
Abstract
Background:
Colon capsule endoscopy (CCE) is a minimally invasive alternative to colonoscopy, but its diagnostic performance depends entirely on adequate mucosal cleansing (adequate cleansing rate, ACR) and complete colonic transit (completion rate, CR). These requirements impose stringent preparation demands. Existing systematic reviews (SRs) show substantial heterogeneity in recommendations.
Objectives:
To identify optimal CCE preparation strategies.
Design:
Umbrella review (overview of SRs).
Methods:
A comprehensive literature search was conducted through November 2025 for SRs and meta-analyses (MAs) assessing CCE bowel preparation regimens. Methodological quality was assessed using AMSTAR2, and primary study overlap was quantified using the Corrected Covered Area (CCA). Outcomes included ACR and CR, stratified by preparation components.
Results:
Fourteen SRs (11 MAs) encompassing 102 primary studies (moderate overlap, CCA 8.59%) were included. Pooled ACR (72.5%–76.8%) and CR (79.8%–83.0%) remained below colonoscopy benchmarks. In inflammatory bowel disease, ACR varied widely (49%–98.5%) with no superior regimen. In the general population, low-volume polyethylene glycol (PEG <4 L) yielded higher ACR (77.5%) than high-volume PEG (72.9%). Sodium phosphate (NaP) boosters outperformed PEG specifically for CR, with NaP + Gastrografin achieving the highest CR (93.1%). Castor oil improved excretion (OR 0.17 of incomplete CCE transit, 95% CI 0.09–0.32), and routine prokinetics improved CR compared with no use (OR 1.86, 95% CI 1.13–3.05). Low-fiber diets provided better cleansing than clear liquids (ACR 78.5% vs 70.0%).
Conclusion:
Current CCE bowel preparation regimens demonstrate variable performance relative to targets, with no single intervention demonstrating unequivocal superiority over others in pairwise comparisons. Evidence supports optimizing performance via low-volume PEG, NaP or Gastrografin-based boosters, routine prokinetics, and a low-fiber diet. A universal regimen is unlikely to suit all patients, highlighting the need for personalized protocols. Standardized cleansing scores and AI-assisted assessment are critical to improving reproducibility and cost-effectiveness.
Plain language summary
Colon capsule endoscopy is a non-invasive procedure that uses a swallowable pill-shaped camera to examine the large intestine to detect conditions like cancer or inflammation. While it offers a comfortable alternative to traditional colonoscopy, its success depends entirely on the colon being perfectly clean. Unlike standard endoscopes, the capsule cannot wash away debris or suction organic fluids. If the bowel is not completely clean, the examination may miss relevant lesion. Currently, there is no universally accepted standard for the best preparation protocol. To address this issue, we analyzed 14 major systematic reviews, encompassing data from 102 primary studies, to identify the most effective strategies for bowel preparation. The findings of this study highlight several key improvements for current protocols. First, a strict clear-liquid diet is not mandatory; allowing patients to eat low-fiber foods the day before the procedure actually improves cleansing results while enhancing patient comfort. Second, patients do not need to consume very high volumes of laxatives. Lower-volume solutions (under 4 liters) proved to be highly effective and are generally better tolerated by patients. Finally, keeping the capsule moving is critical, in order to avoid early battery depletion before the device is excreted. The routine use of specific medications that stimulate bowel movement (prokinetics), alongside targeted booster agents, is essential to ensure the capsule travels through the entire colon. In conclusion, the optimization and tailoring of laxative preparations significantly reduces the rate of incomplete examinations. This minimizes the need for repeat procedures, ultimately making colon capsule endoscopy a more reliable and cost-effective diagnostic tool.
Introduction
Direct visualization of the colonic mucosa underpins diagnosing and managing lower gastrointestinal disorders. Although conventional colonoscopy remains the reference standard for colonic assessment and intervention, its invasiveness, need for sedation, and substantial logistical burden can limit its accessibility and patient acceptance, particularly in the screening population and in those with low-risk symptomatology. 1 Colon capsule endoscopy (CCE), introduced nearly two decades ago, offers a validated, non-invasive alternative. The European Society of Gastrointestinal Endoscopy (ESGE) recommends CCE as a triage option following incomplete colonoscopy and as an alternative for patients unwilling or unable to undergo invasive procedures.2,3 CCE is being evaluated as a potential tool in colorectal cancer (CRC) screening pathways 4 and its role in inflammatory bowel disease (IBD) monitoring is expanding.5,6
However, the clinical utility of CCE is entirely dependent on bowel preparation quality. Unlike colonoscopy, CCE is a passive modality with no insufflation, suction, or washing capabilities; mucosal visualization, therefore, relies exclusively on the pre- and intra-procedural regimen to achieve both adequate cleansing rates (ACR) and complete colonic transit within the battery life (completion rate, CR). Suboptimal preparation frequently results in incomplete examinations that eventually necessitate salvage colonoscopy, undermining both the non-invasive advantage and the cost-effectiveness of the capsule pathway.7,8
Despite numerous trials, no universally accepted or standardized bowel preparation regimen for CCE has been established. Evidence remains inconsistent and often conflicting regarding the relative performance of high- versus low-volume laxatives, the value of dietary restrictions, and the safety and efficacy of booster agents. Although several systematic reviews (SRs) and meta-analyses (MAs) have addressed these components individually, a unified synthesis is lacking. This umbrella review systematically appraises and synthesizes evidence from existing SRs and MAs to identify preparation strategies associated with optimal CCE performance.
