
Abstract
Objective:
The aim of this study was to evaluate the clinical efficacy of intravenous laser irradiation of blood (ILIB) therapy as an adjunct treatment for patients with ischemic stroke.
Background:
Despite the diverse medical applications of ILIB, there was no strong evidence on the efficacy of ILIB for improving the clinical outcomes of ischemic stroke.
Methods:
A total of 22 patients with ischemic stroke were randomly assigned to either the ILIB or the control group. The ILIB group received intravenous laser therapy, whereas the control group received the same intervention but without the output power. The after outcome measures were assessed at baseline and at 3 days, 1 month, and 3 months post intervention: National Institute of Health Stroke Scale score, modified Rankin Scale score, Stroke Impact Scale (SIS) score, Fugl-Meyer assessment-Motor Function (FMA-MF) score, and 6-minute walking test (6-MWT) performance.
Results:
In total, 10 and 12 participants were randomized to the ILIB and control groups, respectively. Compared with the control group, the ILIB group showed significantly better SIS scores at the 3-month follow-up (p = 0.019), significantly higher FMA-MF scores at the 3-day and 3-month follow-ups (p = 0.003 and p = 0.022), and significantly better 6-MWT performance at the 3-day follow-up (p = 0.018).
Conclusions:
ILIB therapy provided short-term improvements in functional outcomes, including SIS, FMA-MF scores, and 6-MWT, in patients with ischemic stroke.
Introduction
Stroke is a major health issue and one of the leading causes of death and long-term disability worldwide.1,2 Stroke can be broadly classified into two main types: ischemic and hemorrhagic.2,3 Ischemic stroke, caused by the blockage of a cerebral artery, accounts for about 85% of all strokes. 3 Interrupted cerebral blood flow initiates an ischemic cascade that leads to progressive neuronal injury. 4 Oxidative stress concurrently arises from the overproduction of reactive oxygen species and free radicals, further compromising membrane integrity and mitochondrial function.4–6 Injury is compounded by activation of the inflammatory response, with microglia and infiltrating leukocytes releasing proinflammatory cytokines and reactive molecules.5,6 Ultimately, these processes result in neuronal apoptosis and necrosis. 6
Clinical symptoms, including hemiparesis or hemiplegia, aphasia, dysarthria, cognitive impairment, visual impairment, and disability, depend on the brain region affected and the extent of injury.2,7 Rehabilitation plays a vital role in promoting neuroplasticity, restoring lost function, and improving quality of life after stroke. Post-stroke rehabilitation encompasses various therapeutic approaches, including physical therapy, occupational therapy, and speech-language therapy.8–10 Emerging modalities, such as robotic-assisted therapy, virtual reality, and noninvasive brain stimulation, are also gaining attention for their potential to enhance recovery. 11 However, ∼40% of stroke survivors live with various disabilities despite multimodal rehabilitation interventions. 7 Therefore, effective novel treatments for ischemic stroke-related disability are continuously researched.
Intravenous laser irradiation of blood (ILIB), originally developed in the former Soviet Union in 1981, is a technique in which low-level laser light is administered directly into the bloodstream through an optical fiber inserted into a venous catheter.12,13 The most commonly used ILIB therapy is He–Ne laser with wavelengths of 630, 650, and 890 nm. 14 Through the inhibition of platelet aggregation and adhesion, the photodynamic reactions of ILIB can effectively reduce blood viscosity. 15 Further, ILIB enhances the function of erythrocytes by improving their oxygen-carrying capacity and deformability, thereby facilitating more efficient systemic oxygen transport.13,15,16 Thus, ILIB was originally utilized in the treatment of cardiovascular diseases, with the goal of promoting circulation and improving blood cells. 13
ILIB has also been shown to regulate immune responses by enhancing mitochondrial function in leukocytes. 17 It affects cellular redox reactions within the respiratory chain through mitochondrial activation. This subsequently modulates the synthesis and release of immune-related proteins, including immunoglobulins, interferons, and interleukins (ILs). 16 Accordingly, ILIB has been widely applied in the treatment of various diseases, such as stroke, fibromyalgia, musculoskeletal pain, insomnia, diabetes mellitus, metabolic diseases, and autoimmune diseases.12,13,15,16,18 Thus, ILIB appears to be a promising therapeutic option for patients with ischemic stroke.
