
Abstract
Background:
Inferior alveolar nerve (IAN) sensory disturbance after mandibular third molar extraction can persist and affect speech, mastication, and quality of life. Photobiomodulation (PBM) has been used to promote peripheral nerve recovery, but the most suitable irradiation strategy remains unclear. Laser acupuncture (LA) delivers PBM to predefined acupoints and may provide both local and central neuromodulatory effects.
Objective:
To compare standardized LA with direct nerve-trajectory PBM for post-extraction IAN hypoesthesia in a randomized, double-blind, sham-controlled trial.
Methods:
Adults aged 18–60 years with unilateral IAN hypoesthesia lasting ≥7 days and ≤12 weeks were randomized (1:1:1) to LA, direct PBM along the external IAN projection, or sham treatment. All participants received mecobalamin (0.5 mg, three times daily) for 30 days. PBM was delivered using an 808-nm diode laser (continuous wave, 100 mW; beam area 1.0 cm2), 90 s/site (9 J; 9 J/cm2), every other day for 15 sessions. LA used a fixed 5 + 2 prescription: ST4, ST6, ST7, CV24, Jiachengjiang (EX-HN19), plus LI4 and PC6. Primary outcomes were two-point discrimination (TPD) and Semmes–Weinstein monofilament examination (SWME) at day 30. Secondary outcomes included Visual Analog Scale (VAS) numbness, additional sensory tests, and day-60 follow-up.
Results:
Sixty participants completed the intervention. Both active groups improved more than sham for TPD and SWME (group × time p < 0.01). Mean TPD change at day 30 was −3.2 ± 1.8 mm (LA) and −2.6 ± 1.7 mm (direct PBM) versus −0.8 ± 1.1 mm (sham). SWME improved by ≥1 grade in 85%, 80%, and 25%, respectively. VAS numbness decreased by 60%, 48%, and 12%, respectively, and the improvement was largely maintained at day 60. No treatment-related adverse events occurred.
Conclusions:
Under matched PBM dosimetry, both irradiation strategies improved sensory recovery compared with sham. LA produced comparable results and was associated with greater improvement in patient-reported numbness.
Keywords
Introduction
Inferior alveolar nerve (IAN) injury is a recognized complication of mandibular third molar extraction and may present as hypoesthesia, paresthesia, or dysesthesia of the lower lip and chin. Even when the deficit is mild, sensory disturbance can interfere with articulation, mastication, oral hygiene, and psychosocial well-being, and it frequently becomes a major source of postoperative dissatisfaction and anxiety. The reported incidence of IAN disturbance varies across populations and surgical difficulty, but clinically meaningful deficits remain an important complication in oral surgery practice.1–3
Most post-extraction IAN disturbances are consistent with neurapraxia or partial axonotmesis rather than complete transection, and spontaneous recovery is possible but often slow and unpredictable. Conventional approaches—including observation, corticosteroids, and neurotrophic vitamins—lack consistent evidence for accelerating functional recovery, and there is no universally accepted noninvasive therapy with reproducible benefit.2–4
Photobiomodulation (PBM), historically referred to as low-level laser therapy, has attracted interest as a potential adjunct for peripheral nerve injury. Mechanistic studies indicate that PBM can modulate mitochondrial signaling (including cytochrome c oxidase–associated pathways), increase ATP availability, influence reactive oxygen species and transcriptional responses, and promote anti-inflammatory effects and tissue repair.5–7 In peripheral nerve models, PBM has been associated with improved axonal regeneration, remyelination, and functional outcomes, potentially mediated through Schwann cell activity and neurotrophic factor signaling.8,9 In dentistry, PBM has been applied to postoperative neurosensory deficits with variable protocols and mixed results, in part because wavelength, dose, treatment sites, and reporting practices have differed substantially across studies.10,11
Laser acupuncture (LA) applies PBM to specific acupoints without needle penetration, offering a painless intervention that may combine local photochemical effects with the neurophysiological framework of acupuncture. In facial nerve disorders, LA feasibility and blinded trial designs have been reported, supporting its investigational use in neuromodulatory rehabilitation.12,13 For postoperative IAN paresthesia, a randomized clinical trial compared direct PBM and LA, but incomplete sham control and protocol heterogeneity in acupoint prescription and PBM parameters limited reproducibility and interpretation. 11 More broadly, the lack of standardized, explicitly justified acupoint prescriptions has long been recognized as a major weakness in acupuncture-related clinical trials, prompting reporting guidance such as Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA). 14
We therefore conducted a randomized, double-blind, sham-controlled clinical trial comparing two PBM strategies under identical dose parameters: standardized laser acupuncture using a fixed 5 + 2 acupoint set and direct PBM along the external projection of the IAN trajectory. By matching energy delivery and the number of treated sites, we aimed to isolate the effect of irradiation strategy rather than dosimetric variation. We hypothesized that laser acupuncture would be at least comparable to direct nerve-trajectory irradiation and that both active interventions would be superior to sham.11–14
Materials and Methods
Study design and ethics
This prospective, randomized, double-blind, sham-controlled clinical trial was conducted at the Department of Oral and Maxillofacial Surgery, Dalian Stomatological Hospital. The study was approved by the institutional ethics committee and registered at the International Traditional Medicine Clinical Trials Registry (ITMCTR2025001819). The trial was conducted in accordance with the Declaration of Helsinki and reported in line with the Consolidated Standards for Reporting Trials (CONSORT) principles, with acupuncture-specific reporting guided by STRICTA where applicable.14–16
Participants
Adults aged 18–60 years were eligible if they developed unilateral IAN sensory disturbance persisting for ≥7 days and ≤12 weeks after mandibular third molar extraction. Sensory impairment was confirmed at baseline by abnormal findings on Semmes–Weinstein monofilament examination (SWME; threshold grade ≥3.22) and/or two-point discrimination (TPD ≥7 mm) in the mental nerve distribution.17–20
Exclusion criteria included diabetes mellitus, systemic immune or neurologic disorders, pregnancy, photosensitivity, prior laser/acupuncture therapy for the current condition, and use of medications known to substantially affect nerve conduction.