Methods
Protocol and registration
This umbrella review (overview of SRs) was conducted in accordance with the Preferred Reporting Items for Overviews of Reviews (PRIOR) guidelines (Supplemental Material S1). 9 The study protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO) (CRD420251229896), and no deviations from the registered protocol occurred.
Search strategy
A comprehensive literature search of PubMed/MEDLINE, Embase, Cochrane Library, and Scopus was conducted from January 2001 (coinciding with the introduction of capsule endoscopy) to November 2025. The search strategy combined Medical Subject Headings (MeSH) terms and free-text terms relating to “colon capsule endoscopy,” “bowel preparation,” “laxatives,” and “cleansing.” The full search strategy is provided in Supplemental Material S2. Reference lists of included studies were hand-searched to identify additional eligible records.
Inclusion and exclusion criteria
We included SRs and MAs evaluating bowel preparation regimens for CCE. The eligibility criteria followed the PICO framework (Supplemental Material S2):
- Population: adults undergoing CCE for any indication (e.g., CRC screening, symptoms, IBD).
- Intervention: any bowel preparation regimen (including different laxatives, volumes, booster agents, prokinetics, or dietary restrictions).
- Comparator: alternative preparation regimens or control groups, as defined by the included SRs.
- Outcomes: SRs reporting extractable quantitative data on ACR and/or CR according to each study’s operational definition.
We excluded: (1) narrative reviews, editorials, and conference abstracts; (2) primary studies (randomized controlled trials, cohort studies); (3) studies reporting data exclusively on small-bowel capsule endoscopy without separate data for the colon; (4) studies not reporting extractable data on the primary outcomes.
Data extraction
Two reviewers (P.C.V. and N.G.) independently screened titles and abstracts. Full texts of potentially relevant records were retrieved and assessed for eligibility. Disagreements were resolved by consensus or consultation with a third reviewer (A.K.). Data were extracted into a standardized template (spreadsheet) capturing study characteristics: review characteristics (first author, year of publication, type of review); number of included primary studies; total sample size; definitions and scoring systems used for ACR and CR; and pooled or reported estimates. When definitions of ACR or CR differed across reviews, these were documented to inform interpretation.
Outcomes
The primary outcomes were:
ACR: Defined as the proportion of CCE examinations rated as “adequate.” When established scoring systems were used, adequacy was defined according to each scale definition (i.e., CC-CLEAR: ⩾6/9 points overall and no segment under 2; Leighton-Rex: overall rating of “good” or “excellent” or at least 4/5 segments rated as adequate).10,11
CR: Defined as the proportion of CCE examinations in which the capsule reached the anal verge or was excreted within battery life.
Given that the included SRs often utilized varying operational definitions, we adopted the specific criteria reported by each review. Where multiple definitions were present, we prioritized the most conservative estimate to ensure the comparability of synthesized data.
Secondary outcomes included colonic transit time (CTT).
Quality assessment
Methodological quality of the included SRs was assessed independently by two reviewers using the AMSTAR 2 (A MeaSurement Tool to Assess Systematic Reviews) tool. 12 Reviews were categorized as high, moderate, low, or critically low confidence based on critical and non-critical deficiencies in the methodological reporting.
Assessment of overlap
To quantify duplication of primary studies across SRs, we calculated the degree of overlap using the Corrected Covered Area (CCA) method. A citation matrix cross-referenced all primary studies included in the selected reviews. CCA values were interpreted as slight (0%–5%), moderate (6%–10%), high (11%–15%), or very high (>15%) overlap. The CCA calculation serves to map the available literature (which encompasses multiple distinct interventions) and estimate the overall redundancy of the evidence base.
Data synthesis and analysis
Substantial heterogeneity in cleansing definitions, scoring thresholds, and regimen components precluded statistical re-pooling of primary studies. Therefore, a narrative synthesis of the results was conducted, prioritizing pooled estimates from existing MAs. Data were stratified and compared according to regimen components: diet (clear-liquid vs low-fiber), laxative volume (high vs low), booster type (sodium phosphate, NaP vs others), use of prokinetics, and specific patient populations (e.g., IBD). Although in routine clinical practice low-volume bowel preparation generally refers to 2 L polyethylene glycol (PEG)-based regimens, in this umbrella review “low-volume” was defined as <4 L in order to remain consistent with the operational definitions used in the included SRs and MAs. Data visualization, including the summary forest plot, was generated using R Statistical Software (v4.5.1; R Core Team 2025) and the ggplot2 package.
