
Abstract
Tribal communities remain under a constant threat of poor maternal health outcomes, including pregnancy and childbirth. Recognizing the considerable scope in enriching the existing knowledge, this qualitative study with an inductive approach was conducted among the Munda community in Odisha. The study adopted the Reflexive Thematic Analysis (RTA) approach in the data analysis process to interpret patterns and meanings within women’s own accounts of pregnancy and childbirth experience. The emerging themes highlight early and unplanned conception generally associated with neglected contraception practices and misconstrued perception of antenatal, childbirth and post-partum care. Furthermore, the study captures emotional distress and the influence of social support and the potential obstacles they face in experiencing healthy and positive maternity. The findings reveal that since pregnancy and childbirth include both subjective and collective factors, even an experience without medical complications can also be perceived as negative. Identifying traditional norms and socio-cultural context as indispensable, the study views that due attention to a multi-pronged approach holds relevance in enabling a healthy and desirable pregnancy and childbirth experience among women.
Keywords
Introduction
Pregnancy and childbirth, two crucial phases in women’s lives, have long been emphasized through extensive studies demonstrating diverse experiences relating to social contexts and cultural predispositions.1–8 As such, it is wrong to dictate a single model of gestation and delivery for all women whose experiences vary on the basis of their social setting. 9 For example, Norr et al. 10 explain birth preparation, including husband’s support, is more encouraged among women having higher status, close marital relations, and liberal sexual role attitudes in contrast to poor women with multiple socio-economic problems and limited life choices. 11
The present study conceptualizes pregnancy and childbirth in line with the World Health Organization’s 12 definition of positive pregnancy that prioritizes maintaining physical and socio-cultural health and normality with effective labor and birth as well as providing essential clinical interventions. Accordingly, comprehending biomedical aspects only, however, does not cover the entire gamut of understanding women’s lived experience of maternity. Rather, it is important to address the socio-cultural influence, availability, accessibility, and utilization of healthcare avenues for pregnancy and childbirth.4,9–13
Although pregnancy and childbirth have been identified as periods when women require physical and social health attention, certain sub-groups, such as tribal women, are less likely to confirm a healthy experience. A vast number of studies have raised concern over poor maternal health status of these women,14–17 such as unspaced pregnancies and negligible contraception practices,14,15 anemia and nutritional deficiency. Also, tribal communities have their own established traditional understanding of conception and birth1,5 and follow cultural practices of food choices and preferences.18,19
However, despite numerous existing literatures, exploring the lived experience of maternity among these women still remains inadequate, especially in terms of qualitative research. Also, though the state of Odisha has domination of diverse tribal communities, it has received less attention compared to other tribal regions like the Northeast of India. Thus, highlighting the significance of understanding maternal health within an underexplored group like the Munda community will address such a significant gap.
With this backdrop, the study aims to understand women’s emotional, social and healthcare experience relating to their pregnancy and childbirth. Also, to explore how the living socio-cultural contexts of women shape their maternal health practices. The study excludes clinical dimensions; instead, it focuses on how these tribal women navigate their maternity episodes in terms of awareness, access, emotional struggle, and overall socio-cultural barriers to attain a healthy pregnancy and childbirth experience.
Materials and Methods
Study Design
A qualitative phenomenological design was used as an appropriate approach to explore women’s shared lived pregnancy and childbirth experience. Methodological insights on qualitative health research were drawn from relevant literature.20–22 Ethical approval for this study was obtained from the Institutional Ethics Committee. Given that majority of the participants were illiterate, verbal informed consent was obtained from them after a clear explanation of the study purpose and confidentiality. Also, as several participants had married before the age of 18, the researchers maintained adherence in line with the legal and ethical aspects of the POCSO Act, 2012, of India throughout the research process.
Study Setting and Sample
The study was conducted among the Munda tribal community who have migrated and presently reside in small semi-urban areas across the Jajpur, Odisha. Their residential area is well-connected in terms of transport facilities, and the primary healthcare center is located within a short distance of one or two kilometers. As per the participants’ accounts, they belong to the neighboring tribal dominated district of Keonjhar but had migrated several years ago in search of livelihood. With the approval of the Chief District Medical Officer (CDMO), the participants were purposefully selected, ranging in pregnancy and recent post-partum experience. Inclusion criteria for selecting participants included women under age 30 (to ensure better recall of first pregnancy experience), having at least one childbirth, having delivered in the last 1 year and willing to participate. Exclusion criteria include women above age 30, not having childbirth experience, last delivery happened more than 1 year or unwilling to participate.