Randomization and blinding
Participants were randomized in a 1:1:1 ratio to LA, direct PBM, or sham using a computer-generated randomization sequence prepared by an independent investigator not involved in treatment or outcome assessment. Allocation concealment was implemented using sequentially numbered, sealed opaque envelopes. Outcome assessors and participants were blinded to group assignment.
To maintain blinding integrity, each treatment visit included two standardized procedures: an “acupoint procedure” and a “nerve-trajectory procedure.” Depending on allocation, only one procedure delivered therapeutic laser, while the other used sham output; sham participants received sham output in both procedures. The device produced identical guide light and sound in all procedures, and only the independent allocator had access to output status.
Laser device and irradiation parameters
Interventions used a clinically certified 808-nm near-infrared diode laser system (Class IIIb; Hager & Werken GmbH & Co. KG, Duisburg, Germany). Parameters were reported according to PBM dose-reporting recommendations and were identical in the two active arms to focus the comparison on treatment location. 21 Output was 100 mW in continuous-wave mode, with a 1.0 cm2 beam area at the tissue surface. Each site received 90 s irradiation (9 J/site; 9 J/cm2). Output power was checked with a calibrated optical power meter. Continuous-wave delivery was selected to minimize parameter variability because the trial was designed to compare irradiation-location strategies rather than pulse structure; current evidence is insufficient to establish pulsed delivery as superior for post-extraction IAN sensory recovery. Treatments were administered every other day for 15 sessions over 30 days. The probe was held perpendicular to the skin with gentle contact, and points were pre-marked to maintain positioning. All participants received mecobalamin 0.5 mg three times daily for 30 days.8,9,11
Interventions
In the laser acupuncture group, PBM was delivered to a fixed seven-point prescription at each visit: five orofacial points (ST4, ST6, ST7, CV24, and Jiachengjiang/EX-HN19) plus two distal points (LI4 and PC6) (Fig. 1). Meridian point locations followed the World Health Organization Standard Acupuncture Point Locations and GB/T 12346-2006; Jiachengjiang localization followed GB/T 40997-2021.22–24 The fixed prescription was selected a priori to cover the mental nerve sensory territory through local points while preserving a standardized local-plus-distal structure. PC6 was included as a distal modulatory point rather than a trigeminally specific local point.14,22–25
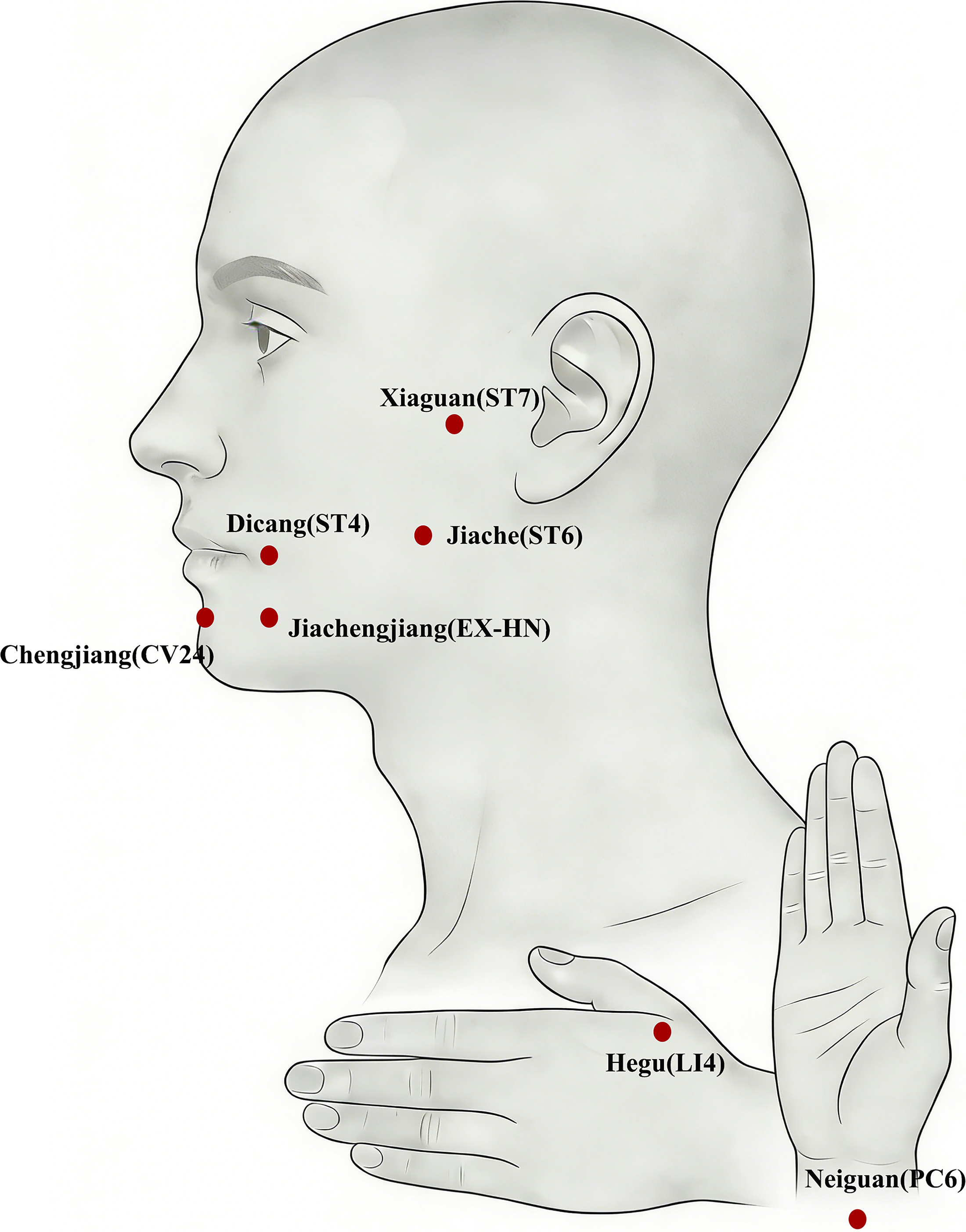
Standardized acupoint locations used for laser acupuncture. Standardized acupoint locations used for laser acupuncture in the treatment of inferior alveolar nerve hypoesthesia. Facial acupoints (ST4, ST6, ST7, CV24, EX-HN) and distal acupoints (LI4 and PC6) are shown on the affected side. Acupoint localization followed the World Health Organization Standard Acupuncture Point Locations to ensure reproducibility.
