
Abstract
Background:
Self-expanding metal stents (SEMS) are recommended for the endoscopic palliation of distal malignant biliary obstruction (DMBO). Placement of SEMS during endoscopic retrograde cholangiopancreatography (ERCP) has been associated with an increased risk of post-ERCP pancreatitis (PEP).
Objectives:
The aim of this study is to evaluate rates of PEP in patients who underwent SEMS placement for pancreatic versus non-pancreatic malignancy.
Design:
Retrospective Cohort Study.
Methods:
Patients who underwent SEMS placement for DMBO between June 2017 and May 2021 were identified retrospectively from a procedural billing database. PEP incidence was compared between pancreatic and non-pancreatic DMBO groups and multivariate logistic regression was performed to identify risk factors for PEP.
Results:
A total of 488 individuals were identified, with 395 (80.9%) cases of DMBO due to pancreatic and 93 (19.1%) due to non-pancreatic malignancy. Stent types included 124 (25.4%) fully covered (FCSEMS) and 364 (74.6%) uncovered metal stents (UCSEMS). The overall rate of PEP in the cohort was 6.3% with no significant difference between pancreatic and non-pancreatic etiologies (6.1% vs 7.5%, p = 0.606). When adjusted for age <50 years old, female sex, and pancreatic stent placement, a non-pancreatic malignancy was not associated with an increased risk of PEP (OR 0.83, 95% CI 0.36–2.15).
Conclusion:
No statistically significant difference in PEP rates was seen after biliary sphincterotomy and SEMS placement for palliation of DMBO in patients with pancreatic versus non-pancreatic malignancies.
Keywords
Background
Endoscopic retrograde cholangiopancreatography (ERCP) remains a cornerstone in the management of patients with distal malignant biliary obstruction (DMBO). The primary goal of ERCP in DMBO is to relieve biliary obstruction, alleviate symptoms such as jaundice and pruritus, improve quality of life, and allow delivery of optimal oncologic therapy.
Self-expanding metal stents (SEMS) are recommended for the endoscopic palliation of DMBO. 1 SEMS offer several advantages over plastic stents, including a larger diameter that provides more durable patency and reduces the risk of stent occlusion, leading to fewer reinterventions and subsequent hospitalizations. ERCP is generally well tolerated but does carry risks related to post-ERCP pancreatitis (PEP), bleeding, infection, and perforation. PEP is the most common serious adverse event attributed to the procedure, resulting in annual estimated costs exceeding 150 million dollars in the United States.2,3
The placement of SEMS has been associated with a significantly increased risk of developing PEP.4,5 This appears to be less prominent in patients with malignant disease, leading some to suggest that some baseline, chronic impairment of pancreatic duct (PD) drainage may confer some protection. 6 Therefore, patients with pancreatic malignancy and chronic remodeling of the PD may theoretically be at lower risk for PEP, particularly when compared to patients with non-pancreatic malignancy who do not necessarily have intrinsic pancreatic disease. There is little data on the type of malignancy and PEP. 7 Therefore, the aim of this study is to evaluate the incidence of PEP in patients who underwent SEMS placement for pancreatic versus non-pancreatic malignancy.
