
Abstract
Background:
Photobiomodulation (PBM) is a noninvasive light therapy that penetrates deeper skin layers, using wavelengths such as near-infrared. Different wavelengths target specific cellular components and pathways, influencing wound healing. Light absorption by both mitochondria and light-sensitive ion channels increases intracellular reactive oxygen species (ROS) levels, thereby affecting inflammation, platelet activation, angiogenesis, tissue remodeling, and cell viability. Concurrent use of multiple wavelengths has an advantage, activating distinct pathways involved in the wound-healing process.
Purpose:
This in vitro study aimed to investigate the effects of concurrent PBM on fibrablasts using a dual-wavelength system (655 nm and 808 nm). The effects of concurrent PBM application at three energy densities on cell viability, intracellular ROS levels, and cell migration were assessed using two modalities: single- and triple-treatment protocols.
Methods:
Three different energy densities (0.5, 1, and 2 J/cm2) of a dual wavelength system were used, and applications were performed using single or triple applications. Cellular responses were evaluated by assessing viability, ROS generation, and migration.
Results:
Concurrent PBM application at an energy density of 1 J/cm2 showed a synergistic effect, increasing cell viability by 3%, intracellular ROS levels by 20%, and accelerating wound closure by 89% compared with the untreated group.
Conclusion:
Concurrent dual-wavelength PBM application may reduce treatment duration and enhance wound healing, offering a promising approach for targeting multiple layers and substructures of complex biological tissue in in vivo models and clinical applications.
Keywords
Introduction
Wound healing is a complex process involving various biochemical, cellular, and physiological pathways to achieve proper recovery. It primarily aims to restore tissue integrity disrupted by multiple factors.1,2 Despite the existence of various successful treatment methods, many types of wounds can resist the treatment. Even the presence of any infection at the wound site makes this process more problematic. 3 For more than five decades, light-based therapies have been used to accelerate the healing process and minimize infection at the site by triggering various biochemical processes. 4 Light-based wound treatments also provide noninvasive approaches that can be applied directly to open wounds. 5 One of the light-based therapies, photobiomodulation (PBM), formerly known as low-level laser therapy, involves low-energy light irradiation of cells to accelerate the healing process, modulate the immune response, reduce inflammation, and relieve pain.6–9 Its mechanism of action has not been proven totally. However, several studies indicate that the commonly used wavelengths for PBM, in the red and near-infrared (NIR) spectrum, are absorbed by cytochrome c oxidase (Complex IV of the electron transport chain) in mitochondria. Photon absorption by Complex IV induces photochemical cascades, which result in the release of nitric oxide (NO) and increases in adenosine triphosphate and reactive oxygen species (ROS) levels. The second proposed mechanism involves the light-gated channels on the cell membrane. 8 The absorption of photons at applied wavelengths by these channels results in increased passage of several ions across the cell membrane, which can participate in cellular physiology. Another proposed one is that ROS generated by PBM activates transforming growth factor β, which plays a role in cell proliferation and inflammation. 7
The PBM application at a certain wavelength to trigger cell proliferation, wound healing, regeneration, and reduction of inflammation and pain has been well investigated in vitro. However, a few studies use more than one light source (combining two different wavelengths) and report positive effects on wound healing by triggering different cellular pathways. The absorption of two wavelengths at different energy densities can simultaneously trigger different pathways. In particular, irradiation at multiple wavelengths has a positive effect, reaching different layers of the tissue. Hence, the travel length of light depends strongly on its wavelength. 10 Better results were generally obtained when irradiation was performed with red and NIR light, especially for deeper wounds. 11
The results of combining different wavelengths vary; some enhanced wound healing compared to using a single wavelength, while others had no effect. Even the application method of wavelengths varies. For example, two different irradiations were performed sequentially, rather than simultaneously. 12 However, the simultaneous application of two wavelengths is very limited. In this work, the effect of a dual-laser system with two wavelengths, 655 and 808 nm, on healthy fibroblast cells was investigated. The effects of this dual-wavelength system, applied through two application modalities, on proliferation, ROS production, and wound healing were examined in vitro.
Materials and Methods
Materials
In this study, Dulbecco’s modified Eagle medium (DMEM), trypsin–EDTA 10X, penicillin–streptomycin, phosphate-buffered saline (PBS), 3-(4,5-Dimethylthiazol-2-yl)-2,5-Diphenyltetrazolium bromide (MTT), and diacetyldicholorofluorescein (DCFH-DA) were supplied from Sigma-Aldrich (St. Louis, USA). Fetal bovine serum (FBS) was purchased from Capricorn Scientific GmbH (Ebsdorfergrund, DE), and dimethyl sulfoxide (DMSO) was obtained from Merck (Darmstadt, DE).
