
Abstract
Background:
Lumbar disc herniation (LDH) is a prevalent major cause of low back pain and radicular syndromes in the lower extremities. Elevated disc herniation volumes and the subsequent progression of spinal canal compromise are positively correlated with higher severity of radicular symptoms, functional disability, and neurological deficits.
Objective:
To investigate the impact of high-intensity laser therapy (HILT) on disc size and functional outcomes in patients with LDH.
Methods:
This study enrolled 40 patients of both sexes (40% male and 60% female), ages from 30 to 45 years, all presenting with lumbosacral radiculopathy secondary to L4–L5 or L5–S1 disc herniation. Participants were randomly assigned to two equal groups. Group A (study group) received HILT group treated with a combined standard physical therapy exercise program, while Group B (control group) underwent a sham HILT procedure alongside the same physical therapy exercise program. Interventions were conducted three times a week over 6 weeks. The primary outcome was the change in disc herniation size in anteroposterior, transverse, and posterior vertical diameter as measured by magnetic resonance imaging. The secondary outcomes included pain intensity assessed by the visual analogue scale (VAS) and functional disability assessed by the Oswestry Disability Index (ODI).
Results:
The HILT group demonstrated statistically significant reductions in all disc size parameters compared to the control group (p < 0.05). Additionally, the HILT group showed significantly higher reduction in VAS scores (63.88% vs. 26.04%) and ODI scores (53.5% vs. 24.58%) compared with the control group (p < 0.001).
Conclusion:
HILT serves as a potent noninvasive modality for reducing the herniated lumbar discs size and providing significant pain relief and improving functional outcomes in individuals with lumbosacral radiculopathy.
Keywords
Introduction
Lumbar disc herniation (LDH) is a condition characterized by the displacement of nucleus pulposus material beyond the intervertebral disc space, potentially resulting in compression or irritation of adjacent neural structures. This displacement frequently results in the compression of adjacent neural structures, manifesting clinically as low back pain (LBP) and radiculopathy. 1 LDH is considered a significant public health concern because of its high prevalence and its impact on functional ability and quality of life. primarily occurring among people between their 30 s and 50 s. 2 The associated pain, sensory impairments, and motor deficits contribute significantly to functional disability and a diminished quality of life.
LDH can be managed using different therapeutic approaches, including conservative rehabilitation, pharmacological treatment, and surgical procedures. Conservative treatments are primarily designed to mitigate pain and inflammation while restoring functional capacity. 3 Recent advancements in clinical practice have seen the burgeoning adoption of HILT as a noninvasive therapeutic modality, primarily attributed to its superior depth of tissue penetration and its capacity to elicit favorable photobiomodulation responses. 4 The hypothesized mechanisms of HILT include potent anti-inflammatory actions, the downregulation of proinflammatory cytokines, enhanced microcirculation, analgesia mediated by endorphin release, and the acceleration of the tissue repair process. 5
Although several studies have documented the analgesic and anti-inflammatory properties of HILT, evidence concerning its direct influence on the morphological structure of herniated discs remains sparse. MRI is considered the most reliable diagnostic tool for detecting lumbar disc abnormalities and determining both herniation dimensions and neural compression. 6 Objective measurement of disc regression through MRI provides crucial evidence for the potential therapeutic efficacy of HILT beyond symptomatic relief. Therefore, the present randomized controlled trial (RCT) was carried out to investigate the impact of HILT on MRI-assessed Disc herniation dimensions and functional outcomes in patients with lumbosacral radiculopathy. 7
Materials and Methods
Study design
This is a single-blind randomized controlled design that took place between 2024 and May 2025 at the Physical Therapy Department of the New Cairo Medical Complex, Ministry of Interior.
Participants
Forty patients were recruited randomly upon presentation to the medical complex hospital if they were between 30 and 45 years old and possessed a confirmed clinical and radiological (MRI) diagnosis. All diagnoses verified by independent neurological or orthopedic consultants. The inclusion criteria encompassed patients who were diagnosed with LDH at L4–L5 or L5–S1 levels with associated radiculopathy, aged 30–45 years; patients of both genders with a body mass index <30 kg/m2; symptom duration of 3–6 months; a minimum VAS score of 40 mm, and independent ambulatory status. Exclusion criteria included prior spinal or hip surgery, cauda equina syndrome, major neurological disorders (e.g., stroke), spinal infections or neoplasms, vascular issues, and pregnancy.
Ethical consideration
The study protocol adhered to international ethical principles and applicable local guidelines. Formal approval was obtained from the Institutional Review Board (IRB) of the Faculty of Physical Therapy, Cairo University (Reference No.: P.T.REC/012/005509; approved 2024). All participants signed a written consent form after being fully informed about the study’s goals, methodology, potential advantages, privacy and data use, and their ability to discontinue participation at any time. The investigation was performed in accordance with the ethical guidelines stated in the Declaration of Helsinki.