However, robust evidence on the efficacy of ILIB for improving the clinical outcomes of ischemic stroke is rare. Hence, this study aimed to investigate the clinical outcomes of intravenous laser therapy in patients with ischemic stroke.
Materials and Methods
Study design
This study was designed as a double-blind, randomized controlled trial and was carried out from January 28, 2022, to August 31, 2024, with ethical approval obtained from the appropriate institutional review board of
Participants
Patients with ischemic stroke were recruited from the outpatient clinic of the Department of Physical Medicine and Rehabilitation. The inclusion criteria were as follows: (1) age 20–80 years, (2) diagnosis of ischemic stroke (duration: 1 month–2 years), (3) National Institute of Health Stroke Scale (NIHSS) score 0–15, (4) modified Rankin scale (mRS) score >1, and (5) clear consciousness and able to communicate. The exclusion criteria were as follows: (1) medical history of cancer, hemorrhagic stroke, hepatitis, unstable angina, coronary artery disease in the past 6 months, cranial surgery or other major surgeries, and mental illness; (2) uncontrolled infections; (3) intravenous thrombolysis; (4) pregnancy or breastfeeding; and (5) NIHSS score > 15 or mRS score < 1. Clinical history and physical examination were performed by a single physician.
Intervention
Participants were randomly assigned in a 1:1 ratio to either the ILIB group or the control group using a computer-generated randomized number. Participants assigned to the ILIB group underwent intravenous helium-neon laser therapy at a wavelength of 632.8 nm (Classconn helium-neon Laser System, Medipark, Korea). A peripheral vein in the antecubital fossa was cannulated using an indwelling needle, allowing insertion of a laser fiber catheter. The ILIB power was set between 2.5 mW and 3.0 mW, performed 60 min/session, energy 9–10.8 J/session, once daily for five consecutive days per week for 2 weeks, with a total of 10 interventions. The control group received the same intervention but without the output power. All participants received physical therapy and activities-of-daily-living training for 1 h each time, three times a week, during the study period. Participants remained unaware of their assigned groups during the course of the trial. The use of other types of therapies during the study period was assessed at each follow-up visit by one investigator.
Outcome measures
All outcomes were measured before the ILIB intervention and at 3 days, 1 month, and 3 months postintervention by an investigator blinded to group allocation. The outcome was set as intergroup differences in the improvement of outcome measures from preintervention to 3 months post-intervention.
Primary outcome measure
Modified Rankin Scale score
The mRS, originally developed in 1957 by Dr. John Rankin, is a widely used clinical tool for assessing the degree of disability in the daily activities of patients with stroke. 19 The mRS score ranges from 0 (no symptoms) to 6 (death). 19 The mRS has been established as a reliable tool for measuring functional outcomes in clinical trials for stroke. 20
Secondary outcome measures
National Institute of Health Stroke Scale score
The NIHSS, developed in the 1980s, is an assessment tool designed to measure neurological deficits in patients with ischemic stroke. 21 The NIHSS evaluates several domains of brain function, including motor strength, level of consciousness, gaze, visual fields, facial palsy, limb ataxia, sensory loss, language, dysarthria, and neglect. 22 The total score ranges from 0 to 42, with higher scores indicating more severe neurological impairment.21,22
Stroke Impact Scale score
The Stroke Impact Scale (SIS) is a comprehensive, patient-centered, self-reporting tool for evaluating the outcomes of recovery from stroke, including eight domains: physical abilities, cognitive function, emotion, communication, activities of daily living, mobility, hand function, and social participation. 23 We used SIS version 3.0, which consists of 59 items. Each item is rated on a 5-point Likert scale, where 1 indicates “could not do it at all” and 5 indicates “not difficult at all. Higher scores indicate better function and less impact from stroke. 23
Fugl-Meyer Assessment-Motor Function
The Fugl-Meyer Assessment-Motor Function (FMA-MF) subscale evaluates movement, reflexes, and coordination of the upper and lower extremities post stroke.24,25 It includes 33 items for the upper limbs (maximum score = 66) and 17 items for the lower limbs (maximum score = 34), with a total motor domain score of 100.24,25 Higher scores indicate better motor function.