In the direct PBM group, the same parameters and number of irradiation sites were used along seven predefined points on the external projection of the IAN/mental nerve pathway, including the mental foramen region, mandibular body, and ascending ramus. (FIG. 3). The sham group received identical procedures with no therapeutic laser output. To reduce operator variability, treating clinicians completed structured training supervised by a senior traditional Chinese medicine practitioner, and all treatment points were marked before each session; deviation from the marked point was restricted to ≤3 mm.
Outcome measures
Primary outcomes were TPD (mm) and SWME grade at day 30. Secondary outcomes were VAS numbness (0–10), pinprick and brush-stroke discrimination, thermal discrimination, and exploratory pulp vitality testing of the ipsilateral mandibular first molar. Assessments were performed at baseline; after the 1st, 3rd, 7th, 11th, and 15th sessions; and at day 60. The same blinded examiner performed tests in a fixed sequence.18–20
Statistical analysis
Continuous outcomes were summarized as mean ± standard deviation. Group-by-time effects were analyzed using repeated-measures analysis of variance with Bonferroni-adjusted post hoc comparisons where applicable. Categorical outcomes were compared using chi-square or Fisher’s exact tests. Statistical significance was set at p < 0.05.
Results
Participant flow and baseline characteristics
Eighty-five patients with postoperative IAN sensory disturbance were screened. Sixty met eligibility criteria and were randomized to LA, direct PBM, or sham control (n = 20 each; Fig. 2). All randomized participants completed the 15-session intervention and provided day-30 primary endpoint data. At day 60, three participants, one in each group, were unavailable; day-60 outcomes were analyzed using available-case data. Baseline demographic and clinical characteristics were comparable among groups, including age, sex, time from extraction to enrollment, affected side, baseline TPD, SWME grade, and VAS numbness (all p >0.05; Table 1).
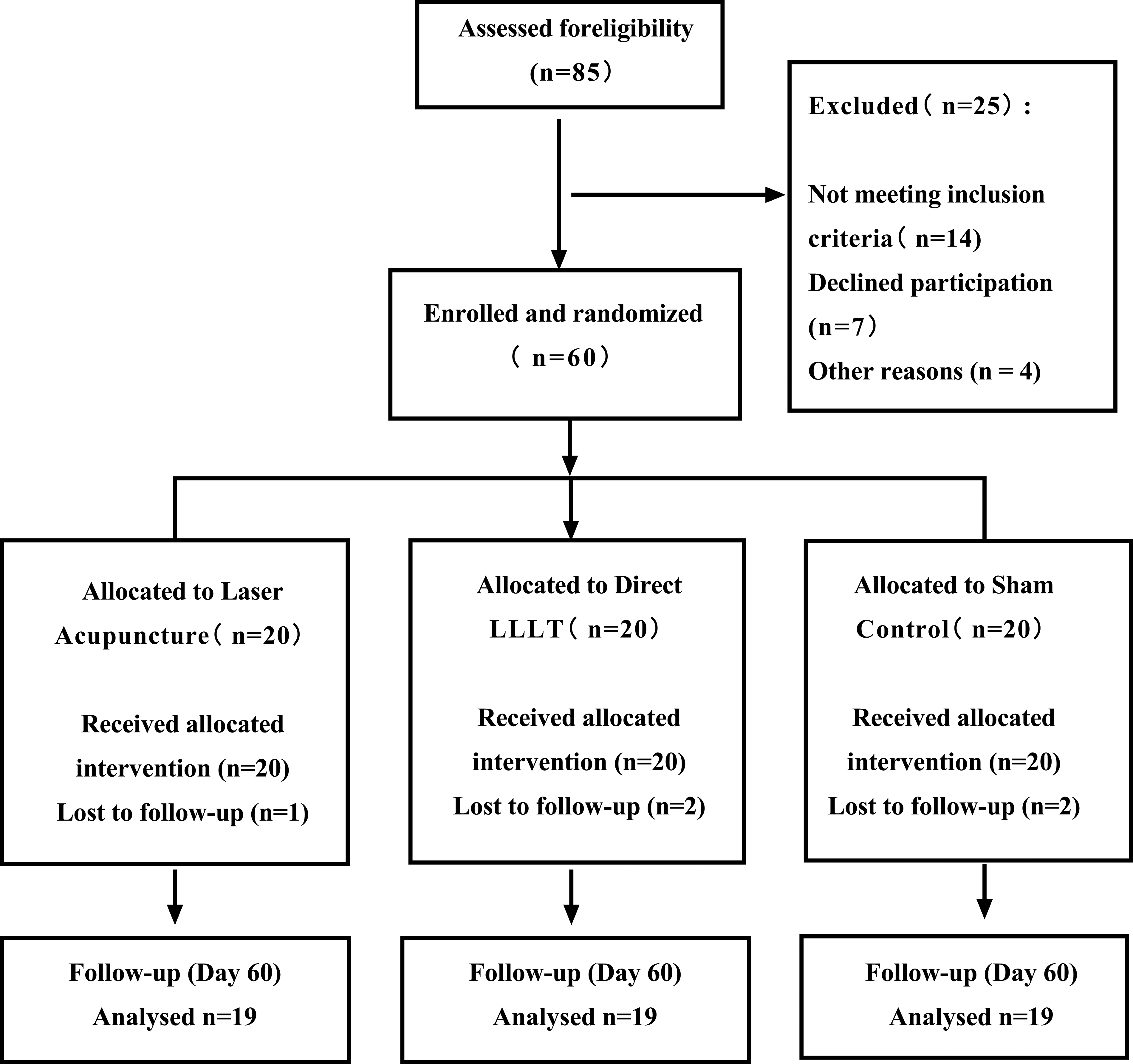
CONSORT flow diagram of the study. CONSORT flow diagram illustrating patient enrollment, randomization, allocation, follow-up, and analysis in this randomized, double-blind, sham-controlled clinical trial.
