
Abstract
Purpose:
Laser–tissue interactions induce photothermal effects governed by wavelength-dependent absorption and circulation of energy. While 980 nm targets hemoglobin for hemostasis and 1470 nm targets water for vaporization, their synergistic optimization in living liver tissue remains undefined, as existing studies predominantly examine ex vivo models or single wavelengths. This study establishes quantitative relationships between laser parameters and tissue outcomes in an in vivo model.
Methods:
Twenty rabbits (female New Zealand White, 1.5–2 kg) underwent hepatic transection using a 400 μm bare fiber diameter (3 mm tissue distance, 10 mm/s advancement speed) in continuous-wave (CW) and pulsed-modulated (100 ms pulse, 50% duty cycle, 5 Hz) modes. Output power: 980 nm (12–160 W) and 1470 nm (6–48 W), with different dual-wavelength power ratios. Measured outcomes: cutting depth, vaporization depth, coagulation depth, and thermal injury depth (quantified by hematoxylin and eosin staining). Statistics: analysis of variance for continuous variables, chi-square/Fisher’s exact test for categorical variables, and the Mann–Whitney U test for non-normal distributions (p < 0.05).
Results:
CW mode achieved greater cutting depth than pulsed-modulated mode (median 943.97 μm vs. 689.43 μm, p < 0.05). In CW mode, 1470 nm-dominated ratios (0:1, 1:1, 1:2, 1:3, 1:4) achieved greater cutting depths than 980 nm alone (1:0). Cutting depth increased with peak power from 6 to 120 W, then decreased at 160 W due to carbonization. At 24 W total power with 1:2 ratio (8 W 980 nm/16 W 1470 nm), cutting depth was 1249.3 ± 15.55 μm, vaporization depth 739.5 ± 35.32 μm, coagulation depth 1302 ± 125.44 μm, and thermal damage 1987.53 ± 154.61 μm.
Conclusions:
The 980/1470 nm wavelength power ratio of 8/16 W in CW mode for liver tissue cutting offers high efficiency, safety, and minimal thermal damage, providing an effective surgical energy device for minimally invasive and precise treatment.
Introduction
Recent studies show that primary liver cancer is the sixth most commonly diagnosed and the third most common cause of cancer death in the world.1,2 Hepatectomy, the surgical resection of part of the liver, is a standard curative treatment for hepatocellular carcinoma and other primary hepatic malignancies. Currently, ultrasonic scalpels and high-frequency electric surgical knives dominate liver resection,3–5 yet laser technology offers precise thermal damage control through wavelength-selective absorption, presenting potential for minimally invasive hepatic surgery.
Biological tissue acts as a turbid optical medium that exhibits absorption, scattering, reflection, and refraction of incident laser energy, and laser irradiation can induce photothermal, photochemical, and photomechanical effects in such tissue. Via flat-cut bare-ended optical fibers, the laser’s photothermal effect can be converted into mechanical force, with the energy precisely concentrated on the target tissue. Once absorbed by biological tissue, the laser energy is rapidly and locally converted into heat within a minimal tissue volume, which triggers the boiling and vaporization of tissue fluid as well as the formation of vapor microbubbles that generate associated mechanical forces. These coupled photothermal and photomechanical processes enable effective tissue vaporization and cutting while concurrently inducing thermal coagulation in the adjacent tissue. Linear movement of the fiber translates the laser’s tissue target from a point to a line, enabling rapid and precise tissue cutting. 6
Tissue light absorption is mediated by chromophores—including endogenous moieties such as oxyhemoglobin, deoxyhemoglobin, bilirubin, melanin, and water, as well as exogenous dyes added to tissues or during treatment. 7 Tissues exhibit wavelength-dependent absorption capacities, with lasers of different wavelengths targeting distinct tissue components. The 980 nm laser primarily targets hemoglobin, with an absorption coefficient of 0.1–2 cm−1 for both oxyhemoglobin and deoxyhemoglobin, inducing coagulation of vascular endothelial cells and histiocytes to achieve effective hemostasis, making it ideal for highly vascularized tissues.8,9 Its relatively high scattering coefficient scatters photons laterally, extending light penetration, thereby supporting deeper coagulation. In contrast, the longer-wavelength 1470 nm laser primarily targets water while also being absorbed by hemoglobin (0.01–1 cm−1). At 1470 nm, the water absorption coefficient of biological tissue is ∼25 cm−1, reportedly 40- to 60-fold that at 980 nm (∼0.43 cm−1), paired with a lower scattering coefficient. This reduced scattering, combined with strong superficial water absorption, enables precise cutting with minimal thermal spread and collateral damage, thereby improving surgical precision and safety.8,10–13
The dual-wavelength laser, as a relatively emerging technology, combines two lasers with complementary wavelength-specific properties to achieve improved surgical outcomes. In photobiomodulation therapy, dual-wavelength protocols have demonstrated synergistic modulation of inflammation, pain, and redox status during tissue repair. Near-infrared combinations such as 810 nm paired with 904 nm exemplify this approach, leveraging complementary absorption profiles to accelerate wound healing. 14 Similarly, Thomé Lima et al. 15 investigated dual-wavelength low-power laser photobiomodulation (660 and 808 nm) for pressure ulcer healing and bacterial bioburden reduction. Beyond therapeutic applications, this principle has been extended to aesthetic and vascular surgery. Gold 16 and Leight-Dunn et al. 17 studied dual-wavelength picosecond lasers (532 and 1064 nm) for treating photoaged skin. Deng Liehua et al. 18 applied dual-wavelength laser (595 and 1064 nm) in the treatment of ulcerated hemangiomas. In urological surgery, Hwang et al. 19 explored the feasibility of dual-wavelength laser (532 and 980 nm) assisted thermal hemostasis for prostate treatment.