6-min walking test performance
The 6-min walk test (6-MWT) is a widely used functional evaluation tool that quantifies the distance an individual can walk over a flat surface within 6 min. 26 It reflects the submaximal level of functional capacity, making it particularly useful for assessing endurance and aerobic capacity in patients with cardiovascular, pulmonary, neurological, and musculoskeletal conditions. 26
Sample size calculation
Because no prior randomized controlled trial has evaluated ILIB in stroke populations, we followed CONSORT recommendations for early-phase pilot trials and derived the effect size from the closest available ILIB randomized trial, in which the WOMAC scale was used as the primary outcome for the sample size calculation. 27 The sample size calculation was performed using STATA software (power analysis for a two-sample means test), with a significance level of α = 0.05 and a power (1–β) = 0.80. The effect size was calculated by the control (39.2 ± 17.5) and experiment groups (20.9 ± 8.4). 27 The required sample size was estimated to be 22 participants. The final analyzed sample (n = 22) met the minimum requirement for statistical analysis.
Statistical analysis
The Mann–Whitney U test, chi-square test, or Fisher’s exact test was used to analyze continuous and categorical data. Intergroup comparisons of mean differences across different time points were conducted using the independent t-test or Mann–Whitney U test. Meanwhile, intragroup comparisons of baseline data were performed using the Wilcoxon signed-rank test. All statistical analyses were conducted using SPSS Statistics, Version 22 (IBM Corp., Armonk, NY, USA), with a significance level set at p < 0.05.
Results
A total of 22 of the 27 participants were ultimately enrolled in the study. Among them, 12 and 10 participants were randomized to the ILIB and control groups, respectively (Fig. 1). There were no significant between-group differences in baseline characteristics, except that the number of patients with hypertension being higher in the control group (7 vs. 10, p < 0.05, Table 1). The mean patient age was 63.75 ± 8.8 years in the ILIB group and 61.8 ± 10.5 years in the control group.
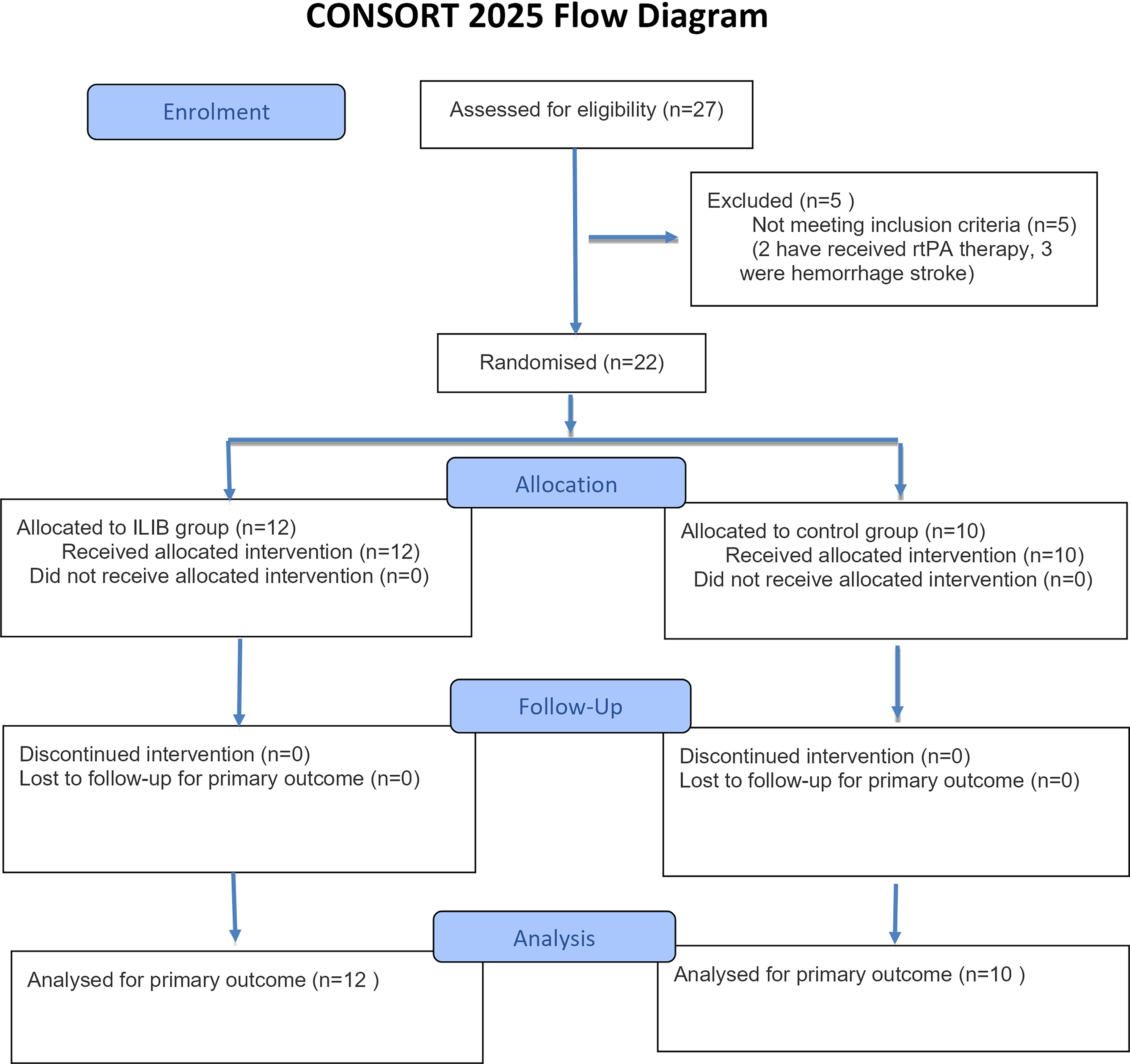
Study flow diagram. ILIB, intravenous laser irradiation of blood.
Demographic Information
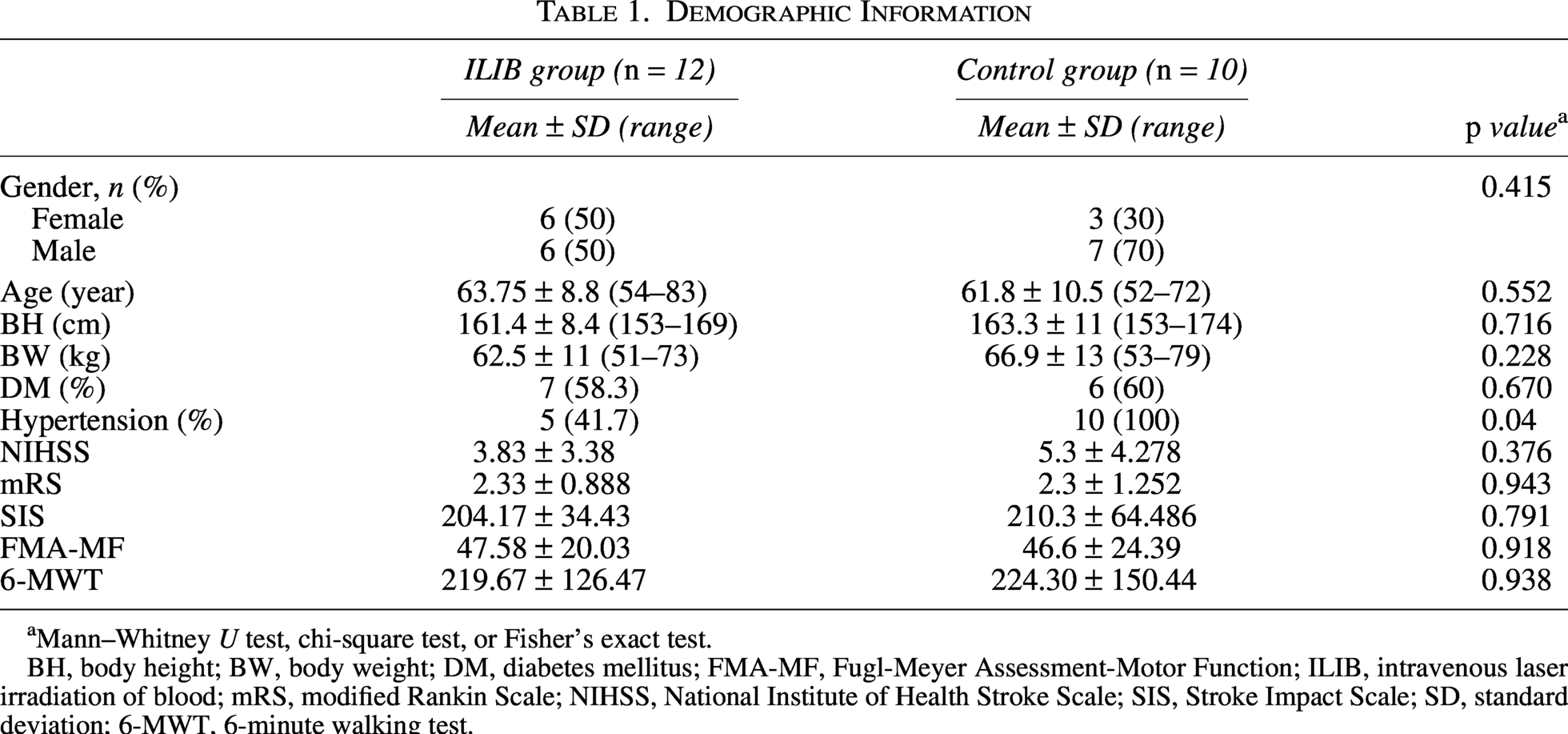
Mann–Whitney U test, chi-square test, or Fisher’s exact test.