Cell line and culture
In this study, healthy mouse fibroblast cells (L-929), obtained from the Animal Cell Culture and Tissue Engineering Laboratory at Ege University, were used. The cells were grown in a 25 cm2 cell culture flask containing DMEM basal media supplemented with 10% FBS, 1% penicillin–streptomycin, and 1%
Dual laser system and PBM applications
Two types of laser devices were used to build a dual-laser system that delivers two different wavelengths simultaneously. A 655-nm diode laser device (PS4 III. LED; Changchun New Industries Optoelectronics Tech. Ltd., China) and 808-nm diode laser device (Teknofil, Türkiye) were used in an optical setup with various optomechanical instruments, focusing their beam to irradiate the cells seeded in the well plates placed on the optical breadboard. The laser spot areas exhibited spatial overlap when both laser systems were operated simultaneously. About 8 cm2 of spot area was illuminated by each laser system, adjusting the distance between the fiber tip and the well-plates where cells were seeded. The distance between the tip of the fiber and the plate was 9 cm for the 655-nm diode laser and 12 cm for the 808-nm diode laser (Fig. 1).
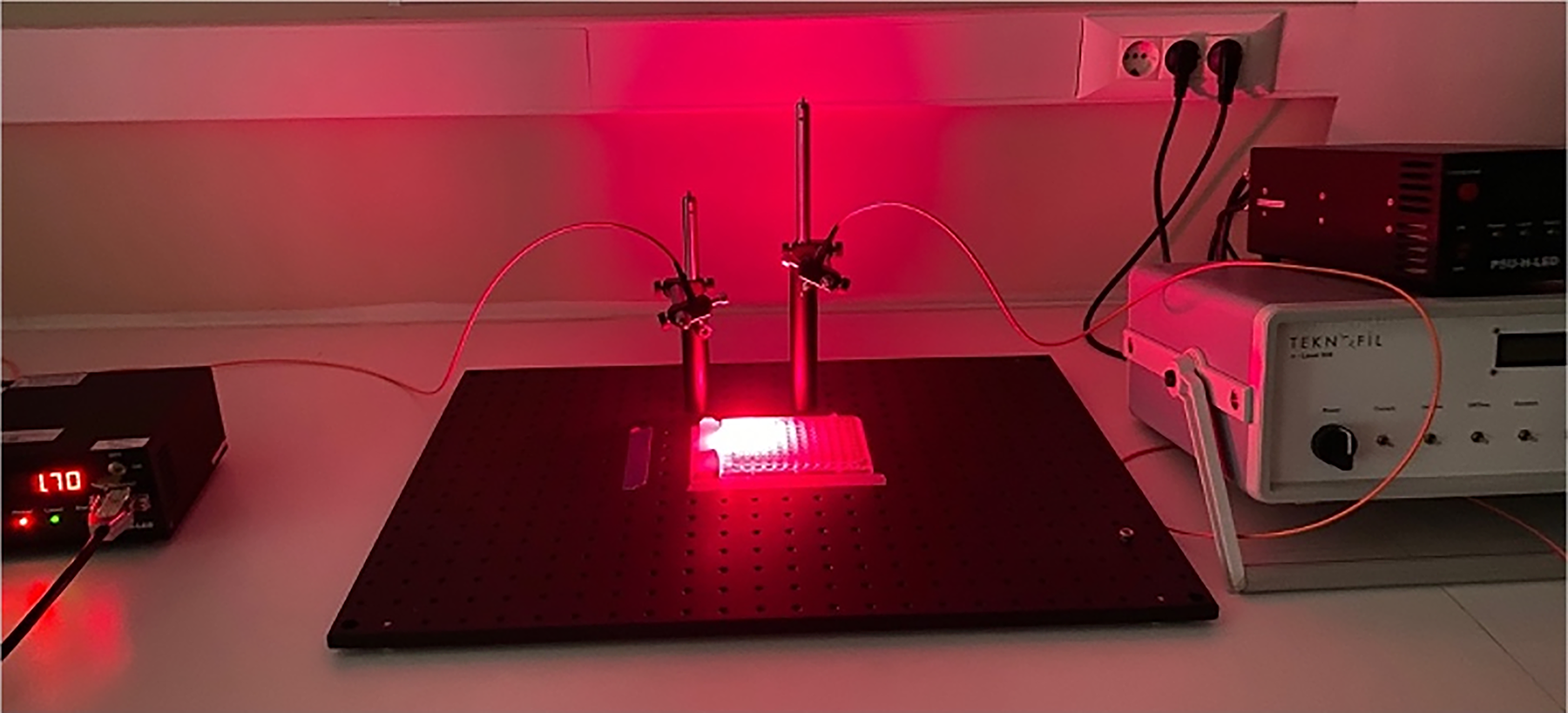
The setup of the dual laser system with 655 and 808 nm wavelength diode laser devices.