The dual-wavelength laser combines the use of two lasers to better utilize the hemostatic function of the 980 nm laser and the tissue vaporization function of the 1470 nm laser. Currently, research on the 980/1470 nm dual-wavelength laser mainly focuses on urological diseases, such as benign prostatic hyperplasia (BPH). Qiao, 20 Hou, 21 Dong, 22 and others indicate that the 980/1470 nm dual-wavelength laser offers advantages such as high safety, minimal tissue damage, and fewer complications when used for transurethral resection of the prostate to treat BPH. Clinical outcomes of 980/1470 nm dual-wavelength laser therapy for BPH include significant reductions in prostate volume (measured by transrectal ultrasound), improvements in maximum urinary flow rate (Qmax), decreases in post-void residual urine, lower International Prostate Symptom Score, and higher quality-of-life scores. 23 Wang, 23 Cui, 24 and others have evaluated the efficacy and safety of the 980/1470 nm dual-wavelength laser for non-muscle-invasive bladder cancer compared with transurethral bladder tumor resection. Wollina et al. 25 have applied the 980/1470 nm dual-wavelength diode laser in dermatology, treating 497 cases of skin and lip vascular lesions and confirming its safety.
Laser applications in hepatobiliary surgery date to 1991 with Nd:YAG laser hepatectomy. Xu et al. 26 applied Nd:YAG laser to experimental and clinical studies of liver small-lesion resection and partial resection. Qian et al. 27 also compared Nd:YAG laser with cavitron ultrasonic surgical aspirator and blunt dissection for liver resection. Zeng et al. 28 investigated the different effects of laser irradiation on rat liver tissue in vivo. Yin et al. 29 discussed the optimal power for Nd:YAG laser liver partial resection. Kirschbaum et al. 30 used the German LIMAX® 120 Nd:YAG laser, demonstrating its excellent prospects for rapid liver resection when applied at maximum output power (120 W) and a constant working speed of 5 mm/s. Gu, 27 Chen, 31 Wu, 32 and others studied laser coagulation in experimental animal liver tissue, observing the coagulative necrosis caused by laser on the liver. Fan et al. 33 evaluated the necrosis range of liver tissue caused by semiconductor lasers at different powers and energies, providing reliable evidence for the treatment of malignant liver tumors with semiconductor lasers. Ma et al. 34 studied the effects of different 980 nm semiconductor laser parameters on liver resection based on resection speed, intraoperative bleeding, and thermal injury assessment. They suggested lowering the average power to improve hemostasis efficiency and reducing peak power to shorten surgery time. Consistent with the hemoglobin-specific absorption characteristic of 980 nm lasers, Chai et al. 35 also confirmed that the 980 nm semiconductor laser has good hemostatic effects while maintaining cutting speed during liver resection.
Although dual-wavelength lasers show promise in urology, their parameter optimization for liver resection remains undefined. Liver resection requires balancing parenchymal transection with hemostasis and minimal thermal damage. This study establishes quantitative relationships between laser parameters (power, wavelength ratio, and working mode) and tissue outcomes in an in vivo liver model, providing evidence for standardized clinical application.
Materials and Methods
This study was approved by the Ethics Committee of the First Affiliated Hospital of Xi’an Jiaotong University (No. XJTUIAF2020LSY-06), following the ARRIVE guidelines.
Animals
In total, 20 female New Zealand Large White rabbits weighing 1.5–2 kg were obtained from the Experimental Animal Center, Xi’an Jiaotong University, Xi’an, China.
Laser system
A semiconductor laser system (LM1470-980-A; Leimai Technologies Inc., Shenzhen, China) emitting dual wavelengths (980 and 1470 nm) was used for liver resection, as shown in Fig. 1. This system operates in both continuous-wave (CW) and pulsed-modulated modes, with a maximum average power of 210 W. Laser energy was delivered via a 3-m flat-cut bare-ended quartz fiber (FL-FP03-SH/B-400/440-0.22-S-3M-N; Laser Medicine Technologies Inc., Shenzhen, China) featuring a 400 μm core diameter. Prior to each laser application, the fiber’s distal end was inspected for irregularities (e.g., breakage or burnout) and polished as needed.
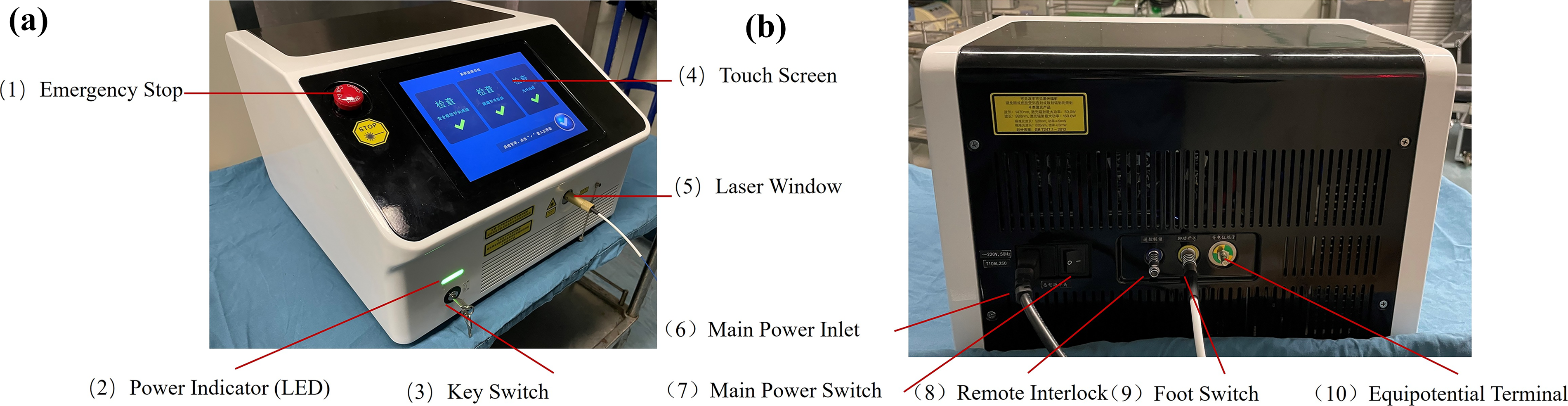
External view of the 980/1470 nm dual-wavelength diode laser console.