BH, body height; BW, body weight; DM, diabetes mellitus; FMA-MF, Fugl-Meyer Assessment-Motor Function; ILIB, intravenous laser irradiation of blood; mRS, modified Rankin Scale; NIHSS, National Institute of Health Stroke Scale; SIS, Stroke Impact Scale; SD, standard deviation; 6-MWT, 6-minute walking test.
Table 2 presents the NIHSS, mRS, SIS, and FMA-MF scores, as well as 6-MWT performance pre- and postintervention in both groups. In the ILIB group, mRS scores were significantly lower at all follow-up time points than at baseline (all p < 0.05). SIS scores were significantly better at the 3 months post intervention than at baseline (p = 0.013, p < 0.05). FMA-MF scores were significantly higher at 3 days and 3 months post intervention than at baseline (p = 0.007, p = 0.009, p < 0.001). Finally, the 6-MWT performance was also significantly better at 3 days and 1 month post intervention than at baseline (p = 0.033, p = 0.026). However, there was no significant improvement in NIHSS scores at all follow-up time points (all p > 0.05). For the control group, the mRS, SIS, and FMA-MF scores, as well as 6-MWT performance at baseline were not significantly different than those at all follow-up time points (all p > 0.05). Only the NIHSS score showed significant improvement at the 1- and 3-month follow-ups (p = 0.014, p = 0.008).
