
Abstract
Background
Primary vaginal melanoma is a rare malignancy, accounting for less than 1% of all melanomas in women. In contrast to cutaneous melanomas, mucosal tumors are not associated with ultraviolet (UV) radiation, have distinct clinical courses and biological/mutational profiles, rarely harbor B-Raf proto oncogene (BRAF) mutations, and ultimately respond poorly to standard therapy regimens. Here, we present the case of metastatic primary vaginal mucosal melanoma harboring co-occurring sensitizing and resistance-associated mutations in the KIT gene.
Case Presentation
A 68-year-old postmenopausal woman presented with pelvic pain and a vaginal mass. Biopsy confirmed a diagnosis of mucosal melanoma and concurrent vulvar melanoma in situ. Positron emission topography (PET)/computed tomography (CT) revealed widely metastatic disease, and she was transferred to our care. A liver biopsy was performed to confirm metastatic disease and obtain tissue for molecular profiling. Next-generation sequencing (OmniSeq INSIGHT, Labcorp; Buffalo, NY) demonstrated co-occurring KIT mutations (L576P and V654A), low tumor mutational burden (7.1 mut/Mb), and no evidence of BRAF mutation. She was treated with nivolumab plus relatlimab-rmbw. The patient experienced disease progression and received palliative radiation, which failed to provide symptomatic relief. The patient expired less than six months after diagnosis.
Conclusion
This case demonstrates the unique features and care limitations of mucosal melanomas. To our knowledge, co-occurring KIT L576P AND V654A mutations in a treatment-naïve primary vaginal melanoma have not been described in previous reports. This finding underscores the complexity of molecular profiling in guiding treatment decisions.
Introduction
Although less common than basal cell carcinoma or squamous cell carcinoma, malignant melanomas are responsible for more deaths than all other skin cancers combined. 1 In the United States, over 100,000 new cases and more than 8,000 deaths are reported annually.1, 2 When detected at an early-stage (I-II), the five-year survival rate exceeds 97%; however, for metastatic disease, the five-year survival rate drops to approximately 16%. 3 Mucosal melanomas comprise less than 2% of all melanomas.4, 5 Although mucosal melanomas constitute a greater proportion of melanomas diagnosed in Black, Asian, and Hispanic individuals, the absolute incidence is higher in the Caucasian population. 6 Among mucosal melanomas, those arising from the female genital tract account for only 0.3%-0.8% of all melanomas in women and predominantly affect postmenopausal women.5, 7 These tumors carry a dismal prognosis, with five-year survival rates ranging from 0% to 25%. 8
The molecular and etiologic profile of female genital tract melanomas differs markedly from that of cutaneous melanomas. Mucosal melanomas are not associated with ultraviolet radiation exposure or human papillomavirus infection. 9 B-Raf proto oncogene (BRAF) mutations, which are common in cutaneous melanomas, are rare in mucosal melanomas; instead, alterations in KIT and SF3B1 are more frequently observed.10-12 Because of its rarity and distinct biological behavior, treatment guidelines for mucosal melanomas are not standardized and disease-specific, and further research is needed to address this gap.4, 13 Here, we report a case of metastatic primary vaginal melanoma in a postmenopausal woman, highlighting the diagnostic and therapeutic challenges associated with this rare malignancy.
Case Presentation
A 68-year-old female presented to her gynecologist in India with pelvic pain and recurrent urinary tract infections. She had a history of type II diabetes and a hysterectomy in 2008 for excessive vaginal bleeding. She had three pregnancies and three vaginal deliveries. She reported no history of alcohol or tobacco use, and there was no known family history of malignancy.
On physical examination, a dark brown nodular mass was seen protruding from the introitus and confirmed on vaginal exam to be present in the anterior vaginal wall. A hard, 3 × 3 cm left inguinal lymph node was also found. Her Papanicolaou test (PAP) smear history was unremarkable. Biopsy of the vaginal lesion was consistent with mucosal melanoma. Biopsy of the vaginal lesion was consistent with invasive mucosal melanoma, while a concurrent biopsy of the vulva demonstrated melanoma in situ. Based on the presence of an invasive, bulky vaginal mass and the absence of invasion in the vulvar specimen, the vaginal lesion was designated as the primary tumor, with the vulvar melanoma in situ interpreted as synchronous multifocal disease rather than the primary site.
