
Abstract
Transgender individuals experience notable disparities in life outcomes relative to their cisgender counterparts. This explanatory mixed-methods study aimed to explore the relationships between early experiences and gender identity to identify factors contributing to different life outcomes among the transgender community. Quantitative data were analyzed from the 2023 Behavioral Risk Factor Surveillance System (BRFSS) survey of the Centers for Disease Control and Prevention (CDC), including 284,929 transgender and cisgender adults in the United States. Online qualitative interviews were conducted among 21 transgender individuals to expand upon the quantitative findings. In the quantitative component, transgender respondents reported significantly more adverse childhood experiences (ACEs) and worse outcomes in mental health, education, and income than cisgender respondents. Key factors such as lack of support, exposure to mental health and substances, household incarceration, and neglect significantly interacted with gender to predict poor life outcomes. In the qualitative component, five themes emerged from the thematic analysis, relating to participant experiences: the impact of family dysfunction, body discomfort before and after transitioning, relatedness and belonging, the importance of social support, and community and healthcare dilemmas. These findings highlight the importance of support systems at the familial, community, and healthcare levels. Transgender individuals who reported positive family functioning, strong support networks, and access to care were found to have better life outcomes. Future research endeavors should examine the perspectives of family members, friends, school faculty, and healthcare professionals to gain a more comprehensive understanding of factors contributing to social inequities within the transgender community.
Keywords
Introduction
Transgender individuals experience notable disparities in life outcomes, including higher rates of depression, anxiety, suicidality, social isolation, and substance use, and lower rates of life satisfaction, education, income, and employment as compared to their cisgender peers.1,2 Research indicates that transgender individuals are at increased risk for poor life outcomes (i.e., education, income, employment, and mental health) compared to their cisgender peers.3–5 These disparities have been attributed to stigma, discrimination, and unstable family environments. However, factors such as positive family functioning have been shown to mitigate adverse outcomes, particularly in mental health.6,7 The family environment plays a crucial role in a child’s development and can have long-lasting effects on an individual’s transition into adulthood.3,6 However, there is a limited understanding of the mechanisms linking early experiences and gender identity to later life outcomes. According to a recent report, over 1.3 million adults (0.5%) and 300,000 youth aged 13–17 (1.4%) in the United States identify as transgender. Moreover, the number of transgender individuals seeking hormone therapy and gender-affirming surgery has increased, particularly in the United States. 8 Given the prevalence of individuals identifying as transgender and seeking care, it is crucial to gain a deeper understanding of transgender experiences and factors that promote positive life outcomes. 9
Literature Review
Research on transgender individuals has consistently identified three major themes: disproportionately higher rates of adverse childhood experiences (ACEs), mental health conditions, and discrimination.2,3,9,10
Adverse Childhood Experiences
Transgender individuals frequently report growing up in unstable family environments during childhood and adolescence. 3 These environments may expose youth to ACEs, which encompass a range of potentially traumatic events occurring before the age of 18, such as household separation, abuse, neglect, bullying, exposure to substances, inconsistent caregiving, lack of support, and financial instability.6,11 These experiences can disrupt a child’s development and their ability to successfully transition into adulthood, contributing to poor outcomes in physical and mental health. 3 Without a supportive environment during critical developmental periods, children may be at a greater risk for developing mental health conditions and face more difficulty navigating milestones. 6
In the United States, transgender individuals report significantly higher rates of both single and multiple ACEs compared to the cisgender population. Specifically, transgender patients are more than twice as likely to report at least one ACE (80% vs. 34%) and nearly five times more likely to report four or more ACEs (28.6% vs. 5.7%) than cisgender individuals, with parental and peer abuse being the most commonly reported. 12 It is important to note that these experiences are not the cause of individuals identifying as transgender. Rather, these findings may shed light on a potential influence between ACEs and later life outcomes within the transgender community, as well as provide insight for improving contemporary interventions.
Mental Health
Transgender individuals report disproportionately higher rates of psychiatric conditions compared to the cisgender population. These conditions include depression, anxiety, suicidality, bipolar disorder, attention-deficit/hyperactivity disorder (ADHD), adjustment disorder, dysthymia, and post-traumatic stress disorder (PTSD).2,12 A large-scale cross-sectional study examining over 50 million patient charts found that 58% of transgender patients had at least one psychiatric diagnosis, compared to 13.6% of cisgender patients. 13 Unstable family environments can exacerbate mental health challenges and hinder an individual’s ability to transition into adulthood.3,14 As a result, transgender individuals often experience worse mental health and socioeconomic outcomes. It is important to note that while several factors contribute to mental health outcomes, family stability is particularly important during a child’s development as it provides a secure environment that is critical for later adjustment into adulthood. 3
Discrimination Experienced by Transgender Individuals
Transgender individuals face unique challenges related to marginalization and victimization that may contribute to an increased risk of adverse outcomes.2,14,15 Discrimination takes many forms, including harassment, bullying, stigmatization, and physical violence, and affects various aspects of life, including healthcare, housing, employment, and education. 16 Social inequities stemming from discrimination serve as major stressors, increasing the risk for mental health conditions such as anxiety, depression, and suicidality.2,17
Transgender individuals face several barriers to accessing care, further contributing to transgender health disparities. These individuals frequently encounter discrimination and mistreatment in clinical settings that may threaten their healthcare status.18–20 Additionally, many general practitioners report a lack of knowledge regarding transgender health needs and express difficulties in communicating trans-specific health information. These gaps in understanding and providing trans-specific healthcare serve to enlarge existing health disparities.18,20
Despite the effects of discrimination, several protective factors have been identified among transgender individuals. Research has shown the importance of parental, peer, and school support in mitigating poor mental health outcomes and promoting positive development. 16 However, little is known about how these protective factors function and change over time as transgender individuals progress from childhood to adulthood. 21
Current Study
Despite the existing body of research, notable gaps exist in our understanding of the mechanisms linking early experiences and gender identity to later life outcomes. Existing studies on transgender individuals have primarily been quantitative investigations that describe trends but alone fail to capture the distinctive experiences of transgender individuals. As a result, quantitative results alone may be inadequate to describe the mechanisms behind these trends.
An explanatory sequential mixed-methods design was used to explore the impact of early experiences and gender identity on later life outcomes among transgender individuals. In the first phase, quantitative data from the Behavioral Risk Factor Surveillance System (BRFSS) provided by the CDC were collected from transgender and cisgender adults to address the relationship between ACEs, gender identity, and life outcomes. 22 In the second phase, semi-structured individual interviews were conducted with transgender individuals as a follow-up to the quantitative results and explored experiences relating to gender identity from childhood to adulthood. As such, the present study aimed to (a) examine the differences in ACEs and life outcomes between transgender and cisgender individuals, (b) explore interactions between ACEs and gender identity and its effect on later life outcomes, and (c) explore early experiences relating to gender identity to inform approaches to provide more effective support for transgender individuals. The study hypothesized that ACEs would disproportionately impact life outcomes within transgender individuals compared to cisgender individuals.
Research Questions
The study included two quantitative questions, two qualitative questions, and one mixed question. The results from the quantitative phase were used to inform the qualitative phase.
What are the differences in ACEs and life outcomes between transgender and cisgender individuals?
What interactions exist between ACEs and gender identity in relation to life outcomes?
How does support for gender identity impact the lives of transgender individuals?
What factors contribute to positive life outcomes among transgender individuals?
How do the experiences of transgender individuals from childhood to adulthood impact later life outcomes?