Methods
Patient identification
A retrospective cohort study was performed at a single tertiary care center. Institutional review board approval was obtained prior to study initiation and deemed minimal risk with consent waiver (IRB #18-008429). Patients who underwent retrograde SEMS placement during ERCP between June 2017 and May 2021 were identified retrospectively from a procedural billing database. Inclusion criteria included an age ⩾18 years, SEMS placement for palliation of DMBO, and successful transpapillary placement of a SEMS in a retrograde fashion. Patients were excluded if they underwent SEMS placement for an indication other than palliation of DMBO, if SEMS placement was attempted and not successful, or if no follow-up data was available after ERCP (Figure 1). The cohort partially overlaps with previously reported data comparing clinical outcomes of UCSEMS to FCSEMS. 8 The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 9
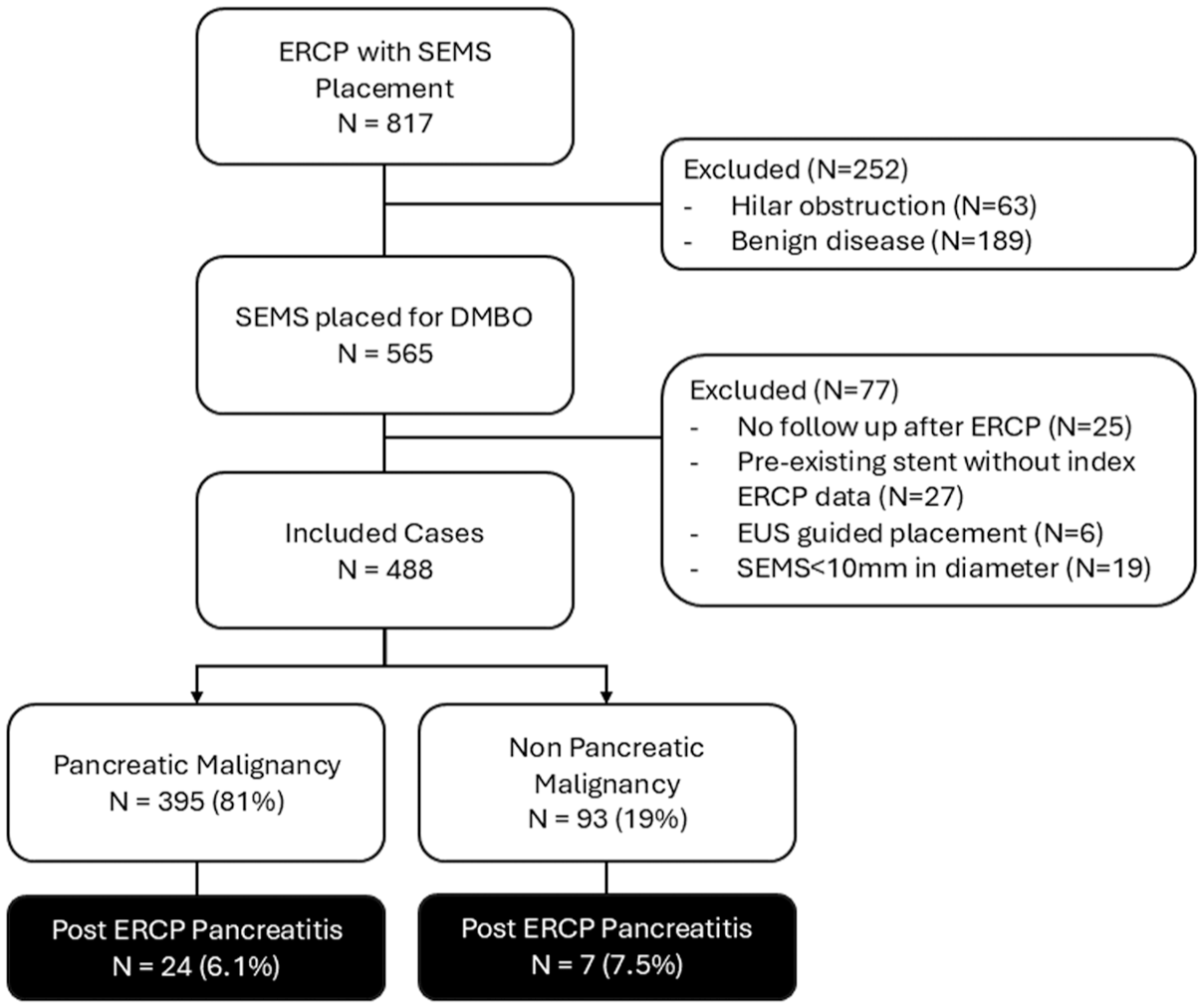
Study diagram including incidence of PEP stratified by etiology of malignancy.
