
Abstract
Introduction
The high cost and complexity of cancer care create substantial financial burdens for patients. We examined the relationship between insurance coverage, treatment patterns, and survival outcomes among adults with hematologic malignancies.
Methods
We queried an institutional cancer registry for adults (≥18 years) with histologically confirmed acute lymphocytic leukemia, acute myeloid leukemia, chronic lymphocytic leukemia, chronic myelogenous leukemia, multiple myeloma, or non-Hodgkin lymphoma treated between 2015 and 2022. Sociodemographic factors, comorbidities, behavioral factors, treatment modality, disease status, and survival were analyzed. Survival differences by insurance were assessed using log-rank testing and univariable and multivariable Cox proportional-hazards models.
Results
Among 2,516 patients (mean age 62.3 years; 55.7% male; 78.1% White), most had Medicare (50.5%) or private insurance (39.6%). Survival differed significantly by insurance (P < .001). Compared to private insurance, higher mortality risk was observed among uninsured (Hazard Ratio (HR) = 1.96, P = .008), Medicaid (HR = 1.75, P < .001), and Medicare patients (HR = 1.26, P = .017). Higher mortality was also associated with not receiving stem cell transplantation. Lower mortality was observed among patients who did not receive chemotherapy or palliation, reported current alcohol use, or had a positive family history.
Conclusion
Insurance status significantly influenced survival. Uninsured and publicly insured patients were most vulnerable, highlighting the need for policy reforms for equitable access to high-quality cancer care.
Introduction
Hematological malignancies can originate from the blood, bone marrow, and/or the lymphatic system. The three main classes of hematological malignancies are leukemia, lymphoma, and multiple myeloma. By interfering with the body’s ability to produce properly functioning red blood cells, platelets, and/or white blood cells, hematological malignancies place these patients at high-risk for developing anemia, bleeding, and severe infection.
Insurance status has been shown to have a significant effect on outcomes of hematological malignancies, influencing access to care, treatment adherence, and overall survival rates. 1 Unfortunately, the complexity and high cost of treatment for patients with hematological malignancies pose a significant financial burden on patients and their families. Medical insurance coverage plays a crucial role in providing access to life-saving cancer treatments, and this is particularly important for individuals of lower socioeconomic status and patients in rural states. Multiple studies have shown that uninsured patients are more likely to present with advanced-stage cancers and have a poorer survival rate in comparison to insured patients. 1
The objective of this retrospective study is to examine the relationship between medical insurance status and its influence on the treatment regimen and clinical outcomes of patients with hematological malignancies in a single academic institution in a rural state. We hypothesized that patients with public insurance or no insurance would have lower survival rates than those with private insurance.
Methods
We conducted a retrospective cohort study using institutional cancer registry data to examine the relationship between insurance status and clinical outcomes in patients with hematologic malignancies.
This study was deemed exempt by our Institutional Review Board (#275855). Data queried from the institutional cancer registry included cases of histologically confirmed acute lymphocytic leukemia (ALL), acute myeloid leukemia (AML), chronic lymphocytic leukemia (CLL), chronic myelogenous leukemia (CML), myeloma, and non-Hodgkin’s lymphoma among ages ≥18 years that received treatment between 2015 and 2022. Data from subjects with incomplete follow-up records or who did not have comorbidity data were excluded. The institutional cancer registry data recorded insurance status, the primary exposure of interest, at the time of diagnosis, and followed patients from the date of diagnosis until death or last known follow-up, with survival outcomes ascertained through 2022.
Demographics that were available from the registry included age at diagnosis, sex, race (White, Black, and other), family history of hematological malignancy, insurance type (Medicaid, Medicare, military, and private), family history, tobacco history, and alcohol history, Elixhauser comorbidity score, 2 and VAN index which assigned a weight to each comorbidity based on the significance of its impact on general health to help minimize potential confounders. 2 Available cancer-related data included treatment modality, cancer status, survival in months, and number of treatments. Treatment modalities included surgery, radiation, chemotherapy, immunotherapy, hematological transplant, endocrine treatment, and palliative care/other.