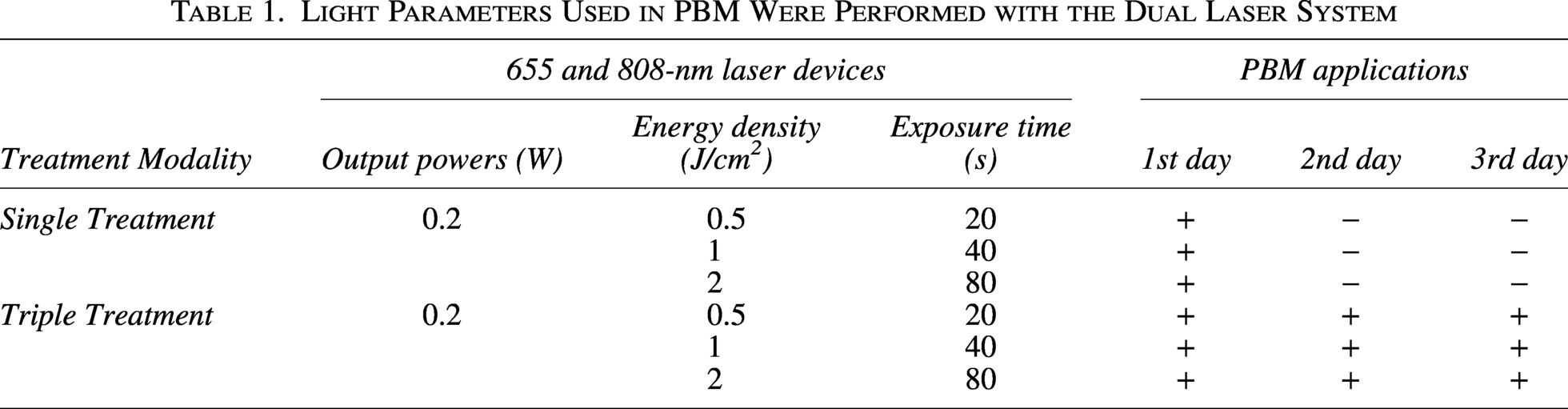
Light Parameters Used in PBM Were Performed with the Dual Laser System

The effect of PBM application using the dual laser system was investigated using two modalities: [1] single and [2] triple treatments. In the single-treatment modality, the cells were exposed to PBM only once, whereas in the triple-treatment modality, they were irradiated three times with 24 h intervals. During the irradiation, the same energy densities were applied with both wavelengths. Two main experimental groups were performed for each modality, as: (1)
Cell viability
The MTT assay was used to determine cell metabolic activity colorimetrically, assessed via the mitochondrial dehydrogenase enzyme. After performing PBM applications for both modalities (single and triple treatments), the 5 mg/mL MTT stock solution was diluted to 10% with culture medium lacking FBS and added to the cells. Cells were incubated for 2 h in a humidified atmosphere supplemented with 5% CO2 at 37°C. The MTT solution was removed, and cells were incubated with DMSO for 10 min in the dark. Then, absorbance values were recorded using a microplate reader (SynergyTM HTX Multi-Mode Microplate Reader, BioTek, USA). The data were normalized to the control and expressed as percentages.
ROS determination
ROS production after PBM applications, which affect cell proliferation, was determined using the DCFH-DA probe. After this probe passes into the cells, it is converted to the fluorescent compound DCF in the presence of ROS. Before performing the PBM applications, the culture medium above the cells was removed, and the cells were rinsed with PBS. Then, 100 µL of 100 µM DCFH-DA was added, and cells were incubated in the dark for 45 min. Then, the probe was discarded, fresh culture media were added, and cells were irradiated for PBM. The intracellular ROS levels were determined by measuring fluorescence at 528/20 nm under excitation at 485 nm.
Scratch assay
The scratch assay was utilized to determine wound healing in vitro. For this assay, L-929 cells were seeded on 24-well plates. The scratches were created in the middle of each well using the sterile 200 µL pipette tip, removing attached cells as a line. After creating scratches, cells were washed once with PBS to remove the detached cells. Fresh culture media were added, and PBM applications were performed for both modalities (single and triple). Scratches were observed for 3 days until the wounds completely closed. The images were captured at 10X magnification with an inverted microscope (Olympus, CKX41, JPN) and analyzed using ImageJ software (NIH, USA) to calculate the scratched area for each day until they closed.
Statistical analysis
All experiments were repeated three times with three samples. The collected data were normalized to the control group and represented as bars ± SD. The data obtained were analyzed using a Student’s t-test to evaluate differences between experimental groups. Statistically significant differences were found when the p value < 0.05.
Results
The effect of the dual laser system on L-929 cell viability
The single and triple treatments were applied separately to fibroblast cells using a dual-laser system at energy densities of 0.5, 1, and 2 J/cm2 for both wavelengths. The results of the MTT analysis are shown in Figure 2. Single treatments at energy densities of 0.5 and 1 J/cm2 slightly increased cell viability, but the increases were not statistically significant. The maximum increase of 2.73% was observed at an energy density of 1 J/cm2. However, cell viability decreased by 20.04% at an energy density of 2 J/cm2. On the other hand, triple treatment slightly reduced cell viability, which can be considered negligible, as the maximum decrease was only 7.70%.