Methods
Sample
Quantitative Sample
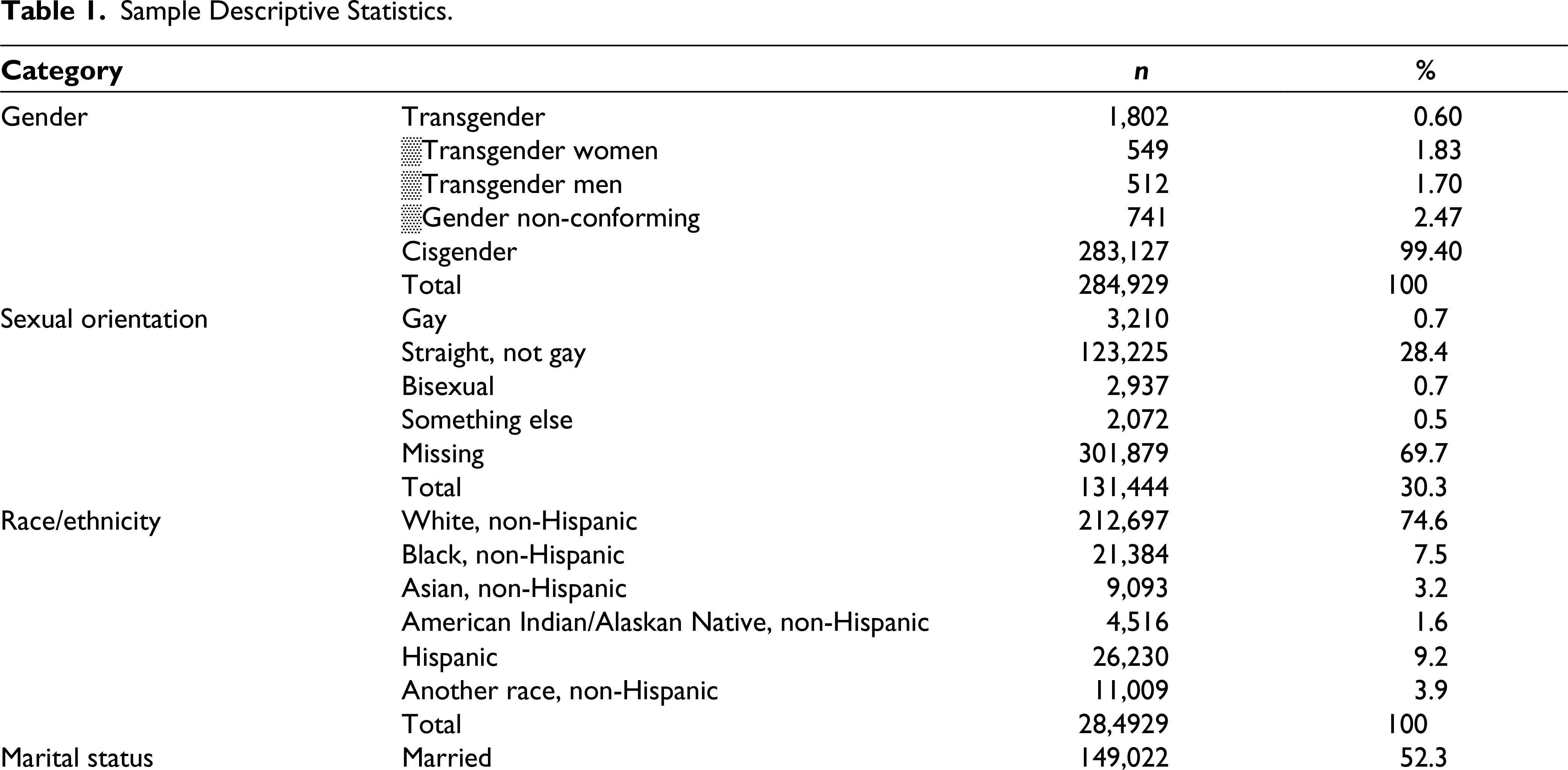
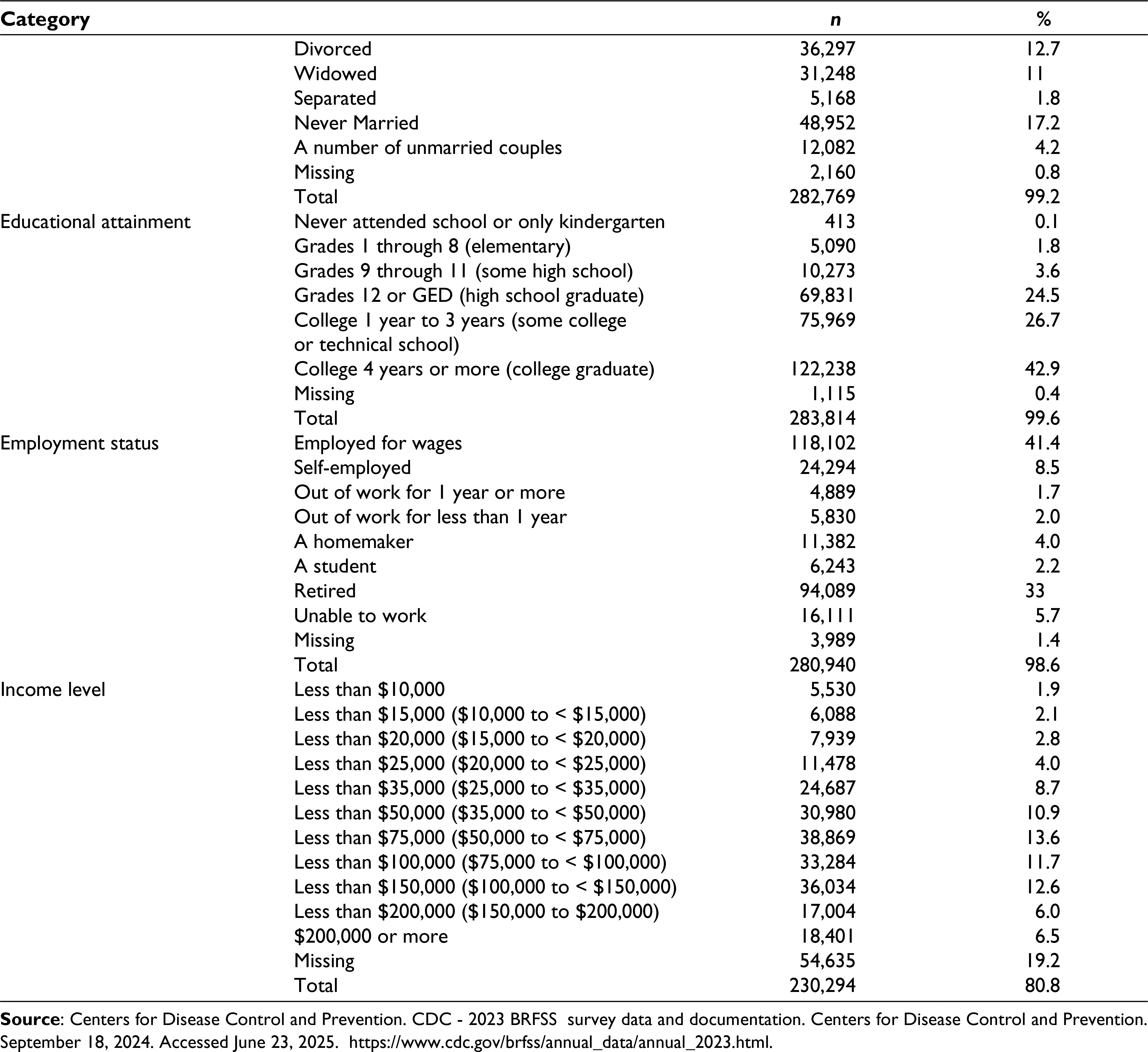
The current study analyzed adults (n = 284,929) who completed the BRFSS telephone survey from the state health departments. 22 These individuals were randomly selected from various regions, contacted by phone, and asked a series of questions by the interviewer. The sample compared transgender individuals (n = 1,802) with cisgender individuals (n = 283,127). The transgender group included participants who identified as transwomen, transmen, and gender non-conforming. Table 1 shows the demographic characteristics of the sample, including missing data, which was removed for analysis. Individuals who did not identify as cisgender or transgender were excluded from the sample.
Sample Descriptive Statistics.
Qualitative Sample
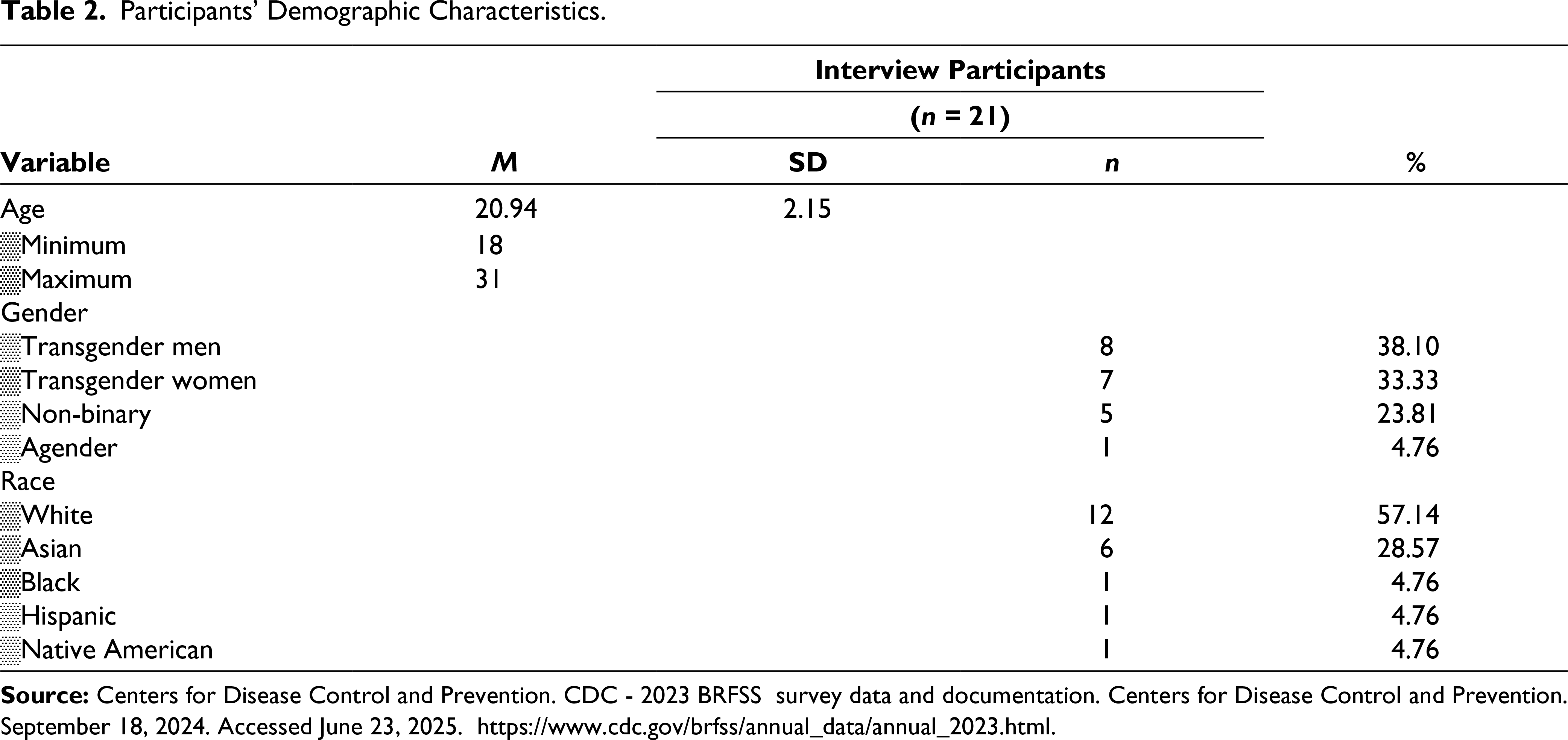
The qualitative phase consisted of individual semi-structured interviews with transgender individuals over the age of 18 years. A total of 21 transgender individuals were recruited between October 2024 and December 2024 in the United States, with a mean age of 20.94 years (SD = 2.15). Table 2 presents the demographic characteristics of the qualitative sample.