Statistical Methods
Descriptive statistics were calculated for the overall sample and for each insurance type following data cleaning and preprocessing. To determine if there were baseline differences between insurance type groups, analysis of variance (ANOVA) was utilized for quantitative variables, and chi-square tests were used for categorical variables. In cases where assumptions were not met, Kruskal-Wallis tests (a non-parametric alternative to the ANOVA) were utilized for quantitative variables and, in the case of categorical variables, the P value for differences was computed for the chi-square tests using a Monte Carlo test with 10,000 replicates. Post-hoc group comparisons were made when necessary.
A log-rank test was utilized to compare the survival curves between the insurance type groups. Univariable Cox proportional-hazards regression analysis was also utilized. Descriptive statistics for the overall survival curve and for the survival curves of each of the insurance type groups were calculated. Multivariable Cox proportional-hazards regression analysis was used to examine the relationship between survival and insurance type, when additionally accounting for demographics such as age, race, and sex. Missing data would have been handled via listwise deletion followed by a sensitivity analysis to assess the impact of this missingness. However, there was no missing data for the variables included in our models and, consequently, no sensitivity analysis was performed. The assumption of proportional-hazards was evaluated for covariates using graphical methods such as log-log survival plots. All analyses were conducted using R version 4.3.3 with statistical significance defined as P < .05.