Data collection
Electronic medical record review was performed to confirm the presence of distal malignant obstruction, determine the etiology of distal malignant obstruction, and document procedural details such as stent type, indication, technical success, and the development of adverse events post-procedure. All patients in this cohort underwent conventional ERCP under general anesthesia in a dedicated endoscopy unit. Endoscopic sphincterotomy was performed routinely and all stents were placed in a transpapillary fashion. All SEMS types were included in this cohort, including fully covered (FCSEMS) and uncovered (UCSEMS). FCSEMS utilized included WallFlex (Boston Scientific, Marlborough, MA, USA) and Viabil (Gore Medical, Newark, Delaware, USA) and UCSEMS included WallFlex (Boston Scientific, Marlborough, MA, USA) and Flexxus (ConMed, Largo, FL, USA). The decision to place a PD stent was at the discretion of the performing endoscopist, but it was generally utilized with repeated PD cannulations, extensive wire manipulation within the PD, or PD injection. Similarly, the decision to utilize rectal non-steroidal anti-inflammatory medication was adjudicated by the performing endoscopist but was routinely used barring strict contraindications.
Definitions
Etiology of malignancy obstruction was defined as pancreatic, representing a primary pancreatic malignancy, or non-pancreatic, representing any other primary malignancy. PEP was defined based on the Atlanta classification and required two of the following: abdominal pain typical of acute pancreatitis, serum lipase >3 times the upper normal value, and characteristic findings of acute pancreatitis on imaging. 10
Statistical analysis
The cohort was divided into two groups, pancreatic and non-pancreatic, based on the etiology of malignant obstruction. Continuous variables were reported as median with interquartile range (IQR) given the bounded nature and non-normal distribution, while categorical variables were summarized using counts and percentages. The incidence of PEP was compared utilizing Pearson Chi Square coefficient with significance defined as a p value less than or equal to 0.05. Multivariate logistic regression was then performed including clinical