Comparison of Changes of National Institute of Health Stroke Scale, Modified Rankin Scale, Stroke Impact Scale, Fugl-Meyer Assessment-Motor Function, and 6-Minute Walking Test Before and After Treatment in Both Group
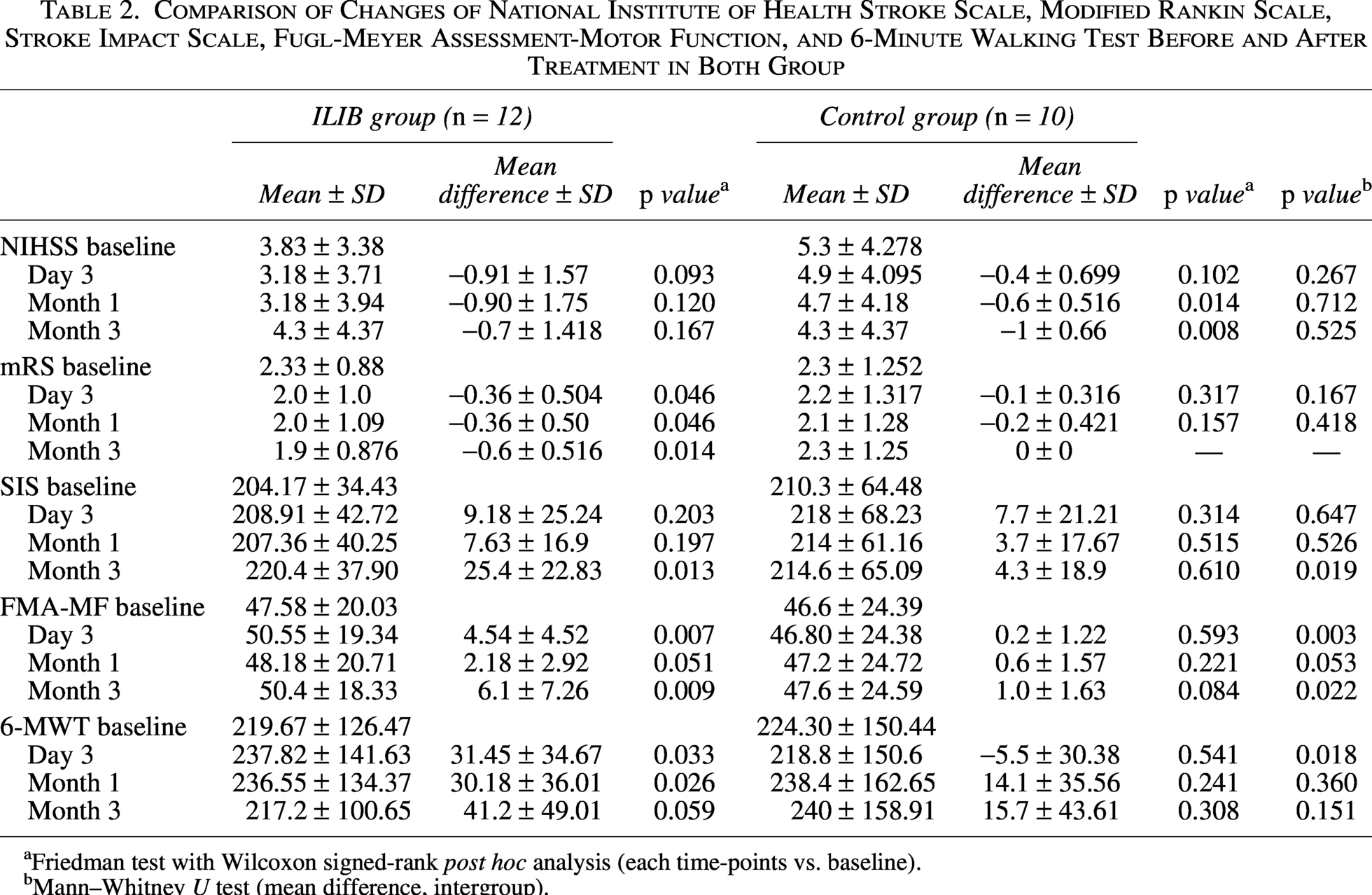
Friedman test with Wilcoxon signed-rank post hoc analysis (each time-points vs. baseline).
Mann–Whitney U test (mean difference, intergroup).
In Figure 2, compared with the control group, the ILIB group showed significantly better SIS scores at the 3 month follow-up (p = 0.019, respectively). However, there was no significant between-group difference in NIHSS at all follow-up time points (all p > 0.05) and no significant between-group difference in mRS score at 3 day and 1-month follow-up time points (p > 0.05). In Figure 3, FMA-MF scores were significantly higher in the ILIB group than in the control group at the 3-day and 3-month follow-ups (p = 0.003 and p = 0.022). Further, the ILIB group also performed significantly better in the 6-MWT than did the control group at the 3-day follow-up (p = 0.018). No adverse events occurred during the study, and none of the participants received additional conservative treatment.
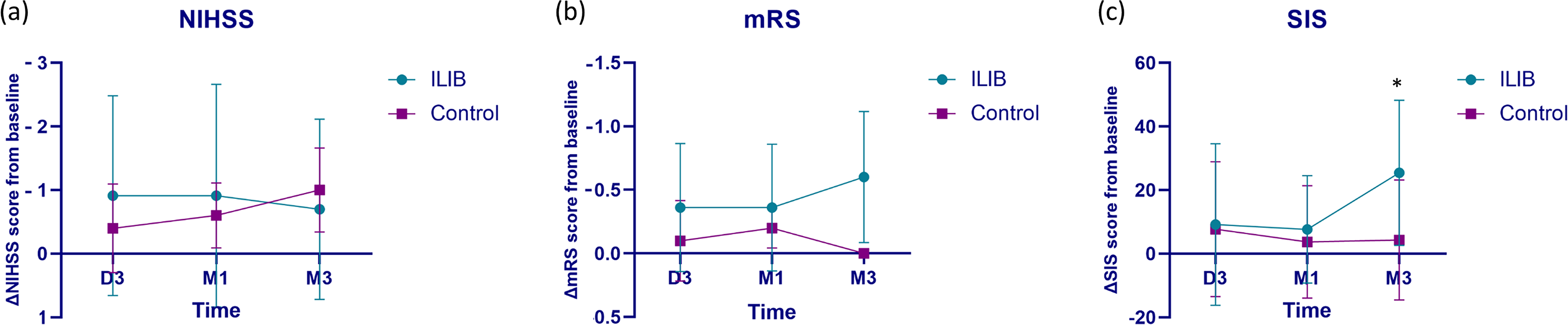
Mean difference at baseline and post-therapy in the National Institute of Health Stroke Scale (NIHSS), modified Rankin Scale (mRS) and Stroke Impact Scale (SIS) in both groups.
