy.18,24
The primary contribution of this study is the demonstration of biomarker stability and safety, not functional improvement. The observed change in BCVA, although statistically significant, was modest and cannot be attributed to PBM in the absence of a control group.
This study has some important limitations that must be emphasized, including its short follow-up, absence of control group, small sample size, and a single-center design. These factors limit the generalizability of our results and preclude definitive conclusions about treatment efficacy or disease progression. Nevertheless, our findings provide valuable preliminary safety data on this innovative treatment for dry AMD, particularly regarding structural and vascular biomarkers evaluated with SS-OCT and SS-OCTA, representing the first such assessment in the literature.
Conclusion
This is the first prospective study in the medical literature that uses SS-OCT and SS-OCTA to evaluate early choroidal and retinal structural and vascular biomarkers of response to PBM in dry AMD, thus providing new insights into this therapy. PBM-Valeda demonstrated a favorable short-term safety and tolerability profile in patients with dry AMD. The stability of SS-OCT and SS-OCTA biomarkers (CMT, SCT, CD, AASP, and AADP) was the key finding and supports the short-term safety of this treatment. In addition, the absence of serious adverse events, no progression to wet AMD, and a low incidence of mild, self-limiting side effects further support its safety. However, these findings should be interpreted with caution due to inherent limitations of the study design (single-center, small sample size, the questionnaire used was exploratory and not a validated endpoint, and short follow-up of only 28 days), which precludes assessment of the progression of GA. Further multicenter, randomized, controlled clinical trials with long-term follow-up are needed to confirm these safety findings and evaluate efficacy.
Authors’ Contributions
The study design was a collaborative effort involving M.P.R., R.B., and T.C., who collectively contributed to the conceptualization and initial study design. M.P.R. served as the principal investigator, formulating the research question, drafting the article, conducting pre- and post-treatment ophthalmological exams and administering the PBM-Valeda therapy. F.A.F. collected medical records and exam data from the SS-OCT and SS-OCTA devices and contributed to the study’s design and planning. J.P. assisted with the literature review and examined relevant research. R.B. conducted comprehensive research and provided a critical review. T.C. contributed during the article review phase. M.P.R. oversaw the data analysis and interpretation, coordinated the submission process, and served as the corresponding author.
Footnotes
Funding Information
The authors have no funding to report.
Ethical Committee Approval
The study was carried out in accordance with the guidelines outlined in Resolution 196/96 of the National Health Council of the Ministry of Health. The research protocol was submitted for analysis and received approval (September 28, 2023) from the Ethics Committee of the Universidade do Oeste Paulista—UNOESTE—Presidente Prudente, SP (CAAE—70635623.5.0000.5515). All patients who participated in this assessment signed a free and informed consent form so that we could carry out this study.
Data Availability
All datasets presented in the study are included in the article/Supplementary Material.
Disclosure Statement
The authors declare that they have no competing interests. The authors declare that neither they nor their institutions have received any financial support, equipment, or other benefits from the manufacturer of the Valeda device (LumiThera Inc.) for this study. No institutional or personal relationships exist between the authors and the device manufacturer.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.