Anesthesia
After fasting for 24 h before surgery, the experimental rabbits were anesthetized after preoperative weighing. The anesthetic drug was slowly injected with 3% pentobarbital sodium (1.0 mL/kg, Sigma-Aldrich, St. Louis, MO) through the auricular vein. At the same time, the vital signs of the experimental animals were closely observed to avoid anesthesia accidents, and the dosage of narcotic drugs was recorded in detail.
Liver resection procedure
Experimental rabbits were maintained in a supine position. To ensure histological consistency among the resected liver lobes, a standardized incision line was established 10 mm from the lobar margin. After adequate exposure of the target lobe, hepatic transection was performed along this predefined line using both CW and pulsed-modulated modes at preset laser parameters. The incision length was fixed at 1 cm, and the advancement rate was maintained at 10 mm/s. Throughout irradiation, the animals’ vital signs were monitored. The fiber-to-tissue distance was maintained at 3 mm via an integrated mechanical–optical protocol: The distal end of the bare fiber was affixed within a stainless-steel capillary whose distal end had been lapped flat.
Study design
Twenty rabbits were randomly allocated to either CW or pulsed-modulated modes (n = 10 each). For single-wavelength delivery, power was raised in equal steps from 12 to 160 W at 980 nm and from 6 to 48 W at 1470 nm. Dual-wavelength emission (980/1470 nm) was tested at the fixed ratios 1:0, 0:1, 1:1, 2:1, 3:1, 4:1, 1:2, 1:3, and 1:4, with total power advanced from 6 to 200 W in the same uniform increments. After every exposure, the fiber was repositioned to an adjacent untreated site; escalation occurred between individual runs to generate an evenly spaced dose–response curve for histological comparison. Pulsed-modulated mode employed 100 ms pulses at 50% duty cycle. All parameter sets are detailed in Table 1.
Parameter Combinations of the 980/1470 nm Dual-Wavelength Laser Used for In Vivo Rabbit Liver Resection
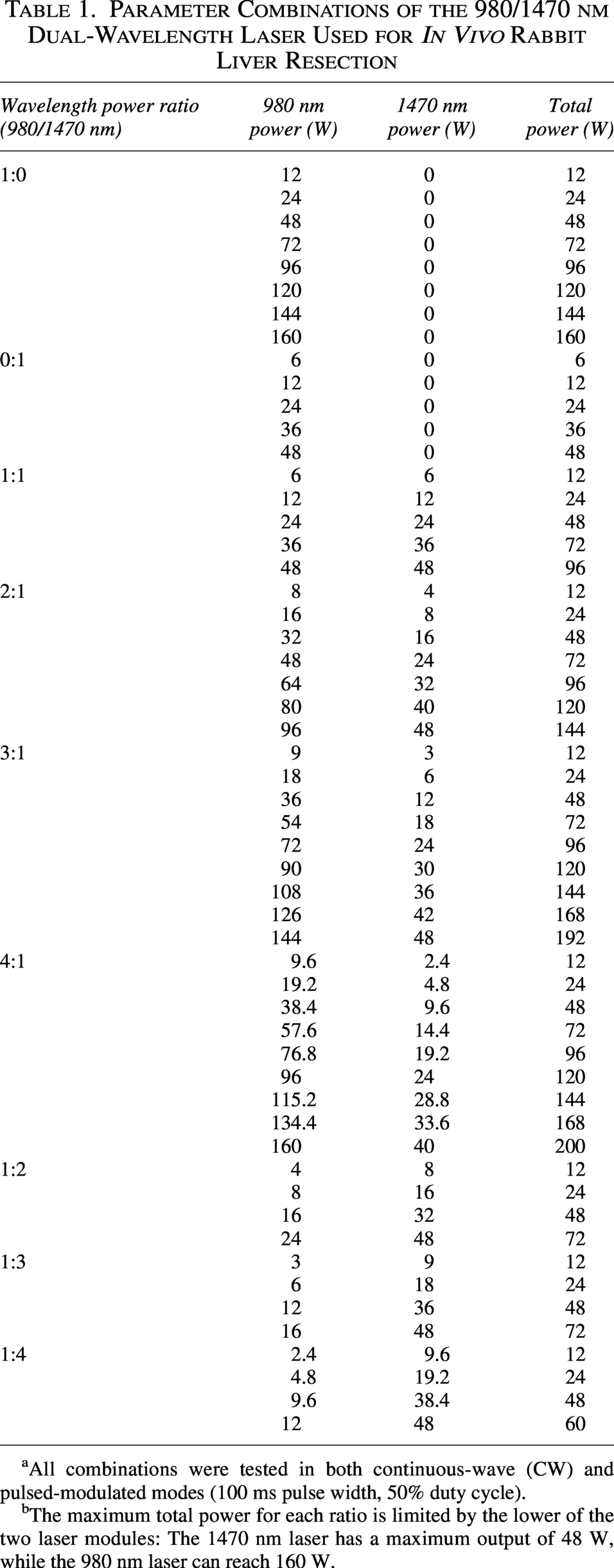
All combinations were tested in both continuous-wave (CW) and pulsed-modulated modes (100 ms pulse width, 50% duty cycle).
The maximum total power for each ratio is limited by the lower of the two laser modules: The 1470 nm laser has a maximum output of 48 W, while the 980 nm laser can reach 160 W.