Results
Search results and study selection
The initial literature search yielded 255 records. After deduplication and preliminary screening of titles and abstracts, 17 full-text articles were assessed for eligibility. One additional record was retrieved via snowballing. Of these, four were excluded: two due to inappropriate study design (narrative reviews) and two for missing quantitative data on the primary outcomes (Supplemental Material S3). A total of 14 SRs met the inclusion criteria and were included in the final synthesis.5,7,13 –24 Eleven of these included an MA. The study selection process is summarized in Figure 1.

PRISMA flow chart.
Characteristics of included reviews and overlap
The included SRs, published between 2016 and 2025, encompassed 102 unique primary studies. The clinical indications were diverse and spanned from CRC screening to symptomatic evaluation and IBD monitoring. The detailed characteristics of the included studies are summarized in Table 1.
Characteristics of included systematic reviews and meta-analyses.
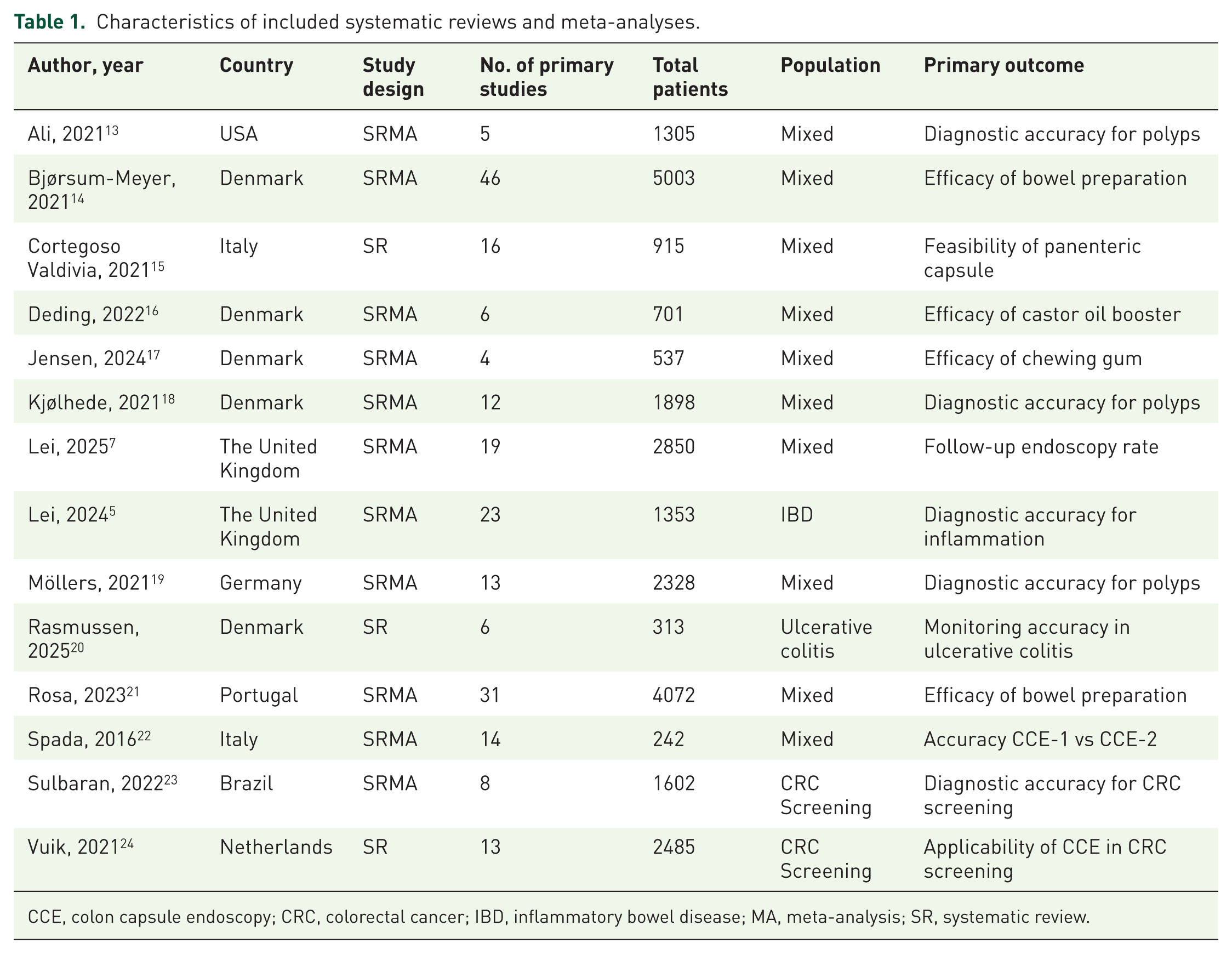
CCE, colon capsule endoscopy; CRC, colorectal cancer; IBD, inflammatory bowel disease; MA, meta-analysis; SR, systematic review.
The degree of overlap of primary studies across the 14 SRs was moderate (CCA 8.59%) (Supplemental Material S4 and Supplemental Figure S1). This suggests the presence of a shared evidence base, but also confirms that the reviews contributed complementary analyses rather than substantial duplication. As primary data were synthesized descriptively without statistical re-pooling, statistical weights were not influenced by overlapping studies.