The patient moved back to the United States for further evaluation and treatment, at which point she entered our care. At this time, she reported increasing difficulty with both bowel movements and urination, occasional hematuria after straining, and had experienced weight loss (~14 lbs.). Physical exam was notable for a palpable left inguinal lymph node and right upper quadrant tenderness; the liver was not palpable, and no supraclavicular lymphadenopathy was appreciated. The patient had an eastern cooperative oncology group (ECOG) performance status of one. Laboratory evaluation demonstrated a hemoglobin level of 14.3 g/dL, mildly decreased albumin of 3.3 g/dL, and normal liver enzymes.
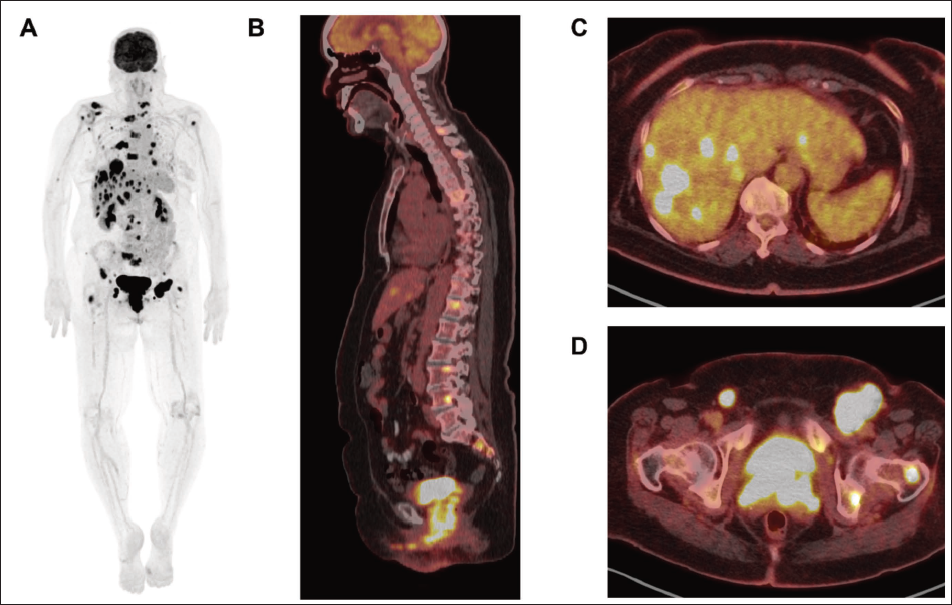
CT imaging was performed and showed hepatic and pulmonary lesions. Positron emission topography (PET)/computed tomography (CT) demonstrated fluorodeoxyglucose (FDG)-avid bilateral pulmonary nodules, left hilar lymph nodes, a large cervical/vaginal/vulvar mass, hepatic lesions, bilateral pelvic and inguinal lymph nodes, multifocal osseous lesions including vertebral metastases, an interventricular septal focus, and a probable right pectineus intramuscular nodule, all consistent with metastatic disease (Figure 1). Of note, the possibility of cardiac metastatic disease was considered, but further workup was not pursued as it would not impact treatment decisions. magnetic resonance imaging (MRI) of the brain showed no intraparenchymal brain metastases.
PET/CT Staging at Initial Presentation. (A) MIP Image Demonstrating Widespread FDG-avid Metastatic Disease Involving Bilateral Pulmonary Nodules, Left Hilar Lymph Nodes, Interventricular Septal Region, Hepatic Lesions, Cervical/Vaginal/Vulvar Mass, Bilateral Pelvic and Inguinal Lymph Nodes, Multifocal Osseous Lesions, and a Probable Right Pectineus Intramuscular Nodule. (B) Sagittal Fused PET/CT Showing Spinal Metastases and the Cervical/Vaginal/Vulvar Mass. (C) Axial Fused PET/CT Showing Multiple Hepatic Metastases. (D) Axial Fused PET/CT Showing the Vaginal/Cervical Mass and Bilateral Inguinal Nodal and Left Femoral/Acetabular Metastases.