Evaluation of resection efficiency
The effects of the laser on liver tissue were investigated by adjusting parameters including working mode, wavelength power ratio, and peak power. Hematoxylin and eosin (H&E) staining was used to assess laser-induced pathological changes in liver tissue, specifically cutting depth, vaporization depth, coagulation depth, and thermal injury depth. Cutting depth was defined as the distance from the tissue surface to the deepest site of tissue loss. Vaporization depth referred to the average depth of regions with evident tissue cavitation. Coagulation depth was the average depth of areas exhibiting irreversible tissue changes, cellular degeneration, necrosis, and coagulation. Thermal injury depth was defined as the average depth of tissue showing pathological alterations.
Data analysis
Categorical variables are presented as counts or percentages, with comparisons via chi-square or Fisher’s exact test as appropriate. Normally distributed continuous variables are reported as mean ± standard deviation and compared using analysis of variance; non-normally distributed ones are expressed as median [interquartile range (IQR)] and analyzed via nonparametric tests. Statistical significance was defined as two-sided p < 0.05. All analyses and visualizations were performed using R software (v4.3.2) and GraphPad Prism 9.
Results
Histological evaluation
As illustrated in Fig. 2, representative H&E-stained sections of rabbit liver tissue treated with the 980/1470 nm laser at 54/18 W in pulsed-modulated mode demonstrated distinct zones of thermal injury. The green bracket indicates the cutting depth, representing the maximum extent of tissue ablation from the surface to the deepest site of tissue loss. The orange dashed line delineates the vaporization depth, corresponding to the average depth of regions with evident tissue cavitation and acute thermal ar=desiccation. The blue dashed line marks the coagulation depth, denoting the average depth of areas exhibiting irreversible tissue changes, cellular degeneration, necrosis, and protein denaturation, which collectively contribute to the hemostatic effect.

H&E staining of the effects of 980/1470 nm laser on rabbit liver at 54 W/18 W laser parameter combination in pulsed-modulated mode (7.5×). H&E, hematoxylin and eosin.
Depth of cutting
The comparison of the liver tissue cutting depth of the 980/1470 nm dual-wavelength laser in different working modes is shown in Fig. 3a. The median cutting depth of the CW mode was 943.97 μm, and the median cutting depth of the pulsed-modulated mode was 689.43 μm. The cutting depths of the liver tissue of the two wor.king modes were significantly different (p < 0.05), so the CW mode was mainly concerned in the study for the purpose of cutting.
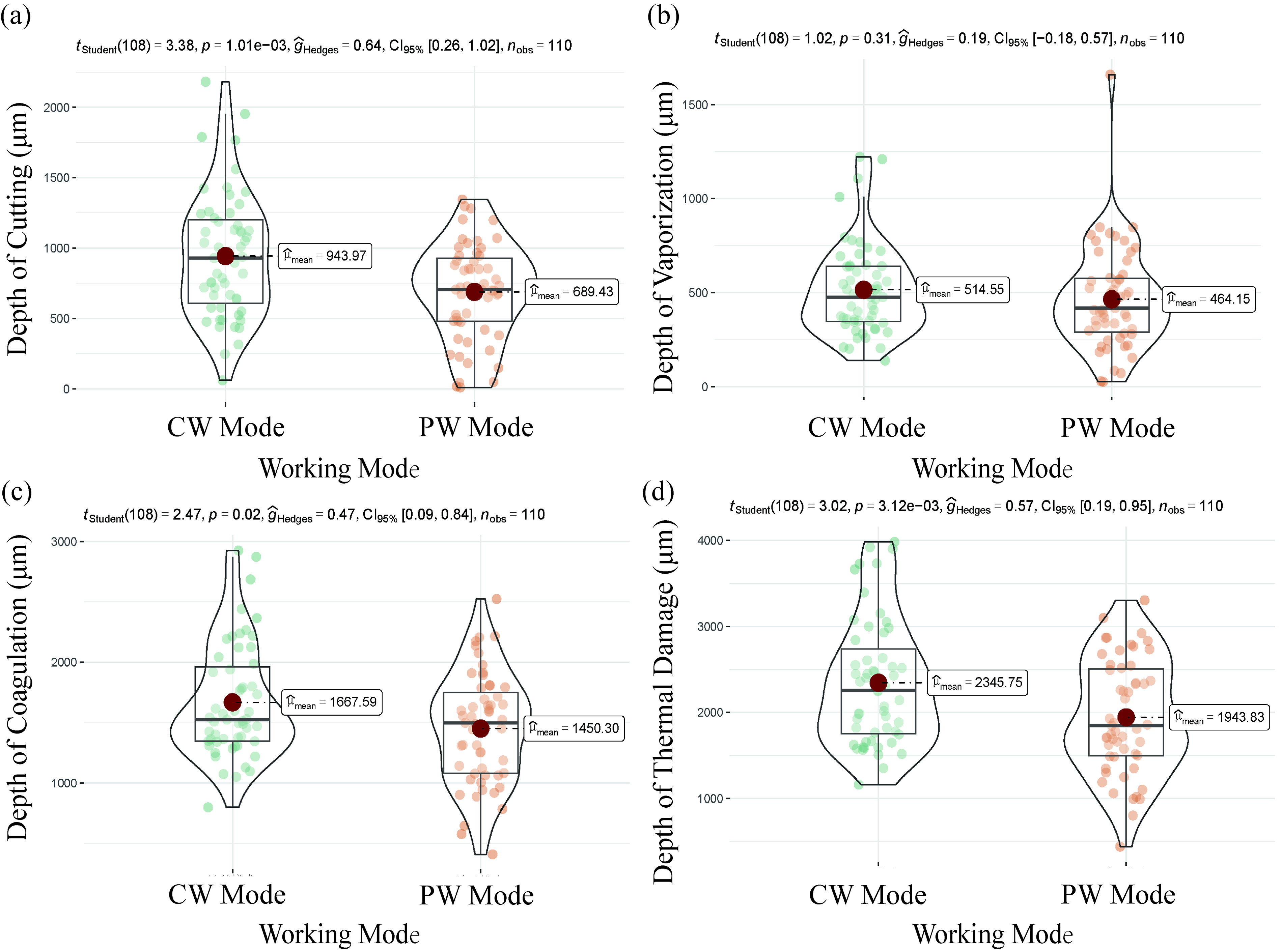
Pathological changes of liver tissue under different working modes.