Methodological quality assessed via AMSTAR 2 varied considerably. Only two SRs achieved a “high” methodological quality rating.16,17 Eight SRs were graded as “low”5,7,18 –23 and four as “critically low,”13 –15,24 largely due to reporting omissions in key domains (e.g., protocol registration, excluded study lists) rather than deficiencies in data synthesis (Supplemental Material S5).
Overall efficacy: Completion rate and adequate cleansing rate
Thirteen reviews reported CR and 14 reviews reported ACR. Across the major MAs, pooled CR ranged from 79.8% (95% confidence interval, CI 76.4%–82.8%) in the largest analysis by Bjørsum-Meyer et al. (n = 5003) to 83.0% (95% CI 78.7%–87.7%) in Rosa et al. (n = 4072).14,21 Similarly, the overall pooled ACR showed variability and remained below the recommended standards for conventional colonoscopy, ranging from 72.5% (Rosa et al.) to 76.8% (Bjørsum-Meyer et al.).14,21 In the specific context of IBD, Lei et al. reported notably wider ranges for both ACR (49%–98.5%) and CR (68%–100%) across primary studies, as the heterogeneity precluded meta-analytical pooling for these specific outcomes. 5 Pooled estimates and ranges from the four included SRs that provided comprehensive meta-analytical data for these endpoints are visually summarized in Figure 2.14,16,21,22 Moreover, as reflected in the overlapping confidence intervals (Figure 2), none of the evaluated single interventions demonstrated unequivocal statistical superiority over the others.
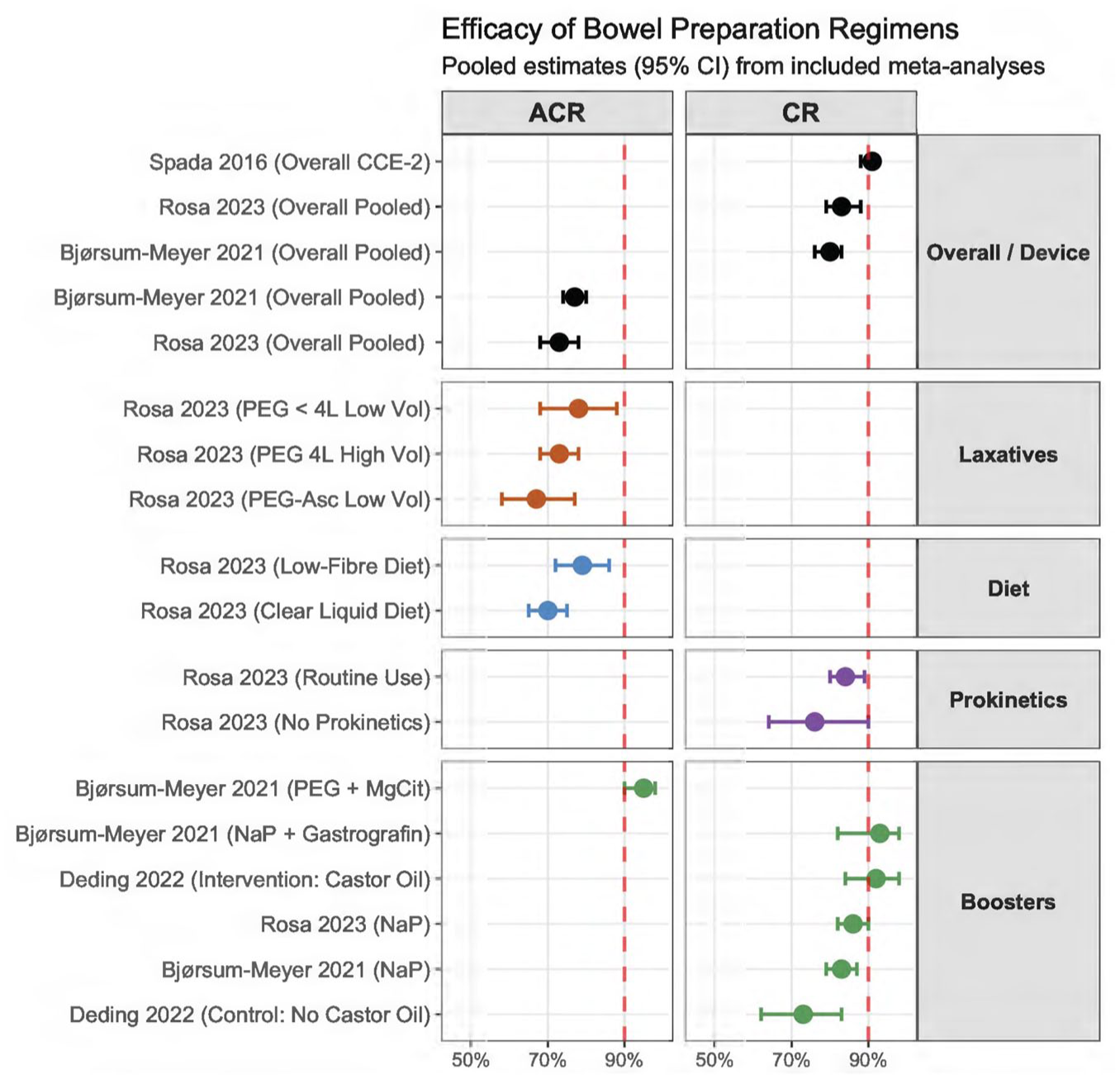
Summary forest plot of pooled estimates for ACR and CR, stratified by bowel preparation component.