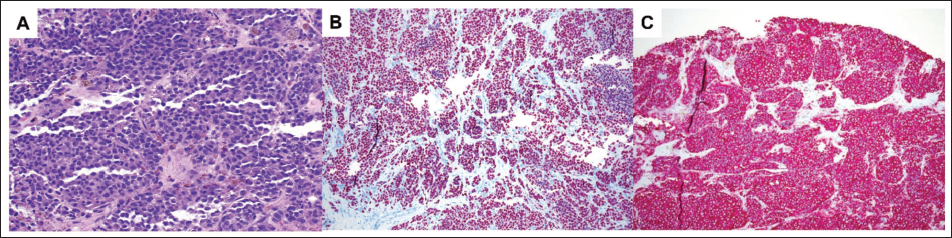
Formal American Joint Committee on Cancer staging is not available for vaginal melanoma; however, the extent of disease was consistent with widely metastatic (stage IV) melanoma. To confirm the presence of metastatic disease, a liver biopsy was performed, which showed a poorly differentiated malignant epithelioid neoplasm with focal intracytoplasmic brown pigment (Figure 2). Tumor cells demonstrated expression of SOX10, HMB45, and S100 (focal staining). The morphology and immunohistochemical profile were consistent with metastatic melanoma. Next-generation sequencing (OmniSeq INSIGHT, Labcorp; Buffalo, NY) demonstrated the following pathogenic single-nucleotide variants: CTNNB1 S33Y (c.98C>A; variant allele frequencies [VAF], 41.0%), KIT L576P (c.1727T>C), KIT V654A (c.1961T>C). Microsatellite sequencing demonstrates stable disease (4 of 121 microsatellite sites unstable, 3.3%). Overall, the tumor had a low tumor mutational burden (7.1 mut/Mb). No rearrangements or definitive copy number variants were observed. PD-L1 immunohistochemistry (22C3 antibody clone) demonstrated a tumor proportion score of <1%.
Histopathology and Immunohistochemistry of Liver Biopsy Confirming Metastatic Melanoma. (A) Sheets of Poorly Differentiated Malignant Epithelioid Cells with Focal Intracytoplasmic Brown Melanin Pigment (H and E, 20×). (B) Diffuse Nuclear Positivity for SOX10 (SOX10 Immunohistochemistry, 10×). (C) Diffuse Positivity for HMB45 (HMB45 Immunohistochemistry, 10×).
Treatment options, including nivolumab plus ipilimumab, single‑agent immune checkpoint inhibition, and nivolumab plus relatlimab‑rmbw, were discussed in detail with the patient and her daughter, including anticipated benefits and toxicity profiles. Given the patient’s widespread and symptomatic metastatic disease, a combination immunotherapy regimen was felt to be more appropriate than single‑agent therapy. Due to concerns regarding the higher toxicity associated with dual CTLA‑4/PD‑1 blockade and the patient’s preference for a regimen with a more favorable safety profile, nivolumab plus relatlimab‑rmbw was selected, supported by data from the RELATIVITY‑047 trial demonstrating improved progression‑free survival with reduced high‑grade immune‑related adverse events compared with nivolumab plus ipilimumab. 24 At the time of treatment initiation, comprehensive molecular profiling results were still pending, and therapy was started promptly in the setting of rapidly progressive disease. Although treatment was initially well tolerated, the patient experienced rapid disease progression. Subsequent palliative radiation therapy did not provide meaningful symptomatic benefit, and the patient ultimately elected hospice care, passing away less than six months after diagnosis.
Discussion
Primary vaginal melanoma is a rare malignant tumor of the female reproductive tract. Primary vaginal melanoma is a rare malignant tumor of the female reproductive tract. Before contextualizing the molecular and therapeutic considerations, it is important to emphasize the markedly aggressive and rapidly progressive clinical course in this case. The patient was initially diagnosed in India on September 28, 2024, and transferred her care to the United States in October 2024. Staging PET/CT and confirmatory liver biopsy were performed in November 2024, after which systemic immunotherapy was initiated on November 19, 2024. Despite treatment, the patient experienced progressive urinary and vaginal symptoms requiring palliative radiation therapy, which was completed in late January 2025. Her disease continued to progress, and she ultimately entered hospice care, passing away in early March 2025, less than six months from the time of initial diagnosis. This compressed clinical trajectory underscores both the biologic aggressiveness of vaginal mucosal melanoma and the limited opportunity for sequential therapeutic interventions.