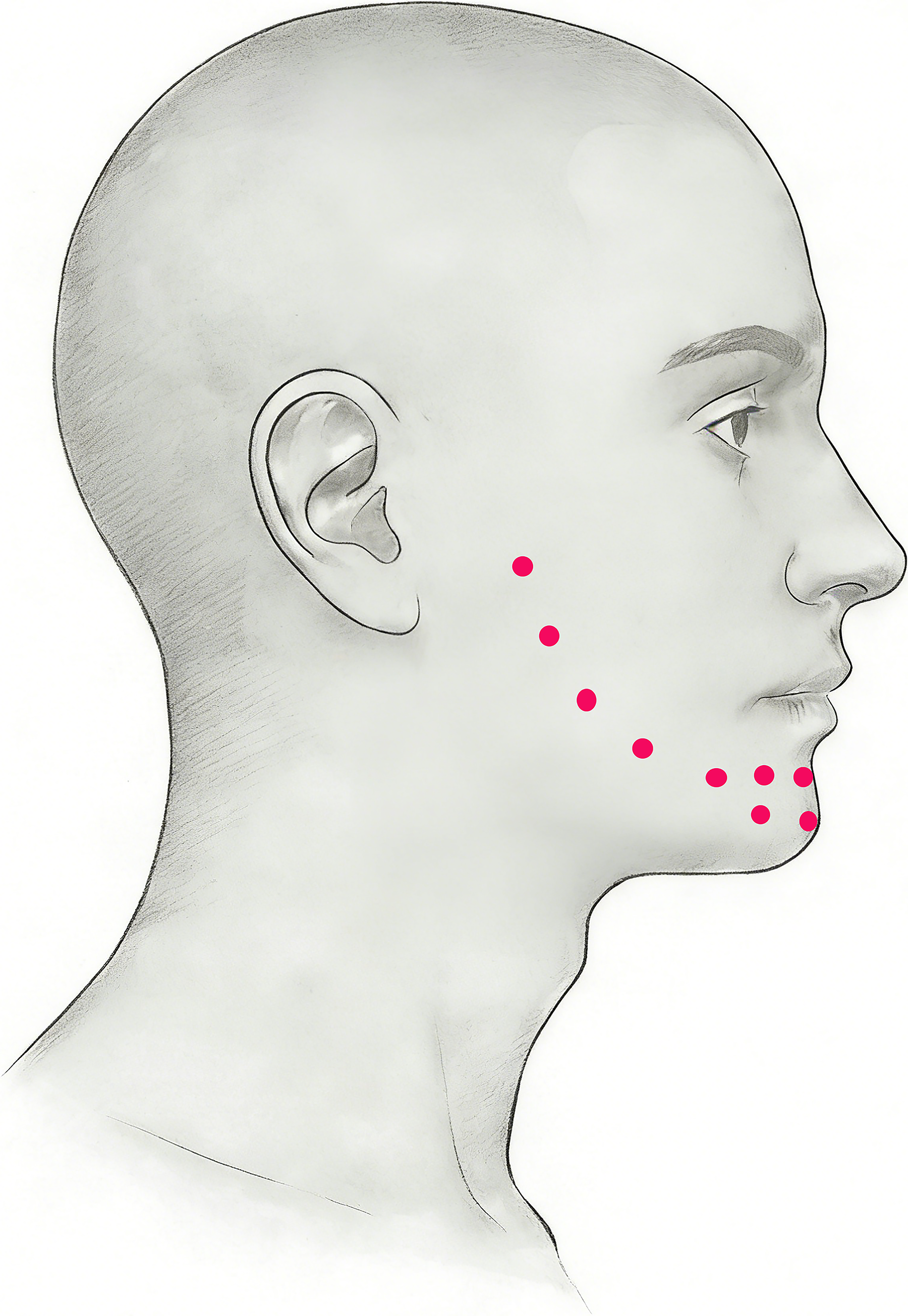
Laser irradiation sites for the direct photobiomodulation (PBM) group. Laser irradiation sites along the projected anatomical course of the inferior alveolar nerve for the direct PBM group.
Baseline Demographic and Clinical Characteristics of Participants
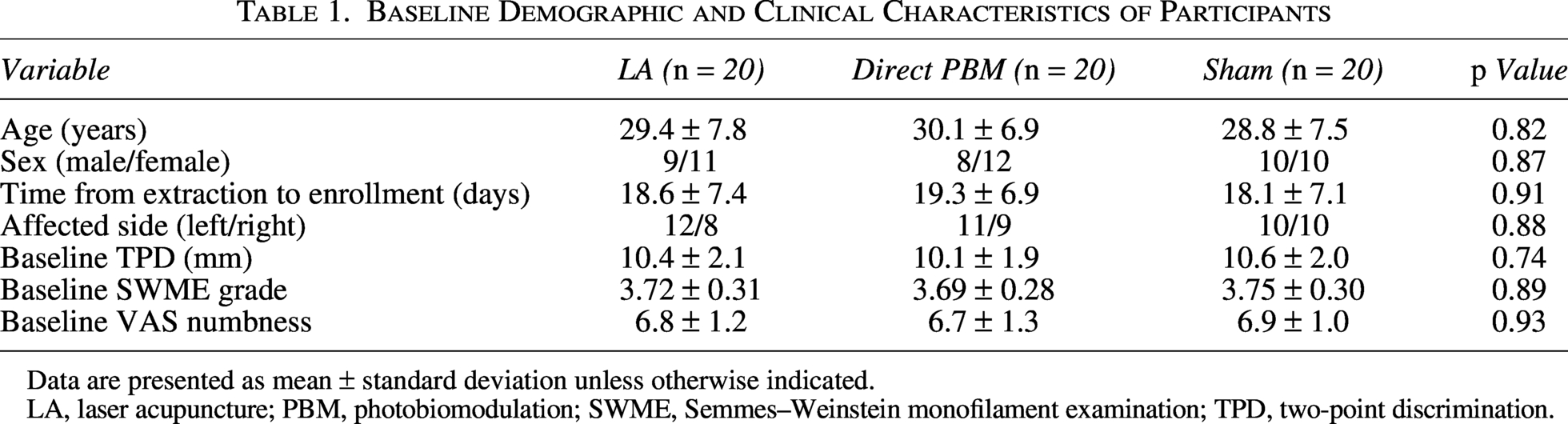
Data are presented as mean ± standard deviation unless otherwise indicated.