Results
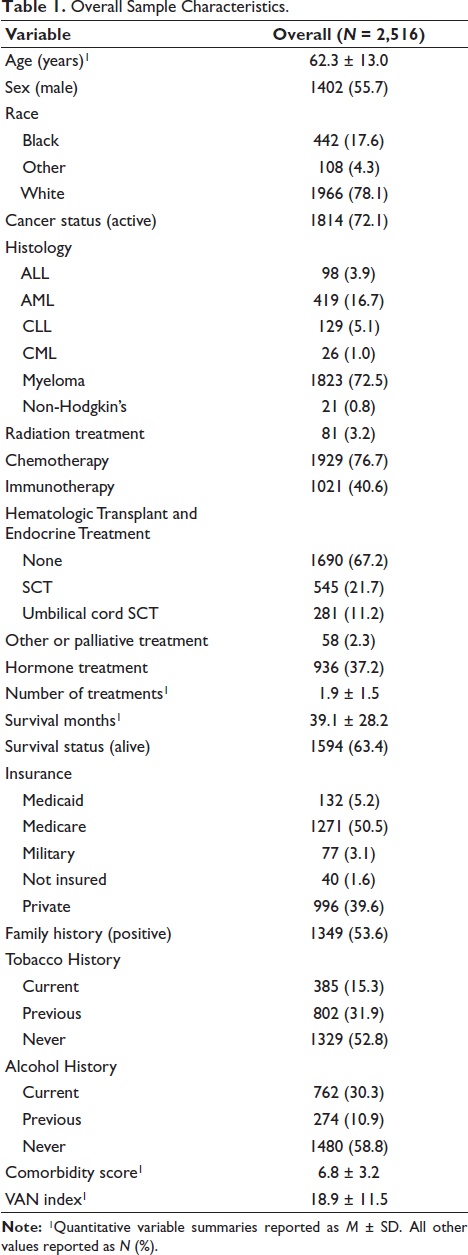
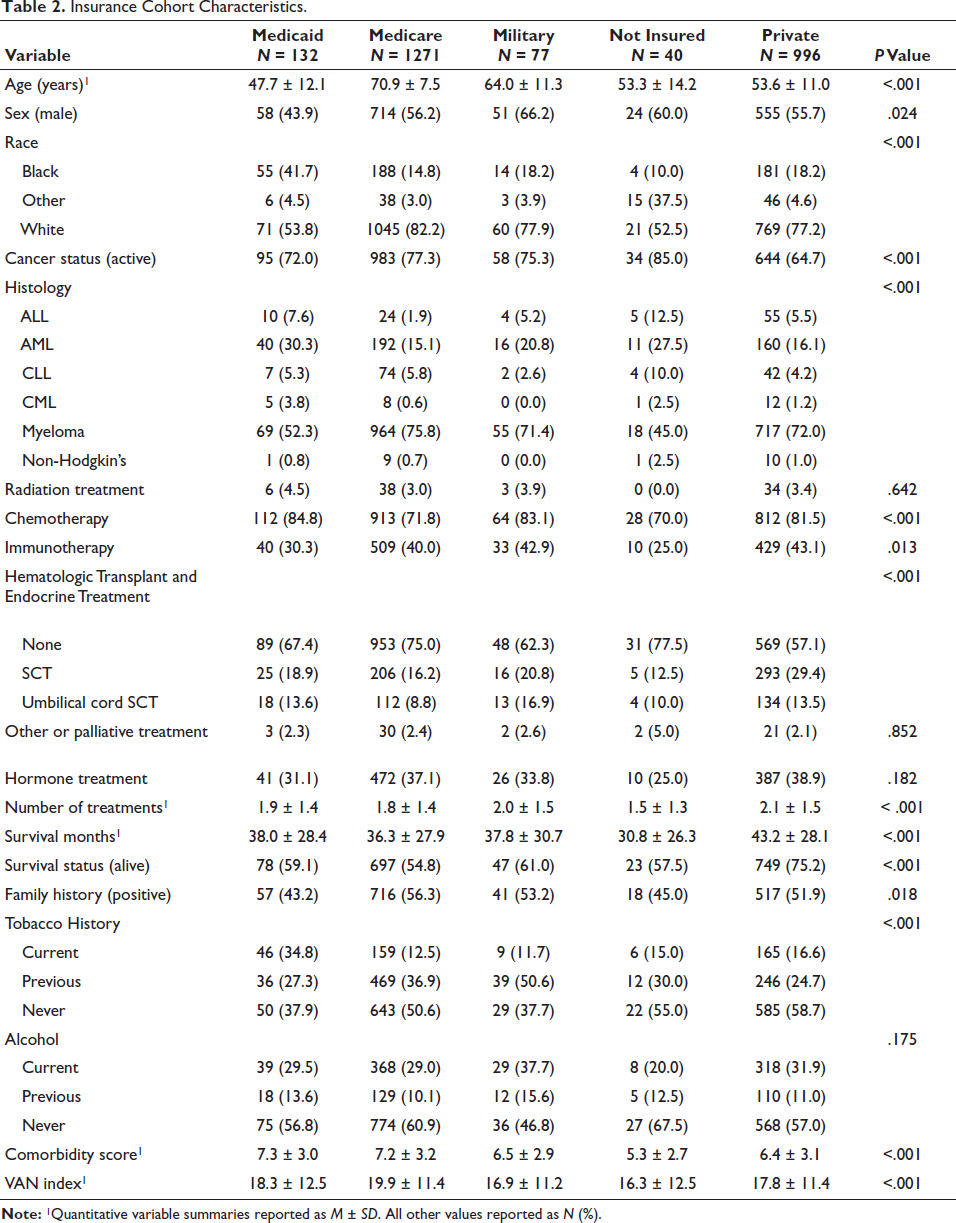
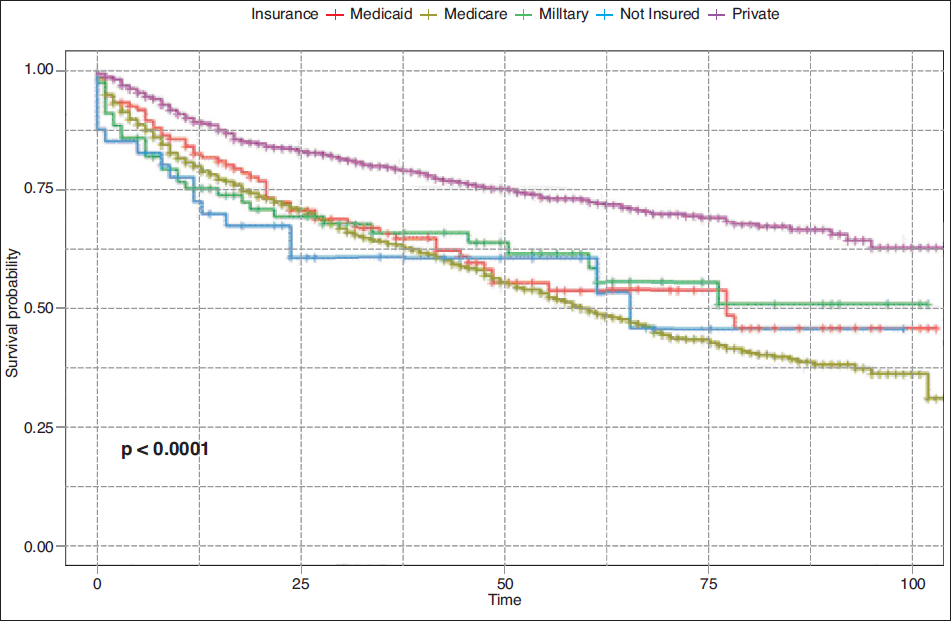
A total of 2,575 patients with hematological malignancies were identified from the cancer registry. Only the 2,516 patients who met the inclusion criteria, had complete follow-up records, and had comorbidity data were included in the final analysis. The mean survival was 39.1 ± 28.2 months. During the follow-up period, 922 deaths occurred among the 2,516 patients included in the analysis. Demographic details can be found in Table 1. Insurance cohorts differed significantly in all study variables except alcohol history and the receipt of radiation, hormone, palliative care, or other treatment (see Table 2). The Elixhauser comorbidity score was used to generate the VAN index, 2 which assigned a weight to each comorbidity based on the significance of its impact on general health (see Table 2). Baseline comorbidities as measured by both the Elixhauser comorbidity score and the VAN index differed significantly between insurance cohorts (P < .001). Overall survival rate and length of survival (months) differed significantly between insurance cohorts (P < .001) (see Table 2; Figure 1). Those patients with private insurance had higher 1-, 3-, and 5-year survival rates compared with other insurance types (see Table 3). A log-rank test also indicated that the survival curves significantly differed by insurance type (P < .001) (see Figure 1).
Overall Sample Characteristics.
Insurance Cohort Characteristics.
Survival Rates Overall and Stratified by Insurance Type.

Log-rank Test Results by Insurance Type.
Univariable Cox proportional-hazards models revealed that 15 of the original 18 independent variables were associated with higher rates of death. Sex, race, and radiation variables did not have any significant association with the survival outcome of the patients in the univariable analysis and, consequently, were not included in multivariable modeling. A preliminary multivariable Cox proportional-hazards model incorporating these individually significant covariates was fit. Due to multicollinearity, a reduced multivariable Cox proportional-hazards model was fit, and results indicated that insurance status is significantly associated with the risk of death while adjusting for other covariates (see Figure 2). All insurance cohorts appeared to have a higher risk of death than those patients with private insurance, and this was significant for all insurance types except for military insurance (not insured: Hazard Ratio (HR) = 1.96, P = .008; military HR = 1.37, P = .118; Medicare HR = 1.26, P = .017; and Medicaid HR = 1.75, P < .001).
Multivariable Results for the Reduced Cox Proportional-hazards Regression Model.