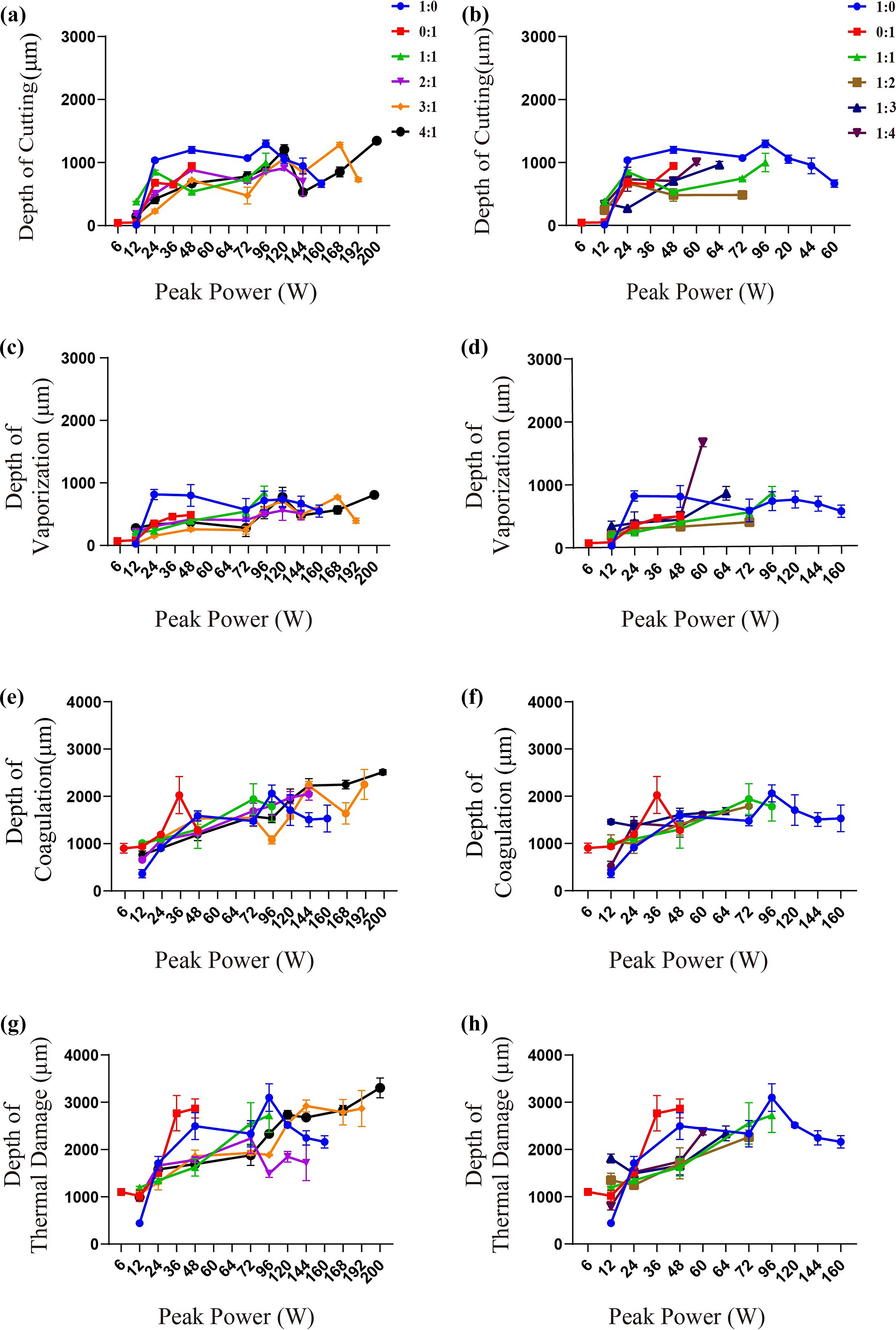
In CW mode, there was no significant difference in the depth of liver tissue cutting between different wavelength power ratios. As shown in Fig. 4a and b, within a certain peak power range, the cutting depths with wavelength power ratios of 0:1, 1:1, 1:2, 1:3, and 1:4 (measured as 1188.53 ± 52.23 μm, 1312.5 ± 60.6 μm, 1249.3 ± 15.55 μm, 1009.73 ± 93.93 μm, and 1115.47 ± 15.53 μm at 24 W, respectively) were greater than those of other combinations, including the 980 nm laser alone (637.13 ± 26.26 μm at 24 W), highlighting the superior cutting capability of the 1470 nm laser. Within this range, statistically significant differences in cutting depth existed between different peak power groups (p < 0.05), and cutting depth increased with peak power when below 120 W but decreased at excessively high peak powers. No significant difference in cutting depth was detected among peak power levels of 24–48 W. In pulsed-modulated mode, the single 980 nm wavelength exhibited higher cutting efficiency compared with all dual-wavelength power ratios, as shown in Fig. 5a and b.