Data Collection
Data was collected between October and December 2024. Semi-structured interviews were conducted, and each interview continued for 40–55 minutes, involving note-taking, audio recording and observation. The interview was conducted at the participant’s place of living. Each interview began with understanding what they think of pregnancy and childbirth, and sharing their own experience of maternity episodes. Further questions were based on what the participants shared about their practices and the issues that needed more clarification for details. The interviewer tried to be sensitive to the language and concepts used by the participants, and therefore, the agenda was kept flexible. This helped in exploring many details about what women say. Using the data saturation principle, our data collection continued till the attainment of repetitive patterns in the 15th and 16th interview transcripts.
Data Analysis and Interpretation
The study has adopted Braun & Clarke’s six-step thematic analysis formula 23 and Reflexive Thematic Analysis (RTA) approach. While acknowledging the researcher’s position, RTA approach facilitates quality, meaningfulness, in-depth interpretation, and coherence of themes.24,25 Thus, this approach aligns with the study for its emphasis on in-depth analysis and interpretation of women’s maternity experience within their unique social and cultural context by taking into account the researcher’s reflexivity.
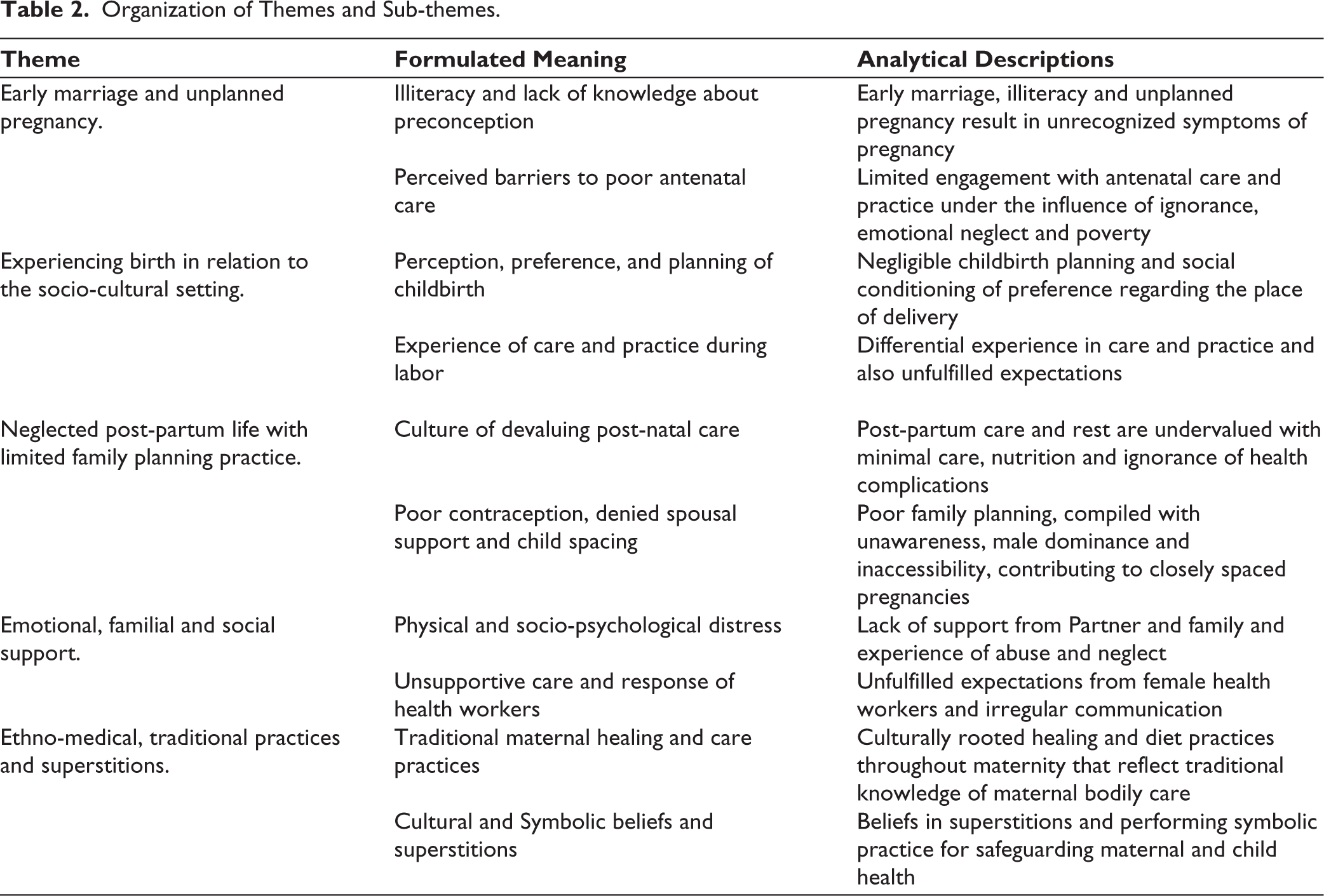
