
Abstract
Background:
There is no consensus on the optimal endoscopic drainage strategy for hilar malignant biliary obstruction (HMBO).
Objectives:
To compare transpapillary plastic stent (PS) plus endoscopic nasobiliary drainage (ENBD) with PSs alone for HMBO, and to evaluate risk factors for cholangitis in the combined strategy group.
Design:
Retrospective cohort study.
Methods:
A total of 175 consecutive patients with HMBO (Bismuth type II–IV) who underwent either PS plus ENBD or PSs alone were enrolled. Propensity score matching (1:1) was performed to reduce selection bias. The primary endpoint was successful drainage. Univariate analysis was used to identify risk factors for cholangitis in the PS plus ENBD group.
Results:
After matching, 74 patients remained in each group, with balanced baseline characteristics. Successful drainage rates were 77.0% in the PS plus ENBD group and 68.9% in the PSs alone group (p = 0.267). The PSs alone group had significantly higher rates of cholangitis (23.0% vs 10.8%, p = 0.048) and overall adverse events (29.7% vs 12.2%, p = 0.009). No significant differences were observed in biliary patency, reintervention, or survival time between groups. In the PS plus ENBD group, initial drainage was associated with cholangitis (100.0% vs 59.3%, p = 0.011), and median drainage volume was lower in patients who developed cholangitis (85 mL vs 250 mL, p = 0.021). In 19 patients, the nasobiliary catheter was snipped to convert external to internal drainage.
Conclusion:
Endoscopic biliary stenting combined with ENBD followed by catheter snipping is a safe and effective approach for HMBO. The addition of ENBD was associated with reduced rates of cholangitis and overall adverse events. In this combined strategy, lack of initial drainage and low drainage volume were associated with cholangitis.
Keywords
Introduction
Hilar malignant biliary obstruction (HMBO) arises from various malignancies, which can result in obstructive jaundice. Effective alleviation of jaundice may improve the quality of life by ameliorating pruritus, poor appetite, and general weakness. 1 Despite the emergence of alternative approaches, including endoscopic ultrasound-guided biliary drainage (EUS-BD) and percutaneous transhepatic biliary drainage (PTBD), endoscopic retrograde cholangiopancreatography (ERCP) remains the preferred endoscopic drainage method.2,3 Bilateral or multi-sectoral drainage for ⩾50% of the total liver volume may be appropriate for satisfactory clinical effect in patients with advanced HMBO (Bismuth type II–IV). 1
Transpapillary drainage approaches include metal stent, plastic stent (PS) and endoscopic nasobiliary drainage (ENBD). The optimal drainage strategy for HMBO remains unclear. Self-expandable metal stents can be used to prolong stent patency and reduce the reintervention rate without increased complication rate. 4 However, one study of metal stents versus PSs for HMBO from unresectable gallbladder cancer showed no difference except for the high cost of metal stents. 5 Compared with the metal stent, utilization of PS may avoid PTBD and prolong the PTBD-free period in patients with HMBO. 6 Actually, the application of metal stents is limited due to the high technical difficulty and cost, especially in relatively small endoscopic centers. Alternatively, PSs are relatively cheap and can easily be exchanged if they malfunction. PSs are commonly used for biliary drainage, regardless of the severity or level of the HMBO may be. Except for a high rate of malfunction, undetermined drainage volume and recurrent early cholangitis possibly from duodenobiliary reflux, prompt us to seek other feasible drainage options.7,8
ENBD was reported to have a lower rate of cholangitis compared with endoscopic biliary stenting in hilar cholangiocarcinoma. 9 The Japanese Society of Hepato-Biliary-Pancreatic Surgery recommended ENBD as the most appropriate procedure for preoperative biliary drainage, based on reducing serum bilirubin levels in a shorter period. 10 However, nasopharyngeal discomfort after ENBD impedes its extensive use in countries outside Asia. The personality characteristics, social patterns, and health care environment may be the reasons for the widespread use of ENBD in East Asia. Nevertheless, ENBD is mainly used for temporary drainage as it can result in bile loss, and subsequent electrolyte imbalance and dyspepsia. The combination of biliary stenting and ENBD may be expected to avoid their respective defects.
Herein, we performed a retrospective study to compare the safety and efficacy of transpapillary PS plus ENBD and PSs alone in patients with HMBO, and further evaluated the risk factors on the outcome of cholangitis in the PS plus ENBD group.
Methods
Study design
We retrospectively screened 388 consecutive patients who underwent ERCP with PS plus ENBD or multiple PSs for HMBO between January 2021 and November 2023 at Nanjing Drum Tower Hospital. Malignancy was determined by pathological diagnosis, including brush cytology, ERCP-guided transpapillary forceps biopsy, digital single-operator cholangioscopy (DSOC)-guided biopsy, and endoscope with direct vision biopsy in infiltrating lesions. For the cytologic diagnosis, malignancy was confirmed for unequivocal carcinoma based on established cytologic criteria. The following exclusion criteria were applied: (a) younger than 18 years of age; (b) Bismuth type I HMBO; (c) unilateral drainage; (d) combined with EUS-BD or PTBD; (e) placement of metallic stent; (f) biliary fistula; (g) surgically altered anatomy. Written informed consent was obtained from all patients. The reporting of this study conformed to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement (Supplemental Material).