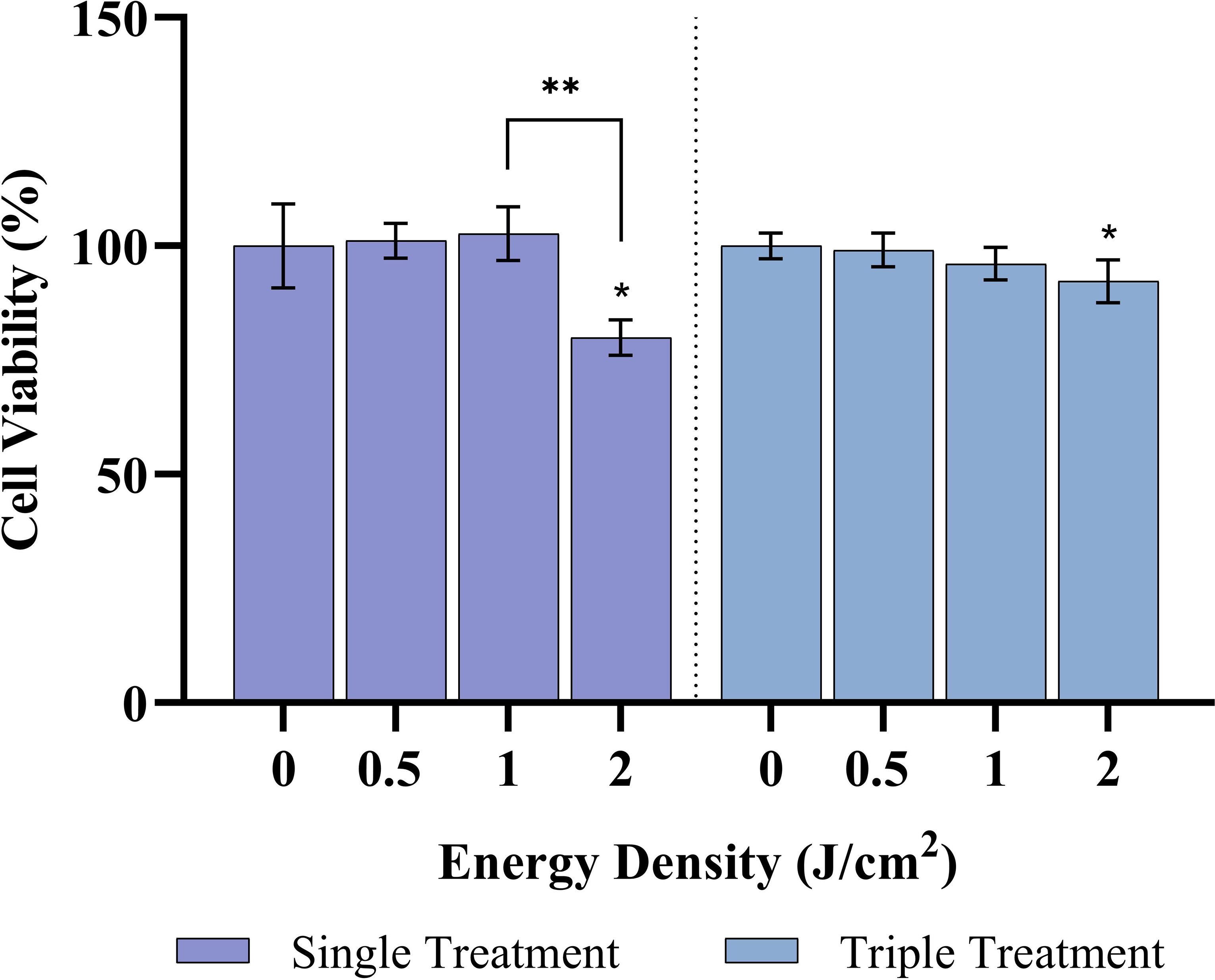
Cell viability analysis after dual-wavelength PBM applications with single and triple treatment. * and ** specify the statistically significant difference between the control and experimental groups and the difference between experimental groups, respectively (p < 0.05). PBM, photobiomodulation.
Intracellular ROS generation after irradiation with dual laser system
A DCFH-DA probe was used to assess ROS generation following both single- and triple-PBM treatments. After irradiation was completed, the fluorescence intensity was recorded immediately. As shown in Figure 3, dual-wavelength PBM with both treatment modalities (single and triple) increased ROS generation. The highest ROS levels were observed at energy densities of 1 and 2 J/cm2 in both treatments. The highest increase, 19.40%, was observed with triple treatment at an energy density of 1 J/cm2 compared to the control.