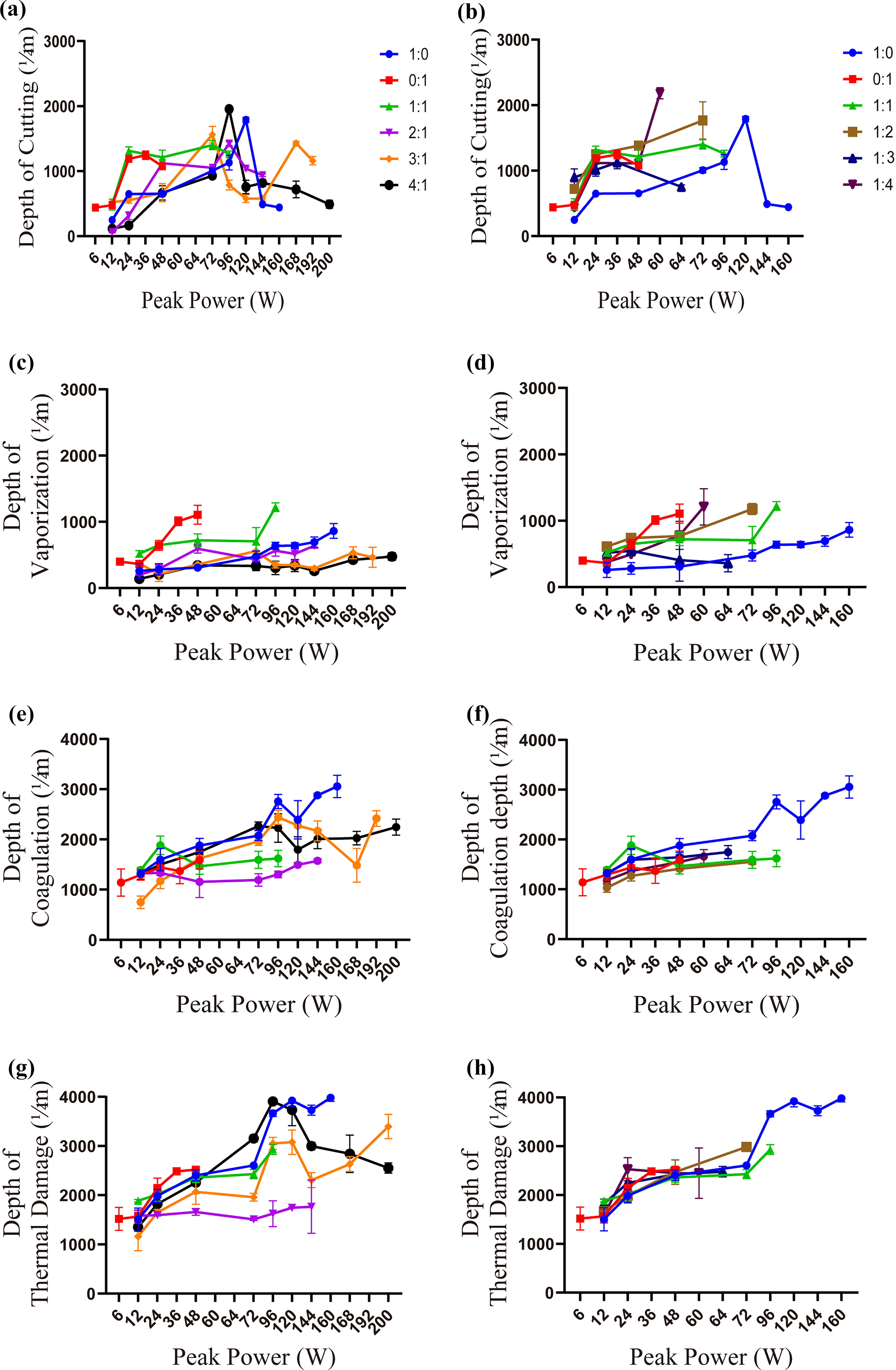
Power ratio of different wavelengths and pathological changes of liver tissue at peak power.
Power ratio of different wavelengths and pathological changes of liver tissue at peak power.
Depth of vaporization
The comparison of liver tissue vaporization depth of 980/1470 nm dual-wavelength laser under different operating modes is shown in Fig. 3b. The median ablation depth in CW mode was 514.55 μm, while in pulsed-modulated mode it was 464.15 μm. There was no significant difference in vaporization depth between the two operating modes in liver tissue.
As shown in Fig. 4c and d, in CW mode, there was a significant difference in vaporization depth between power combinations with different wavelengths (p < 0.05). For combinations with peak powers ranging from 24 to 48 W, those with a higher proportion of the 1470 nm wavelength exhibited deeper vaporization depths compared with those dominated by the 980 nm wavelength. In pulsed-modulated mode, deep vaporization was achieved when only the 980 nm wavelength was utilized. These findings indicate that the synergistic vaporization and cutting capabilities of the combined 980 and 1470 nm lasers have not yet been fully exploited in pulsed-modulated mode, as shown in Fig. 5c and d.
Depth of coagulation
There was no significant difference in the coagulation depth of liver tissue between the two working modes of the 980/1470 nm dual-wavelength laser, as shown in Fig. 3c. The median coagulation depth in CW mode was 1667.59 μm, while in pulsed-modulated mode, the median cutting depth was 1450.30 μm.
There was a significant difference in the depth of coagulation between different wavelength power ratio combinations in the CW mode (p < 0.05), which can be seen from Fig. 4e and f. Combinations with a higher proportion of the 980 nm wavelength exhibited greater coagulation depths, while those with wavelength power ratios of 1:2 and 1:4 (measured as 1302 ± 125.44 μm and 1376.4 ± 4.38 μm at 24 W, respectively) showed smaller coagulation depths. The combinations of peak power in different working modes of the 980/1470 nm dual-wavelength laser showed statistically significant differences in coagulation depth (p < 0.05). Coagulation depth increased with increasing peak power, with relatively small coagulation depths observed at peak powers of 6–36 W; thus, 24–36 W was identified as a more suitable optical parameter range. In the pulsed-modulated mode, there were no statistically significant differences in coagulation depth among various wavelength power ratios, as shown in Fig. 5e and f.
Depth of thermal damage
Figure 3d showed that the median thermal damage depth of liver tissue was 2345.75 μm in CW mode and 1943.83 μm in pulsed-modulated mode, and there was a significant difference in the thermal injury depth of liver tissue between the two working modes (p < 0.05).