Procedures
ERCP was performed using a therapeutic duodenoscope (TJF-260, Olympus Optical Co. Ltd., Tokyo, Japan) by experienced endoscopists with the patient under sedation by using intravenous propofol and remifentanil. After successful bile duct cannulation, 0.035-inch guidewires (Boston Scientific, Natick, MA, USA) were advanced through the stricture to the desired ducts. In difficult cases, a 0.035-inch guidewire with a bent end (Terumo, Tokyo, Japan) was used. Endoscopic sphincterotomy was performed to facilitate stent and nasobiliary catheter (Willson-Cook, NC, USA) insertion. The stricture was dilated sequentially by Soehendra biliary dilation catheter (Willson-Cook, NC, USA) or balloon dilation catheter (Boston Scientific, Natick, MA, USA) at the discretion of the operators. PSs (Boston Scientific, Natick, MA, USA) were used with different types, sizes, and lengths as required, and all stents were placed across the papilla. The size of the PSs included 5F, 7F, 8.5F, and 10F. After PS insertion, ENBD was performed in the PS plus ENBD group. The selection of the bile duct branch for ENBD was at the operator’s discretion. In this group, one or multiple PSs were used combined with ENBD. The nasobiliary catheter might be snipped with scissor forceps (Jiuhong Medical Instrument Co. Ltd., Changzhou, China) when the post-procedural course showed no evidence of cholangitis and the external bile output was persistently high in another endoscopic procedure (Figure 1).
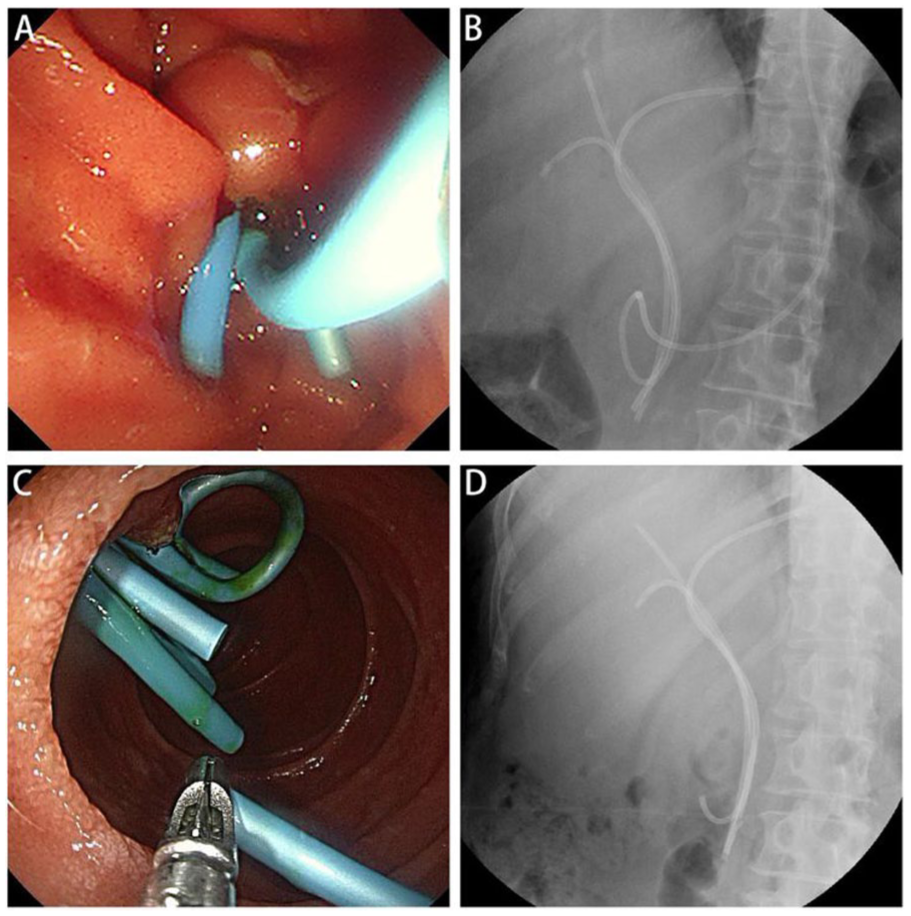
Endoscopic biliary stenting combined with ENBD for HMBO. (a) Endoscopic view of PSs and nasobiliary catheter. (b) Fluoroscopic view of PSs and nasobiliary catheter. (c), Endoscopic view of snipped nasobiliary catheter with scissor forceps. (d) Fluoroscopic view of PSs and snipped nasobiliary catheter.