LA, laser acupuncture; PBM, photobiomodulation; SWME, Semmes–Weinstein monofilament examination; TPD, two-point discrimination.
Primary outcomes
TPD improved in both active groups but changed only modestly in the sham group (Table 2 and Fig. 4). At day 30, mean TPD decreased from 10.4 ± 2.1 to 7.2 ± 1.6 mm in the LA group and from 10.1 ± 1.9 to 7.8 ± 1.7 mm in the direct PBM group, compared with 10.6 ± 2.0 to 9.8 ± 1.9 mm in the sham group. Repeated-measures analysis showed a significant group × time interaction (p < 0.001). The benefit was largely maintained at day 60.
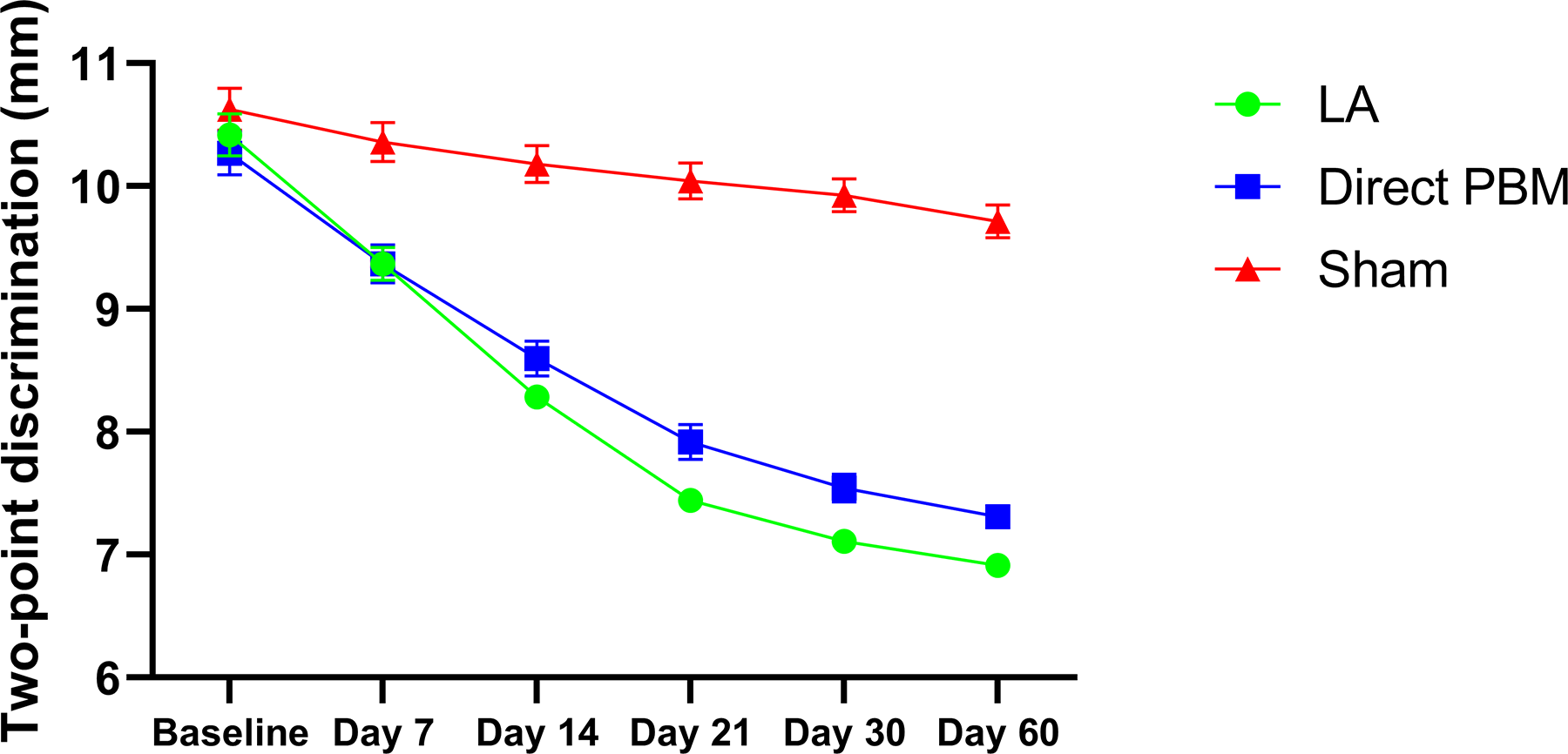
Changes in two-point discrimination (TPD) over time. Time course of TPD measurements in the laser acupuncture, direct photobiomodulation, and sham groups from baseline to the 60-day follow-up. The plotted values represent group means at each time point, and error bars indicate standard error. Lower TPD values indicate improved spatial discrimination.