factors previously associated with increased risk for PEP including age <50 years old, female gender, placement of a prophylactic PD stent, and SEMS type. 11 A subgroup analysis was performed in a similar manner, comparing rates of PEP only in patients who underwent FCSEMS placement. Multivariate logistic regression in the subanalysis included age <50 years old, female gender, and placement of a prophylactic PD stent.
Results
A total of 488 patients were identified in the final cohort with a mean age of 68.5 years (IQR 60.0–75.0) with a BMI of 26.0 kg/m2 (IQR 22.8–29.8; Table 1). Females represented 42% of the cohort. Most patients underwent placement of an UCSEMS (364, 74.6%) which included 218 Flexxus stents and 146 WallFlex stents. FCSEMS were placed in 124 patients (25.4%) and included 90 WallFlex stents and 34 VIABIL stents. Median stent length was 6 cm (IQR 4–6 cm). Prophylactic PD stents were placed in 18 (3.7%) cases. The overall rate of PEP in the cohort was 6.8%.
Overall cohort information.
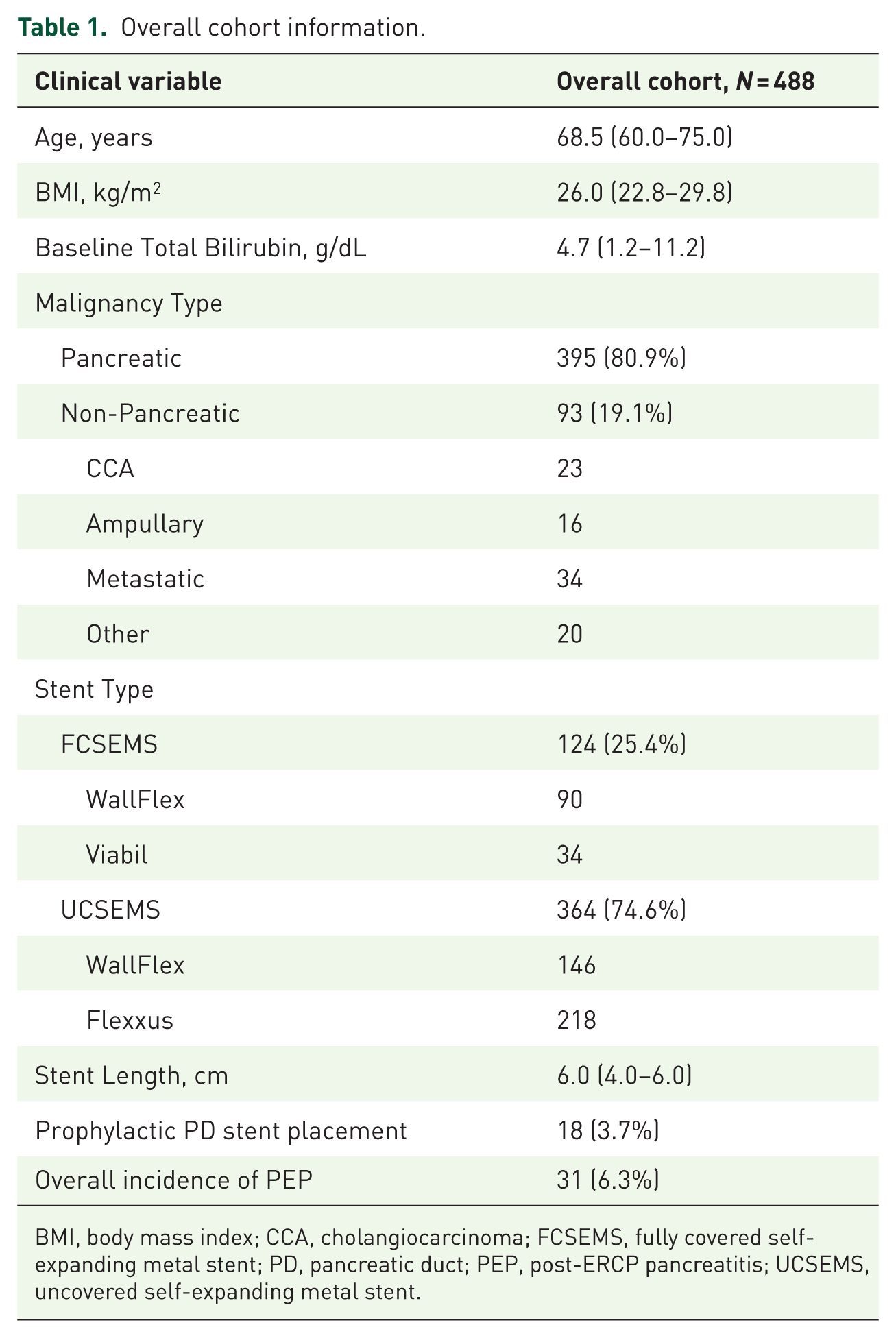
BMI, body mass index; CCA, cholangiocarcinoma; FCSEMS, fully covered self-expanding metal stent; PD, pancreatic duct; PEP, post-ERCP pancreatitis; UCSEMS, uncovered self-expanding metal stent.
Three hundred ninety-five (80.9%) cases of DMBO were due to a primary pancreatic malignancy and 93 (19.1%) cases were due to non-pancreatic malignancy. Etiologies of non-pancreatic malignancy included 23 cases of cholangiocarcinoma, 16 ampullary adenocarcinoma, 39 metastatic non-pancreatic malignancy, 7 duodenal carcinomas (not obviously ampullary), 1 gallbladder adenocarcinoma, 4 lymphoma, and 3 intraductal papillary mucinous neoplasms of the bile duct. The rate of PEP was non significantly different between the groups with 6.1% of patients with pancreatic malignancy developing PEP compared to 7.5% in the non-pancreatic group (p = 0.606; Figure 1). After adjusting for age <50 years old, female gender, stent type, and placement of a prophylactic PD stent, a non-pancreatic etiology of obstruction was not significantly associated with the development of PEP (OR 0.84, 95% CI 0.35-2.25; Table 2).
Multivariate logistic regression evaluating risk of developing post-ERCP pancreatitis.