Analysis of bowel preparation components
To evaluate preparation performance, data were stratified by regimen component. Key findings are summarized in Table 2.
Summary of findings stratified by bowel preparation component and impact on outcomes.
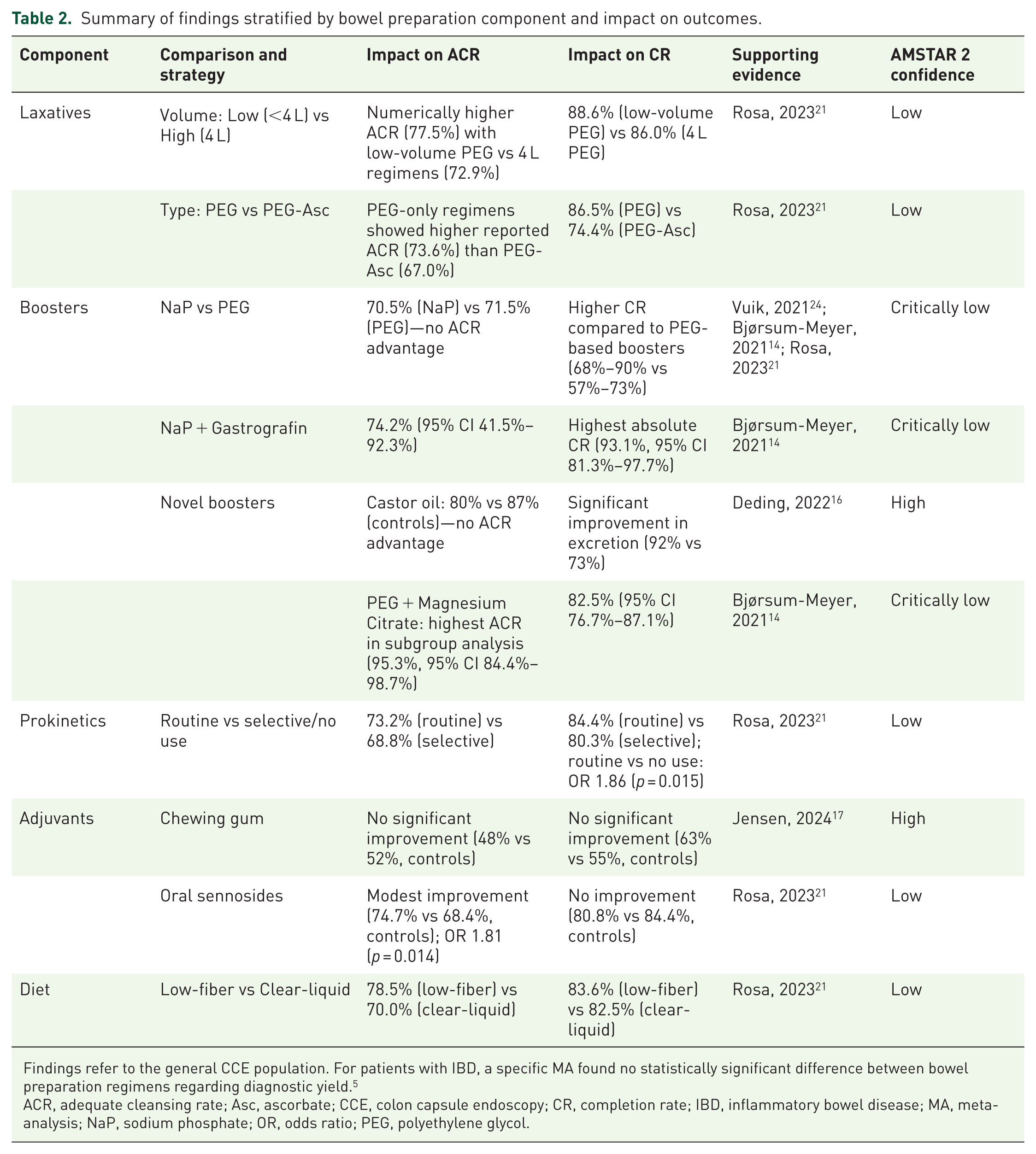
Findings refer to the general CCE population. For patients with IBD, a specific MA found no statistically significant difference between bowel preparation regimens regarding diagnostic yield. 5
ACR, adequate cleansing rate; Asc, ascorbate; CCE, colon capsule endoscopy; CR, completion rate; IBD, inflammatory bowel disease; MA, meta-analysis; NaP, sodium phosphate; OR, odds ratio; PEG, polyethylene glycol.