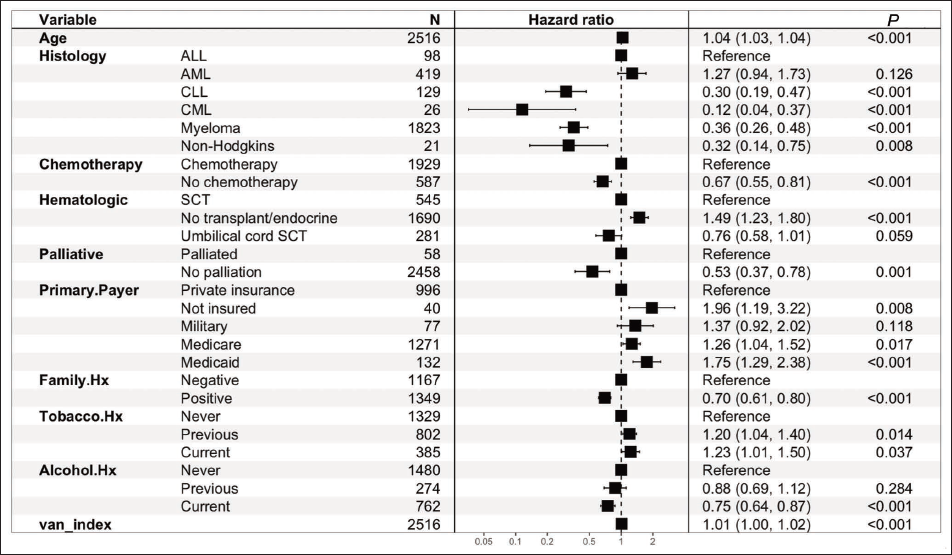
There was a lower risk of death in patients who did not receive chemotherapy (HR = 0.67, P < .001) or palliation (HR = 0.53, P = .001), those who had a positive family history of cancer (HR = 0.70, P < .001), and those who reported current alcohol use (HR = 0.75, P < .001). A lower risk of death was also seen in patients diagnosed with CLL (HR = 0.30, P < .001), CML (HR = 0.12, P < .001), myeloma (HR = 0.36, P < .001), and non-Hodgkin (HR = 0.32, P = .008) compared to patients diagnosed with ALL. Patients who reported previous/current tobacco use also had a higher risk of death compared to those who reported no tobacco use (see Figure 2).
Discussion
The purpose of this study was to assess the impact of health insurance coverage on the clinical outcomes of patients with hematologic malignancies in a rural state. Our study found a 5-year overall survival rate of 59.2%. When considering insurance status, the survival rate for our study was highest in privately insured patients, 72.5%, and fell with those with military insurance, no insurance, Medicaid, and Medicare, respectively. In addition, the risk of death was almost two times higher in uninsured and Medicaid patients compared to privately insured patients. The Surveillance, Epidemiology, and End Results Program has reported that the 5-year survival rate for patients with non-Hodgkin lymphoma, leukemia, and myeloma was 74.3%, 67%, and 61.1%, respectively, in the years 2014-2020.3-5 Our findings highlight the survival disparity between private and public health insurance for patients with hematological malignancies, especially so for those in rural states.6-9
A systematic review encompassing multiple studies revealed that 15%-59% of patients with hematologic malignancies experience financial burden, with constituent out-of-pocket expenses for medications, transportation, and appointment costs. 10 Patients with allogeneic hematopoietic cell transplantation were found to have faced substantial financial burdens, with some experiencing bankruptcy, selling their homes, or using their retirement savings. 11 These findings highlight the reality of the financial burden of hematologic malignancies and the impact on patients’ quality of life. It is critical not to underscore the need for policies that provide comprehensive insurance coverage, including support systems to help mitigate the financial burden.
In our state, with an estimated three million people, 38% of residents are low income, that is, make less than 200% the federal poverty level, and 27% of residents are covered by Medicaid. Our state does not currently enforce a work requirement for Medicaid. However, even though 53% of adults on Medicaid are working, the state is looking to enforce a work requirement.12-15 This could cause a significant number of people to lose health insurance coverage if their income surpasses the state’s income requirement, 138% of the federal poverty level, meaning more than $15,060 for an individual. Persons with income-underemployment have reported less functional health, which includes key lifestyle factors such as diet, exercise, and access to nutritious food, that help prevent chronic diseases such as cancer.16, 17 Additionally, our state is a Medicaid expansion state. Patients in expansion states have been shown to receive higher quality cancer care, and have been associated with improved survival rates. 18
Previous research demonstrates that disruptions in health insurance coverage have negative impacts on cancer patients. Disruption is associated with a later stage of diagnosis, treatment delay, and decreased likelihood of receiving treatment. 19 The importance of having insurance coverage cannot be overstated. The uninsured have been shown to have worse survival at earlier stages of treatment. One study that looked at the survival of patients with non-Hodgkin’s lymphoma found that uninsured patients with Stage I cancer had worse survival than privately insured patients with Stage II cancer. 20
The lower risk of death in patients who did not receive chemotherapy, palliative therapy, and had a positive family history can likely be explained by selection bias. These patients may have presented with earlier-stage, less aggressive disease, and/or higher baseline functional status. Additionally, a positive family history could have resulted in increased screening, again leading to earlier cancer detection, and thus did not require intensive treatment or palliative care.