Participants’ Demographic Characteristics.
Protection of Human Subjects
This study was approved by the University of Michigan Institutional Review Board (IRB).
Measures
Quantitative Measures
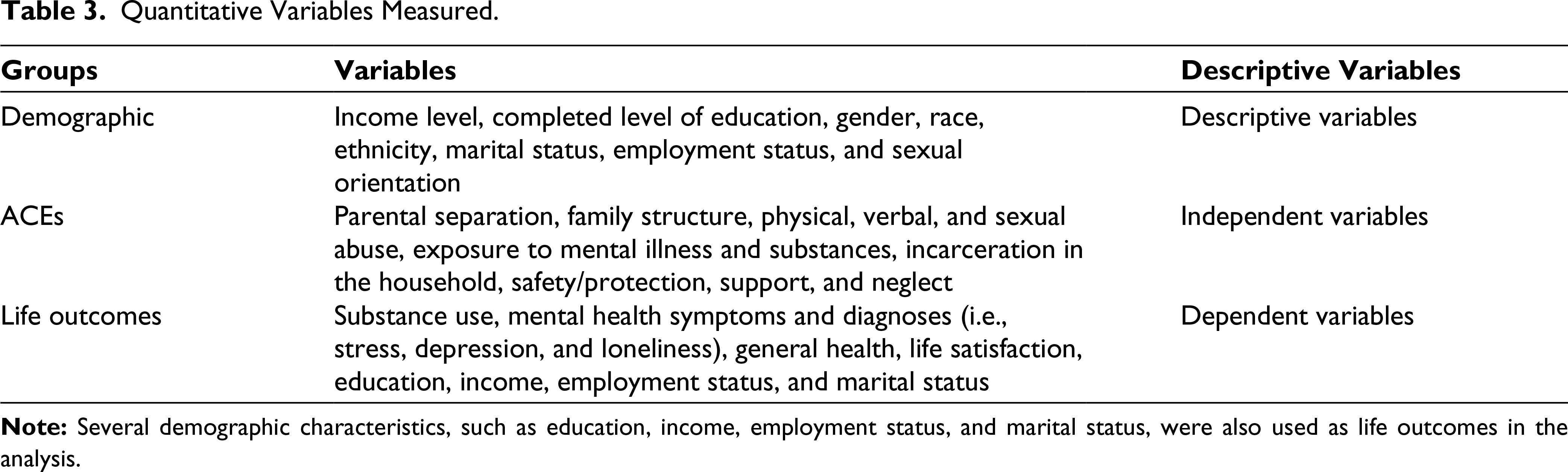
Quantitative data were collected from the 2023 BRFSS, which included self-reports of gender identity that provided options for respondents to identify as transgender men, transgender women, and gender non-conforming. 22 The BRFSS survey is broadly representative of US adults, utilizing a dual-frame (landline and cellular) sampling design and an advanced raking-based weighting. The data set included 350 variables that were analyzed using SPSS 29.0. These variables were grouped into three categories: demographic variables, ACEs, and life outcomes. Table 3 shows a full listing of variables used in the analysis.
Quantitative Variables Measured.
Qualitative Measures
Interview questions were developed based on preliminary quantitative findings to explore the experiences of transgender adults from childhood through adulthood and inform contemporary treatment approaches.
The interview questions are listed below:
How would you describe your relationship with your family growing up? In relation to caretakers In relation to siblings In relation to other family members What was your experience when you first started exploring gender? What was it like to share your identity with people in your life? How does the support for your identity now compare to when you first came out? What aspects of support positively impact your life? What experiences (if any) negatively impact your life? What challenges (if any) have you faced with your identity? How has your gender identity impacted your life regarding employment and school? How would you describe your current health and overall well-being? What factors in your life improve or worsen your mental health in relation to your gender identity? What could the community or the health care system change to better support transgender individuals?
Quantitative Data Collection
Quantitative data were collected from existing secondary data. The 2023 BRFSS collected data from 433,323 US residents (>17 years) on health-related risk behaviors, chronic health conditions, and healthcare access. 22
Qualitative Data Collection
Participants were recruited through flyers posted at the University of Michigan, Michigan Medicine clinics, and on social media platforms. Once participants provided their written consent, the lead researcher scheduled a 30–45-minute semi-structured interview using video conferencing software. Audio recordings were taken from each interview and transcribed verbatim for analysis to identify recurring themes from participants.
Data Analysis
Quantitative Data Analysis
The quantitative data were analyzed using SPSS 29.0 through a positivist paradigm. Data was pre-processed by identifying and removing invalid responses and updating variable labels. To address Aim 1, univariate explorations were performed to examine distributions such as frequency, mean, mode, and standard deviation for demographic variables to describe the sample. Bivariate analyses were performed to identify the frequency of ACE and life outcome variables between transgender and cisgender individuals. Chi-square tests and independent t-tests were used for categorical and continuous variables, respectively. Additionally, one-way ANOVA analyses were conducted for ACEs and life outcomes to account for potential confounding variables, including race and ethnicity. To address Aim 2, linear regressions were used for interaction analyses to determine if any significant interactions existed between ACEs and gender in relation to life outcomes.
Qualitative Data Analysis
The qualitative component used NVivo 15.0 for thematic analysis to address Aim 3 through a critical realist paradigm. This method was used to identify, analyze, and interpret recurring patterns and themes among participants. 23 The lead researcher first became familiar with the data by re-reading all participant interview transcripts, listening to the audio recordings, and taking preliminary notes. A second researcher coded 20% of the transcripts that were de-identified to add inter-rater reliability. The transcripts were systematically coded, and recurring themes were identified with the support of participants’ quotations. The lead researcher contacted participants and provided them with the opportunity to review and verify the findings from the analysis, and several confirmed the accuracy of the findings.24,25
Results
Quantitative Phase
Adverse Childhood Experiences
Chi-square tests were conducted to compare the frequency of ACEs in transgender and cisgender individuals. Results indicate that transgender individuals were more likely to report several ACEs compared to their cisgender counterparts, as shown in Table 4. Significant interactions were found between gender and exposure to alcohol (χ²(1) = 15.46, P < .0011), exposure to mental illness (χ²(1) = 150.69, P < .001), exposure to illegal drugs (χ²(1) = 17.09, P < .001), household incarceration (χ²(1) = 9.05, P = .003), parental separation (χ²(1) = 30.74, P < .001), physical abuse (χ²(1) = 37.41, P < .001), verbal abuse (χ²(1) = 81.01, P < .001), sexual abuse (χ²(1) = 17.15, P < .001), and domestic abuse between parents (χ²(1) = 24.18, P < .001). Transgender individuals were significantly more likely to report these ACEs.
Adverse Childhood Experiences and Gender Chi-square Analyses.