- Laxatives: PEG was most frequently used. Low-volume PEG (<4 L) was associated with higher ACR (77.5%) than high-volume PEG (72.9%), although the difference was not statistically significant. PEG-ascorbate regimens performed least well (ACR 67.0%). 21
- Booster agents: booster choice strongly influenced CR. Sodium phosphate (NaP) consistently outperformed PEG-based boosters, with CR ranging 68%–90% compared with 57%–73% for PEG. 24 The highest CR (93.1%) was observed with NaP + Gastrografin. 14 Castor oil increased CRs markedly (estimated prevalence proportions 92%, 95% CI 84%–98% vs 73%, 95% CI 62%–83%) compared to controls (odds ratio, OR 0.17 of incomplete CCE transit, 95% CI 0.09–0.32), although cleansing benefits were not statistically significant (ACR 80% vs 87%, p > 0.05). 16 PEG + magnesium citrate achieved the highest ACR (95.3%) in the subgroup analysis. 14
- Prokinetics and Adjuvants: routine prokinetic use improved CR (84.4%) compared with selective use (80.3%) and no use (75.7%), with routine administration showing a significant benefit over no use (OR 1.86, 95% CI 1.13–3.05, p = 0.015). 21 Chewing gum did not significantly affect outcomes. 17 Sennosides improved ACR modestly (74.7% vs 68.4%). 21 In IBD, no regimen component demonstrated superiority, underscoring challenges in standardizing preparation in inflamed bowel states. 5
- Dietary Recommendations: Data challenged the necessity of a strict clear-liquid diet. Rosa et al. found that a low-fiber diet on the day before the procedure was associated with higher ACR (78.5%) compared to a clear-liquid diet (70.0%), suggesting potential benefit despite the lack of statistical significance in the multivariate model (p = 0.324). 21
The administration timing across the included SRs generally followed standardized protocols. Laxatives were predominantly administered in a split-dose schedule, dividing the volume between the evening prior and the early morning of the procedure. This timing proved critical for efficacy, as split-dose PEG-only regimens were associated with a significantly higher CR compared to other schedules or formulations (OR 2.03, 95% CI 1.01–4.09, p = 0.048). 21 Booster administration was mostly event-dependent, with the first dose given upon CCE passage over the pylorus and a second dose typically administered 2–3 h later if excretion was not achieved.14,21,24 Finally, a rescue laxative was routinely employed 1–2 h after the second booster if the capsule remained in the colon.21,24
Colonic transit time
Data on transit times were reported in three studies, with significant heterogeneity observed. Bjørsum-Meyer et al. reported an overall mean CTT of 197.2 min (95% CI 166.7–227.9), noting that transit times were significantly influenced by the type of booster used (p < 0.05). Specifically, regimens including NaP or Gastrografin tended to result in faster transit compared to PEG-only boosters. 14 A previous MA from our group reported a wide range of mean CTTs across included studies (124–321 min), highlighting the variability introduced by different protocols. 15 Jensen et al. found no significant difference in CTT between patients using chewing gum and controls. 17
Impact on clinical outcomes
The clinical relevance of optimizing ACR and CR was substantiated by Lei et al.: in their meta-regression analysis, both CR and ACR were identified as significant inverse predictors of the follow-up endoscopy rate (FER) (p = 0.033 and p = 0.04, respectively). 7 This demonstrates that improvements in preparation quality may be associated with a reduction of unnecessary subsequent invasive procedures.
Discussion
This umbrella review synthesizes evidence from 14 SRs comprising 102 primary studies. Standard bowel preparation regimens for CCE, with pooled 72.5%–76.8% ACR and 79.8%–83.0% CR,14,21 consistently fall below performance thresholds established for colonoscopy: specifically, ESGE defines a minimum target of ⩾90% for both CR (defined as cecal intubation) and ACR in conventional procedures. 25 Although these benchmarks are designed for colonoscopy, they serve as critical aspirational targets for CCE, especially since CCE-specific performance indicators have not yet been formalized. While acknowledging the limitations related to the passive nature of the capsule, the rationale for aiming toward colonoscopy thresholds is to provide a realistic baseline for CCE to establish itself as a conclusive test in diagnostic pathways. Achieving high standards is essential to minimize FERs, particularly when CCE is used as a triage tool. On the other hand, real-world data frequently report even lower CRs for CCE, with substantial proportions of patients requiring salvage colonoscopy.26 –28 Closing this gap through optimization of bowel preparation is essential if CCE is to realize its diagnostic and operational potential. Nevertheless, a critical appraisal of our results highlights a lack of significant statistical superiority for any specific regimen, suggesting that conclusions drawn from single MAs should be interpreted with caution.