Sample size calculation
Sample size calculation was conducted utilizing G*POWER statistical software (version 3.1.9.2; Franz Faul, Universitat Kiel, Germany). Based on an alpha of 0.05, 80% power, and an effect size of 0.93, a minimum of 20 subjects per group was deemed necessary.
Randomization
This is a single-blind RCT in which participants remained blinded to their respective group allocation. To eliminate inter-investigator variability, a single trained investigator performed all clinical examinations and oversaw data collection. Participants meeting the inclusion criteria were randomly allocated to either the experimental group or control group via a secure allocation method involving sequentially numbered, opaque, sealed envelopes.
Outcome measures
Outcome measures were assessed at baseline and after a 6-week intervention period. The primary outcome was disc herniation size, measured by MRI. Secondary outcomes included pain intensity assessed by the Visual Analogue Scale (VAS) and functional disability assessed by the Oswestry Disability Index (ODI).
Disc herniation size
The disc herniation size was measured using MRI. To evaluate the lumbar intervertebral disc, participants underwent lumbar spine scanning in the supine position, and the following standardized sequences were done on all patients. The following morphometric parameters were measured: Anteroposterior diameter (mm) in the axial view (assessing the distance between the midpoints of the anterior and posterior intervertebral herniation boundaries); transverse diameter (mm) in the axial view (assessing the maximum distance between the lateral-most points of the intervertebral disc); and posterior vertical diameter (mm) in the sagittal view 8 (to quantify the cephalad or caudal migration of the herniation using superior or inferior vertebral endplates as reference landmarks).
Pain intensity
Pain intensity was evaluated by the 100-mm VAS, where a score of 0 represented “no pain” and 100 denoted “the most excruciating pain imaginable." Each patient was asked to document their pain levels both before and after completing the treatment program. Functional disability was evaluated with the ODI, a questionnaire consisting of 10 items, with total scores ranging from 0% to 100%; higher scores reflect greater levels of functional impairment. 10
Interventions
Both groups participated in a total of 18 treatment sessions over a 6-week duration, with an intervention frequency of three sessions per week.
High-intensity laser therapy
Study group (HILT intervention)
Participants in the study group received HILT via a pulsed Nd: YAG laser system (Hilterapia®, ASA, Italy) characterized by a 1064 nm wavelength, 3 kW peak power, and a pulse frequency of 10–40 Hz. The device utilized a 1 cm2 spot beam diameter with fluences ranging from 510 to 1780 mJ/cm². Each 20-minute session was administered with the patient in a prone position using a manual scanning technique. The handpiece was maintained in perpendicular contact with the skin over the lumbosacral region at the level of the herniation, with scanning performed in both lateral and transverse directions.
The treatment protocol was structured into three distinct phases, each subdivided into three subphases: Initial Phase: Conducted using rapid manual scanning to deliver a total energy of 1.248 J. This phase involved three consecutive subphases with fluences of 510, 970, and 1070 mJ/cm2. Intermediate Phase: Three specific paravertebral locations identified via trigger point localization. A total of 25 J was administered using fluences of 360, 510, and 610 mJ/cm², with a 6-Second duration per point. Final Phase: Followed the same parameters as the initial phase but utilized a slow manual scanning technique to complete the session.
The control group
The control group underwent an identical procedural setup; however, the laser device remained deactivated to serve as a placebo. 11
Physical therapy exercise program
Both groups received the same 25-minute physical therapy program consisting of the following interventions:
Flexibility exercises: Targeted stretching of the hamstrings, piriformis, and lumbar musculature. Strengthening exercises: Static abdominal contractions, bridging, and pelvic rocking. Supervision and dosage: All exercises were performed with specific sets and repetitions under the direct supervision of a physical therapist to ensure proper technique and adherence.
Statistical analysis
Statistical analysis and comparative assessments between groups were conducted through the SPSS software suite (version 23; SPSS Inc., Chicago, IL), utilizing a predetermined significance threshold of α = 0.05. To ensure the robustness of the statistical framework, preliminary evaluations were executed to verify the homogeneity of variance, identify potential outliers, and assess distributional normality. The Shapiro–Wilk test demonstrated that all continuous parameters adhered to a normal distribution (p > 0.05). Quantitative outcomes are expressed as mean values accompanied by standard deviations (SD). Conversely, qualitative variables—specifically sex distribution and the lateralization of radiculopathy—are delineated as absolute frequencies and corresponding percentages.