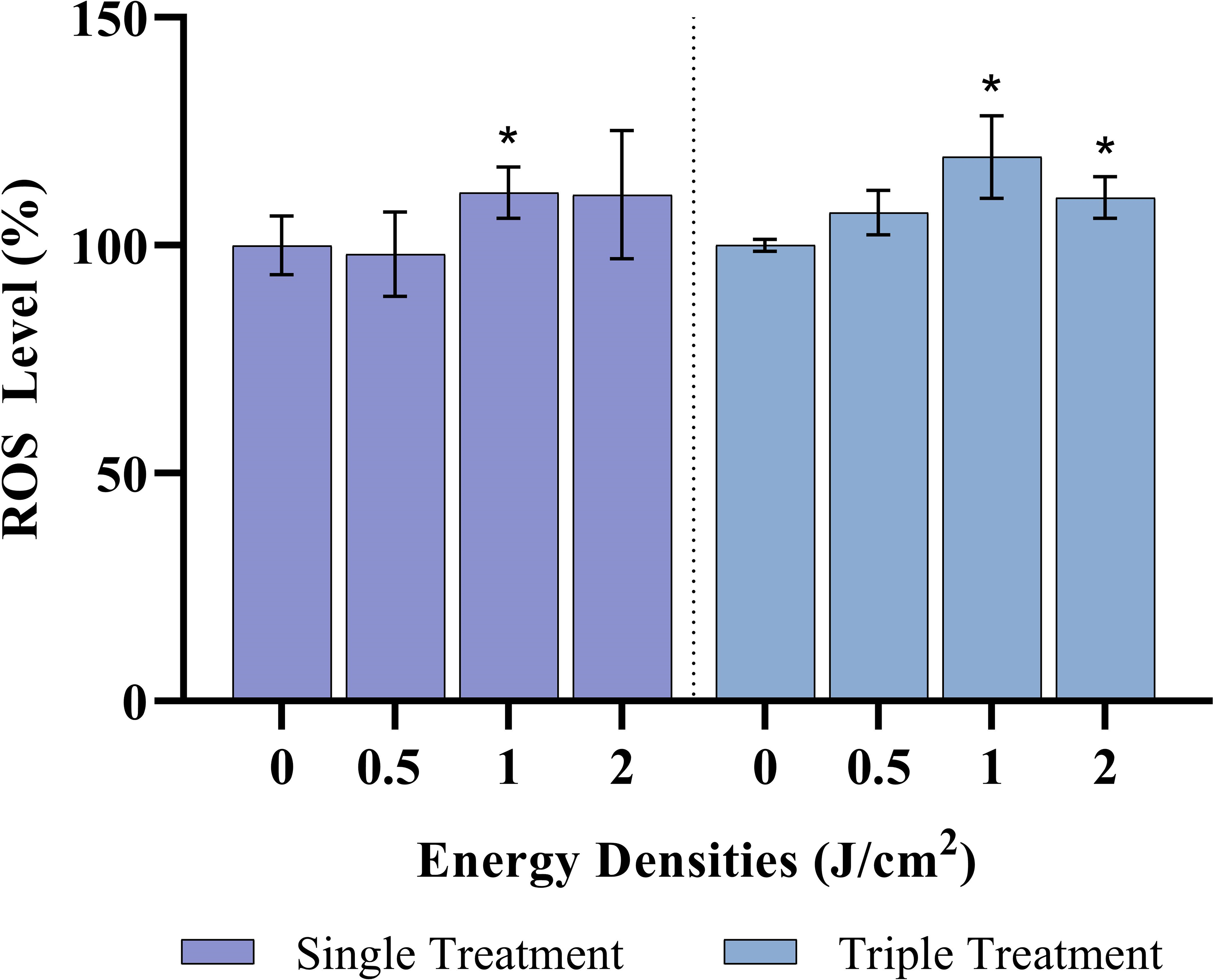
Percentage changes in intracellular ROS level after dual-wavelength PBM applications with single and triple treatment. * specifies statistically significant differences between control and experimental groups (p < 0.05). ROS, reactive oxygen species
Wound healing assessment in vitro
To determine the effect of the dual-wavelength application on wound healing, in vitro scratch models were created with L-929 cells. After the light irradiation to induce the PBM mechanism, the microscopic images of cells, together with their scratches, were taken from zero-day to the third day every 24 h. Dual-wavelength PBM application, whether single- or triple-treated, enhanced wound healing compared with the control. Figure 4a. reveals the wounds after a single PBM application and control. A single treatment with a dual laser system resulted in maximum closure, or in other words, minimum wound area, at an energy density of 1 J/cm2.