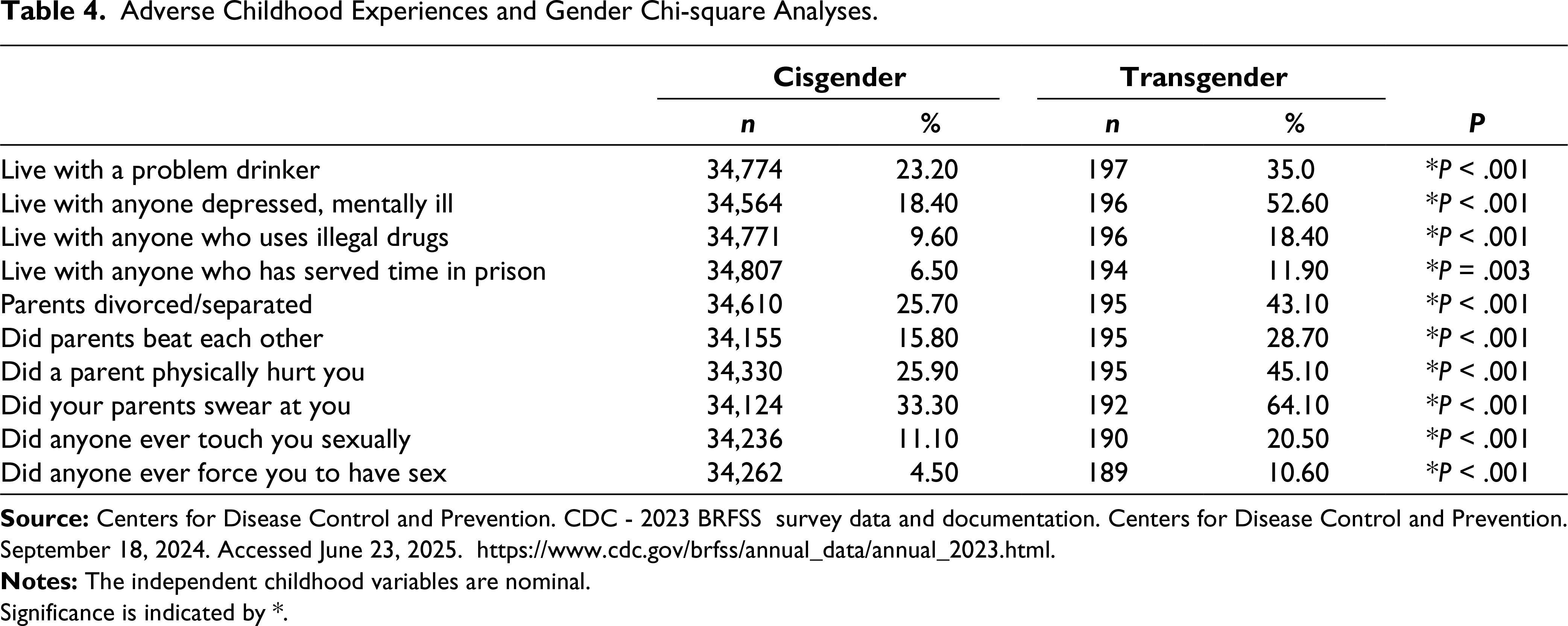
Significance is indicated by *.
Cisgender individuals were significantly (P < .001) more likely to report always having basic needs met (98.3% vs. 92.2%), always feeling safe and protected (95.1% vs. 76.3%), and always receiving social and emotional support (93.2% vs. 82.8%) compared to transgender individuals.
Life Outcomes
Chi-square tests and independent t-tests were conducted to examine the relationship between gender and life outcomes. The cisgender sample was significantly (P < .001) more likely to be married (75.5% vs. 33.7%) and retired (39.9% vs. 17.3%) compared to the transgender sample. Additionally, transgender individuals were significantly (P < .001) more likely to be told they had depression (55.6% vs. 20.5%) than cisgender individuals.
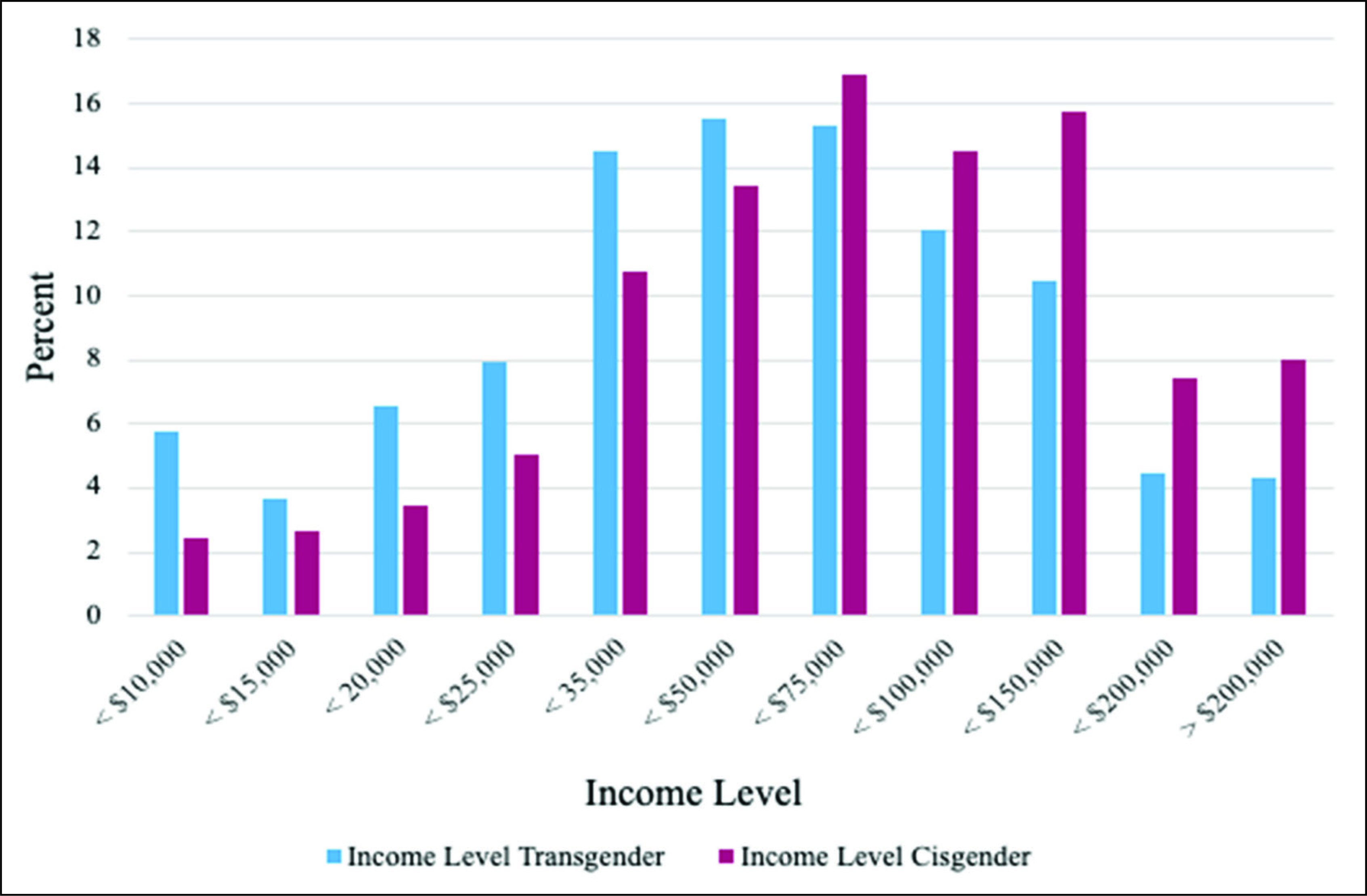
Independent t-tests analyzed gender and continuous life outcome variables: education, income, poor physical and mental health days, substance use, life satisfaction, and loneliness. The results are shown in Table 5. Independent t-tests found a significant difference in education t(1807.01) = –11.03, P < .001, and income t(1391.83) = –13.403, P < .001 between the means of the two groups. Further analysis revealed that cisgender individuals were significantly (P < .001) more likely to complete four or more years of college (63.7% vs. 51.4%) and earn $50,000 and above (62.4% vs. 46.3%) than transgender individuals. Figure 1 displays the income levels of the transgender and cisgender samples.
Independent T-tests for Gender and Life Outcomes.