Themes were not pre-determined but gradually developed through manual open-ended coding following multiple readings of transcripts. Reflective formulated meanings were drawn for establishing familiarity and patterns after several reviews of the data items and codes supporting each theme and sub-theme. Data interpretation has primarily followed an experimental orientation, with some elements of critical interpretation to use both semantic and latent codes. As a result, the study has identified five themes to explain women’s experience to pregnancy and childbirth: (a) early marriage and unplanned pregnancy, (b) experiencing birth in relation to socio-cultural setting, (c) neglected post-partum life with limited family planning practice, (d) emotional, familial, and social support, and (e) ethno-medical, traditional practices and superstitions.
Utilizing Broun and Clarke’s reflective thematic analysis approach, trustworthiness was maintained throughout data collection, analysis and interpretation process following guidelines from significant literature.26–28 Bracketing as a process of setting aside researchers’ bias and being open to data was followed, 29 and reflexivity was also maintained by consciously acknowledging researchers’ position, gender identity, and prior experience.
Result
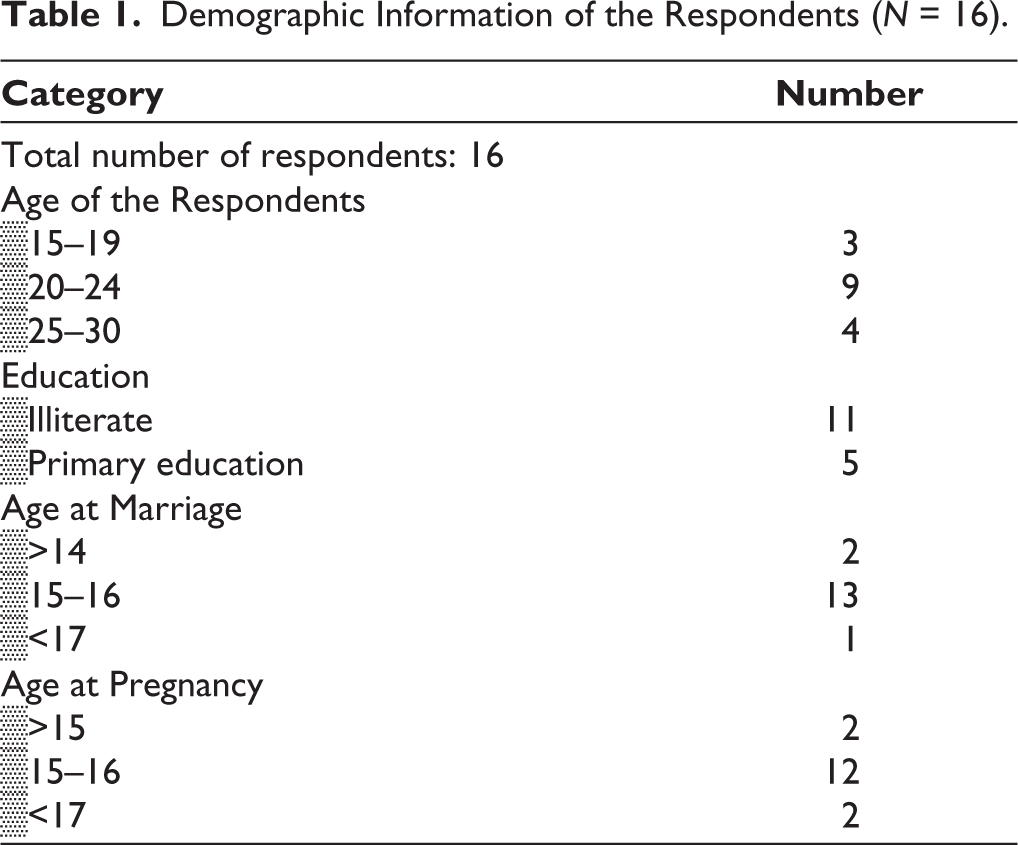
Women under the study are predominantly disadvantaged, living in poor households and are mainly engaged in agricultural and manual labor activities. The participants were interviewed who had a birthing experience in the last 1 year. Three mothers were in their teens (17–19 years), ten were in their twenties (20–29), and three were above thirty. The following Table 1 includes the socio-demographic information of the participants under study, and Table 2 represents the organization of themes.