To evaluate the collective efficacy of the intervention across the specified outcome metrics, a two-way mixed-design multivariate analysis of variance (MANOVA) was executed. To mitigate the risk of type I error inflation, significant MANOVA findings were subsequently analyzed through independent univariate analysis of variance (ANOVA) for each dependent variable, incorporating the Bonferroni adjustment to account for multiple comparisons. The magnitude of the independent variable’s influence was quantified using partial eta squared (η2p). These effect size estimates were categorized based on established empirical benchmarks, where the values of (0.01, 0.06, and 0.14) represented (small, medium, and large) effects, respectively.
Results
Demographic characteristics of participants
The procedural trajectory of the current study is delineated in the flowchart provided in Figure 1. The results in Tables 1 and 2 revealed no statistically significant difference between both groups regarding demographic characteristics as well as baseline clinical variables (p > 0.05). Specifically, participants in Group A exhibited a mean age of 38.25 ± 3.67 years, with a sex distribution of 11 females and 9 males. Similarly, Group B, demonstrated a mean age of 37.25 ± 4.44 years, with 13 female and 7 male subjects.
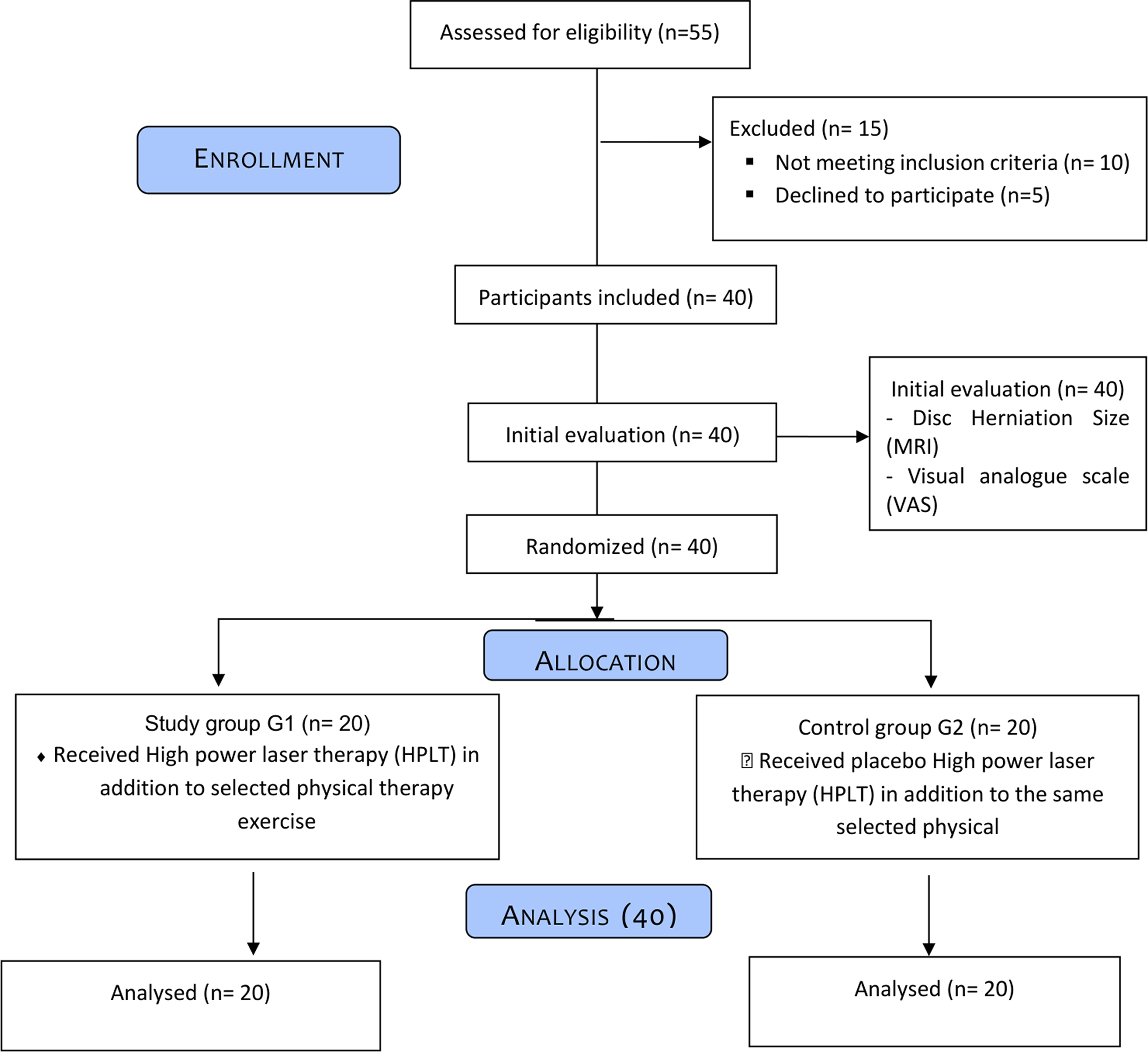
Study flow chart.