Changes in Primary and Secondary Sensory Outcomes During Treatment and Follow-Up
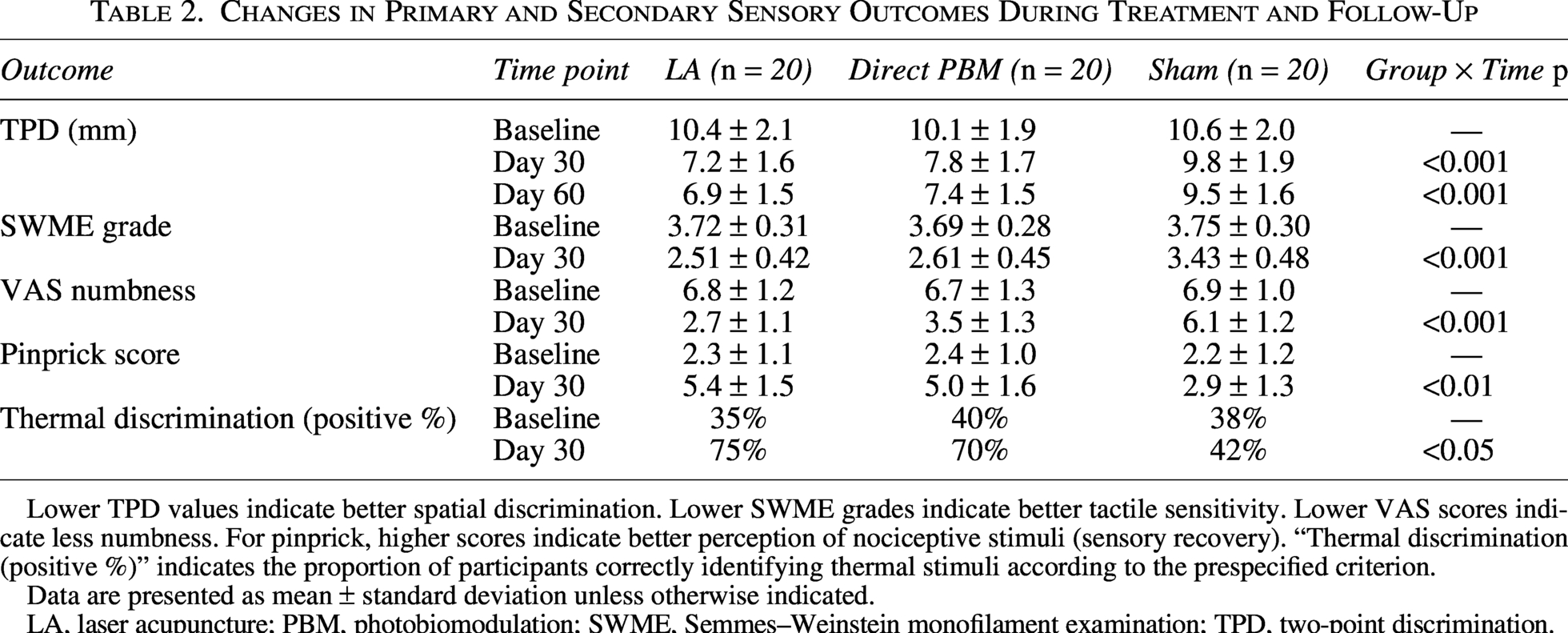
Lower TPD values indicate better spatial discrimination. Lower SWME grades indicate better tactile sensitivity. Lower VAS scores indicate less numbness. For pinprick, higher scores indicate better perception of nociceptive stimuli (sensory recovery). “Thermal discrimination (positive %)” indicates the proportion of participants correctly identifying thermal stimuli according to the prespecified criterion.
Data are presented as mean ± standard deviation unless otherwise indicated.
LA, laser acupuncture; PBM, photobiomodulation; SWME, Semmes–Weinstein monofilament examination; TPD, two-point discrimination.
SWME outcomes showed a similar pattern (Tables 2 and Table 3; Fig. 5). By day 30, SWME grade improved more in both active groups than in sham (group × time p < 0.001). Using the predefined responder criterion of ≥1-grade improvement, 85% of participants in the LA group and 80% in the direct PBM group responded, compared with 25% in the sham group (p < 0.001). Return to normal/protective tactile sensation occurred in 40%, 35%, and 5% of participants, respectively (p = 0.004).
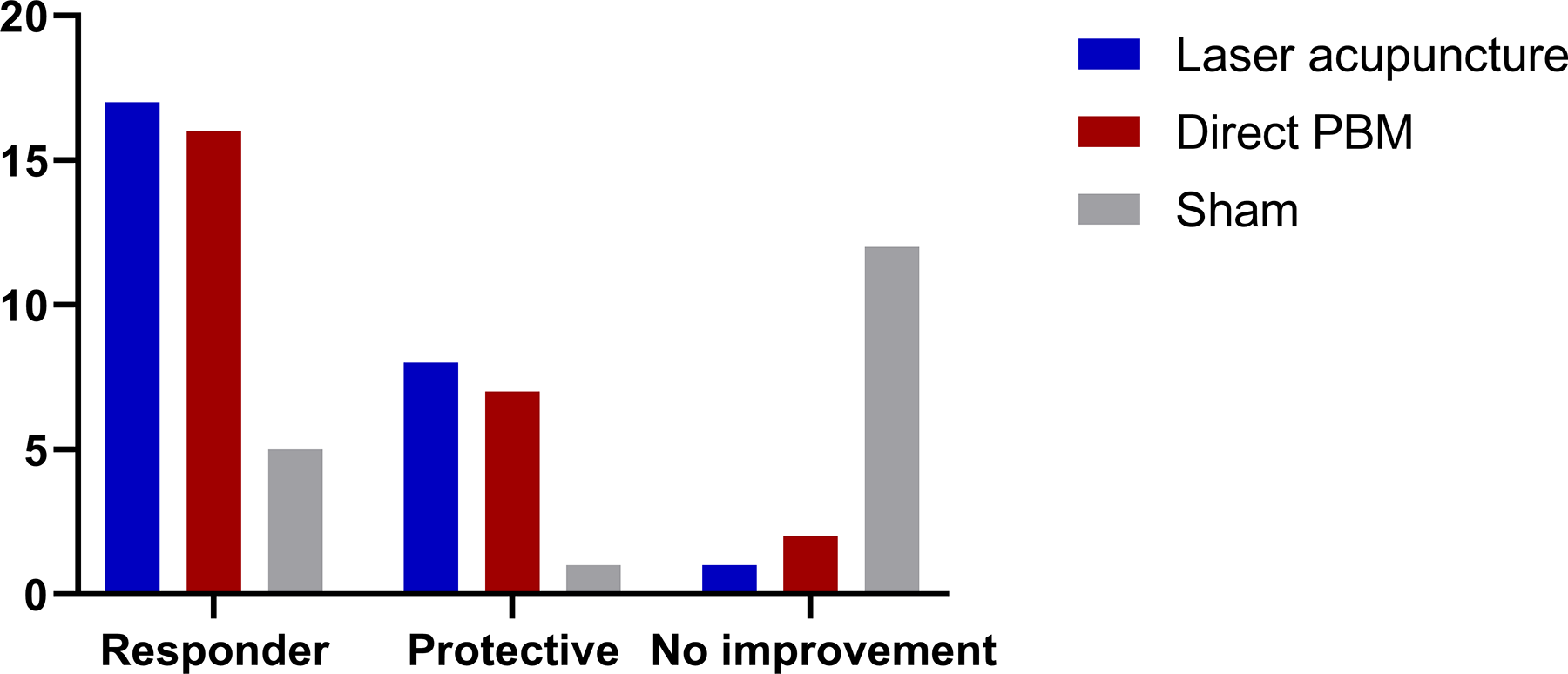
Improvement in Semmes–Weinstein monofilament examination (SWME) grades. Categorical recovery outcomes based on the SWME at day 30 in the laser acupuncture, direct photobiomodulation, and sham groups.