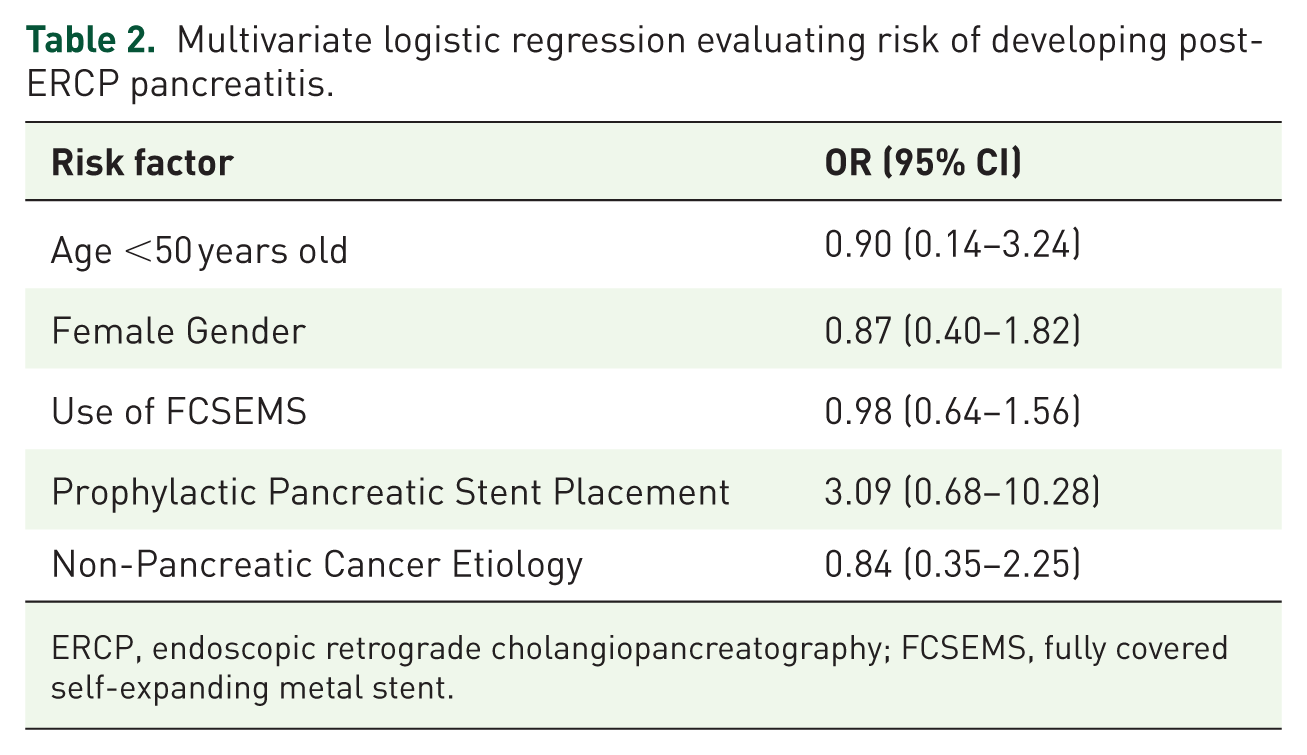
ERCP, endoscopic retrograde cholangiopancreatography; FCSEMS, fully covered self-expanding metal stent.
Subgroup analysis restricted to the 124 patients who received FCSEMS similarly showed no significant difference in PEP between groups (7.5% pancreatic vs 4.5% non-pancreatic malignancy, p = 0.41). On multivariate logistic regression including age <50 years old, female gender, and placement of a prophylactic PD stent, etiology of DMBO was not associated with increased risk of PEP (OR 3.4, 95% CI 0.54–66.7)
Discussion
This study suggests that patients undergoing SEMS for DMBO represent a low to average risk cohort for PEP with an overall incidence of 6.8%. 12 Etiology of malignancy does not seem to impact this risk without significant differences between pancreatic and non-pancreatic malignancy on univariate and multivariate analysis.
Data over several decades has suggested an increased risk of PEP with the use of SEMS including a cohort of 544 patients from 2010 which found a marked increase in the rate of PEP with placement of SEMS (OR 5.7 compared to plastic stent placement) and a more recent cohort of 358 patients (OR 2.3 compared to no SEMS placement), being attributed to a compression effect impairing PD drainage.4,5 Notably, the risk seems to be markedly higher in patients with benign disease and does not necessarily translate to those with malignant obstruction. 6 This has led to the general hypothesis that patients with malignant disease have some degree of underlying, chronic impairment of PD drainage, which is protective against PEP, supported by the observation that many patients with malignant biliary obstruction display some degree of PD dilation at baseline. 13 A similar phenomenon is seen in patients with chronic pancreatitis, where atrophy and decreased enzyme activity are felt to drive some degree of protection against PEP. 11
Therefore, one might consider that patients with non-pancreatic malignancy may be more susceptible to PEP and the risk portended by SEMS placement. This is particularly relevant to this patient population where SEMS is almost universally recommended as the treatment of choice for palliating DMBO.1,14,15 The overall PEP rate in this cohort is on the lower end of what has been previously reported after SEMS placement, which ranges from 6.0 to 10.6%.4 –7 This highlights the importance of evidence-based practices to reduce the risk of PEP regardless of underlying disease, which includes performing sphincterotomy prior to the SEMS placement, appropriate use of intravenous fluids and rectal non-steroidal inflammatory drugs, and placement of a PD stent if the PD is inadvertently accessed. Biliary sphincterotomy prior to SEMS placement is not universally recommended but may decrease the risk of PEP after SEMS use. 16 Therefore, centers that do not routinely perform endoscopic sphincterotomy may note higher rates of PEP overall.