Definitions
Successful drainage was defined as either (a) a decrease in total bilirubin level to less than 30% of the pretreatment value within 2 weeks or to less than 50% within 4 weeks or (b) no increase in the total bilirubin level over 1 mg/dL within 2 weeks if the pretreatment value was low (less than 1 mg/dL).11,12 Prophylactic intravenous antibiotics with cephalosporin or quinolone were given before, during, or after the procedure within 24 h. Bismuth types were determined according to ERCP and/or magnetic resonance cholangiopancreatography. The drainage area was divided into the left hepatic duct, the anterior branch of the right hepatic duct, and the posterior branch of the right hepatic duct. Right hepatic (anterior and posterior branches of the right hepatic duct), bilateral (left hepatic duct and the anterior branch or posterior branch of the right hepatic duct) or trisegmental (left hepatic duct, anterior branch, and posterior branch of the right hepatic duct) drainage were conducted according to the endoscopist’s discretion. Biliary patency was defined as the period between stent or nasobiliary catheter placement and the need for exchange due to dysfunction. Stent or nasobiliary catheter exchanges were performed in case of biliary occlusion, the occurrence of cholangitis, or periodic replacement. Biliary occlusion was defined as an increase in bilirubin from the plateau level after stent or nasobiliary catheter insertion. Data regarding patient death and periodic replacement of stent or nasobiliary catheter without obstruction were censored. The definitions of post-ERCP adverse events (AEs) were modified from those of Cotton et al. 13 and Freeman et al., 14 including pancreatitis, cholangitis, and hemorrhage. Pancreatitis was defined as new or worsened abdominal pain for longer than 24 h with elevation of serum amylase at least 3-fold the upper limit of normal. Cholangitis was considered with a new onset of fever more than 38℃ for at least 24 h without other causes outside the biliary tract. Hemorrhage was considered when hemostatic interventions were required, or blood transfusion was needed after the process of ERCP. Biliary patency was defined as the period between initial biliary stenting or ENBD and biliary obstruction diagnosed based on the biochemical evidence of cholestasis. 15 When stenting or ENBD was regularly performed without biliary obstruction, we estimated that biliary patency was maintained. Data regarding patient death without biliary obstruction were censored. Overall survival (OS) was measured from the day the procedure was performed for the HMBO to the date of death or loss to follow-up.
Outcome measures
The patients were assessed for basic demographics, malignancy types, laboratory data, including total bilirubin, international normalized ratio (INR), albumin, and white blood cell (WBC), Bismuth types of HMBO, and the application of DSOC and ERCP-guided radiofrequency ablation (RFA). The primary endpoint was successful drainage, whereas secondary endpoints included biliary patency, post-ERCP AEs, reintervention, and OS.
Statistical analysis
Statistical analysis of the data was performed using the software package SPSS 24.0 and R software, version 4.2.2 (SPSS Inc., Chicago, IL, USA), along with the MSTATA software (www.mstata.com). Propensity score matching was performed to identify matched cohorts to reduce selection bias in each case of the two study groups, with the use of 1:1 nearest neighbor-matching without replacement and a caliper width of 0.2. Age, sex, primary cancer, Bismuth type, prophylactic antibiotics, initial drainage, drainage area, DSOC, RFA, postoperative surgery, total bilirubin, INR, albumin, and WBC were selected as the observed covariates. The propensity score was estimated using a logistic regression model based on the set of covariates. After matching, clinical outcomes were compared between the two matched groups. Continuous variables in different groups were compared with Student’s t-test or Wilcoxon rank-sum test. Categorical variables were evaluated by chi-squared or Fisher’s exact test as appropriate. p value of <0.05 was considered significantly different.
Results
Patient characteristics
A total of 388 patients who underwent ERCP for HMBO were included. Under the screening, PS plus ENBD was performed in 101 patients, and PSs alone were performed in 74 patients. In the PS plus ENBD group, a nasobiliary catheter was inserted in the left hepatic duct (47/101, 46.5%), the anterior branch of the right hepatic duct (37/101, 36.6%), or the posterior branch of the right hepatic duct (17/101, 16.8%). Nasobiliary catheter with a diameter of 7F (94/101, 93.1%) or 5F (7/101, 6.9%) was used in the procedure. In the PS plus ENBD group, one PS was inserted in 80 patients (79.2%), two PSs were inserted in 20 patients (19.8%), and three PSs were inserted in 1 patient (1.0%). The maximum diameter of PSs was 5F in 1 patient (1.0%), 7F in 73 patients (72.3%), 8.5F in 26 patients (25.7%), and 10F in 1 patient (1.0%) in the PS plus ENBD group. And the minimum diameter of PSs was 5F in 2 patients (2.0%), 7F in 79 patients (78.2%), 8.5F in 19 patients (18.8%), and 10F in 1 patient (1.0%). In the PSs alone group, two PSs were inserted in 54 patients (73.0%), three PSs were inserted in 18 patients (24.3%), and four PSs were inserted in 2 patients (2.7%). The maximum diameter of PSs was 7F in 41 patients (55.4%), 8.5F in 32 patients (43.2%), and 10F in one patient (1.4%). The minimum diameter of PSs was 5F in seven patients (9.5%), 7F in 56 patients (75.7%), and 8.5F in 11 patients (14.9%).
After 1:1 propensity score matching, 74 patients each were selected from the PS plus ENBD and PSs alone groups (Figure 2). A comparison of the baseline characteristics of the two groups is shown in Table 1. There were no significant differences between the two groups in age, sex, Bismuth type, prophylactic antibiotics, initial drainage, drainage area, DSOC, RFA, WBC, total bilirubin, INR, and albumin. Significant differences in primary cancer and postoperative surgery were observed between the two groups. However, significant differences did not persist after propensity score matching, and the patient distribution was closely balanced between the groups.