Categorical Improvement in Semmes–Weinstein Monofilament Examination
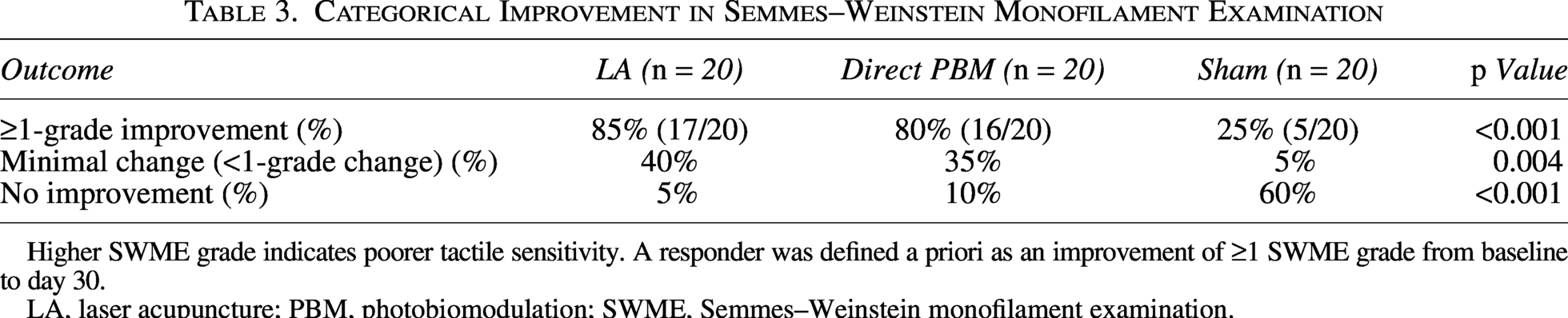
Higher SWME grade indicates poorer tactile sensitivity. A responder was defined a priori as an improvement of ≥1 SWME grade from baseline to day 30.
LA, laser acupuncture; PBM, photobiomodulation; SWME, Semmes–Weinstein monofilament examination.
Secondary outcomes
VAS numbness decreased more in the two active groups than in the sham (group × time p < 0.001), with a numerically larger reduction in the LA group (Table 2). Pinprick perception and thermal discrimination also improved more frequently after active treatment than after sham (p < 0.01 and p < 0.05, respectively). No adverse events were reported, and no participant discontinued treatment because of discomfort or symptom worsening. Session completion and medication compliance were high across all groups (Table 4).
Safety and Treatment Compliance
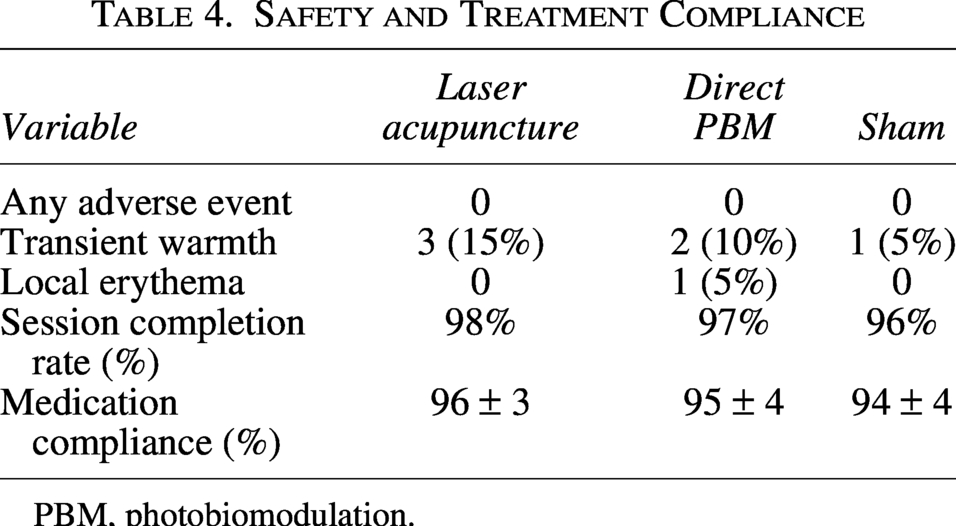
PBM, photobiomodulation.
Discussion
This randomized, double-blind, sham-controlled trial showed that both LA and direct nerve-trajectory PBM improved neurosensory recovery after IAN hypoesthesia following mandibular third molar extraction, compared with sham. Across objective discrimination thresholds and tactile testing, the two active strategies produced broadly comparable improvements, while patient-reported numbness showed a numerically greater reduction in the LA group. These results suggest that acupoint-based PBM may be a practical noninvasive option for postoperative IAN sensory disturbance.
Post-extraction IAN hypoesthesia is usually related to compression, traction, edema, or inflammatory injury rather than complete transection. Recovery therefore depends on resolution of local inflammation, remyelination, axonal repair, and functional reorganization within the trigeminal somatosensory system.2–4 PBM may contribute to this process through mitochondrial activation, improved cellular energy availability, anti-inflammatory effects, and modulation of repair pathways.5–7 Experimental studies further suggest effects on Schwann cell activity, neurotrophic signaling, and remyelination, which are directly relevant to recovery from neurapraxia or partial axonotmesis.8,9 The greater improvement in both active groups than in the sham is consistent with a treatment-related contribution beyond spontaneous recovery, although spontaneous improvement remains an important background process in this condition.