Baseline Demographic Characteristics of Participants (N = 40)
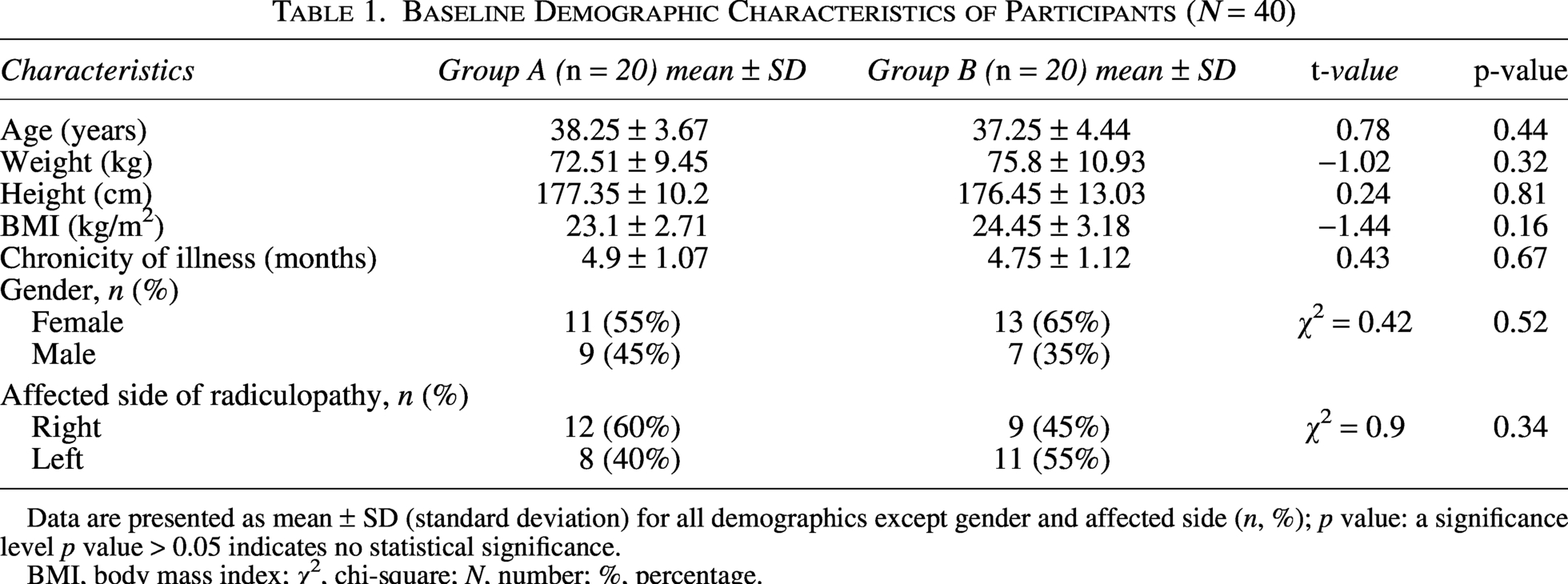
Data are presented as mean ± SD (standard deviation) for all demographics except gender and affected side (n, %); p value: a significance level p value > 0.05 indicates no statistical significance.
BMI, body mass index; χ2, chi-square; N, number; %, percentage.