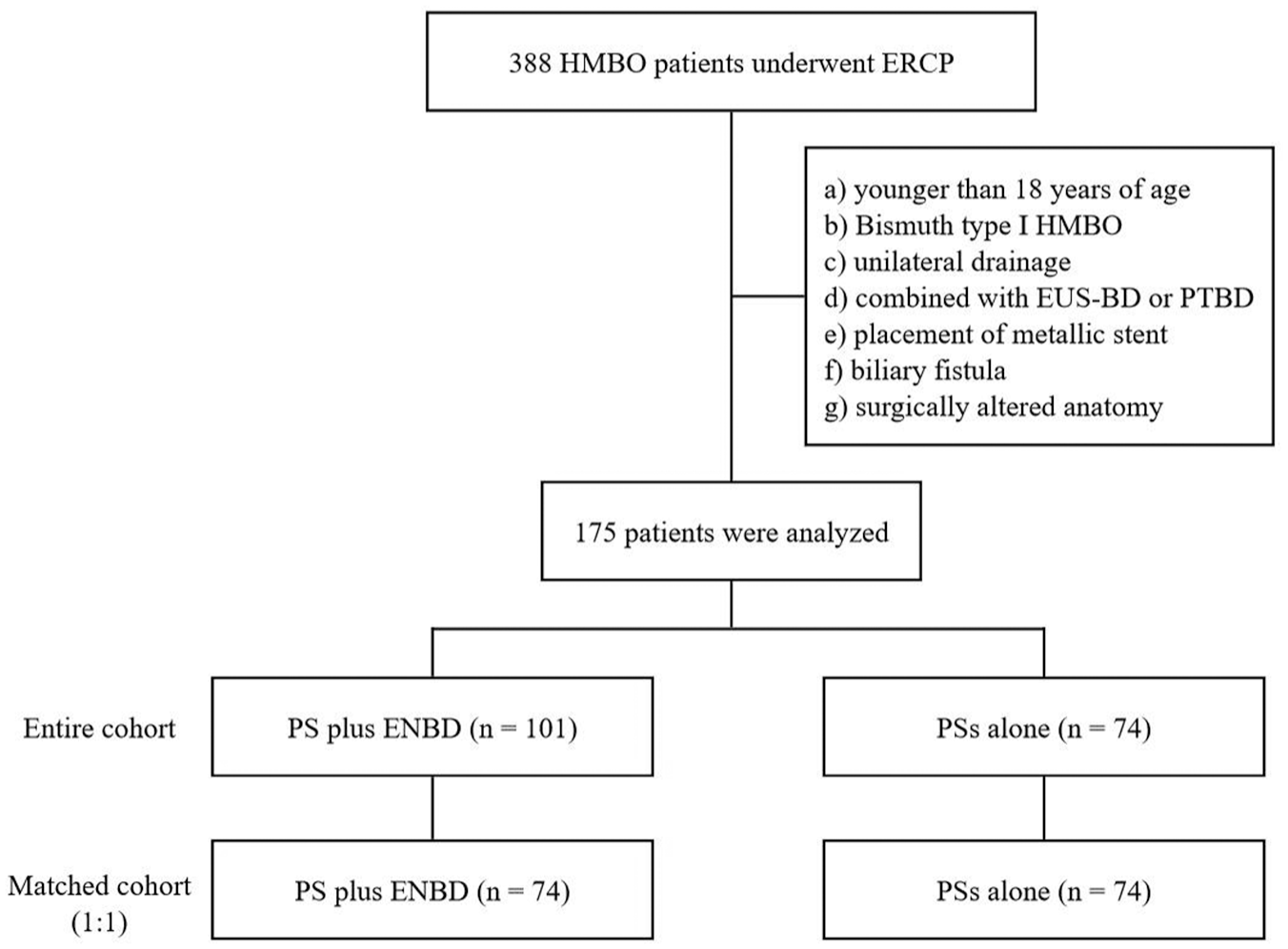
Study flow chart.
Baseline characteristics of the patients.