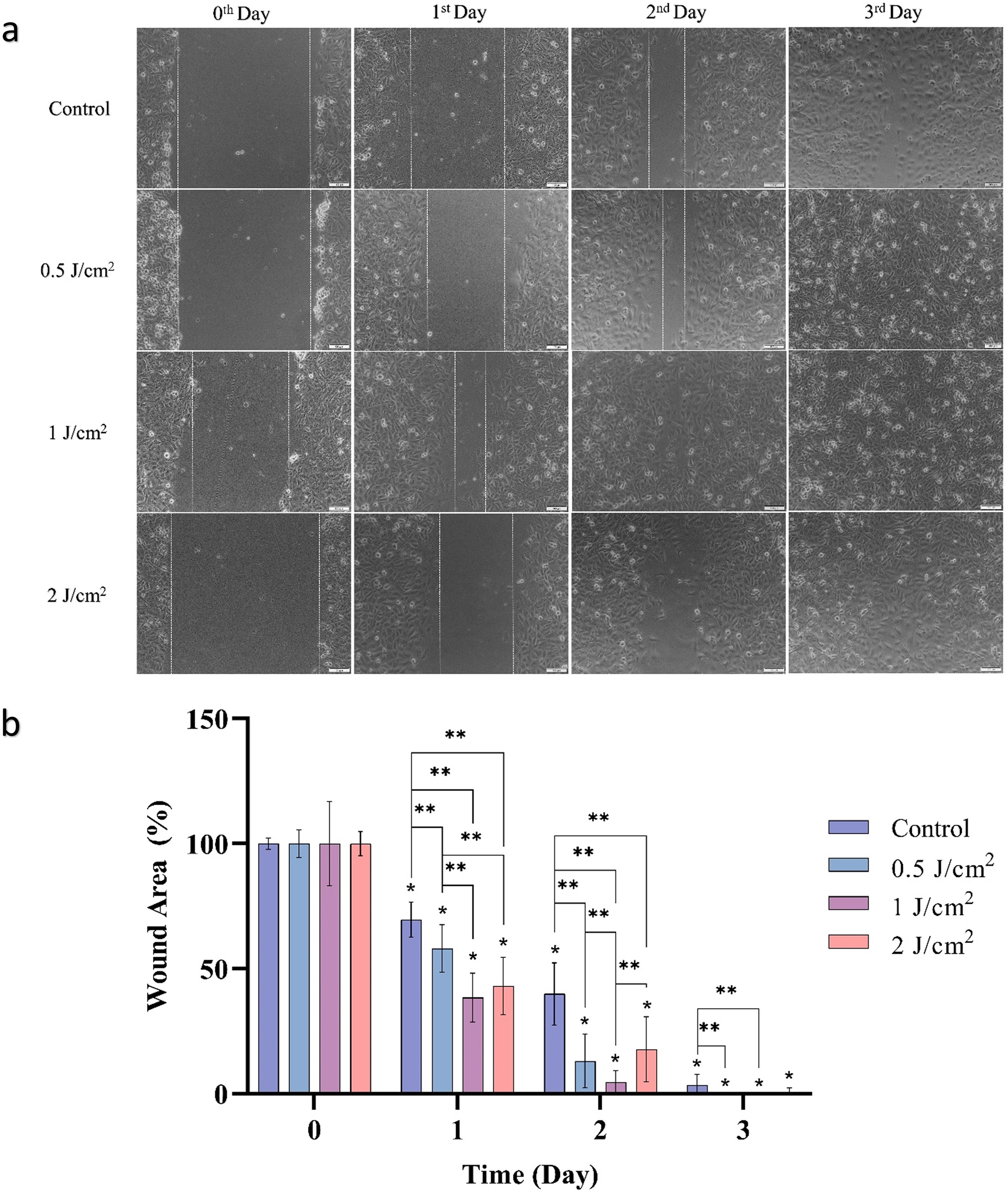
The percentage of wound area after the single dual-wavelength PBM treatment is shown in Figure 4b. Wound area was determined on the second day as 39.88%, 13.10%, 4.59%, and 17.78% for the control and at energy densities of 0.5, 1, and 2 J/cm2, respectively. By the end of the third day, these were 3.47%, 0.06%, 0%, and 0.76%, respectively. Based on both the microscopic images and wound areas, single PBM treatment at 1 J/cm2 energy density provided the fastest wound healing when both wavelengths were applied simultaneously.