Within- and Between-Group Comparison All Measured Variables (N = 40)
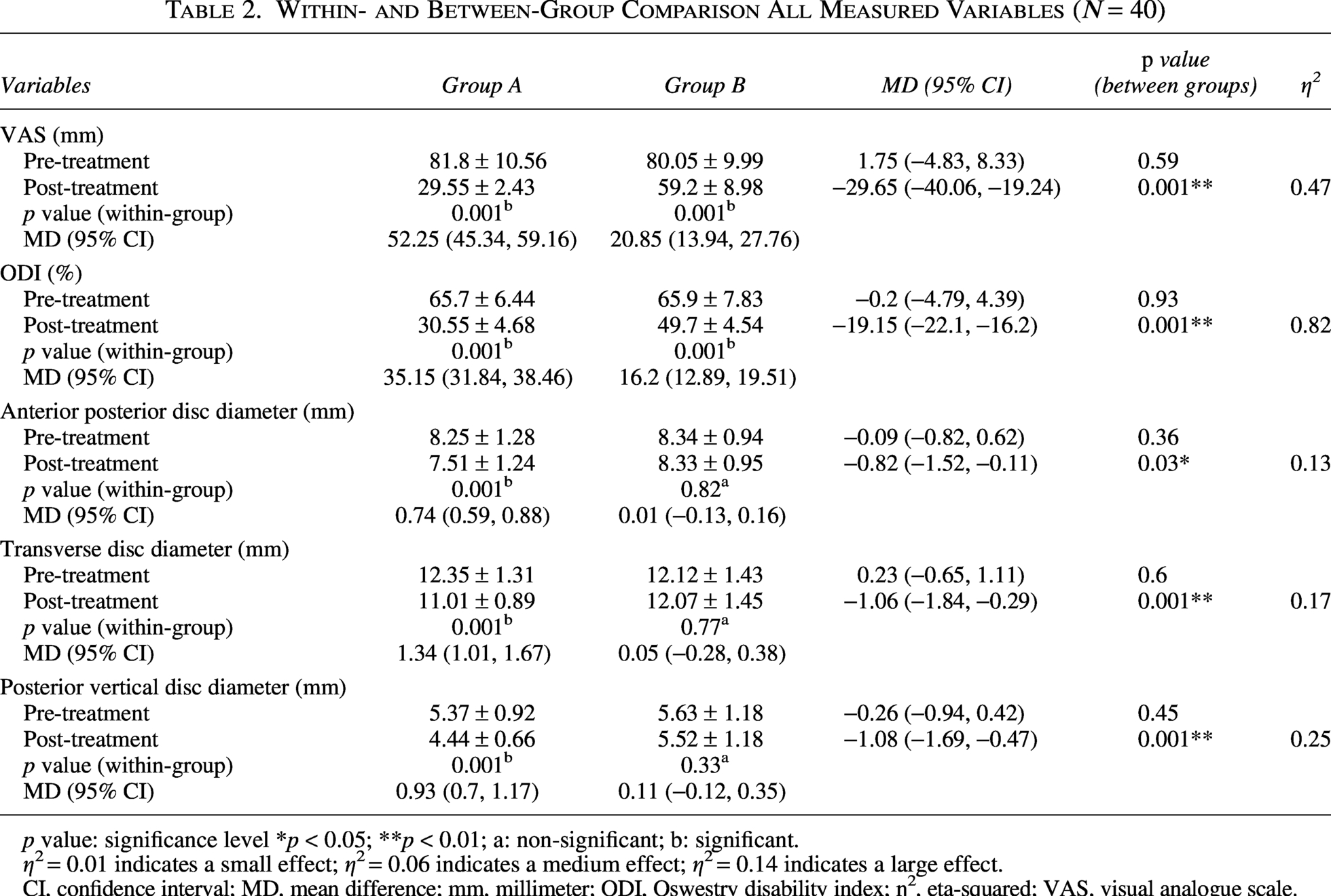
p value: significance level *p < 0.05; **p < 0.01; a: non-significant; b: significant.
η2 = 0.01 indicates a small effect; η2 = 0.06 indicates a medium effect; η2 = 0.14 indicates a large effect.
CI, confidence interval; MD, mean difference; mm, millimeter; ODI, Oswestry disability index; ƞ2, eta-squared; VAS, visual analogue scale.
A 2-way mixed-model MANOVA was employed to assess the differences in score changes on the outcome measures among participants in both groups over time. There was a statistically significant difference among groups on the combined dependent variables (VAS, ODI, anterior–posterior disc, transverse disc, and posterior vertical disc diameter of the intervertebral disc as Wilks’ λ = 0.37, F (5, 34) = 11.73, p-value < 0.001, partial eta squared (ƞ 2 = 0.63)). Additionally, the analysis revealed a statistically significant effect of time, comparing pre-intervention to post-intervention status (Wilks’ λ = 0.04, F (5, 34) = 181.83, p < 0.001, ƞ2 = 0.96). Furthermore, a significant group-by-time interaction effect was identified (Wilks’ λ = 0.13, F (5, 34) = 45.07, p < 0.001, ƞ2 = 0.87), indicating that the magnitude of change over the treatment period differed significantly between the groups.
Between-groups comparison
Upon completion of the 6-week therapeutic protocol, comparative analysis revealed statistically significant differences between the investigated groups across all assessed parameters. Specifically, Group A exhibited superior clinical outcomes, characterized by more pronounced reductions in VAS (p = 0.001) and ODI (p = 0.001) relative to Group B. Furthermore, structural enhancements in disc morphology—encompassing anterior posterior disc diameter (p = 0.03) and transverse disc diameter (p = 0.001) as well as posterior vertical disc diameter (p = 0.001)—favored Group A more, as shown in FIG. 2 & Table 2.