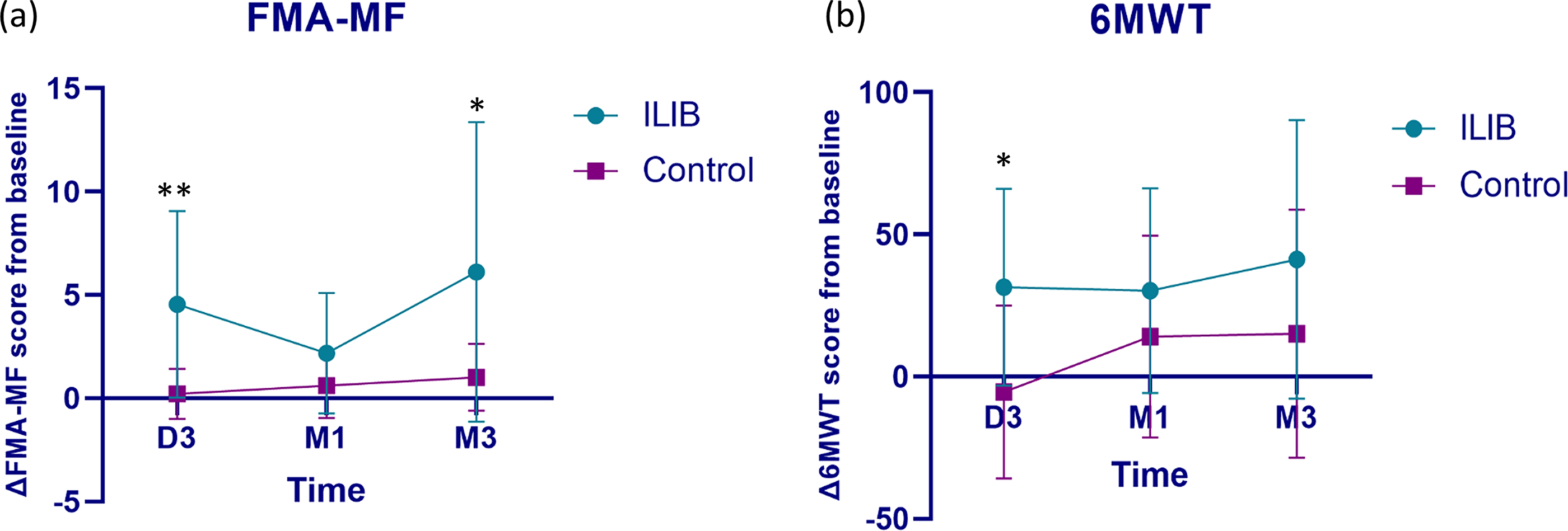
Mean difference at baseline and post therapy in Fugl-Meyer assessment-Motor Function (FMA-MF) and 6-minute walking test (6-MWT) in both groups.
Discussions
To the best of our knowledge, this study is the first double-blind randomized controlled trial to investigate and confirm the clinical effectiveness of ILIB therapy in ischemic stroke patients. The present study shows that ILIB can improve motor function and reduce disability within 3 months post intervention in patients with ischemic stroke. SIS and FMA-MF scores were significantly better in the ILIB group than in the control group at the 3-month follow-up. In addition, FMA-MF scores and 6-MWT performance were significantly better in the ILIB group than in the control group at the 3-day follow-up. However, there was no significant NIHSS improvement during the 3 months follow-up. The absence of significant NIHSS improvement may be attributed to its lower sensitivity for detecting subacute motor recovery, whereas the FMA-MF and SIS capture more motor functional changes.