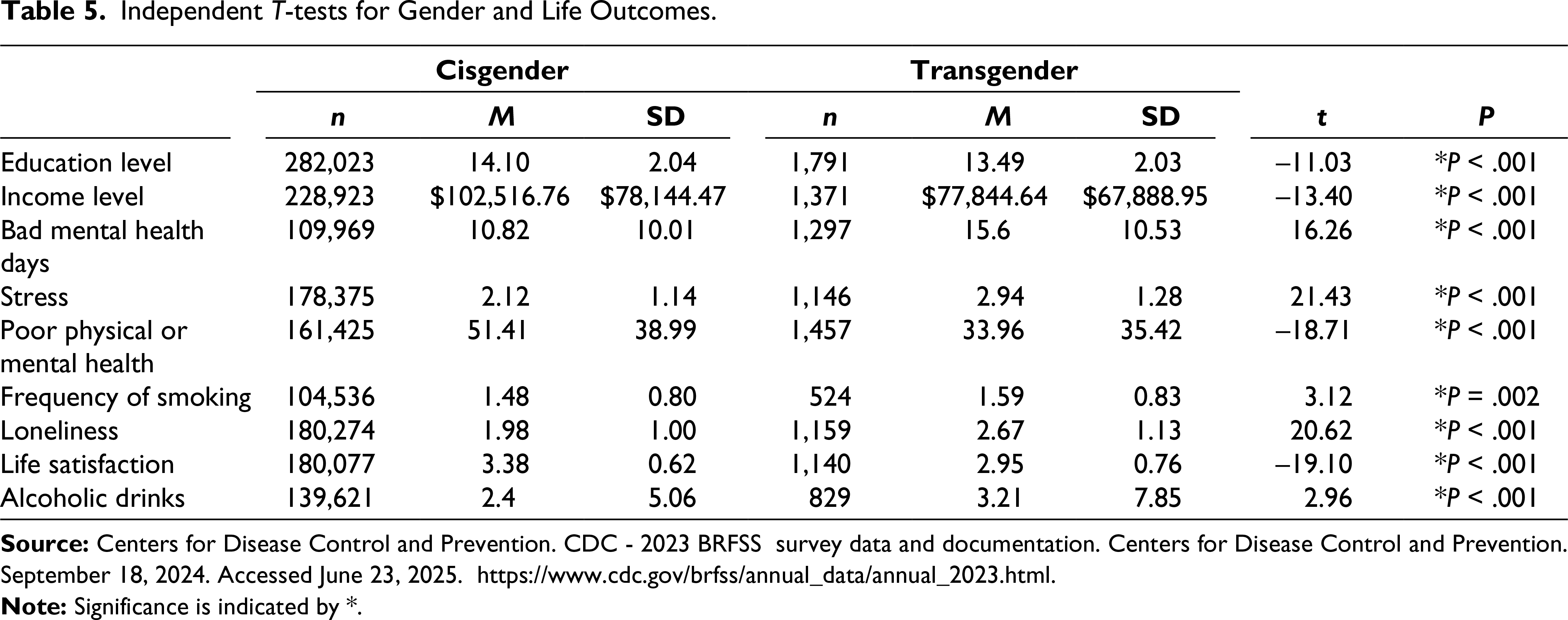
The transgender sample had significantly (P < .001) worse mental health outcomes than the cisgender sample, including a higher average of bad mental health days, t(1323.74) = 16.26, P < .001. Transgender individuals were significantly more likely (P < .001) to report being stressed (54.7% vs. 15.0%), feeling lonely (39.7% vs. 8.2%), and dissatisfied with life (43.5% vs. 8.5%) compared to cisgender individuals.
Confounding Variables
Gender remained significant (P < .05) for poor physical and mental health days, education level, income level, life satisfaction, loneliness, depression, stress, employment status, marital status, smoking, alcohol use, and all ACE variables after controlling for race and ethnicity.
Interaction Analysis
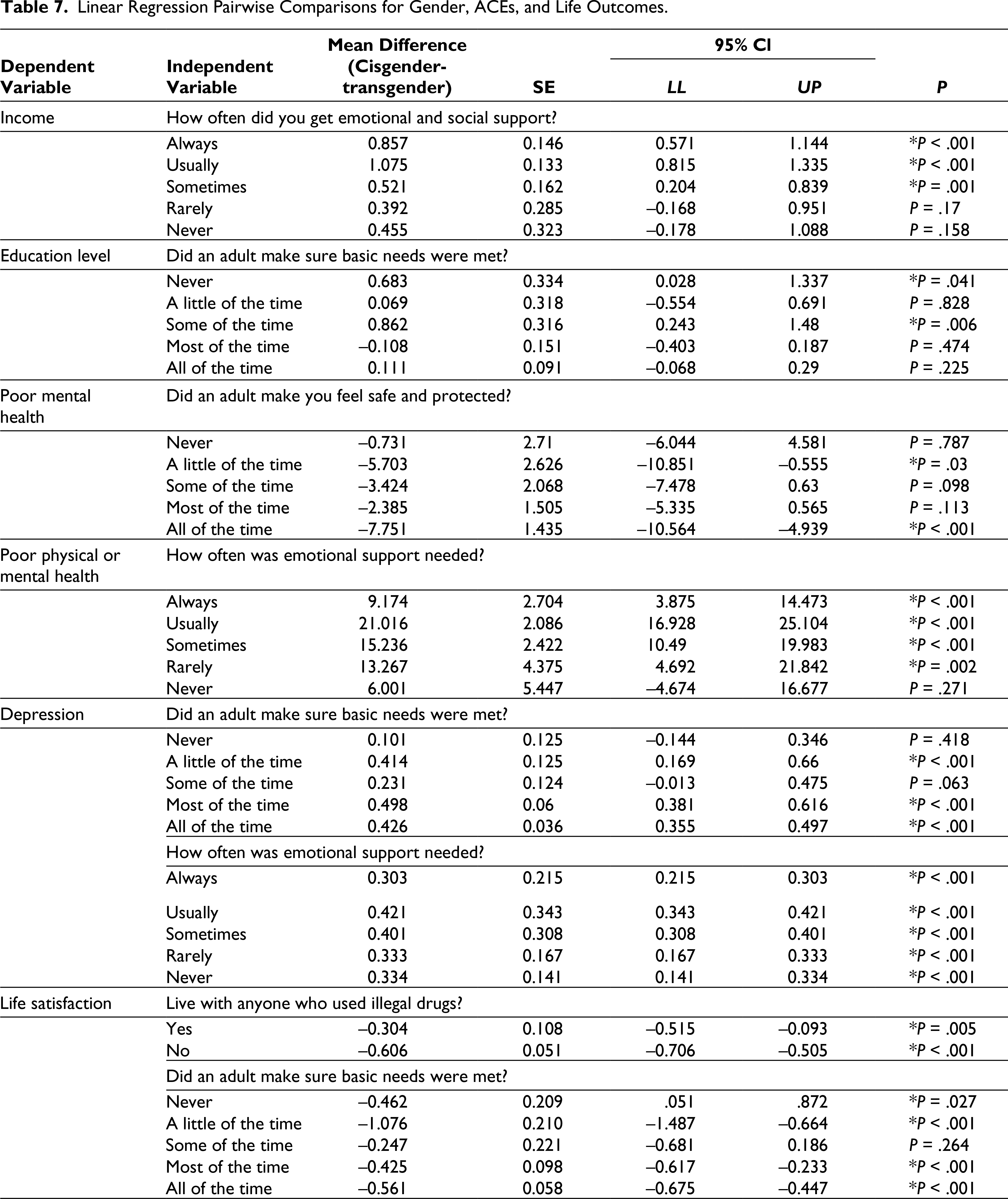
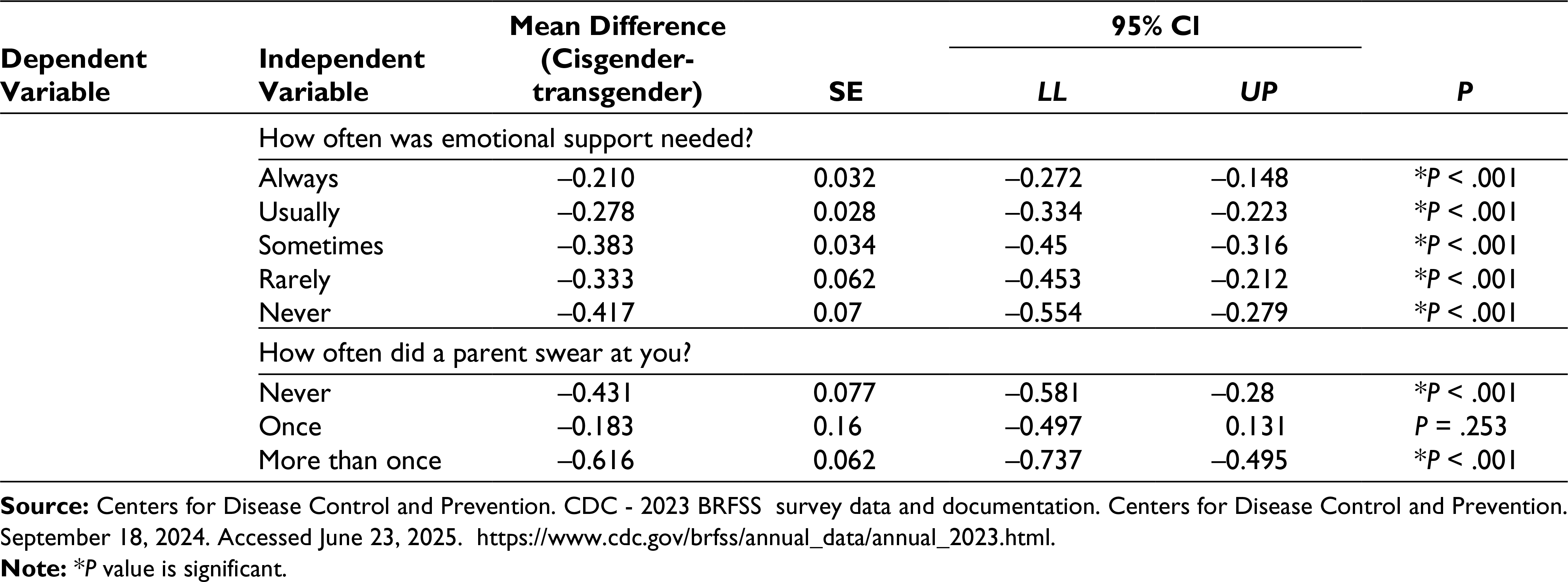
For Aim 2 of the quantitative phase, linear regression analyses were performed between ACEs, gender, and life outcomes. Significant interactions were found between ACEs and gender for education, income, poor physical or mental health days, and life satisfaction. Descriptions for between-subject effects for gender, ACEs, and interaction variables are shown in Table 6. Pairwise comparisons examining the mean differences between the two groups for each interaction are shown in Table 7.