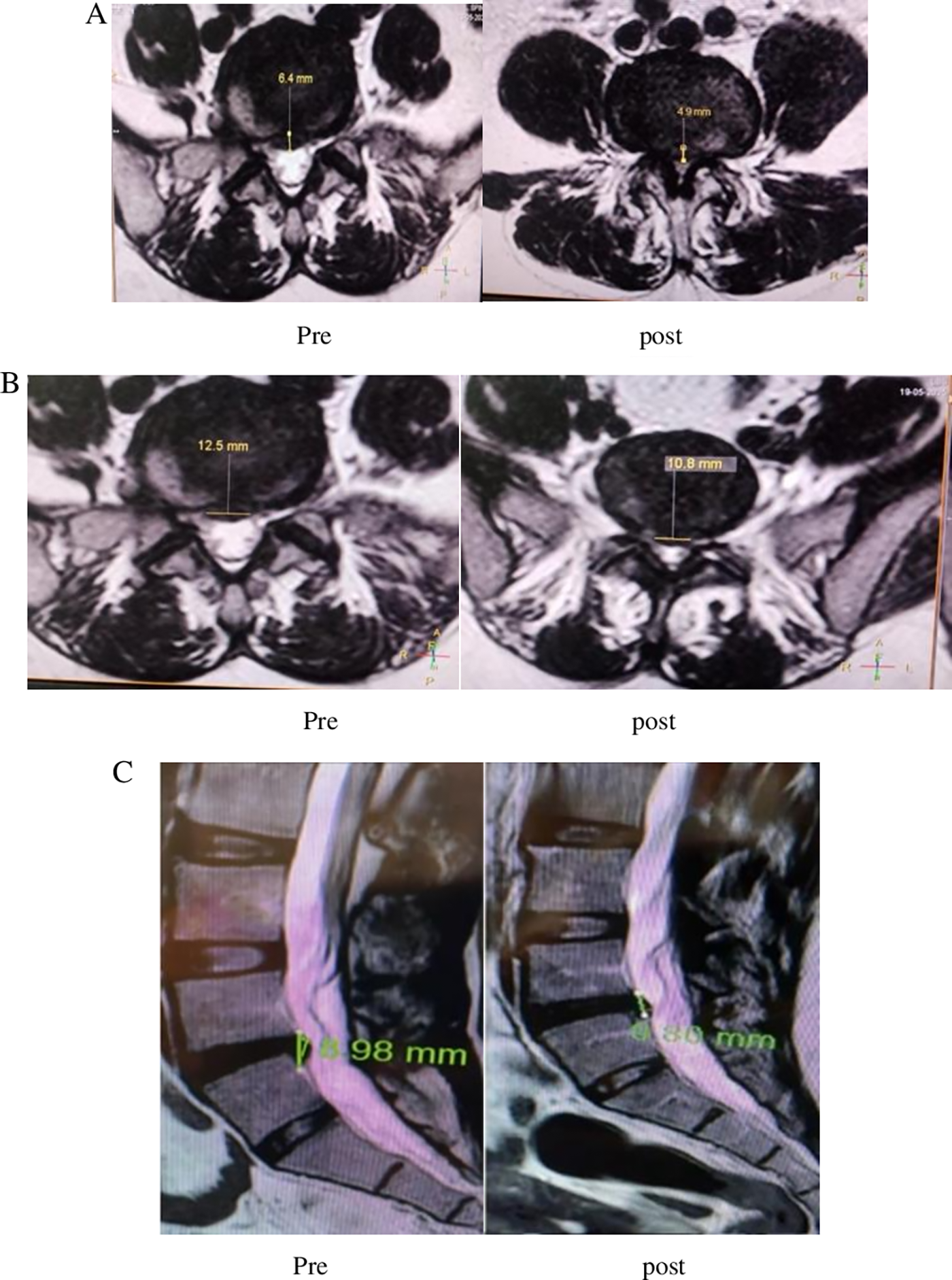
Pre- and post-treatment MRI images.
Within-groups comparisons for all outcome measures
Within-group comparison demonstrated that Group A showed statistically significant differences between pre- and post-interventions in all outcome measures, including the VAS, ODI, and all three dimensions of disc morphology (anterior-posterior, transverse, and posterior-vertical) after the treatment period (all of them significant at p = 0.001). whereas in Group B, there were statistically significant differences only in VAS and ODI (p = 0.001), as shown in Table 2.