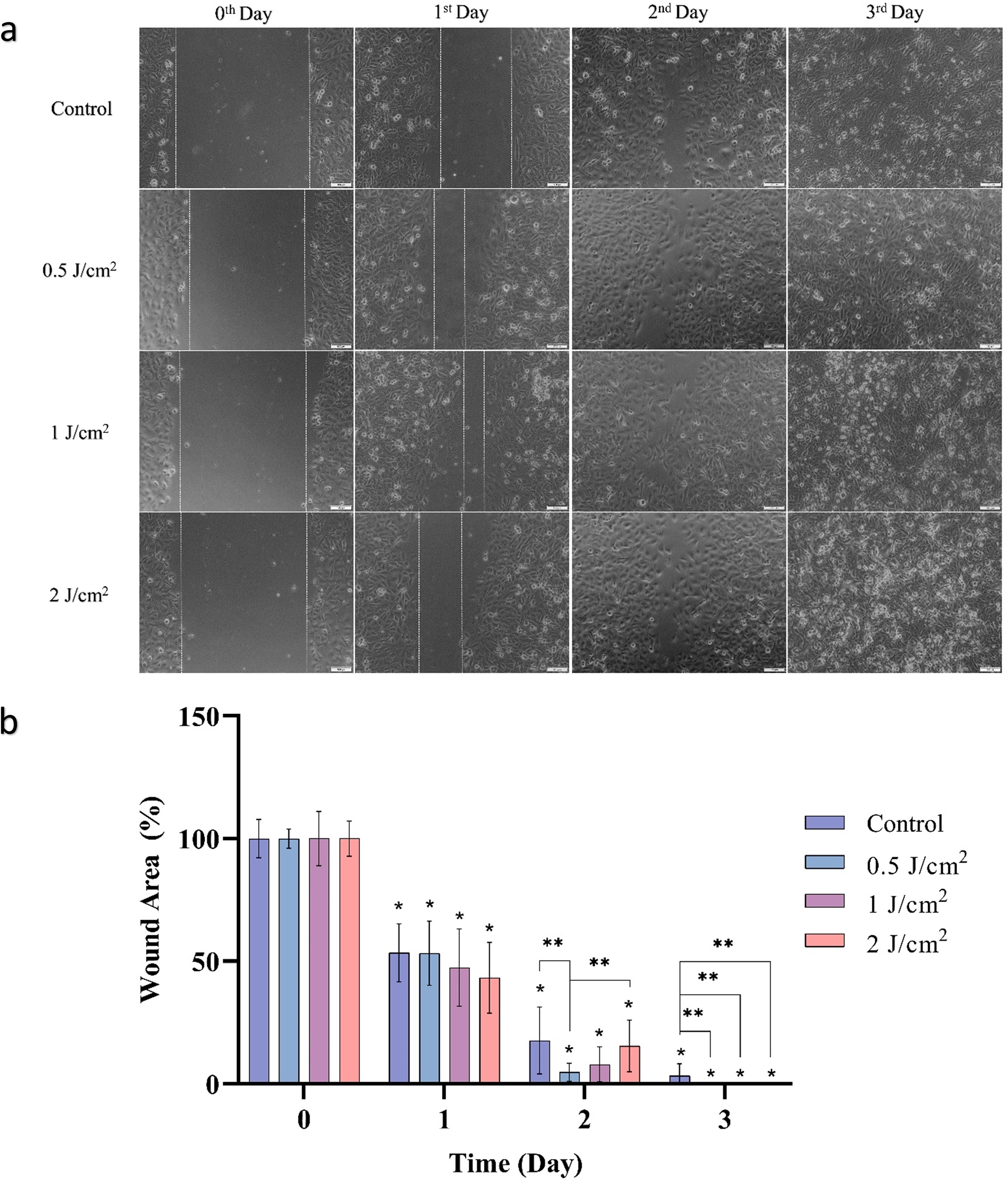
The microscopic images of the triple treatment are shown in Figure 5a and show the wound areas after PBM application and in the control. On the second day, the percentages of wound area measured in the control and after triple dual-wavelength PBM treatment at energy densities of 0.5, 1, and 2 J/cm2 were 17.68%, 4.77%, 7.94%, and 15.41%, respectively. Although the minimum wound area was observed at 0.5 J/cm2 energy density on the second day, Triple treatment with the dual laser system at 1 and 2 J/cm2 energy densities resulted in maximum wound closure (minimum scratched area) at the end of the third day (Fig. 5b).
Discussion
Wound healing is an important concept for complete recovery, and cell proliferation plays an essential role during the proliferation phase. Generally, using two different wavelengths for this therapy resulted in faster healing than therapy with a single wavelength, indicating a synergistic therapeutic effect.12–14 Although visible wavelengths resulted in better healing in vitro, the situation changes in vivo, where light penetration becomes more important. By combining red and NIR light for PBM, the light penetration in the superficial and also deeper layers of the skin can be achieved. Even the sequential and concurrent application of two different wavelengths could exhibit a synergistic effect.12,15–17 However, the sequential approach could increase treatment duration and hospitalization, underscoring the importance of concurrent application. In this study, the concurrent application of two wavelengths (655 and 808 nm) was evaluated in vitro. Among the three applied energy densities (0.5, 1, and 2 J/cm2), a single treatment with dual-wavelength PBM at 1 J/cm2 resulted in the greatest increase in cell viability, the highest intracellular ROS level, and the fastest wound closure compared to the control group. In our previous study, 655 and 808 nm of wavelengths were investigated separately on cell proliferation and wound closure capability of the fibroblasts and keratinocytes. In that study, an energy density of 5 J/cm2 was the most effective parameter for inducing accelerated wound healing. However, this energy density decreased cell viability, especially under NIR light exposure, indicating an adverse effect of the application. 18 In this study, a similar acceleration in wound healing was observed at an energy density of 1 J/cm2, and it also stimulated cell proliferation. Concurrent application provided an opportunity to reduce energy density, thereby minimizing adverse effects and promoting better healing outcomes. Triple dual-wavelength PBM treatment slightly reduced fibroblast cell viability in the present study. Despite this reduction in cell viability, increased intracellular ROS levels and accelerated wound closure were observed across all three energy densities compared to the control group. In particular, triple dual-wavelength PBM at 1 J/cm2 energy resulted in the maximum increase and accelerated wound closure. Even if the triple dual-wavelength PBM treatment did not increase cell proliferation, an enhanced therapeutic outcome was still observed. These results suggest that mechanistic changes, such as elevated ROS levels, play a significant role in promoting wound healing. The role of ROS metabolism can explain this. ROS play a role in almost every stage of healing, from hemostasis to maturation. Its elevated levels can upregulate the expression of tissue factor (the initiator of the coagulation pathway) in smooth muscle cells, leading to vasoconstriction. Also, ROS exhibited antimicrobial activity either directly or through the activation of signaling molecules, depending on their concentration. In addition, these reactive molecules regulate angiogenesis through mitogen-activated protein kinases and the phosphatidylinositol 3-kinase/Akt pathway, and stabilize hypoxia-inducible factor-1 alpha. ROS generation alone is not sufficient; their concentration is a critical determinant of biological outcomes. While moderate ROS levels can support tissue repair, excessive accumulation induces oxidative stress, which can impair and disrupt wound healing. Therefore, maintaining ROS within an optimal level is essential for promoting efficient and accelerated wound closure. 19 Although the increase in ROS levels due to triple dual-wavelength PBM may be sufficient to limit cell viability, it remains within a range that accelerates wound healing and regulates inflammation and angiogenesis. 20 While the increase in intracellular ROS is not markedly high, it can trigger the activity of antioxidant enzymes such as catalase and superoxide dismutase. 17 This, in turn, helps control the healing process and inflammation by reducing oxidative stress and cellular damage.