Non-pancreatic malignancy was not associated with a significantly increased risk of PEP in this study. Subtyping of pancreatic versus non-pancreatic malignancy is not consistently reported in existing literature, and available data on outcomes are mixed. One report describes a markedly increased risk of PEP in non-pancreatic cancer (OR 5.52), but this has not been reliably demonstrated in other large cohorts that evaluate the etiology of malignancy, such as the work by Cote et al. which found pancreatic cancer etiology was not significantly associated with the development of PEP.5,7
The use of FCSEMS did not impact the incidence of PEP in this cohort, and indeed several others have highlighted no difference in PEP rates regardless of whether FCSEMS or UCSEMS are utilized.5,6,8 However, the majority of stents utilized in this cohort were UCSEMS, which are theoretically less likely to obstruct the pancreatic orifice due to their open meshwork. While no difference in PEP rates was seen in the FCSEMS subanalysis, the favored use of UCSEMS may have attenuated any differences in PEP rates driven by stent-related factors.
Limitations
The limitations of this study are largely driven by the retrospective study design, where not all variables that may impact the development of PEP are captured, such as cannulation difficulty, PD injection, guidewire passage, and failed cannulation rates. Low event rates also reduce the ability to detect clinically significant differences in PEP incidence. Importantly, key structural characteristics such as the presence of PD dilation or parenchymal atrophy are not captued by ERCP. Therefore, we are unable to comment on mechanistic factors which may have contributed to variable PEP rates, particularly given the heterogeneity of the non-pancreatic malignancy group. Heterogeneity is somewhat reduced given all procedures were performed at the same institution with similar practice across endoscopists; however, given all procedures were performed by experienced endoscopists at a single center, this may reduce generalizability. We attempted to further evaluate for potential confounding with the use of multivariate analysis incorporating known risk factors, which supported the findings of univariate analysis.
The classification of malignancy as pancreatic and non-pancreatic is likely oversimplistic, with non-pancreatic malignancy encompassing a spectrum of disease. It is not uncommon in clinical practice to have difficultly determining whether obstruction is related to a pancreatic or non-pancreatic malignancy, such as a distal cholangiocarcinoma or small pancreatic head adenocarcinoma. In this retrospective study, a combination of pathology, imaging findings, and management strategy selected by a multidisciplinary cancer center was utilized, which performing endoscopists may not have access to at the time of ERCP. Lastly, multiple stent designs are included, and it should be noted that stent designs have variable radial and axial forces, which may impact the risk of pancreatitis. 17
Conclusion
Overall, the findings of this study support the use of SEMS regardless of the etiology of malignant obstruction, consistent with guidelines from multiple societies. Endoscopists should follow best practices to reduce the risk of PEP, which remains the most common serious adverse event after ERCP; however, there does not appear to be an inherent risk of PEP secondary to SEMS placement in patients with non-pancreatic malignancy.
Supplemental Material
sj-docx-1-cmg-10.1177_26317745261458987 – Supplemental material for Post-ERCP pancreatitis after self-expanding metal stent placement in patients with pancreatic versus non-pancreatic malignant biliary obstruction
Supplemental material, sj-docx-1-cmg-10.1177_26317745261458987 for Post-ERCP pancreatitis after self-expanding metal stent placement in patients with pancreatic versus non-pancreatic malignant biliary obstruction by Jad AbiMansour, Bret T. Petersen, Eric J. Vargas Valls, Ryan Law, Samuel Han and Vinay Chandrasekhara in Therapeutic Advances in Gastrointestinal Endoscopy
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.