Discussion
The present study evaluated the therapeutic influence of high-intensity laser therapy (HILT) on the morphological regression of LDH (by measuring the disc size), alongside its effects on pain severity and functional impairment among patients with LDH. It was shown that the application of HILT facilitates substantial structural retraction of herniated disc matter and yields a higher reduction of pain and disability than isolated exercise regimens. This study specifically focused on patients with symptom durations ranging from 3 to 6 months, representing the subacute or persistent phase of the pathology. Consequently, these findings underscore the short-term clinical effects and structural utility of HILT over a 6-week intervention period and should not be extrapolated as conclusive evidence of sustained, long-term therapeutic outcomes.
Based on the empirical evidence obtained, HILT represents a viable conservative modality for managing LDH, potentially accelerating the morphological regression of herniated material within a relatively short period. This structural recovery was paralleled by superior symptomatic relief and an expedited return to work. The findings revealed that the majority of subjects in the study group exhibited a profound contraction in both the transverse and anteroposterior disc dimensions relative to the control group. These objective anatomical improvements were verified through postintervention MRI assessments following the administration of 18 therapeutic sessions over the standardized 6-week HILT framework.
Regarding the demographic characteristics of the study population, a higher proportion of female participants was observed relative to males. While extant literature typically characterizes LDH as more prevalent among males—frequently citing a male-to-female ratio of approximately 2:1—the observed discrepancy may be attributed to sampling variation and gender-specific healthcare-seeking behaviors. Specifically, evidence indicates that females are more likely to pursue medical intervention and adhere to rehabilitation programs. This observation aligns with established epidemiological data regarding patient presentation in clinical settings. 12
The current results align with several previous studies highlighting the therapeutic advantages of HILT in facilitating pain attenuation, functional restoration, and enhanced clinical prognosis for individuals suffering from lumbar disc pathologies. Our findings are supported by Alayat et al., 13 who reported that HILT yields a superior reduction in chronic LBP and functional impairment when compared to a sham laser intervention. These researchers postulated that such clinical gains are mediated by the photochemical properties of laser irradiation, which stimulate mitochondrial metabolism and optimize microcirculatory flow, thereby accelerating the resolution of localized edema and fostering tissue regeneration. Furthermore, Chen et al. 14 demonstrated that augmenting spinal decompression with HILT for lumbar disc protrusion led to markedly superior improvements in ODI ratings, sagittal plane lumbar flexibility, and straight leg raise excursions relative to control cohorts.
Comparable findings were also reported by Boyraz et al., 15 who evaluated three cohorts of patients with LDH receiving HILT, therapeutic ultrasound, or conventional medical therapy combined with exercise. Although clinical improvements were observed across all groups, the HILT group exhibited markedly superior attenuations in both VAS ratings and ODI scores, along with superior improvements in several SF-36 domains. Critically, these benefits persisted at the 3-month follow-up, suggesting that HILT may offer more sustained therapeutic effects compared to conventional modalities.
Furthermore, several reviews and meta-analyses, including the work of Starzec-Proserpio et al., 16 have established that HILT yields significant pain reduction and functional enhancement across a spectrum of musculoskeletal conditions, frequently exhibiting moderate-to-large effect sizes. Experimental evidence provides a biological basis for these clinical observations; for instance, Hwang et al. 17 demonstrated that HILT stimulates extracellular matrix synthesis in nucleus pulposus cells by upregulating the production of proteoglycan and type II collagen—the fundamental structural components required for disc integrity and hydration. These observations suggest that the disc regression documented in the current investigation may not be solely a consequence of anti-inflammatory pathways; rather, it likely involves a combination of active tissue remodeling and intrinsic regenerative mechanisms.
The underlying mechanisms driving the morphological changes observed in this study may be elucidated by the complex biological interactions of HILT. According to Angelova and Ilieva, 18 these biological effects are mediated through both thermal and mechanical mechanisms. The thermal component elevates fluid temperature, facilitating phase state transitions and modulating intracellular pressure. Simultaneously, the mechanical effects involve kinetic alterations and mechanostimulation at the cellular level. Synergistically, these mechanisms likely contribute to enhanced tissue metabolism, the downregulation of inflammatory mediators, and the acceleration of reparative processes, thereby reinforcing the clinical validity of HILT as a robust conservative intervention.
Further supportive evidence was reported by Song et al. 19 who evaluated patients with LDH who underwent enzymatic decompression via collagenase chemonucleolysis, with a subset of the cohort receiving adjunct HILT postoperatively. The combined treatment group demonstrated significant symptomatic improvement alongside MRI-documented disc shrinkage. These observations are congruent with our current data and lend further credence to the hypothesis that HILT may accelerate recovery through the modulation of inflammatory pathways, enhancement of microcirculation, photobiomodulation, and the stimulation of endogenous tissue repair mechanisms.