A key feature of this trial was that PBM parameters, number of treatment sites, and treatment schedule were matched between active groups. This design reduces a common source of bias in PBM studies, in which differences in wavelength, energy, spot size, and exposure time make it difficult to attribute outcomes to the intended therapeutic strategy. 21 Direct PBM attempts to irradiate tissues near the injured IAN, but surface projection of the mandibular canal is imprecise and varies with mandibular anatomy and soft-tissue thickness. LA instead uses reproducible surface landmarks and may engage both local orofacial afferents and broader neuromodulatory pathways. The comparable objective recovery observed here suggests that clinically meaningful improvement may not require irradiation directly over the presumed nerve course, provided that PBM dose and treatment frequency are standardized.
The fixed 5 + 2 acupoint protocol was designed to balance biological plausibility with reproducibility. ST4, ST6, ST7, CV24, and Jiachengjiang were chosen to cover the lower facial and mental nerve sensory territory, while LI4 and PC6 provided a predefined distal component commonly used in acupuncture practice for orofacial symptoms.22–25 We retained Jiachengjiang as a fixed, rather than optional, point to improve coverage of the mental region without allowing individualized point selection to introduce within-group variability. PC6 was not intended as a trigeminally specific point; its role was to preserve a standardized local-plus-distal structure and support central/autonomic modulation. This approach is consistent with STRICTA’s emphasis on transparent reporting and reproducible acupoint selection. 14
The possible advantage of LA for subjective numbness deserves cautious interpretation. VAS numbness captures not only tactile threshold but also perceived sensory discomfort, attention to the affected region, and affective response to persistent hypoesthesia. Acupuncture-related stimulation has been shown to modulate brain regions involved in somatosensory integration, affective processing, and pain regulation.26–28 Thus, LA may combine peripheral PBM effects with central neuromodulatory influences, potentially explaining why patient-reported symptoms appeared to improve slightly more than objective thresholds. Nevertheless, this study was not powered to prove superiority between the two active strategies, and the between-active-group difference should be regarded as exploratory. The numerical advantage of LA for VAS numbness should therefore be considered hypothesis-generating rather than confirmatory, but it provides a clinically relevant signal for designing larger trials.
Because early intervention for IAN hypoesthesia is often decided in outpatient settings before definitive prognostic information is available, a protocol that is simple, noninvasive, and repeatable has practical value. In our study, the treatment time, total energy, and contact procedure were deliberately kept identical between the two active groups, while sham exposure reproduced the visible and auditory cues of treatment. This design does not eliminate all procedural placebo effects, but it makes the comparison more clinically interpretable and reduces the risk that differences are merely caused by unequal treatment intensity.
From a clinical standpoint, these results may help physicians counsel patients who present with early sensory disturbance after third molar surgery. The goal of treatment is not only to reduce measured sensory thresholds but also to shorten the period of uncertainty during which patients are worried about permanent numbness. A standardized laser-acupuncture protocol may be easier to explain, schedule, and repeat than individually adjusted irradiation patterns. It also avoids needle insertion, which is relevant for patients who are anxious after a surgical complication. These pragmatic considerations do not replace efficacy data, but they strengthen the rationale for testing this protocol in broader clinical settings. In daily practice, this also means that clinicians can document a prespecified protocol, improve treatment consistency, and reduce disputes related to subjective selection of treatment sites.
The findings also fit with the broader literature showing that PBM protocols for oral neurosensory problems remain heterogeneous and incompletely standardized. Recent reviews have emphasized uncertainty regarding optimal dosage, timing, and treatment site selection for iatrogenic trigeminal nerve paresthesia and third molar-related outcomes.29,30 Our data suggest that a fixed acupoint protocol with explicit beam area, energy per point, and treatment schedule is feasible and reproducible in routine outpatient practice. This may be particularly useful where precise nerve-trajectory projection is difficult or where clinicians prefer a standardized protocol that can be taught and replicated across centers.
Several limitations should be acknowledged. This was a single-center study with a moderate sample size and a 60-day follow-up; longer observation is needed to determine whether early recovery translates into durable sensory normalization. Clinical neurosensory testing was used as the primary assessment, whereas electrophysiological testing, magnetic resonance neurography, and quantitative sensory testing could provide complementary objective endpoints.17–20 Dose–response relationships, alternative wavelengths, pulsed delivery, and combined PBM plus neurosensory retraining should also be examined. Finally, although the sham design and matched procedures strengthened internal validity, complete blinding of operator output status is difficult in procedural laser trials and should be addressed with independent device programming in future multicenter studies.
Conclusions
Under identical PBM parameters, both LA and direct nerve-trajectory PBM improved post-extraction IAN sensory recovery compared with sham. A standardized 5 + 2 acupoint protocol produced objective recovery comparable to direct irradiation and may offer a reproducible, clinically practical approach for postoperative neurosensory disturbance. Larger multicenter studies with longer follow-up and more objective sensory endpoints are warranted.
Authors’ Contributions
Y.Q.M.: Conceptualization, methodology, investigation, supervision, and writing—review and editing. M.M.Y.: Data curation, formal analysis, visualization, and writing—review and editing. J.S.: Project administration, resources, and provided supervision.
Footnotes
Acknowledgments
The authors would like to thank Dr. Shenyi Liu for professional guidance on acupoint selection and standardized localization in the LA protocol. They also thank the clinical staff of the Department of Oral and Maxillofacial Surgery, Dalian Stomatological Hospital, for their assistance with participant coordination and follow-up assessments.
Informed Consent Statement
Written informed consent was obtained from all participants prior to enrollment. For any identifiable images (if applicable), separate written consent for publication was obtained.
Ethical Approval
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Ethics Committee of Stomatological Hospital of Dalian University (Approval No. DLKQLL20250203). The trial was registered at the International Traditional Medicine Clinical Trials Registry (ITMCTR2025001819).
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
This research was supported by the 2024 Dalian Life and Health Guidance Program (Project No. 2024ZDJH01PT174).The funding body had no role in the study design, data collection, data analysis, manuscript preparation, or decision to publish.