Demographic Information of the Respondents (N = 16).
Organization of Themes and Sub-themes.
Findings
Theme 1: Early Marriage and Unplanned Pregnancy
Reflexive engagement with the data led to the emergence of this theme that explores how women’s initial maternity journeys. Two sub-themes have emerged as interconnected patterns: first, women narrating their lack of prior conception knowledge coupled with illiteracy, young age marriage and absence of spousal communication; second, poor antenatal care attitude influenced by poverty, cultural beliefs, and neglected spousal support.
Illiteracy and Lack of Knowledge About Preconception
A large number of women narrated their first conception experience with a tone of uncertainty and detachment, reflecting upon the social norms of early marriage and unplanned pregnancy. For instance, a 17-year participant shared:
I got married at the age of 14 forcefully by my in-laws when I visited to my relative’s place and got pregnant at 15. That time I had no idea how a woman becomes pregnant. (Interview-4, age-17)
Another woman who had a teenage conception told:
My husband left home to his work place after few days of marriage. To confirm whether I’m expecting, I could not go anywhere being new to this place. I decided to wait. When my belly became large and the baby started to kick, the neighbor women told me that I’m pregnant. (Interview-3, age-16)
These expressions reveal how women entered into motherhood, confusing pregnancy symptoms, lacking confidence and freedom for seeking timely care and formal confirmation of pregnancy. Also, for most women, neighborhood females served as the trusted informal networks for discussing reproductive health concerns, including pregnancy—other than family members and formal healthcare providers. As a woman shared:
Whatever little I know about family planning, my neighborhood friends have been my source. (Interview-12, age-20)
It was also captured from many women’s accounts that reproductive knowledge emerged gradually through repeated lived experiences of childbirth. One participant, having four children, shared:
I have never been to a school, and I don’t exactly remember at what age I got married and conceived. I understood many things about pregnancy and childbirth after two deliveries. (Interview-13, age-24)
These shared accounts reflect the social norm of illiteracy, early marriage and unplanned pregnancies intersecting together, shaping women’s maternal experience.
Perceived Barriers to Poor Antenatal Care
With regard to the perception and practice of antenatal care, most participants expressed hesitation and confusion about the right time to disclose their pregnancy to the health workers. Consequently, many women had delayed and irregular antenatal care-seeking practice. Such patterns indicate the deep-rooted social conditioning of maternal health practices, where delayed or minimal formal healthcare engagement is normalized. The widespread myths around biomedical practice further reinforce women’s minimal antenatal healthcare. For example, a participant shared:
During my first antenatal visit, they gave me some medicines to eat every day, but after taking those for few days, I threw up rest, as the baby will grow bigger, and cause labor obstruction. (Interview-12, age-20)
The response also reveals the persisting fear and mistrust among women toward biomedical care, discouraging adherence to healthy maternal healthcare practice. Other indicators of negligence would include diet, rest, work burden, spousal support, etc. As a participant painfully shared:
I work for 12 months to sustain my children …. Even during pregnancy, I went to work till my delivery, left only 3 days. She further added: When I refuse sometimes to go for work, my husband says …. I’m acting. He only wastes money on alcohol and would become angry, if I tell him about my craving during pregnancy. His alcohol is more important than my food. So, I used to eat only twice a day. (Interview-9, age-27)
While expressing the agony, pain and emotional neglect were visible on her face, she was burdened by economic constraint and lack of care and love.
Theme 2: Experiencing Birth in Relation to Socio-cultural Setting
Building on the previous analysis, the interpretation of this theme connects multiple narratives around childbirth and explains its cultural construction under social norms and practices. The sub-themes capture not just what they do during childbirth but also why they do it?