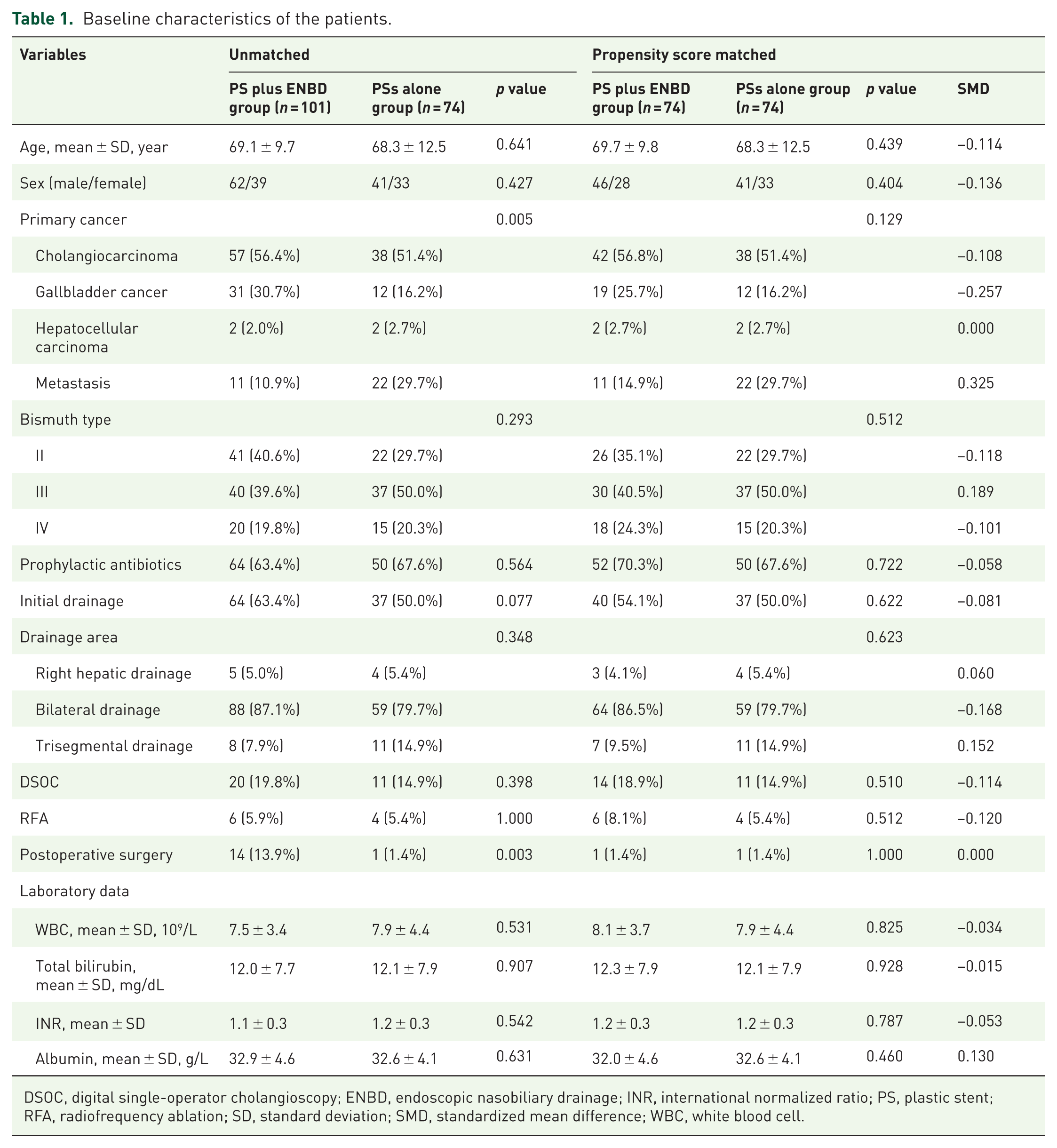
DSOC, digital single-operator cholangioscopy; ENBD, endoscopic nasobiliary drainage; INR, international normalized ratio; PS, plastic stent; RFA, radiofrequency ablation; SD, standard deviation; SMD, standardized mean difference; WBC, white blood cell.
Procedural outcomes
In the PS plus ENBD group, the maximum 24-h nasobiliary drainage volume within 1 week was 10–700 mL (median 250 mL). Displacement of nasobiliary catheter occurred in 10 patients (9.9%). An adjustment of the nasobiliary catheter was done in six patients (5.9%) due to an unsatisfactory drainage volume. We converted external drainage to internal drainage based on patient preference by snipping the nasobiliary drainage catheter with scissor forceps in 19 patients (18.8%). The nasobiliary catheters were snipped in the descending part of the duodenum (8/19, 42.1%), duodenal bulb (4/19, 21.1%), or the antrum of the stomach (7/19, 36.8%). The period between ERCP and catheter snipping was 2–21 days (median 5 days). Among the 19 patients, the maximum 24-h drainage volume within 1 week was 40–550 mL (median 250 mL). The survival time was 36–599 days (median 122 days).
Table 2 demonstrates the outcomes of both groups after propensity score matching. There were no significant differences between the two groups in successful drainage and reintervention. The approaches for reintervention included ERCP and PTBD. In the PS plus ENBD group, nine patients had procedure-related AEs, including cholangitis and pancreatitis. Additional ERCP was needed in three patients, and PTBD was needed in one patient with cholangitis; other patients with cholangitis or pancreatitis were managed conservatively. All patients with procedure-related AEs recovered after active clinical treatments in the PS plus ENBD group. In the PSs alone group, 22 patients had AEs, including cholangitis, pancreatitis, and hemorrhage. Additional ERCP was needed in five patients with cholangitis or hemorrhage, PTBD was needed in one patient with cholangitis, and other patients with cholangitis or pancreatitis were managed conservatively. Despite receiving active conservative treatments, two patients with cholangitis died 20 and 28 days after the procedure, respectively. Cholangitis was the most common AE in each group. Cholangitis (23.0% vs 10.8%, p = 0.048) and overall AEs (29.7% vs 12.2%, p = 0.009) rates were statistically higher in the PSs alone group than in the PS plus ENBD group. No statistical differences were found in the biliary patency (p = 0.318) and survival time (p = 0.083) between the two groups. At the time of retrospective assessment (July 10, 2024), all other patients had died except for one patient. Figure 3 exhibited the Kaplan-Meier curves for OS time in the two groups among HMBO individuals. The median survival time in the PS plus ENBD and PSs alone groups was 102 and 81 days, respectively (p = 0.078). There was no significant difference in the aspect of overall patient survival between the two groups.