ILIB therapy improves functional status in ischemic stroke possibly through the after mechanisms. First, ILIB may increase vascular microcirculation, decrease blood viscosity, and increase cerebral blood flow by improving the vascular endothelium. 28 An animal study also demonstrated that transcranial photobiomodulation using a low-power near-infrared laser improved cerebral blood flow and stroke outcomes via endothelial nitric oxide (NO) synthase phosphorylation. 29 Further, a case report showed marked improvements in muscle power, decreased level of homocysteine, and increased blood flow in the ischemic cerebral area after three courses of ILIB treatment in a subacute stroke patient. 30
Another case report showed improvement in crossed cerebellar diaschisis during the subacute poststroke stage after a course of ILIB therapy. 31 De Scheerder et al. also found that ILIB therapy could reduce the restenosis rate after coronary stenting procedures.32,33 Collectively, these results indicate that ILIB therapy can increase endothelial function and microcirculation and decrease blood viscosity. This further increases cerebral blood flow to improve motor function and decrease disability in patients with ischemic stroke. In an observational study, patients with ischemic stroke who received ILIB plus conventional rehabilitation showed more improved Barthel Index scores, 6-MWT, and FMA-upper extremity scores than those who received conventional rehabilitation group, although the difference was not significant. 34
Second, ILIB therapy may modulate the immune response in ischemic stroke patients. Several inflammatory cytokines and chemokines participate in immune regulation; these include ILs, tumor necrosis factor-α (TNF-α), eotaxin, and macrophage inflammatory protein-1β. These cytokines and chemokines play an important role in modulating immune responses and inflammation after ischemic stroke.35,36 IL-1β stimulates the activation of microglia, which aggravates the inflammatory response and promotes apoptosis of damaged neurons. 35 Kazemikhoo et al. also found that ILIB therapy could inhibit epidermal growth factor receptor (EGFR) expression. This, in turn, decreased arginase expression, increased NO production, improved vasodilation, and decreased nerve inflammation in diabetes patients. 12 Inhibition of the EGFR/mitogen-activated protein kinase signaling pathway has been shown to reduce the production of proinflammatory cytokines TNF-α and IL-1β in microglia after spinal cord injury. 37
A randomized controlled trial also demonstrated that ILIB therapy can reduce blood concentrations of IL-1β and IL-13 for up to 3 months and relieved pain for up to 1 month in patients with knee osteoarthritis. 27 ILIB reduced TNF-α expression in animal studies with experimentally induced acute inflammation in the lungs.38,39 A systematic review of six articles also concluded that ILIB could increase the levels of anti-inflammatory cytokines, decrease those of proinflammatory cytokines, and increase NO production. 40 Overall, ILIB therapy may decrease inflammatory cytokines and chemokines, decrease nerve inflammation, increase microcirculation, and further improve motor functions and reduce disability in ischemic stroke patients.
The present study has several limitations. First, the sample size was small; therefore, the results should be interpreted as preliminary efficacy signals rather than definitive conclusions. Future multicenter studies with larger sample sizes studies are warranted to validate the therapeutic effects of ILIB in ischemic stroke. Second, outcomes were only monitored for 3 months; long-term follow-up is needed to assess the sustained effects of ILIB therapy beyond this timeframe. Third, only one course of ILIB therapy was administered, highlighting the need for further research on the cumulative therapeutic benefits of multiple courses. Fourth, although the ILIB parameters (wavelength, output power, and duration) were controlled in this study, the optical fibers used for ILIB therapy are not standardized, leading to variability in energy density and power density delivered during treatment. This technological limitation should be addressed in future clinical trials. Lastly, the biological mechanism of changes, such as mitochondrial functions, after ILIB therapy in patients with ischemic stroke was not clarified, necessitating further research.
Conclusions
ILIB therapy may offer short-term benefits in the functional outcomes, including SIS, FMA-MF scores, and 6-MWT performance of patients with ischemic stroke. Additional studies with larger sample sizes and longer follow-up periods are needed to confirm clinical efficacy.
Authors’ Contributions
Y.-C.S.: Conducted the study, interpretation of data, and drafted the article. L.-C.C. and Y.-C.S.: Conceptualized the study. C.-Y.C., T.-C.C., W.-Y.C., and C.-Y.H.: Conducted the study. K.-T.P. and S.-M.H.: Analyzed and interpreted the data. All authors edited, revised, and approved the final version of the article.
Ethical Approval Details
This study was approved by the institutional review board of
Footnotes
Acknowledgments
The sponsor had no role in the study design, data collection and analysis, decision to publish, or preparation of the article.
Author Disclosure Statement
The authors declared no potential conflicts of interest.
Funding Information
This study was supported by the