A counterintuitive finding of this review is that high-volume lavage, traditionally considered advantageous for colonoscopy, did not consistently translate into better CCE performance. Low-volume PEG regimens (<4 L) yielded numerically higher ACR than 4 L PEG regimens, 21 possibly because excessive intraluminal fluid without active propulsion leads to pooling and impaired visualization. Evidence also shows that very low-volume regimens can be effective when paired with potent boosters. 29 Additionally, reducing preparation volume may improve patient acceptability, a key determinant of adherence and broader implementation, 30 and lower the incidence of potential volume-related adverse events (fluid overload), which is crucial in a non-invasive procedure like CCE. Our findings also challenge the traditional reliance on clear-liquid diets the day before CCE, as a low-fiber diet was associated with numerically higher ACR than liquid-only restriction, suggesting that permitting a light meal may promote more effective physiological transit without compromising preparation quality. 21
Given the passive nature of CCE, our synthesis indicates that boosters and prokinetics are central determinants of procedural success. NaP-based boosters consistently outperformed PEG-based boosters in terms of CR, whereas ACR results were comparable between the two strategies. The highest performance was achieved through targeted combinations: PEG + magnesium citrate yielded the highest ACR (95.3%), while NaP + Gastrografin demonstrated the highest CR (93.1%).14,21,24 However, NaP is known to be associated with a risk of electrolyte disturbances and acute phosphate nephropathy, particularly in elderly patients or those with comorbidities such as chronic kidney disease or congestive heart failure.31,32 Given that CCE is frequently indicated for frail individuals or those who have experienced incomplete colonoscopies, the risk-benefit ratio of NaP must be strictly individualized. In this landscape, castor oil emerges as a valuable option for patients with contraindications to NaP or those with known slow colonic transit. While our analysis showed it did not significantly enhance ACR, castor oil demonstrated a marked benefit in promoting capsule excretion. 16 Routine administration of prokinetics improved CR relative to selective or no use, 21 underscoring the importance of active motility stimulation to ensure complete colonic transit within the device’s battery life. 33
Although regimen optimization is essential, a uniform approach may be inadequate. Patient-related predictors of poor preparation, including diabetes, smoking, psychotropic medication use, prior inadequate cleansing, chronic laxative use, and reduced mobility, suggest that tailored protocols may be required.34,35 Notably, the rising prevalence of patients on glucagon-like peptide-1 receptor agonists (GLP-1RAs) warrants particular attention due to their potential to significantly slow gastrointestinal motility, 36 resulting in inadequate bowel cleansing regardless of the presence of diabetes. 37 High-risk individuals may benefit from intensified or modified regimens, careful symptom assessment and multidisciplinary discussion, whereas average-risk patients could be managed effectively with lower-burden, better-tolerated protocols. The rationale for personalized preparation is reinforced by findings in IBD populations, where no regimen demonstrated superiority. 5 Inflammation likely confounds cleansing assessment, and modifying laxative type alone may not overcome impaired motility or altered luminal characteristics in active disease.
The implications of preparation quality extend to the economic viability of CCE. Both ACR and CR inversely predict the FER, meaning inadequate preparation drives downstream costs. 7 Modeling suggests that CCE is currently less cost-effective than fecal immunochemical test or colonoscopy primarily because incomplete examinations necessitate additional procedures. 8 Reducing the FER through optimized or personalized regimens may be essential to achieve cost-effectiveness and support broader implementation. 28
As an umbrella review synthesizing existing SRs rather than primary data, this study is inherently constrained by variability in definitions, reporting standards, and methodological quality across included reviews. First, substantial variability existed in the bowel cleansing scales used across primary studies, ranging from validated metrics like the Leighton-Rex scale and CC-CLEAR to various ad-hoc, unvalidated scoring systems. The lack of a universally accepted standard complicates direct comparisons and likely contributes to the observed heterogeneity in pooled ACR estimates, potentially obscuring the true comparative efficacy of specific cleansing protocols; this, combined with inconsistent definitions of adequacy, and suboptimal inter-observer agreement, as demonstrated in previous studies,38,39 precluded a re-meta-analysis of the primary data. Emerging approaches using artificial intelligence (AI) for automated cleansing assessment, including recent work demonstrating high reproducibility and standardization, 40 may help address this inconsistency in future research and should be incorporated into validation frameworks. Second, methodological quality across SRs was inconsistent, as only two SRs achieved a “high” AMSTAR 2 rating,16,17 while the majority were classified as “low” or “critically low,” although several downgrades were primarily due to reporting omissions rather than analytic flaws. However, the predominance of lower-confidence evidence, especially regarding core components like PEG volume and NaP boosters, affects the overall strength and reliability of the pooled conclusions. Third, definitions of completion varied, with some studies requiring excretion and others accepting visualization of the anal verge, thus affecting the comparability of CR across different studies. Fourth, safety data, particularly regarding NaP in older or comorbid populations, were inconsistently reported, limiting stratified assessment. Fifth, umbrella reviews rely on existing SRs and may omit newly published primary studies; hybrid designs may help address this in future work. Sixth, the included SRs had heterogeneous primary outcomes: some underlying primary studies were not specifically designed to evaluate preparation regimens as a primary endpoint, potentially affecting the robustness of the extracted data. Finally, although overlap was moderate, aggregation at the review level may obscure patient-level determinants of preparation performance.