Clinical outcomes of the patients.

AE, adverse event; ENBD, endoscopic nasobiliary drainage; PS, plastic stent; SD, standard deviation.
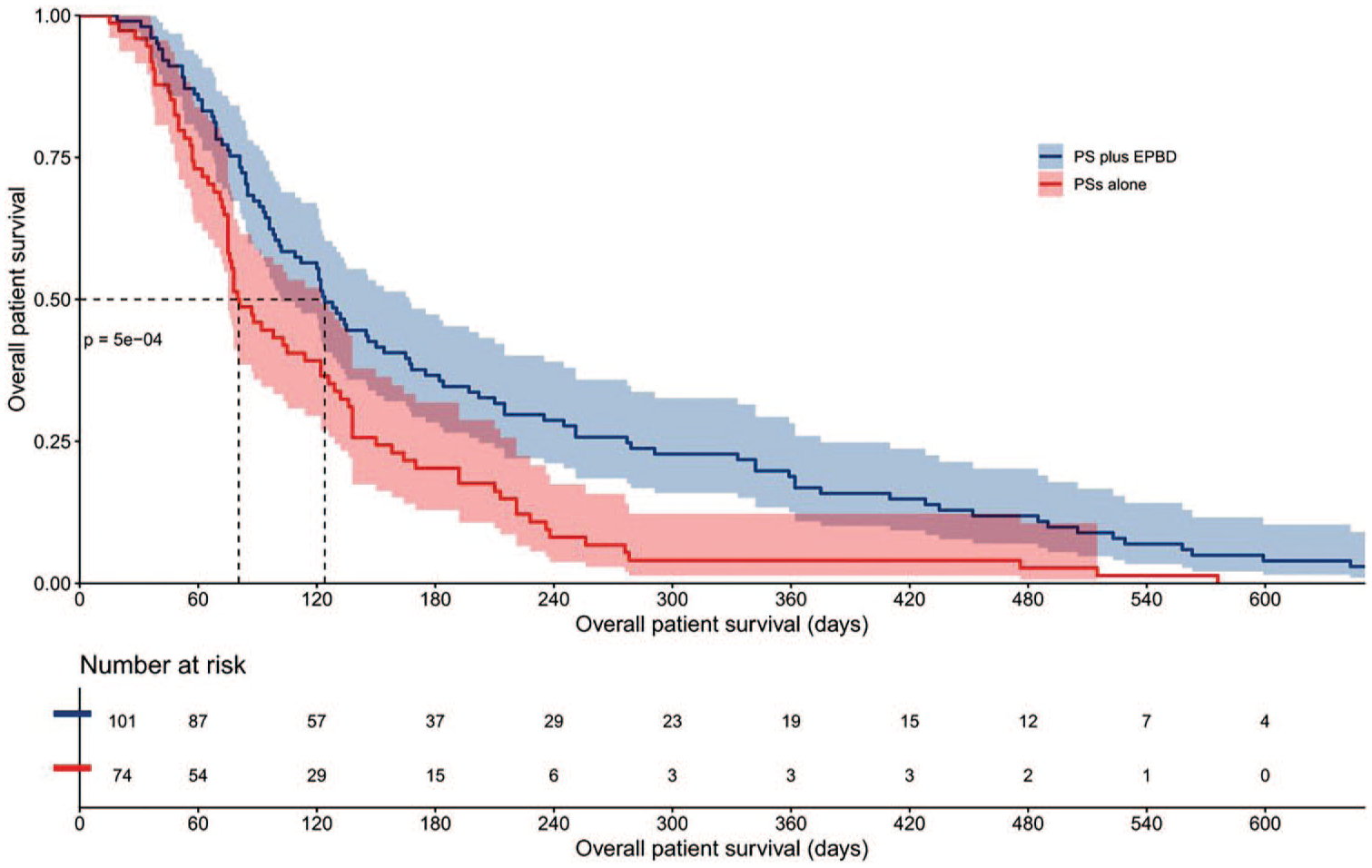
The Kaplan-Meier curves for the overall patient survival time in PS plus ENBD and PSs alone groups in patients with HMBO.
Risk factors for cholangitis in the PS plus ENBD group
Table 3 showed the assessment of predictive factors associated with cholangitis after endoscopic biliary stenting combined with ENBD for HMBO. Univariate analyses demonstrated that there was a significant relationship between the cholangitis and initial drainage. Initial drainage was more frequent among cholangitis patients (100.0% vs 59.3%, p = 0.011). A significant relationship was also identified between the cholangitis and the drainage volume of the nasobiliary catheter. The median drainage volume in the cholangitis and non-cholangitis groups was 85 and 250 mL, respectively (p = 0.021).
Univariate analysis of various factors for predicting cholangitis in 101 HMBO patients with PS plus ENBD.