Perception, Preference, and Planning of Childbirth
This particular sub-theme reveals how childbirth is perceived and planned under cultural influence. Childbirth through normal vaginal mode is perceived to be natural across the community. Women commonly stated that remaining engaged in physical activities throughout pregnancy would facilitate smooth labor and an easy birth. This reflects that their preparation for childbirth is reinforced with the idea of physical strength and endurance.
Relating to the place of childbirth, some women expressed clear willingness to deliver at home with no plan for institutional delivery. One woman shared her view on hospital birth:
At hospital you have to follow their rules and depend on foods that they provide timely. But at home, we have freedom to follow and do whatever we want. (Interview-15, age-22)
Another woman shared:
I always fear for hospital childbirth. My husband and in-laws also wanted me to deliver at home. (Interview-10, age-24)
While preference for home birth reveals psychological comfort, emotional reassurance, and trust in traditional birth practice among some women, the narratives also revealed patriarchal norms, such as family and spousal influence over individual childbirth decisions, shifting an individual choice to a collective one. As one woman revealed:
Because of my underage pregnancy, my in-laws refused to take me hospital for delivery. (Interview-4, age-17)
The interpretation shows that the childbirth process is not just a preference but carries a deep socio-cultural value within it. On the contrary, some participants who had delivered at the hospital expressed their own concerns. One woman shared:
All my four deliveries happened at the community health center. As I live only with my husband, without any elder female member, it was difficult to manage childbirth and post-partum care at home. (Interview-1, age-27)
Similarly, another woman who lives in a nuclear family shared:
My two deliveries happened in hospital. Only the third child got delivered at home as we could not call ambulance on time. (Interview-15, age-22)
It is also seen that there is a differential preference for means of childbirth patterns based on type of family, where nuclear families prefer institutional childbirth due to a lack of elderly support at home, whereas joint families prefer to deliver at home. A similar finding is also noted by Borah and Sengupta 30 in a tribe of Assam.
Experience of Care and Practice During Labor
Being based on previous sub-theme’s interpretation of participants’ choice and preference relating to childbirth under several influences, this sub-theme captures women’s diverse lived experience of their childbirth process—both at home and hospital setting, and also how they navigate medical emergency situations.
Descriptions of women suggest childbirth process at home was not free from complications. A woman told:
After the delivery of the baby, when the placenta did not come out, family members suggested to wait for a while before taking me hospital. After sitting down in a particular position for around two hours, it came out … it all happened at home. (Interview-10, age-24)
Another participant shared:
I delivered my three children at home. But during the fourth childbirth labor, I felt difficulty in breathing and became unconscious. Then, I was taken to the hospital. (Interview-7, age-25)
Another participant recalled:
I had to go hospital for delivery when it did not happen at home after three days of prolonged labor. (Interview-8, age-19)
Such medical care-seeking instances are interpreted as necessary steps, not as a planned choice, which have already been mentioned by other studies.8,31 Contrary to this, women who delivered in a hospital, majority of them shared a range of experiences. A participant recalled:
After delivery, the doctors advised about taking good care by using warm water, taking milk and healthy foods in diet. There were two lady doctors who were well behaving and treated me well. (Interview-1, age-27)
But one woman shared:
Though the doctors were good, midwife was continuously shouting on me to push and I could see her doing the same on other women also in the labor room. (Interview-16, age-23)
Thus, women’s mixed expressions of both appreciation of treatment and dissatisfaction over institutional birth can be interpreted as women evaluate their childbirth experience not only through clinical treatments but also through emotional care and interaction.
An interesting observation is reported in this study that not a single case of cesarean delivery was found, even though most of them underwent teenage pregnancy; all childbirths occurred through vaginal delivery-whether in home or in hospital. The pattern deeply connects to the wider prevailing local norms around normal childbirth as natural, which is shaped by traditional belief, intergenerational practice, and lesser medical interventions.
Theme 3: Neglected Post-partum Life with Limited Family Planning Practice
Culture of Devaluing Post-natal Care
At a crucial stage of maternal health, the analysis of this sub-theme captures how most women experience minimal or absence of post-partum care. Many women expressed their survival necessity for continuing physical work during the immediate post-partum period. One participant stated painfully:
Husband spends all his earning in alcohol. So, I have to go to work even when I’m ill or weak as I have to feed my children. (Interview-7, age-25)
Their early return to physical work reflects upon economic vulnerability, lack of partners’ support, and cultural norms undervaluing post-partum care and rest.