As shown in Fig. 4g and h, there was a significant difference in thermal damage depth between wavelength power ratio combinations in CW mode (p < 0.05). Wavelength power ratios of 2:1 and 1:2 (measured as 1595.27 ± 15.4 μm and 1987.53 ± 154.61 μm at 24 W, respectively) resulted in minimal thermal injury to liver tissue. Considering the study’s focus on liver tissue cutting, the 1:2 ratio was identified as the more optimal laser parameter.
Statistically significant differences in thermal damage depth were observed among different peak power groups of the 980/1470 nm dual-wavelength laser, with more severe thermal damage associated with higher peak powers. When peak power was below 24 W, thermal damage was statistically minimal, indicating that 24 W represents a more appropriate peak power parameter.
Under the pulsed-modulated mode, as shown in Fig. 5g and h, the application of dual wavelengths within a specific power range mitigates thermal injury to liver tissue. Notably, thermal injury severity increases with increasing peak power.
In summary, for clinical preoperative studies and clinical experiments focused on tissue cutting, the optimal parameter combination is CW mode with a peak power of 24 W and a 980/1470 nm wavelength power ratio of 1:2 (cutting depth was 1249.3 ± 15.55 μm, vaporization depth 739.5 ± 35.32 μm, coagulation depth 1302 ± 125.44 μm, and thermal damage 1987.53 ± 154.61 μm). Specifically, the 8/16 W wavelength power ratio achieves a greater liver tissue cutting depth while maintaining a sufficient vaporization depth, concurrently minimizing thermal injury to liver tissue.
Discussion
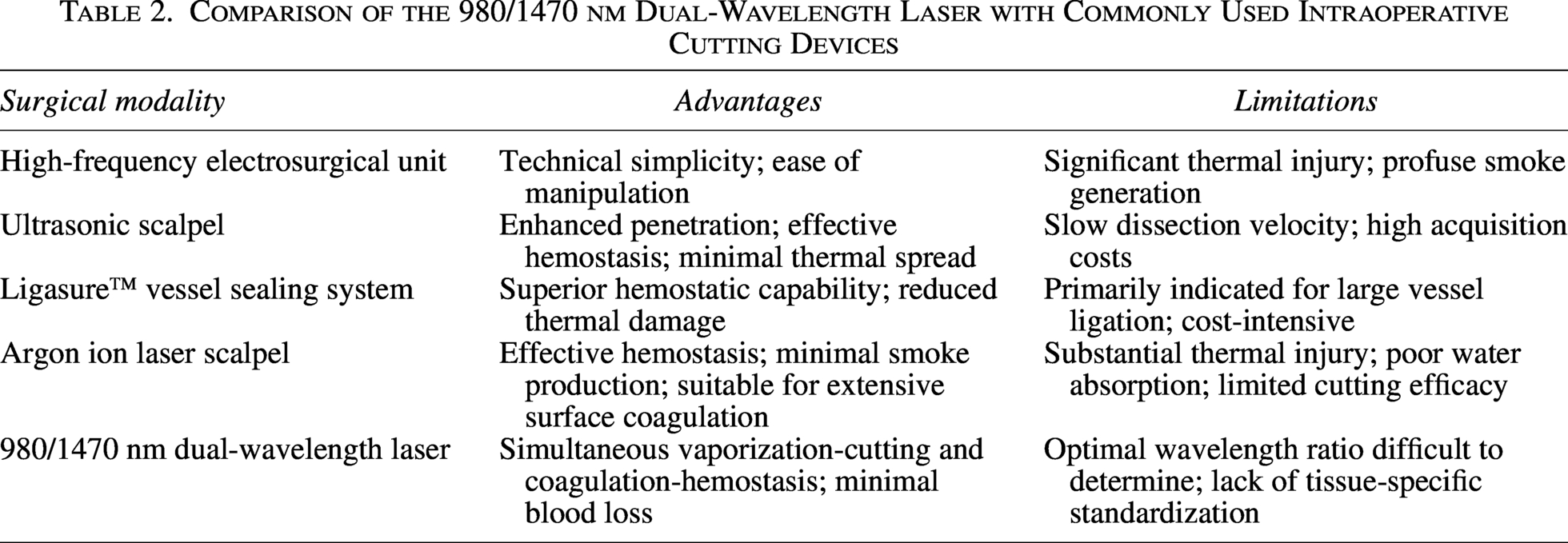
Table 2 compares the 980/1470 nm dual-wavelength laser with conventional intraoperative cutting devices, confirming the value of the laser as a feasible alternative for tissue dissection.3–5
Comparison of the 980/1470 nm Dual-Wavelength Laser with Commonly Used Intraoperative Cutting Devices
In the study of different scholars, the potential influence parameters of laser surgery process can be summarized as follows: wavelength, pulse duration, water cooling or air cooling, laser power, laser scanning speed, and linear energy density. In order to quantify the quality of cutting, some scholars have created a scoring system to evaluate the impact on tissue during laser surgery. 36 Riedinger et al. demonstrated that for thulium fiber laser lithotripsy, pulse duration exceeding the calculated thermal relaxation time (11.4 ms) poses an independent risk for excessive nonspecific heat generation, with long-pulse settings producing significantly higher temperatures than short-pulse equivalents at identical energy dosimetry (79.6°C vs. 71.8°C, p = 0.002). 37 However, according to Chai, 35 pulse width and pulse repetition frequency are not independent risk factors in laser hepatectomy. Therefore, the effects of laser power, working mode, and wavelength on liver tissue were mainly discussed.
Power is the core factor of laser hepatectomy. 38 As output power increases, both cutting depth and thermal injury increase correspondingly. 39 Yamamotol et al. 40 reported that for 980 nm lasers, the depth of the high-temperature layer (i.e., tissue dissociation and carbonization) increases with increasing laser power. Consistent with prior findings by Ma et al., 35 the present study demonstrated that within a specific peak power range, cutting depth increases with peak power, while excessively high peak power leads to reduced cutting depth. However, overall, vaporization depth, coagulation depth, and thermal injury severity exhibited an increasing trend with rising peak power, which is consistent with previous literature reports. 41 Additionally, increased peak power was associated with greater intraoperative smoke generation, while no significant difference in hemostatic efficiency was observed. Notably, CW mode with a peak power of 24–48 W ensured high liver tissue cutting efficiency: a peak power of 36 W yielded a smaller coagulation depth, and 24 W minimized thermal injury.