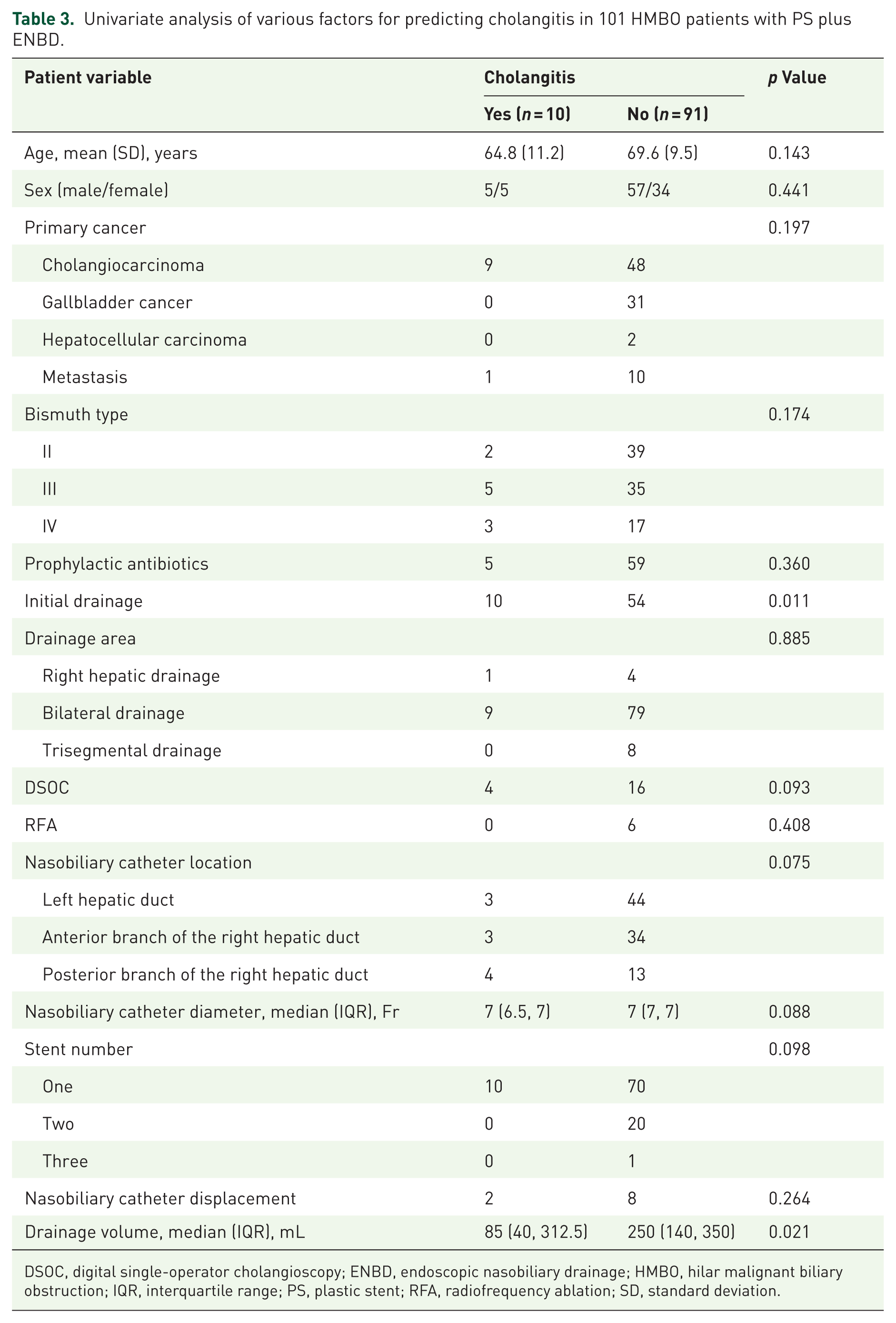
DSOC, digital single-operator cholangioscopy; ENBD, endoscopic nasobiliary drainage; HMBO, hilar malignant biliary obstruction; IQR, interquartile range; PS, plastic stent; RFA, radiofrequency ablation; SD, standard deviation.