Conclusion
Current bowel preparation strategies for CCE remain suboptimal. To improve diagnostic yield and cost-effectiveness, clinical practice should move toward optimized regimens incorporating low-volume, split-dose PEG, NaP- or Gastrografin-based boosters, routine prokinetics, and a low-fiber diet. Large-scale studies are needed to validate personalized preparation protocols tailored to patient risk profiles, emphasizing caution with NaP given the limited safety data. The integration of AI for objective cleansing assessment offers a potential mechanism to reduce variability and strengthen the reliability of CCE in clinical pathways, remaining a critical question for future research.
Supplemental Material
sj-docx-1-cmg-10.1177_26317745261463059 – Supplemental material for Optimizing bowel preparation regimens for colon capsule endoscopy: an umbrella review (overview of systematic reviews)
Supplemental material, sj-docx-1-cmg-10.1177_26317745261463059 for Optimizing bowel preparation regimens for colon capsule endoscopy: an umbrella review (overview of systematic reviews) by Pablo Cortegoso Valdivia, Noemi Gualandi, Giuliano Francesco Bonura, Mauro Manno, Marco Pennazio, Ervin Toth, Jean-François Rey, Reena Sidhu and Anastasios Koulaouzidis in Therapeutic Advances in Gastrointestinal Endoscopy
Supplemental Material
sj-docx-2-cmg-10.1177_26317745261463059 – Supplemental material for Optimizing bowel preparation regimens for colon capsule endoscopy: an umbrella review (overview of systematic reviews)
Supplemental material, sj-docx-2-cmg-10.1177_26317745261463059 for Optimizing bowel preparation regimens for colon capsule endoscopy: an umbrella review (overview of systematic reviews) by Pablo Cortegoso Valdivia, Noemi Gualandi, Giuliano Francesco Bonura, Mauro Manno, Marco Pennazio, Ervin Toth, Jean-François Rey, Reena Sidhu and Anastasios Koulaouzidis in Therapeutic Advances in Gastrointestinal Endoscopy
Supplemental Material
sj-docx-3-cmg-10.1177_26317745261463059 – Supplemental material for Optimizing bowel preparation regimens for colon capsule endoscopy: an umbrella review (overview of systematic reviews)
Supplemental material, sj-docx-3-cmg-10.1177_26317745261463059 for Optimizing bowel preparation regimens for colon capsule endoscopy: an umbrella review (overview of systematic reviews) by Pablo Cortegoso Valdivia, Noemi Gualandi, Giuliano Francesco Bonura, Mauro Manno, Marco Pennazio, Ervin Toth, Jean-François Rey, Reena Sidhu and Anastasios Koulaouzidis in Therapeutic Advances in Gastrointestinal Endoscopy
Supplemental Material
sj-docx-4-cmg-10.1177_26317745261463059 – Supplemental material for Optimizing bowel preparation regimens for colon capsule endoscopy: an umbrella review (overview of systematic reviews)
Supplemental material, sj-docx-4-cmg-10.1177_26317745261463059 for Optimizing bowel preparation regimens for colon capsule endoscopy: an umbrella review (overview of systematic reviews) by Pablo Cortegoso Valdivia, Noemi Gualandi, Giuliano Francesco Bonura, Mauro Manno, Marco Pennazio, Ervin Toth, Jean-François Rey, Reena Sidhu and Anastasios Koulaouzidis in Therapeutic Advances in Gastrointestinal Endoscopy
Supplemental Material
sj-tiff-1-cmg-10.1177_26317745261463059 – Supplemental material for Optimizing bowel preparation regimens for colon capsule endoscopy: an umbrella review (overview of systematic reviews)
Supplemental material, sj-tiff-1-cmg-10.1177_26317745261463059 for Optimizing bowel preparation regimens for colon capsule endoscopy: an umbrella review (overview of systematic reviews) by Pablo Cortegoso Valdivia, Noemi Gualandi, Giuliano Francesco Bonura, Mauro Manno, Marco Pennazio, Ervin Toth, Jean-François Rey, Reena Sidhu and Anastasios Koulaouzidis in Therapeutic Advances in Gastrointestinal Endoscopy
Supplemental Material
sj-tiff-2-cmg-10.1177_26317745261463059 – Supplemental material for Optimizing bowel preparation regimens for colon capsule endoscopy: an umbrella review (overview of systematic reviews)
Supplemental material, sj-tiff-2-cmg-10.1177_26317745261463059 for Optimizing bowel preparation regimens for colon capsule endoscopy: an umbrella review (overview of systematic reviews) by Pablo Cortegoso Valdivia, Noemi Gualandi, Giuliano Francesco Bonura, Mauro Manno, Marco Pennazio, Ervin Toth, Jean-François Rey, Reena Sidhu and Anastasios Koulaouzidis in Therapeutic Advances in Gastrointestinal Endoscopy
Footnotes
Acknowledgements
During the preparation of this work the authors used Google Gemini (Large Language Model) solely for language refinement and organizational support; all analyses, interpretations, and conclusions were generated and verified by the authors. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the published article.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.