Working mode is a key factor influencing laser-mediated liver cutting. Wendt Nordahl et al. 42 showed in an in vitro porcine kidney model that at 100 W 980 nm laser output, tissue coagulation area was 208.8 ± 30.8 μm (pulsed mode) versus 255 ± 28.2 μm (CW mode). Although Seitz et al. 43 argued that this conclusion is inconsistent with in vitro and in vivo experiments investigating optical penetration depth correlations, O’Dey et al. 44 confirmed that pulsed-mode laser caused fewer carbonized and necrotic areas, so pulsed mode should be used more in endovenous laser ablation (EVLA) to prevent perforation. 45 In the present study, CW mode achieved deeper cutting depth and greater thermal injury depth. This may be explained by the absence of power delivery during the pulse interval in pulsed-modulated mode, which allows tissue self-cooling. Tunc et al. 41 reported that CW mode ablation yields a larger coagulation area, while pulsed-modulated mode with lower energy input over the same duration induces greater tissue edema. Lower time-averaged power delivery in pulsed-modulated mode may also cause more extensive thermal injury to adjacent tissues, a phenomenon mitigable by shortening laser operation time. Notably, in pulsed-modulated mode, 980 nm single wavelength (24–96 W peak power) achieved deeper cutting, failing to leverage the dual-wavelength (980/1470 nm) advantage. While vaporization/coagulation depths did not differ statistically between modes, CW mode’s deeper median vaporization depth supports intraoperative safety.
Wavelength, as one of the characteristic parameters of laser, 38 affects the cutting depth and thermal damage degree of tissue, etc. Due to the limitation of this semiconductor laser, the maximum total power of 1470 nm wavelength reaches 50 W. The results of this experiment showed that the wavelength power ratio with a larger proportion of 1470 nm in CW mode had a deeper cutting depth, which was similar to the results of Kabnick et al. 46 in veins, demonstrating the selective destruction effect of long-wavelength laser on tissues, while less energy is required to achieve the same effect. He et al. 47 believed that under the same power (120 W), the vaporization efficiency of 1470 nm laser was greater than that of 980 nm laser, and the coagulation depth of 980 nm laser was >1470 nm laser. These findings were consistent with the pathological changes of liver tissue under CW mode in this study. But Huang et al. 48 believed that the coagulation effect of short-wavelength laser was weaker, while the vaporization effect was stronger.
Despite the laser’s primary advantage of precision, lateral thermal diffusion can still induce thermal injury to adjacent tissues—an important consideration in preclinical applications, particularly for procedures requiring delicate manipulation. 49 The 1470 nm laser wavelength exhibits excellent tissue vaporization capacity, enhancing cutting depth while reducing tissue thermal injury and enabling lower peak power usage to avoid excessive thermal damage. Combined with the aforementioned working mode findings, the 980/1470 nm dual-wavelength laser should adopt CW mode for cutting to achieve higher efficiency while ensuring surgical safety. Although the 2:1 wavelength power ratio in CW mode minimized liver tissue thermal injury, considering the primary goal of liver cutting, ratios with a higher proportion of 1470 nm are preferred within the range of controllable tissue thermal damage. At 24 W peak power in CW mode, the 980/1470 nm wavelength power ratios of 1:2 and 1:4 yielded smaller coagulation depths; among these, the 1:2 ratio—with lower thermal injury—is a more suitable laser parameter for liver cutting.
This experiment has several limitations. Constrained by respiratory motion in living animals and the nonplanar hepatic anatomy, tissue-to-light distance was regulated via limiting measures instead of a stepper motor, thus precluding precise speed control. Formalin fixation and subsequent histological processing induce protein cross-linking and cell shrinkage, but shrinkage was not quantified because all specimens were processed identically and only intraexperiment comparisons were intended. 50
Further investigations should systematically examine laser parameters (pulse width, pulse repetition frequency, scanning speed, line energy, and thermal dynamics) to characterize laser–tissue interactions. However, 980/1470 nm dual-wavelength laser presents practical barriers including stringent coupling precision requirements, safety oversight complexities, and elevated maintenance costs that warrant careful institutional evaluation.
Conclusions
For preclinical and clinical cutting-focused trials, CW mode with 24 W total power (980/1470 nm wavelength power ratio 8/16 W) is recommended, offering deep cutting (1249.3 ± 15.55 μm), sufficient vaporization (739.5 ± 35.32 μm), and minimal thermal injury (1987.53 ± 154.61 μm) relative to coagulation depth (1302 ± 125.44 μm). This study clarifies quantitative relationships between dual-wavelength laser parameters and liver resection key indices, establishing a foundation for standardized preclinical/clinical application and expanding lasers’ utility in precise minimally invasive partial liver resection.
Authors’ Contributions
Conceptualization: Y.L. Methodology: R.W. and L.P. Experiment implementation: Y.L., G.L., K.C., M.L., L.S., M.Z., and L.J. Data analysis and interpretation: Y.L. and G.L. Article writing: Y.L. and G.L. and Final approval of article: Y.L., R.W., and G.L. All authors read and approved the final article and agree to be accountable for all aspects of the research in ensuring that the accuracy or integrity of any part of the work is appropriately investigated and resolved.
Footnotes
Author Disclosure Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding Information
This work was financially supported by the Key Research and Development Program of Shaanxi (Project Nos. 2020ZDLSF04-08 and 2022ZDLSF04-09) and “Two—Chain Integration” Key Project of Shaanxi Science and Technology Department (Project No. 2021LL-JB-06).