Additional indirect supportive evidence is provided by Karimi et al. 20 who noted attenuations in both pain severity and the volumetric dimensions of herniated discs following the application of segmental traction combined with standard physiotherapeutic interventions, including ultrasound and transcutaneous electrical nerve stimulation (TENS). Nevertheless, the validity of those conclusions is tempered by substantial methodological constraints, such as a restricted sample size, the lack of a comparative control cohort, and the potential for confounding variables arising from multi-modal treatments. In particular, the independent contribution of ultrasound therapy to the observed morphological changes in the disc complicates the isolation of efficacy for any singular therapeutic component.
Despite these positive findings, some studies have reported divergent or nonsuperior results concerning HILT efficacy. Abdelbasset et al., 21 in a comparative analysis of HILT and low-level laser therapy (LLLT) for chronic nonspecific LBP, observed that while both modalities yielded significant clinical improvements—specifically regarding pain intensity, functional disability, and spinal kinematics, there were no statistically significant differences between the two protocols. Consistently, a multicenter randomized controlled trial conducted by Kuculmez et al. 22 in patients diagnosed with cervical disc herniation indicated that HILT failed to demonstrate a substantial therapeutic advantage over traditional physiotherapy and structured exercise programs.
Furthermore, Hassan et al., 23 in a meta-analysis comparing extracorporeal shock wave therapy with laser therapies, including both LLLT and HILT, found no clear superiority of laser therapy for pain reduction across pooled studies. These contradictory findings may be explained by the considerable heterogeneity among studies regarding laser wavelength, energy density, pulse frequency, treatment duration, and the total number of sessions, as well as patient selection criteria and follow-up periods. Additionally, many previous investigations assessed only symptomatic outcomes without radiological evaluation of disc regression, which complicates direct comparisons with the current MRI-based findings. Variability in concomitant interventions—such as exercise therapy, spinal decompression, traction, or pharmacological treatment—may also have influenced therapeutic responses and contributed to discrepancies across the literature.
It is important to note that the current findings represent short-term outcomes assessed immediately following the conclusion of the 6-week intervention. While significant improvements were documented in disc morphology, pain intensity, and functional disability, the durability of these effects beyond the immediate post-treatment phase remains to be established. Lumbar disc remodeling and long-term symptomatic resolution are dynamic processes that may necessitate extended longitudinal observation. Consequently, these results should be interpreted as evidence of early therapeutic efficacy rather than confirmation of sustained, long-term structural or clinical recovery.
The present study has several limitations. First, the relatively small sample size may constrain the generalizability of the findings to a broader clinical population. Second, the follow-up duration was restricted to the six-week intervention period, which only permits the assessment of acute therapeutic effects and precludes conclusions regarding the durability of the reported improvements over extended follow-up periods. In addition, the use of a single blind design could have increased the risk of measurement bias. Future research incorporating larger cohorts, extended longitudinal follow-up periods, and multicenter designs is warranted to confirm the persistence of these clinical and structural benefits.
Conclusion
HILT appears to be an effective conservative intervention for patients with LDH, facilitating significant short-term improvements in pain intensity, functional disability, and disc morphology over a 6-week treatment protocol. However, these results should be interpreted carefully, as they represent only immediate post-treatment outcomes. Further longitudinal research with prolonged follow-up periods is necessary to determine the long-term sustainability of these therapeutic effects and to establish the enduring clinical and structural efficacy of HILT.
Recommendations
The clinical application of HILT is recommended as a promising short-term conservative intervention for the management of LDH. However, further randomized controlled trials incorporating larger sample sizes and extended follow-up periods are essential to determine whether these acute improvements can be sustained over time and to establish definitive long-term clinical protocols.
Ethical Considerations
The study protocol adhered to international ethical principles and applicable local guidelines. Formal approval was obtained from the Research Ethical Committee of the Faculty of Physical Therapy, Cairo University (Reference No.: P.T.REC/012/005509; Approved 2024).
Consent to Participate
Written informed consent was obtained from all participants. Each individual was thoroughly informed regarding the study’s objectives, procedures, potential benefits, and data confidentiality protocols, as well as their right to withdraw at any stage without consequence.
Declaration of Conflicting Interest
The authors declared that no conflicts of interest were associated with this investigation.
Footnotes
Acknowledgments
The authors gratefully acknowledge Princess Nourah bint Abdulrahman University for supporting this research through Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2026R168), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Author Disclosure Statement
The datasets generated or analyzed in the current investigation are available from the corresponding author upon reasonable request to the principal investigator.
Funding Information
The study received financial support from