Tests of Between-subject Effects: Interaction Analysis.
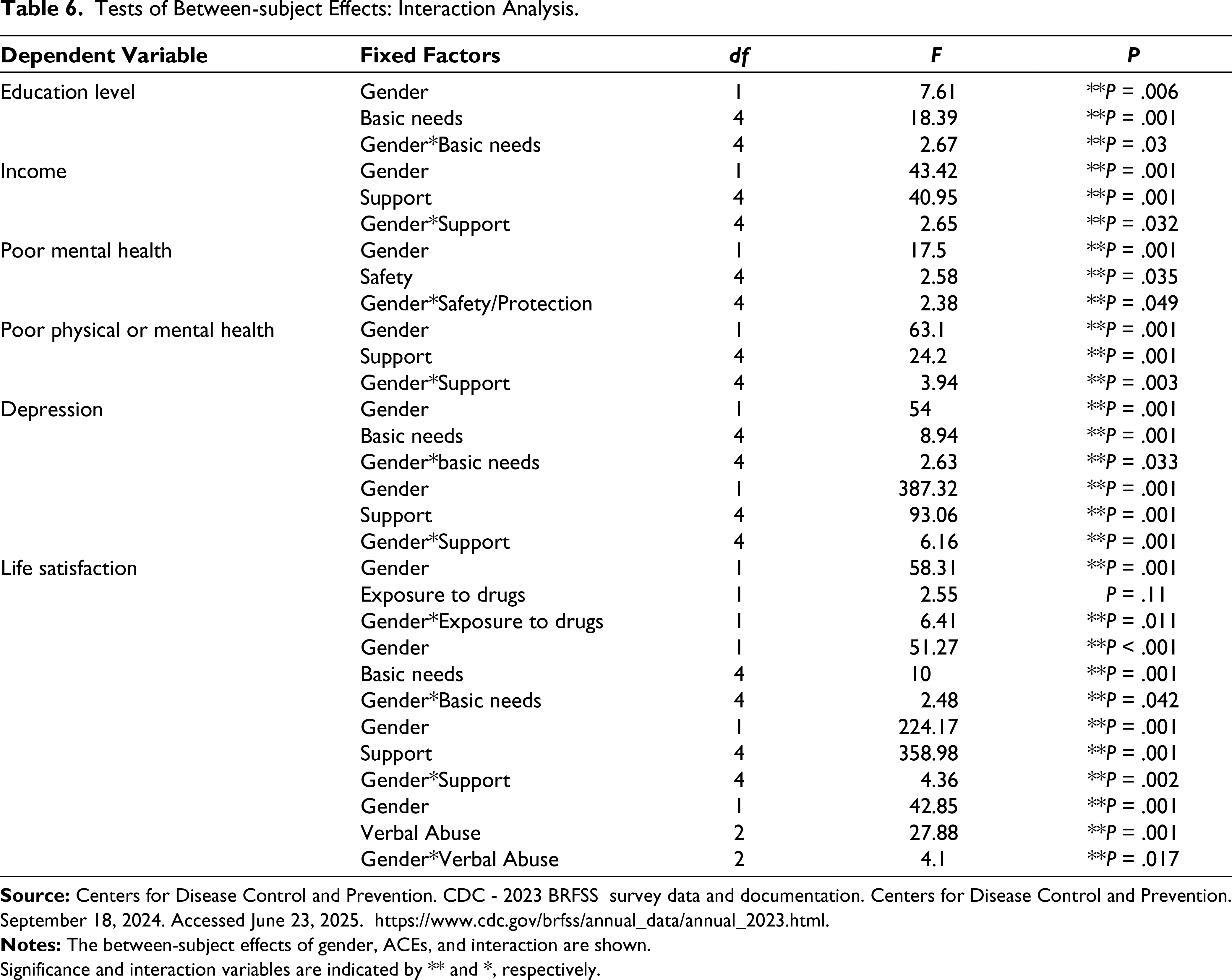
Significance and interaction variables are indicated by ** and *, respectively.
Linear Regression Pairwise Comparisons for Gender, ACEs, and Life Outcomes.
Education & Income
Analysis revealed a significant interaction, F(4, 34,494) = 2.669, P = .030, R² = 0.025 between gender and basic needs for education level. Levels of education generally increased for both groups as their basic needs were met from “never” to “all of the time,” with cisgender individuals reporting higher mean education levels across all categories. A significant interaction was also found, F(4, 149,489) = 2.65, P = .032, R² = 0.046, between gender and support for income. As support increased, income levels also increased for both groups, with the cisgender sample reporting a higher mean income for all levels of support, particularly for those who “usually” received support. Figure 2 shows the interaction between gender and support for income level.
Mental Health
A significant interaction was found between gender and safety/protection with mental health, F(4, 13,078) = 2.380, P = .049, R² = 0.024. Transgender individuals reported more bad mental health days on average across all levels of safety/protection compared to cisgender individuals.
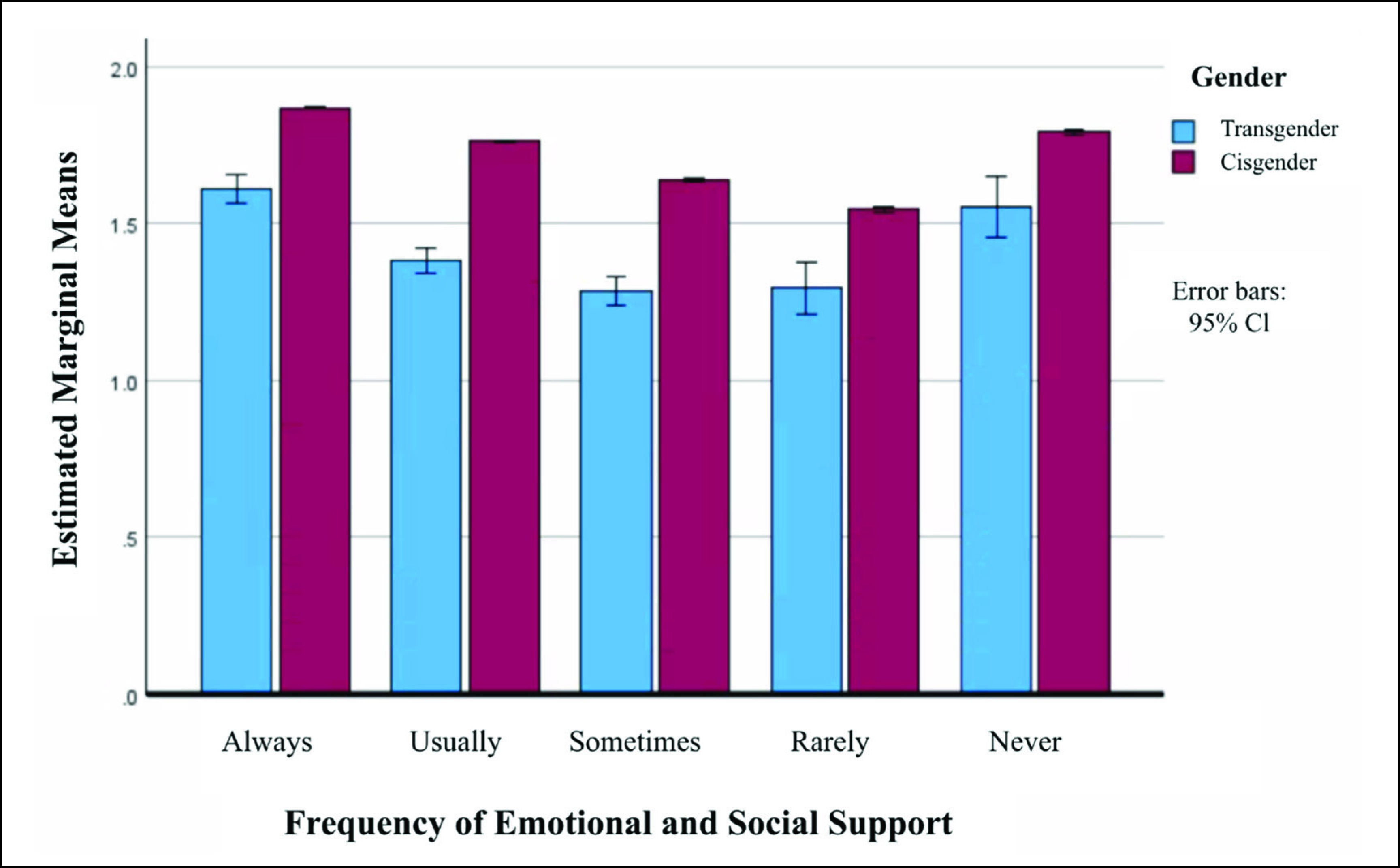
Significant interactions were found between gender, support F(4, 179,407) = 6.158, P < .001, R² = 0.056, and basic needs F(4, 34,413) = 2.628, P = .033, R² = 0.024 with depression. Transgender individuals were more likely to be told they had a depressive disorder across all levels of support and basic needs. However, both groups reported less depression as they received more emotional and social support, with the exception of “never” receiving support, as captured in Figure 3.