Alcohol is a known carcinogen. Yet, in certain cancers, there have been studies showing a potential protective effect of alcohol use.21, 22 These studies found a reduced risk of non-Hodgkin lymphoma in those with light, moderate, and heavy alcohol consumption. The effect was strongest in those with diffuse large B-cell lymphoma and follicular lymphoma. It is also possible that the lower risk of death that we saw in those who reported alcohol use in our study was a result of non-response bias. Our study also showed that those who did not undergo stem cell transplantation (HCT) experienced higher mortality. It is possible that selection factors such as age, comorbidity burden, and access to specialized care prevented those patients from receiving transplantation.
The ethnic/racial health disparities in cancer care have been well-documented. In our state, 44% of non-elderly Medicaid recipients are persons of color. 12 Black patients are less likely than their White counterparts to receive a full diagnostic workup after presenting with multiple myeloma symptoms at their primary care office. 23 In fact, the average diagnostic delay in multiple myeloma is 6 months if presenting to primary care, or 3 months if presenting to hematology. Regarding treatment disparities, Black/African American patients, older age, and lower socioeconomic status patients are less likely to receive hematopoietic HCT, mostly due to lack of access. 24 Additionally, prolonged medical follow-up after HCT may not be possible in vulnerable populations that may end up with suboptimal benefits/insurance coverage after treatment. One study showed that factors such as non-White race, older age, uninsured, or Medicaid/Medicare insurance, and lower educational status were associated with decreased usage of HCT, despite a diagnosis of intermediate to high-risk AML. 25 HCT can cure hematologic malignancies, but patients must have adequate social and financial support, as it is highly intensive and the post-transplant period requires specialized care.
Limitations
The results of this study, which utilized the cancer registry, are limited by the retrospective study design and relatively small sample size (n = 2,516), as well as uneven distribution of insurance types among the data. This limits the statistical power of the study and introduces bias toward more common insurance groups. The survival data are also limited by the effectiveness of each treatment strategy and the patient’s response to treatment and compliance, resulting in either overestimation or underestimation of the true association between insurance status and survival. However, these limitations are unlikely to fully account for the magnitude of survival differences observed across insurance groups. Because this was a single-institution study conducted in a rural state, generalizability to urban populations or regions with differing Medicaid expansion status and access to specialty oncology services may be limited. Additionally, although we adjusted for insurance status, residual confounding may persist. Insurance status is often used to adjust for “access” but does not account for whether a patient can afford co-pays or find transportation to their appointments, which is certainly relevant to rural communities. Because of this, our results fail to paint the full picture due to the absence of these and other socioeconomic factors in our study.
There are multiple potential confounders in our dataset, and it is further challenged by the exclusion of other racial groups than Black and White, which was necessary due to a lack of statistical power. As with any retrospective cohort study, we use right-censoring in our survival estimates, which may distort our findings.
Conclusion
In this retrospective cohort study, survival outcomes in our rural state were heavily influenced by insurance status, with private insurance coverage showing more favorable outcomes. Our findings were consistent with prior evidence that suggests public insurance status is associated with poorer cancer outcomes. Ensuring Medicaid is available to those in need, preventing coverage disruptions, and addressing racial and socioeconomic barriers in cancer care may help narrow the gap in survival outcomes for patients with hematologic malignancies. Further research is needed to explore policy-driven solutions that enhance access to high-quality cancer care and improve survival across all patient populations.
Footnotes
Acknowledgments
None.
Authors’ Contributions
KN and HJ conceived the study idea. SL acquired regulatory approvals and data. SR and MMR performed the statistical analyses. All authors contributed to the manuscript.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the University of Arkansas for Medical Sciences Institutional Review Board. The requirement for informed consent was waived due to the use of de-identified registry data.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.