Discussion
At present, the preferred drainage method for HMBO remains controversial in endoscopic biliary stenting and ENBD. Compared with ENBD, drainage tube occlusion with cholangitis was significantly more common in endoscopic biliary stenting. 16 Preoperative ENBD was rarely complicated with segmental cholangitis; placement of a nasobiliary catheter in the future remnant lobe was effective treatment for Bismuth type I–III HMBO. 17 In this retrospective study, the choice of the target bile duct for ENBD was at the operator’s discretion. Based on our clinical experience, the branch in the future remnant lobe was generally selected to achieve effective drainage and infection control. The latest guideline provided recommendations with ENBD as the most appropriate procedure for preoperative biliary drainage in patients with HMBO based on limited results. 10 In the setting of acute cholangitis because of occlusion of the previously placed stents, one-step simultaneous triple ENBD seemed to be the most suitable drainage technique for patients with advanced HMBO. 18 However, for preoperative biliary drainage of HMBO who underwent laparotomy for radical surgery, the proportion of cholangitis after endoscopic biliary drainage until surgery was similar when either ENBD or biliary stenting was used in a multicenter retrospective study. 19 In another multicenter retrospective study, ENBD as a means of preoperative biliary drainage for HMBO was comparable with endoscopic biliary stenting with PSs across the papilla or above the papilla in rates of dysfunction and AEs. 20 In our study, the majority of patients were unable to undergo surgical procedures, especially in the two groups of patients after propensity score matching, which might be the reason for the discrepancy between our results and those of previous studies. Therefore, our results supplemented the patients who required palliative treatment and were more in line with real-world situations. A key finding of this study is that the addition of ENBD to transpapillary plastic stenting significantly reduced the incidence of cholangitis and overall AEs, despite comparable results in stent patency and survival. Cholangitis is a critical clinical endpoint in HMBO, as it often leads to sepsis, prolonged hospitalization, and impaired quality of life. Therefore, the observed reduction in cholangitis represents a meaningful advantage of the combined strategy, even in the absence of superiority in stent patency. Inside PSs have been associated with longer patency periods compared with the transpapillary stents used in this study. However, they also pose challenges such as difficult removal when reintervention is required. On the other hand, ENBD was inappropriate to be used as a long-term drainage method in patients with unresectable HMBO due to the disadvantages of nasopharyngeal discomfort and the loss of bile. In our study, the nasobiliary catheter was used as a transitional drainage technique before the surgical procedure in resectable HMBO patients, while in unresectable patients, it could also be bridged to snip with scissor forceps. Meanwhile, we found that drainage volume from the nasobiliary catheter was associated with the occurrence of cholangitis. The advantages of ENBD are the ability to monitor bile quality and quantity and to perform cholangiography via the nasobiliary catheter whenever necessary. When the drainage volume was insufficient, nasal cholangiography could be performed to observe the position of the nasobiliary catheter, and adjustments could be made in a timely manner if necessary. Therefore, ENBD can be used as a trial method for stent placement in unresectable HMBO patients.
Due to the disadvantages of the ENBD mentioned above, it often serves as a transitional technique and cannot be retained in place indefinitely. We converted external drainage to internal drainage by snipping the nasobiliary catheter with endoscopically available scissor forceps. In an early study, the procedure was thought to be beneficial to patients undergoing ENBD. 21 The sequential drainage can serve as a potential approach for future preoperative and palliative treatment in HMBO. In our decision framework, a patient was considered suitable for nasobiliary catheter snipping when the post-procedural course showed no evidence of cholangitis and the external bile output was persistently high, which confirmed correct selection of the targeted bile duct branch. Under these clinical conditions, conversion from external to internal drainage by endoscopic snipping was considered unless the patient explicitly insisted on maintaining external drainage. However, the snipping timing and position of the nasobiliary catheter were determined at the discretion of the endoscopists, and there was currently no clear indication. It must be emphasized that the snipping subgroup was small, and no long-term follow-up data on biliary AEs are currently available. Therefore, while snipping appeared feasible and safe in this limited cohort, our findings should be considered preliminary. The procedure cannot be recommended for routine practice without further validation in larger, prospective studies with extended surveillance. Moreover, the decision framework described here represents a single-center, non-protocolized experience and should not be generalized without caution.
Limitations
This is the first study to investigate the efficacy and safety of endoscopic biliary stenting combined with ENBD for HMBO. Nevertheless, several limitations should be acknowledged. First, the retrospective nature of the study might introduce potential selection bias, which could limit the validity of the conclusions. Operators were more likely to choose ENBD in patients with surgical opportunities, although this bias was reduced after propensity score matching. We also note that factors such as tumor extent, anatomical complexity, effective liver volume, rate of dilation procedure, oncologic treatment, baseline infection status, and patient performance status were not accounted for in the matching process and could influence the results. In addition, closer monitoring in the PS plus ENBD group, including assessment of drainage volume, catheter adjustment, and snipping, may have facilitated earlier detection of acute cholangitis, introducing potential procedural bias. Second, due to the retrospective design, several key indicators were not evaluated, including the decrease in quality of life caused by ENBD, medical costs for nasobiliary catheter snipping, and digestive tract symptoms caused by the snipped catheter in the gastric antrum. Similarly, the number, diameter, and position of plastic stents might affect the results, but accurate evaluation was difficult. Third, in the univariate analysis, the small number of cases in the cholangitis group may also affect the credibility of the results. Therefore, more prospective, randomized controlled studies are needed to confirm our findings.
Conclusion
In summary, our preliminary findings from this limited retrospective subgroup suggest that endoscopic biliary stenting combined with ENBD and subsequent nasobiliary catheter snipping may be safe and effective for HMBO. The successful drainage, biliary patency, reintervention, and survival time for HMBO using PS combined with ENBD were comparable with those of PSs alone. Cholangitis rates were statistically higher in the PSs alone group than in the PS plus ENBD group. Furthermore, initial drainage and drainage volume were associated with cholangitis in the PS plus ENBD group. More prospective studies in large populations are needed for clinical practice guidance.
Supplemental Material
sj-docx-1-cmg-10.1177_26317745261457315 – Supplemental material for Endoscopic biliary stenting combined with nasobiliary drainage in hilar malignant biliary obstruction
Supplemental material, sj-docx-1-cmg-10.1177_26317745261457315 for Endoscopic biliary stenting combined with nasobiliary drainage in hilar malignant biliary obstruction by Yonghua Shen, Zongliang Wu, Xinyi Zhao, Taishun Li, Lei Xu, Nannan Zhang, Xiaojiao Zheng, Xiaoliang Zhou, Yanqing Zheng and Lei Wang in Therapeutic Advances in Gastrointestinal Endoscopy
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.