Life Satisfaction
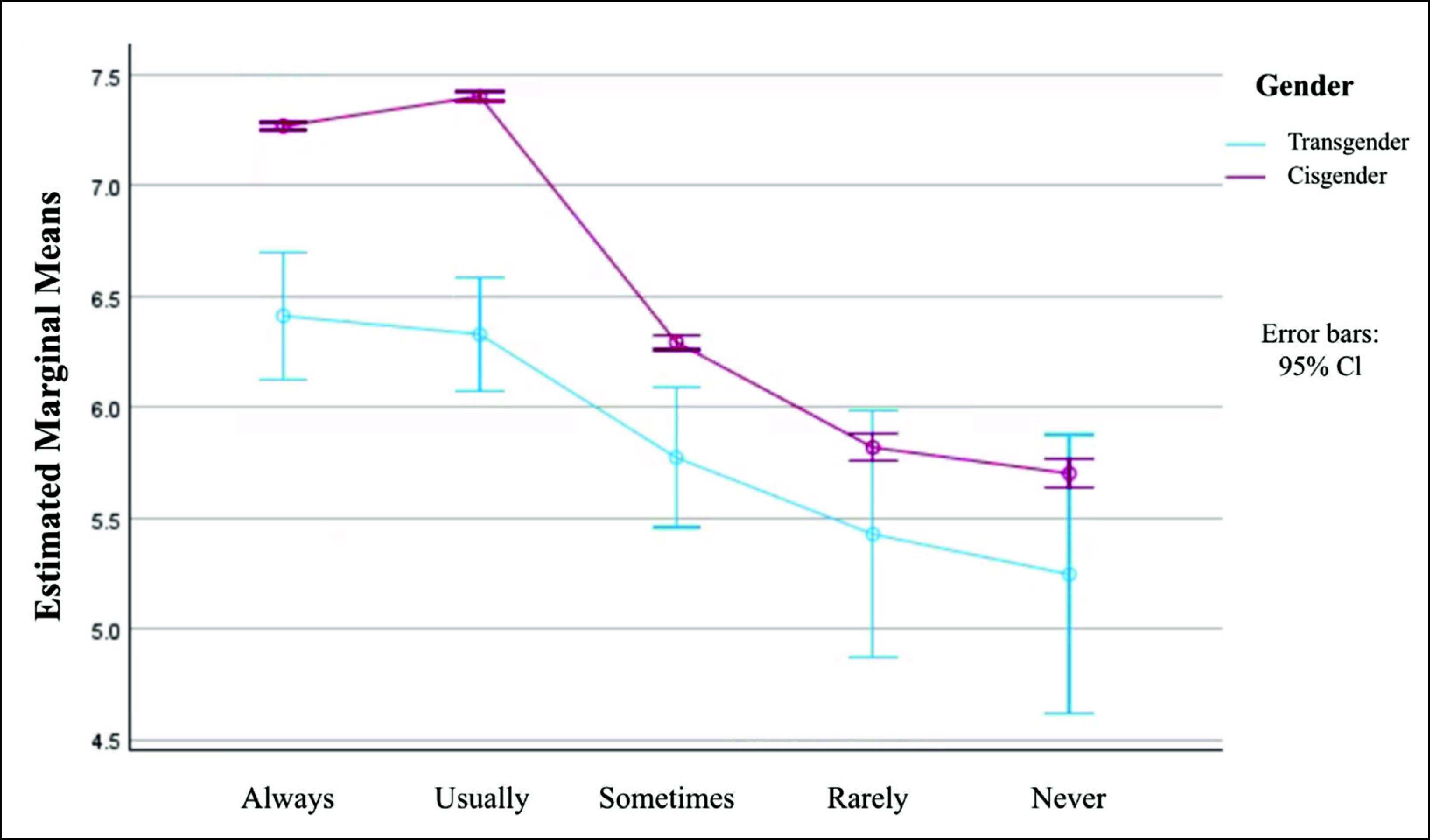
Significant interactions were found between gender, exposure to illegal drugs F(1, 34,108) = 6.412, P = .011, R² = 0.018, having basic needs met F(4, 34,068) = 2.482, P = .042; R² = 0.029, social and emotional support F(4, 178,863) = 4.359, P = .002 R² = 0.188, and verbal abuse F(2, 33,622) = 4.104, P = .017, R² = 0.041 with life satisfaction. Transgender individuals reported lower life satisfaction across all categories of these ACE variables. Within both groups, life satisfaction increases with more support, except for those who “rarely” receive support and as the frequency of verbal abuse decreases.
Qualitative Phase
Qualitative Research Design
Aim 3 within the qualitative phase was designed to explore experiences related to individuals’ gender identity that can be used to inform approaches to provide more effective support for transgender individuals.
Common Themes
Analysis of data obtained from transgender interviews yielded five themes that were common to the experiences of transgender individuals.
The Impact of Family Dysfunction
Body Discomfort Before and After Transitioning
Relatedness and Belonging
Importance of Social Support
Community and Healthcare Dilemmas
Theme 1: The Impact of Family Dysfunction
A total of 81% of participants described their childhood as dysfunctional by characterizing their caregivers as neglectful, unresponsive, combative, or abusive. Moreover, many participants reported not receiving adequate support and stability from their families during childhood and adolescence. The following quote illustrates the participants’ family dynamics:
I had a pretty tumultuous childhood, on paper. Everything was pretty stable, but emotionally, I had a very volatile mother and a very absent father, and they were frequently fighting.
Sub-theme: Fear of Family Rejection and Harassment
The majority of participants felt unsafe exploring or sharing their identities with their families for fear of pushback, harassment, and punishment. As a result, they experienced guilt, struggled to accept their identities, and tried to deny or hide it from family members, as captured in the following quote:
The environment that I’m in, it’s not really safe for me to question it, so I just had to kind of deal with it … Oh, something’s not right here, but I don’t want to question it because it’s not safe for me to question it.
Individuals raised in conservative communities discussed their experiences with harassment and tension created by conservative family members. Several participants reported that family members pathologized their identity by labeling them as mentally ill. Others were told that their identity was a phase or that they were delusional and confused. These family reactions had a negative impact on participants’ mental health, as shown in the following quote.
So family, like, I said, they’re not that supportive … part of my family, and including my dad are … kind of ignoring it…. My oldest brother … has told me explicitly to my face before that, Oh, you have a disease.… And one day, you’re gonna change and get out of this.
Theme 2: Body Discomfort Before and After Transitioning
Participants described discomfort with their bodies from a young age and reported feeling constrained by gender stereotypes, which limited their ability to explore different identities. 86% of participants described intense negative feelings regarding their bodies and struggled to identify themselves when looking in the mirror, as one participant explained, “I experienced a lot of discomfort and a lot of self-hatred … it was really difficult to express myself in a way that felt comfortable.” Many individuals believed these feelings of incongruence were not normal and tried to suppress them.
Despite discomfort with their bodies, many participants reported improvements in their mental health after transitioning socially and/or medically. Some expressed feeling alive and free after their transition, as one participant noted, “Since I’ve started medically transitioning, I do feel a bit more alive … I feel less dull … I’ve always hated my body, and I know that’s a harsh term, but it’s made me nauseous.”
Additionally, participants reported increased confidence, self-acceptance, and self-recognition after transitioning. Many felt more secure in their identity and expressed feelings of hope and optimism as their outward appearance better aligned with their internal sense of self.
Theme 3: Relatedness and Belonging
Relatedness and belonging were especially important for improving participants’ mental health. Forming connections with other transgender individuals helped alleviate feelings of loneliness and provided participants with a sense of belonging as they could relate to others’ experiences. This theme was recognized by the participants, who stated the following:
A big part of my mental health being better is just having those spaces where I’m not made to feel like I don’t belong where I’m not … told to hate myself and to be someone else, and to put on this mask.