Women in their post-delivery usually perceived health issues of anemia, weakness, giddiness, body pain pertaining to their extensive workload, lack of a healthy diet and rest. A few participants mentioned about prolonged bleeding for days following childbirth. A participant shared in a painful voice:
I feel weak many times, due to workload and lack of care for my own food. Now, Sometimes, I think being married early and bearing small children affecting my health badly. (Interview-15, age-22)
Another participant shared:
I started doing household chores only after seven days of my delivery. My mother-in-law never helps me with any work. Instead, she scolds me and says bad things about my character. (Interview-3, age-16)
However, despite such issues, women barely took post-partum health assistance, medicines, and follow-up checkups. It is interpreted as how women’s post-partum practice is adversely affected under economic compulsion, emotional and physical neglect. Only in a few cases, women revealed that their husbands’ support in household chores helped them recover, indicating some variance existing in post-partum care and support under individual family dynamics within the community.
Poor Contraception, Denied Spousal Support and Child Spacing
Like post-partum care and rest, contraception practice among women was seen to have unfavorable attitude. Reasons include prevailing misconceptions, fear of side effects, spousal denial, and lack of awareness. These findings are also consistent with the earlier studies15,21,32 conducted among tribes of Odisha. Generally, women in the study reported abstaining from sexual intercourse for spacing childbirth. A participant sharing her post-partum contraceptive practice told:
I make sure to avoid intercourse after one delivery, at least for one year. (Interview-5, age-22)
Another woman told:
We husband and wife never discuss on such things. I gave three years gap between two deliveries only being abstained from intercourse.
However, this method was not supported by her partner, as she further expressed in a distressing voice:
When I refused to have sex after my first delivery, husband brought another woman and stayed with her for 3 years. (Interview-10, age-24)
Such cases highlight the absence of spousal cooperation, gendered coercion, and emotional vulnerability of a woman, making the post-partum period fragile.
Also, some women specifically voiced that their husbands resist their sterilization due to mistrust about infidelity. One woman shared with visible distress on her face:
My husband says… after your sterilization, you will sleep with many men (Interview-1, age-27)
This expression captures the prevailing suspicious norms under patriarchy, suppressing women’s reproductive decision-making autonomy. Women usually self-terminated pregnancy by taking informal help without medical consultation. These instances capture the norm of silence and secrecy surrounding contraceptive decision-making across the community, strongly advocating the existence of family planning illiteracy, male dominance, and limited autonomy over their sexual and reproductive health.
Theme 4: Emotional, Familial, and Social Support
Following the interpretation of neglected post-partum life of the participants, this theme emphasizes upon understanding the emotional and social realm experienced by them in everyday life in terms of stress, abuse and support and its potential impact on maternal health. Like many other studies,8,10,33,34 the research has recognized the influence of emotional factors on pregnancy and childbirth pertaining to several shifting changes and influence of partner and family.
Physical and Socio-psychological Distress
This study revealed that unsupported and stressful events shared by women are primarily experienced from partners and family members. For instance, a participant who had a teenage pregnancy described:
My in-laws blamed me for my teen age gestation throughout pregnancy and post-pregnancy. Despite the fact, their son had married me forcefully. (Interview-4, age-17)
A woman shared:
We husband and wife often get indulge in fight when I refuse to have more children. As I have two girl children, my in-laws and husband want me to give birth till a male child is born. But I do not want to give birth again. (Interview-5, age-22)
Verbal and physical abuse is widely practiced against women throughout maternity. A participant showing her facial injury told:
My husband beats me and hurts with weapons often. He even had kicked me in the abdomen while I was seven months pregnant. (Interview-2, age-25)
Physical violence and abuse during pregnancy as a significant risk factor has already been stated by many35–37 who make women vulnerable to unspaced childbirth, fear of negotiation in sexual relations and poor control over their own fertility. On the contrary, a woman said:
My husband helped me doing household chores throughout my pregnancy and childbirth. I even remained at home and he never forced me to go for work as I was feeling weak throughout my pregnancy. (Interview-6, age-22)
While a few received some help, most women underwent physical and mental distress, and loneliness due to alcoholic and abusive partners, a strong patriarchal attitude, and an unsupportive family, making maternity experiences more isolated, powerless, and oppressive.