The first reported case of vaginal melanoma was in 1887. 8 Vaginal mucosal melanomas often present with vaginal bleeding, vaginal mass, painful intercourse, or obstructive symptoms, 7 and the most common site of presentation is the anterior wall of the vagina. 8 Since these melanomas can be bland and amelanotic, clinicians should have a low threshold for further workup in the setting of a suspicious vaginal mass. 14
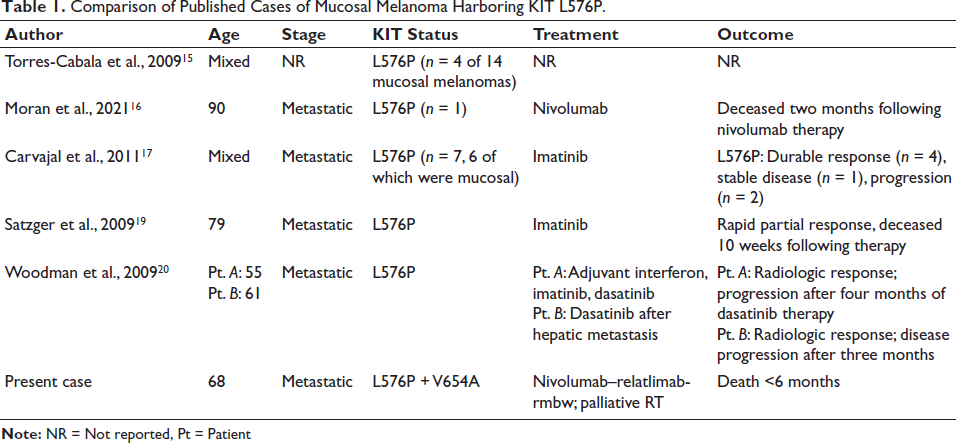
Several published cases of mucosal melanomas harboring KIT L576P allow comparison with the present case (Table 1).15-19 To our knowledge, our patient’s co-occurrence of KIT L576P and V654A has not been previously reported in a vaginal primary, nor has the use of nivolumab plus relatlimab-rmbw in this tumor type. KIT L576P is a common activating mutation located in exon 11, which encodes the juxtamembrane domain of the KIT receptor, and this alteration leads to constitutive activation of the kinase domain and downstream activation of mitogen-activated protein kinase (MAPK) and PI3K/AKT pathways. In contrast, KIT V654A has been documented in imatinib-resistant cases, and it is a common resistance mechanism typically seen secondary to imatinib exposure. Importantly, in our case, there was no known history of imatinib treatment. Moreover, both alterations co-occurred with similar VAFs (59.4% for L576P and 61.2% for V654A), providing evidence for their co-occurrence in tumor cells. This constellation effectively represents a tumor harboring both an activating KIT oncogenic driver and a primary resistance alteration, limiting the therapeutic utility of KIT-targeted inhibition. The clinical significance of KIT V654A in a treatment-naïve tumor is itself a surprising finding and would likely have reduced the efficacy of KIT-directed therapy in our patient.17, 20
The rapid clinical decline observed in our case is consistent with other reports showing no significant improvement in survival for vaginal melanoma patients, even in the immunotherapy era. 18 Currently, there are no well-established, site-specific guidelines for the standard treatment of vaginal mucosal melanomas. Recommendations have extrapolated evidence from cutaneous melanomas and must be interpreted with the understanding that mucosal melanomas do not have the same response rates or outcomes. Localized lesions can be treated surgically, and wide excision is most often preferred to more radical procedures. 13 Due to the low risk of lymph node metastatic disease in early-stage disease, lymphadenectomy is generally not recommended in this context. Of course, patients may present with definitive metastatic disease, as in the case described, raising important clinical questions about chemotherapy, particularly which agents should be used and for what indications. Most vaginal mucosal melanomas demonstrate low tumor mutational burden, and BRAF mutations are relatively rare at this site. Therefore, BRAF-directed therapies are typically not indicated.
Comparison of Published Cases of Mucosal Melanoma Harboring KIT L576P.
Conclusion
This case underscores the potential limitation of molecularly targeted therapy in the presence of concurrent activating and resistance-associated mutations, emphasizing the need for integrated genomic interpretations and rare malignancies. Vaginal melanoma is a rare malignancy with a poor prognosis compared to cutaneous melanoma and other vaginal malignancies. Due to the rare occurrence of mucosal melanomas, there are no standard staging or treatment guidelines. This case highlights several key clinical considerations: (a) Vaginal melanoma can present with widely metastatic disease at diagnosis; (b) molecular profiling is essential as it may reveal actionable but complex mutations; and (c) prognosis remains dismal, despite modern immunotherapy, and more effective treatments are needed.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics and Consent Statement
Written and informed consent was obtained from the patient’s next of kin for publication of this case report and accompanying images. Institutional ethics approval was not required for a single case report in the setting of informed consent.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.