Growing up and understanding people like me exist, understanding people like me want to help me understand they’re there for me has been like an integral part of sticking with being trans.
Theme 4: Importance of Social Support
All participants identified social support as a key factor in improving their mental health. Support for their identity helped build their confidence and contributed to greater self-acceptance. Participants primarily received support from their friends, with whom they felt more secure sharing their experiences. Participants described the impact of their friends’ support in the quote below:
I think if I didn’t have them I would be in that fearful state forever … I have these times when I’m with the people who accepted me and I could feel normal. I could feel good. I could feel like a human and not constantly always be on edge.
Conversely, many participants reported having family members who were unsupportive and unaccepting of their gender, which negatively impacted their mental health, as one participant described, “My family is really rough.… Their opinions on trans people have really negatively affected me. Thinking about my future is really scary because there’s a big possibility they won’t be in it.”
Theme 5: Community and Healthcare Dilemmas
Several participants emphasized the importance of education and acceptance of transgender individuals within society and the healthcare arena. They believed that accurate information and education should be made accessible to transgender individuals seeking care and to society to reduce the spread of misinformation about the transgender community. Many participants raised concerns about the anti-trans movement and hatred toward the LGBTQ+ community, which they believed stemmed from misinformation and ignorance, as illustrated in the quotes below.
I’m trying to fight against the idea that trans people are dangerous.… Because once you get rid of that fear, I think it’s a lot easier to talk about the facts, and how to help people. But I think fighting against the fear of and the hatred of trans people … would really help a lot of people.
I think … social movements paint trans people as evil, which I think is the biggest thing standing in the way of trans people being able to access medical treatment easily or be able to fit in socially easily … I think … it’s kind of an information issue.
Sub-theme: Barriers to Care
Regarding the healthcare system, participants discussed challenges with treatment accessibility, affordability, and poor trans-medical education. Participants described poor trans-medical care and barriers to healthcare, noting “Having education classes about how to interact with pronouns other than he/him and she/her is really necessary,” and “I have to make pleas to licensed therapists or psychiatrists, to write me letters of support, to be able to then pursue the care I need.… It gatekeeps a lot of really important care.”
Discussion
This study triangulated quantitative and qualitative data to explore the experiences of transgender individuals. The findings emphasize the critical role of family functioning, support networks, societal acceptance, and access to care in fostering positive life outcomes and offer implications for healthcare and policy.
The transgender individuals reported significantly more ACEs, including abuse, neglect, lack of support and safety/protection, parental divorce/separation, exposure to mental illness and substances, and household incarceration, in comparison to cisgender individuals. Furthermore, transgender individuals experienced significantly worse life outcomes, including lower income, fewer years of education, higher levels of loneliness, poorer mental health, and lower life satisfaction, and were significantly less likely to be married. These findings align with previous research studies on the transgender community that identified greater economic instability, adverse health outcomes, experiences of violence and discrimination, and limited access to transgender healthcare.10,26 Interaction analyses revealed that several childhood variables interacted with gender identity to produce significantly different life outcomes between groups. Specifically, transgender individuals were disproportionately affected by these ACEs, resulting in worse life outcomes in income, education, mental health, and life satisfaction, supporting the first hypothesis. In summary, the quantitative analysis revealed significantly higher rates of ACEs and poor life outcomes within transgender individuals, who were disproportionately affected by these early experiences.
Five central themes emerged from the analysis of participant experiences. The first theme focused on family dysfunction, which was commonly reported during childhood and adolescence. Participants in the study who felt unsupported by their caregivers often concealed their gender identities and self-isolated, which exacerbated their mental health struggles. 27 The second theme involved body discomfort and the effects of transitioning. From an early age, participants identified an incongruence between their physical appearance and internal sense of self, which many initially believed was abnormal and attempted to suppress. As a result, they developed strong negative feelings toward their body and felt distress during puberty. Although transitioning brought both positive and negative emotions, participants generally reported increased confidence, self-recognition, acceptance, and improved mental health after transitioning. 22
In the third theme, relatedness and belonging, several participants felt unsafe exploring their identity at home and turned to the internet and external social groups to learn more about gender. Prior to these connections, participants expressed feelings of loneliness and isolation; however, the internet afforded them the ability to find individuals who accepted and validated their identity, which improved their confidence and mental health. 28 The fourth theme, social support, had a positive impact on participants’ mental health as they felt accepted and comfortable in their identity, lending to a sense of normalcy.
The fifth theme identified dilemmas within the community and the healthcare system. Participants expressed the need for increased education and awareness for the transgender community to combat misinformation and reduce stigmatization. Understanding the lived experiences of transgender individuals is critical for informing policymakers of the potential legislative effects on the transgender community. Barriers to care, such as accessibility, affordability, and negative encounters with healthcare professionals, discouraged participants from seeking care, raising concerns for health status among the transgender community. 18 Medical school curricula would benefit by integrating holistic approaches that account for trans-specific needs to better equip doctors to provide high-quality care to transgender patients.19,20
Integration of the Findings
Integration revealed the importance of strong family cohesion, social support, and acceptance in the promotion of positive outcomes for transgender individuals. Acceptance and validation from family, peers, school, and work were linked to greater self-confidence, self-acceptance, and a stronger sense of belonging. Given these findings, it is important to focus on the role of different social groups within the transgender community. Moreover, experiences of minority stress, such as discrimination, harassment, and stigmatization, uniquely contribute to poor outcomes. These distinctive experiences help explain the outcome disparities between transgender and cisgender populations. Having a positive self-outlook, supportive relationships, and family understanding are critical in promoting resilience and success in transgender individuals. Therefore, caregivers, educators, policymakers, healthcare professionals, and the broader public should gain a deeper understanding of transgender experiences to reduce gender discrimination and social inequities. Additionally, multilevel interventions are needed to target family relationships and transgender youth, increase training for healthcare providers, and guarantee equal protection under the law within the transgender community.
Strengths
The explanatory mixed methodology allowed researchers to examine the interactions between early experiences, gender identity, and life outcomes, providing deeper insight into the underlying mechanisms behind these interactions. Threats to external validity were reduced by using participant data across the United States to perform the quantitative data analysis. The sample size and diversity of respondents from the BRFSS survey improved generalizability to the population. Similarly, the sample size of the qualitative component was sufficient to reach data saturation. Threats to validity and reliability were accounted for in the qualitative component by sharing the results with participants to ensure findings accurately reflect their experiences. Moreover, inter-rater reliability was conducted for 20% of the interview transcripts to ensure consistency with codes and themes for the thematic analysis and helped mitigate potential researcher bias.24,25
Limitations
The authors are based in Western academic institutions and identify as cisgender, which may limit insight into the nuanced lived experiences of transgender individuals. The quantitative component involved a cross-sectional and correlational design that limits the ability to determine causal relationships between variables. While it was hypothesized that ACEs and gender identity influence later life outcomes, further research is needed on the direction and magnitude of these effects. However, ACEs and life outcomes were adjusted for covariates to account for potential confounding variables and improve the accuracy of findings.
Another limitation is the use of open data, which prevented researchers from following up with respondents who were missing data from the BRFSS survey. As such, respondents may have interpreted questions differently or chosen not to answer, which limits representation. Convenience sampling for the quantitative and qualitative portions may have increased the likelihood of selection bias. For the qualitative component, participant recruitment was primarily done on the University of Michigan campus, which may have skewed the sample toward younger, college-educated participants. The majority were White/Caucasian and college-educated, which may limit the applicability of the findings to transgender individuals from racially diverse or economically marginalized backgrounds. Future research could include more racially, geographically, and economically diverse samples to better understand the impact of these factors on transgender individuals’ experiences.
Summary
Given the social inequities within the transgender community, exploring the experiences of transgender individuals from childhood through adulthood is instrumental in identifying factors relating to positive life outcomes. The findings underscore the importance of family functioning, support networks, societal acceptance, and access to care in promoting positive life outcomes in adulthood. Moreover, the research discerned factors to improve community acceptance and transgender healthcare, including increased education among the public and healthcare systems on transgender experiences. Additional research on this topic is warranted to examine the perspectives of family members, friends, school faculty, and healthcare professionals to gain a more holistic view of factors influencing transgender individuals’ experiences and life outcomes.
Footnotes
Acknowledgements
LB and NB participated in planning the study and revising the article. All authors contributed to the article and approved the submitted version.
Data Availability Statement
Datasets analyzed during the current study are available in the [Centers for Disease Control and Prevention (CDC) BRFSS repository] [
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The studies involving human participants were reviewed and approved by the University of Michigan Health Sciences and Behavioral Sciences Institutional Review Board (IRB-HSBS; HUM00000246).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded through the Tanner Memorial Award and Senior Honors Research Funding Award by the Department of Psychology at the University of Michigan.
Informed Consent
The participants provided their written informed consent to participate in this study.