Unsupportive Care and Response of Health Workers
Women discussed the irregular contact and visits made by the village health worker, that is, the ASHA. They said the ASHA visits when a woman gives birth. But she often informs them over phone calls regarding immunization and antenatal or post-natal care. A few women also mentioned:
Many times, we had to pay some amount of money to the ASHA to get her company during check-up and delivery.
Another woman, already having three childbirths, viewed:
ASHA never explained what to use and how to use. So, from where will I get the information? I only know that a woman can terminate her pregnancy by taking some kinds of pills. (Interview-7, age-25)
Women are less inclined to use effective maternity health services since they think that the health workers do not show concern during critical times. For instance, a woman said:
During my second childbirth we could not contact an ambulance and ASHA also refused to accompany us for hospital birth. So, I delivered at home. (Interview-6, age-22)
Two other participants shared:
ASHA informs about the family planning sterilization camp but does not arrange any transport facility and also never accompanies us. (Interview-7 and -8)
Moreover, women shared poor informational and follow-up care throughout their maternity from the health workers. These expressions not only reveal dissatisfaction with the village health workers, but also a contributing factor toward their feeling of neglect from institutional healthcare, compelling women toward their traditional practices and informal networks of care.
Theme 5: Ethno-medical, Traditional Practices and Superstitions
Being based on all stages of maternity experience—this final theme draws a better interpretation of all intertwined cultural and traditional healing practices and carried superstitions among women. The theme captures the ethno-medical aspects that include not just herbal treatments, but also food, medicines and symbolic beliefs.
Traditional Maternal Healing and Care Practices
This sub-theme explores healing practices followed during pregnancy, childbirth, and post-partum phases, reflecting on indigenous ethno-medical care methods. These tribal women revealed a contrasting picture of traditional food practices followed during pregnancy and the post-partum period. Unlike many findings,
19
these Munda women did not avoid eating papaya, considering it a traditionally healthy food to be consumed during pregnancy. A participant told:
Eating papaya during pregnancy is commonly followed from ancestor times. We eat all vegetables including non-veg during pregnancy…. but when delivery happens, we don’t eat non-veg at least for one month. The more one avoids non-veg and oily foods, it’s good for health. (Interview-9, age-27)
Interestingly, some women also did not avoid taking alcohol (Handia), as one participant replied:
Alcohol consumption is a regular thing for us … it is harmless as it is made from fermented rice. (Interview-13, age-24)
While pregnancy is associated with no such food restrictions, their immediate post-partum phase is marked by many dietary restrictions of avoiding alcohol, non-veg, oily and spicy foods, and cold water. They eat bland and boiled food, hot rice water, garlic, roasted salt and even some roasted vegetables. These food practices reflect upon the culturally practiced healing ritual and the community’s ethno-medical belief of post-partum recovery and good maternal and child health.
Their childbirth healing and care practices at home involve mustard oil massage to ease labor, burying placenta securely, and delaying the bath of the newborn to ensure safe drying of the naval cord and isolating the mother and the newborn. One participant revealed:
If a woman becomes weak or unconscious during her labour at home, hot oil message is applied on her feet and palm. Also, she is given warm water or milk to drink. (Interview-14, age-21)
These practices reflect on the localized maternal knowledge of bodily care and healing methods. However, conducting delivery by elderly women without medical assistance also points to the higher possibility of adverse maternal health risks and emergencies.
Cultural, Symbolic Beliefs and Superstitions
In the present study, the people were found to follow and cherish their ethno-medical practices and traditional belief system, though they are distanced from their native environment. However, they managed to follow some culturally competent practices in many possible ways. One participant explained:
In our village it is easy to find herbal medicines like plants, roots and leafs from the healers and from jungle. People visit the local healer on regular basis. But here we are mostly dependent on medicines available in the hospital. The local healer of this place also has limited access to herbs. (Interview-11, age-23)
However, the ethno-medical practices are interwoven with superstitious beliefs, influencing the understanding and management of women’s reproductive health. One woman sharing her experience of confirming her pregnancy told:
When I suspected that I might be pregnant and my husband was away from home, he advised me to visit the ‘Gunia’ (local healer) with vermilion (Sindoor) to confirm the pregnancy. (Interview-3, age-16)
Another woman told:
I have seen that a woman of our village lost her three infants one by one because of the evil witchcraft. So, we avoid stepping out to specific places … who will waste money by visiting the local healer or temple to seek remedies if anything bad happens? (Interview-13, age-24)
These traditional practices and superstitions can be interpreted as deeply rooted cultural strategies functioning as protective agencies during a vulnerable phase of life, like maternity.
Discussion
The study exploring lived experience of pregnancy and childbirth among the Munda tribal community identifies early marriage as a deeply rooted social norm, and women become pregnant before they can fully comprehend its implications and undergo difficulty in planning and executing a healthy maternity. Additionally, the burden of survival and emotional neglect under unequal gender power relations places them on the verge of detrimental maternal health effects.
Modern healthcare still remains largely underutilized among these women, similar to the documentation of other studies.31,38 The women are also seen not to access the Primary Health Center (PHC) even though they stay very close to it, capturing the fact that the availability of a healthcare facility does not always ensure their usage. This relates to the other existing studies. 36 Moreover, these tribal women found less likely to experience positive and healthy maternity, as stated by the World Health Organization. 12
Thematic interpretation captures how the biological process of pregnancy and childbirth are contextualized culturally through a series of rituals, traditional practices and superstitions. As Haq 2 makes the point, often culture mediates through people’s own perception, reflected in their cultural significance attached to home childbirth. In contrast, institutional birth is simply understood as a medical event 6 and constitutes an outsider’s domain. 7 In line with the existing findings, 39 reluctance toward institutional childbirth in this study reflects upon the existing conflict between the biomedical understanding and with those cultural and symbolic maternal health practices of the community. However, other than cultural, traditional, and emotional factors, their hesitation for institutional birth also reflected on practical challenges like getting cooperation from the health worker, timely information or arranging ambulance transportation.
The findings of limited choice and autonomy of contraception even in the post-partum period-such as being forced not to adopt sterilization under male domination, reflect deep-rooted patriarchy reproductive domination. Lazarus 11 had made the point that choices, expectations, and desires are limited for the women living under socio-economic constraints. As a result, these women fail to execute healthy maternal practice having lack of social resources. 40 In line with the existing studies,8,10 unlike higher-class women with liberal gender roles, these poor and disadvantaged women undergo mostly unsupported and neglected birthing experiences.
While the study documented several adverse maternal outcomes, the practice of normal deliveries reflects a complex interplay between their cultural resilience of supporting normal childbirth and widespread silence over emotional suffering and also discourages timely care.
By recognizing their poor maternal practice, foremost is deep engagement with the contextual realities that shape their pregnancy and childbirth experience. Special concern is for addressing the persistent domestic violence, patriarchal structure and abuse against these women. In a study, Blanc 34 had pointed out that the issue of unequal power relations can be addressed through healthcare provision to improve women’s health. To fulfill the large communication gap between women and modern healthcare, primary healthcare workers can create a conducive environment for effective provision of maternal health services by integrating emotional and cultural aspects. The study appeals to the need for using a gender-sensitive approach to promote women’s reproductive decision-making power and autonomy.
Conclusion
In conclusion, the study reveals a complex interplay of social context, cultural norms, gendered power relations and structural barriers affecting tribal women’s pregnancy and childbirth experience. As traditional beliefs and cultural norms are deeply associated with poor maternal healthcare-seeking practices, the healthcare provision in such a context requires a culturally sensitive approach.
Limitations and Strengths
The study carries a limitation that it has not collected data from the side of health workers of the community, which may likely have some information gaps. Despite this limitation, the current study has methodological strength to get a more comprehensive understanding of women’s experience relating to pregnancy and childbirth within their socio-cultural context. The findings and knowledge would help in identifying potential underlying issues affecting poor maternal health status of these women.
Footnotes
Acknowledgements
I am very grateful to my research supervisor for her guidance throughout the research process. The authors extend their sincere gratitude to the respondents for their responses and coordination.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The ethics approval was obtained from the Institutional Ethics Committee (IEC) of Gangadhar Meher University, India (Reference No- 12318).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Verbal consent has been obtained from the respondents included in the study. Information regarding the research aim, questions, and objectives and respondents right provided to the respondents to ensure voluntary participation. The research strictly maintained the ethics of research and confidentiality, including the identity of the respondents.
Notes
Gunia: Local healer
Handia: Local alcohol made from Rice