The role of ROS in wound-healing stages, such as platelet aggregation and angiogenesis, is crucial. It has been stated that a 40% increase in ROS levels is necessary for platelet activation. In the present study, concurrent PBM application with dual-wavelength light induced an approximately 20% increase in ROS, which is sufficient to contribute to platelet activation and accelerate platelet action. 21 Similar findings have been reported by Chen et al., who observed enhanced proliferation of embryonic skin fibroblasts with concurrent PBM application at 635 and 808 nm, accompanied by a slight increase in intracellular ROS levels, as observed in the present study. Moreover, they also observed an enhanced activity of antioxidant enzymes. 17 Likewise, McDaniel et al. observed increased expression of the Collagen 1A1 gene in human fibroblasts when the 870 and 590 nm wavelengths were applied simultaneously, compared with expression levels after each wavelength was applied separately. This is an important point that concurrent PBM application can affect gene expression, supporting the idea that it may enhance and accelerate the wound-healing process by promoting collagen synthesis and extracellular matrix remodeling. 22 Nevertheless, this study has some limitations, as it is far from in vivo models. Future studies should take this into account and investigate additional parameters to elucidate the mechanistic pathways altered by concurrent dual-wavelength PBM. Although this study was conducted in vitro, it expressed synergistic effects of concurrent PBM application in terms of intracellular ROS generation and scratch assay. Combining red and NIR wavelengths and optimizing doses to determine effective PBM parameters (such as output power, energy density, and exposure times) will provide information for in vivo and clinical studies. Based on the findings of this study, chronic wounds such as diabetic foot, venous leg, and pressure ulcers will be treated, reaching different tissue layers and potentially enhancing both superficial and deep wound healing.
Conclusion
Wound healing is an essential process for the body’s regeneration and repair. It is highly regulated by various pathways and biocompounds. 19 PBM has been used for wound healing, and many studies have explored its impact at a single wavelength. Although in vitro studies of concurrent PBM application for wound healing are limited, several clinical and in vivo studies have sought to address this issue. However, due to the biphasic response of the PBM, it is important to carefully determine the optimal parameters in vitro to enhance therapeutic outcomes in whole organisms. Dose optimization in vitro is important for preventing potential harm, saving time and money, and helping the design of in vivo models and clinical trials. On the whole, the simultaneous application of dual wavelengths is very limited. Therefore, the promising results of the present work can guide future research toward developing more effective PBM-based therapeutic strategies and highlight the importance of identifying the underlying mechanisms that elicit synergistic effects.
Authors’ Contributions
All authors contributed to the study’s conception and design. Material preparation, data collection, and analysis were performed by A. B. and B.S. The first draft of the article was written by B.S. All authors read, edited, and approved the final article.
Ethics Approval
This study does not involve any research with human participants or animals by any of the authors.
Consent
The authors affirm that they have reviewed and approved the content of the article and have given explicit consent for its submission for publication.
Data Availability and Materials
The datasets generated in this study are available from the corresponding author upon reasonable request.
Footnotes
Declaration of Competing Interest
The authors declare that they have no conflicts of interest with the contents of this article.
Funding Information
This study is supported by the Scientific and Technological Research Council of Turkey (TUBITAK) under Grant No: