
Abstract
Background:
Dhat syndrome, a culture-bound condition related to anxiety and somatic complaints due to perceived semen loss, is rarely studied in relation to depression.
Objective:
To determine the prevalence of dhat syndrome in young men with depressive disorders and compare those with and without dhat syndrome, along with their socio-demographic and clinical correlates.
Methods:
A total of 147 men (18–45 years) with depressive episodes (Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition [DSM-5]) at a government hospital’s psychiatric Out Patient Department (OPD) were assessed for 18 months. Dhat syndrome was diagnosed using perception of semen loss, distress, and attribution of symptoms to semen loss.
Results:
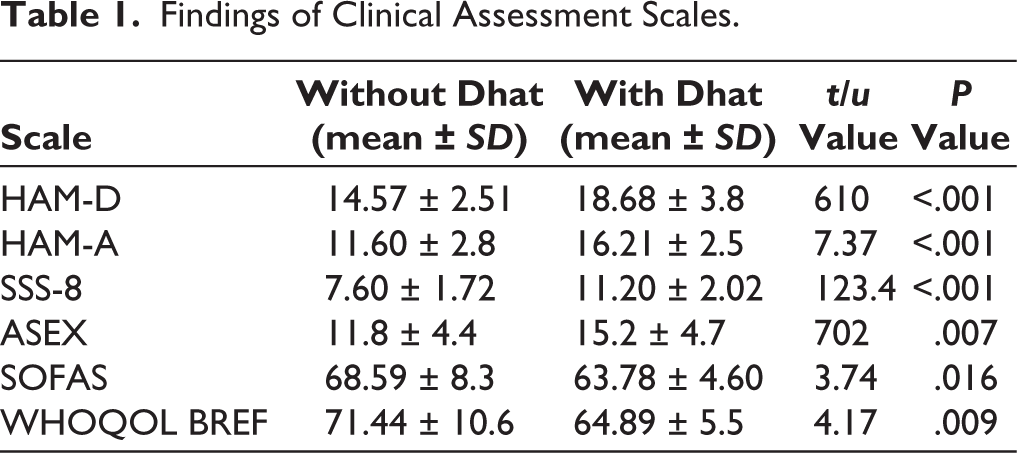
Prevalence was 12.9% (19 of 147). Lower education was significantly associated (P = .023). Those with dhat syndrome had higher Hamilton Depression Rating Scale (HAM-D), Hamilton Anxiety Rating Scale (HAM-A), and Somatic Symptom Scale-8 (SSS-8) scores (P < .001), more sexual dysfunction Arizona Sexual Experiences Scale (ASEX) (P < .05), and poorer Social and Occupational Functioning Assessment Scale (SOFAS) and World Health Organization Quality of Life (WHOQOL) scores (P < .05).
Conclusion:
Dhat syndrome magnifies psychological, somatic, and sexual burden in depressed men, especially the less educated.
Introduction
Dhat syndrome, originally reported by Malhotra, 1 is characterized by the emergence of somatic and psychological symptoms due to the perceived loss of semen. The belief that semen is a vital fluid and its loss has disastrous consequences is rooted in the traditional Indian school of thought. The condition has been found to be most common among rural and socioeconomically modest young men.
Dhat syndrome is a syndrome of somatic and psychological symptoms ascribed to semen loss, based on Ayurvedic and folk conceptions that semen (“shukra”) is the life fluid of the body. It has areas of overlap with established psychiatric illnesses, specifically depression. 2 The patients have fatigue, anxiety, sexual dysfunction, and somatic symptoms that they associate with the loss of semen. Even with improvements in socioeconomic and educational status, these conceptions continue, especially in young, less educated men, and commonly co-occur with depressive and anxiety disorders.
Empirical evidence testing this condition in the context of clinical depression is minimal. This study seeks to explore the prevalence and clinical associations of dhat syndrome in young men with depression and close the knowledge gap. Previous research has reported its clinical presentation and comorbidities, 2 but there have been few systematic investigations of its prevalence and effects in the depressed population. This work addresses this deficit by measuring the prevalence of dhat syndrome among patients with depression and investigating its demographic and clinical correlates.
Methodology
This cross-sectional, observational study was carried out for 18 months in the Outpatient Department of Psychiatry at King George’s Medical University, Lucknow, India. Purposive sampling was used to recruit 147 male patients in this study. The first five patients with depression, visiting the hospital on each Out Patient Department (OPD) day, were included in the current study. The inclusion criteria were: Male gender, aged between 18 and 45 years, a diagnosis of depression based on Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria, a lack of psychotropic medication for at least one month before participating, and the possibility and willingness to provide written informed consent. Patients were excluded if they had psychotic symptoms or suicidal thoughts, bipolar depression or other comorbid psychiatric conditions (with the exception of tobacco use disorder), sexually transmitted infections, genital discharge of organic etiology, or severe medical or surgical illness.
Dhat syndrome in this study was operationalized using the following criteria: (a) Perceived semen loss, through urine or nocturnal emissions; (b) psychological distress associated with semen loss; and (c) attribution of physical or psychological symptoms to the perceived semen loss.
All participants were evaluated using a battery of standardized instruments. A structured socio-demographic and clinical proforma was created to document personal, clinical, and illness-related information. The diagnosis of depression was established by DSM-5 criteria. The severity of depressive symptoms was measured by the 17-item Hamilton Depression Rating Scale (HAM-D), and the level of anxiety was measured by the 14-item Hamilton Anxiety Rating Scale (HAM-A). The Somatic Symptom Scale-8 (SSS-8) was used to measure the burden of somatic symptoms, and sexual dysfunction was measured using the Arizona Sexual Experiences Scale (ASEX). Social and occupational functioning was evaluated using the Social and Occupational Functioning Assessment Scale (SOFAS), and quality of life (QOL) was assessed on four domains, physical health, psychological health, social relationships, and environmental well-being, using the World Health Organization Quality of Life-BREF (or Brief) version (WHOQOL BREF).
Procedure and Data Analysis
The study was approved by the Institutional Review Board (XX-PGTSC-IIA/P31). Those fulfilling the inclusion criteria were debriefed about the study, and written informed consent was taken from the selected participants. Each participant then went through a structured clinical interview. This was followed by a battery of standardized assessment instruments being applied. All the collected data was anonymized to protect confidentiality and then transferred to a secure database for statistical analysis. Analysis of the data was conducted with the Statistical Package for the Social Sciences computer program. Descriptive statistics were employed to describe socio-demographic and clinical characteristics. Comparative analysis was undertaken to investigate differences between participants with and without dhat syndrome.
Results
A total of 176 patients were screened, out of which 147 male participants met the inclusion criteria. Among them, 19 patients with depression have been identified as having dhat syndrome. The prevalence of dhat syndrome in this patient group is 12.92%, indicating that a notable proportion of patients with depression are also experiencing dhat syndrome.
Most of the participants were in the 26–35 years age group (35.4%), 33.3% were in the 18–25 years age group, while 31.3% were in the 36–45 years age group. The majority of the patients were from rural (63.9%) and nuclear family (63.3%) backgrounds. Almost half the patients were unmarried (51.7%), and only 1.4% were divorced. With regard to education, 41.5% of participants were graduates and above, while 31.3% had been educated up to the 12th grade. With regard to work, 47.6% were unemployed, and 30.6% were students.
The duration of illness for depression distribution shows that 48.3% of patients had been ill for less than 6 months, followed by 36.7% who had been experiencing illness from 6 months to 1 year, and 15.0% had been ill for more than 1 year. The onset of illness for depression shows that the largest group of patients, 34.7%, experienced the onset of depression at or before the age of 25 years. This was followed by patients with onset between 26 and 30 years (18.4%) and 31 and 35 years (15.0%). Additionally, 15.6% had their depression onset between 36 and 40 years, and 16.3% experienced it between 41 and 45 years.
The mean age of patients with dhat syndrome was 29.58 years (SD = 9.3), while those without dhat syndrome had a mean age of 31.05 years (SD = 8.6), with no significant difference between the groups (t = 0.677, P = .493). A significantly larger proportion of patients with dhat syndrome (52.6%) had education up to the 10th standard or below compared to those without dhat syndrome (23.4%) (χ² = 7.55, P = .023). Marital status and domicile did not differ significantly between the groups. Among patients with dhat syndrome, 52.6% were married compared with 46.1% of those without (χ² = 0.53, P = .768), and 63.2% of patients with dhat syndrome lived in rural areas compared with 64.1% of those without (χ² = 0.006, P = .939). Although a greater proportion of patients with dhat syndrome (73.7%) reported a monthly income between ₹10,000 and ₹30,000 compared to 52.3% among those without dhat syndrome, this difference was not statistically significant (χ² = 3.79, P = .150). Between the two groups, no variation was found for age, marital status, residence, or monthly income. While the clinical scale scores are reported in Table 1.
Findings of Clinical Assessment Scales.
Discussion
Dhat syndrome is a culture-bound disorder that is most commonly reported in South Asia, specifically India. 3 It is characterized by anxiety over semen loss and is combined with weakness, fatigue, somatic complaints, and sexual dysfunction. 4 The present study contributes to the literature by exploring the incidence and clinical influence of dhat syndrome in patients already diagnosed with depressive disorder.
This study found that 12.92% of young male patients diagnosed with depression also met the operationalized criteria for dhat syndrome, indicating that a considerable proportion of depressed patients also experience distress related to semen loss. This supports earlier findings by Strong et al., who reported that depression is the most common psychiatric comorbidity in patients with dhat syndrome and is present in 40%–66% of cases. 2 The presence of both conditions together reflects how psychological distress in the form of depression may be culturally expressed through somatic concerns, such as semen loss. 5
The average age in the dhat group was 29.58 years, suggesting that dhat syndrome commonly affects young adults. 6 These findings are consistent with the cultural context where young males often have limited access to scientific sexual health information, increasing their vulnerability to myths and anxieties about semen loss. 7 In terms of domicile (rural vs. urban), education level, marital status, and family income, no statistically significant differences were observed between the dhat and non-dhat groups. This is particularly important because earlier studies suggested that dhat syndrome was more common among individuals from rural areas and lower-income backgrounds.8,9 Newer research suggests that dhat is not just prevalent in the rural areas of the country. 10 This could be attributed to the widespread rural-to-urban migration, as well as cultural beliefs across both urban and rural populations, and the increasing exposure to misinformation via the internet and social media.
The relationship between lower education and dhat syndrome was statistically significant, reinforcing earlier findings attributing restricted exposure to education as a cause of heightened susceptibility to sexual myths and culture-bound syndromes. 11 Individuals with primary or lower-secondary level education might be deprived of sufficient knowledge of reproductive physiology and, therefore, susceptible to false ideas about semen loss and its claimed health implications. 12 In contrast, more advanced educational levels appear to offer some protection, probably as a result of improved health literacy and exposure to reliable information. 13 While no strong associations were found with marital status, religion, family structure, or residential location, the dhat group had a greater percentage of unmarried persons and nuclear family households, perhaps indicative of reduced familial and spousal support, increased pre-marital anxiety, or a conservative attitude toward sex. 14 Also, the somewhat greater prevalence in rural areas can be explained by the more entrenched traditional health beliefs there, although urban populations are not exempt from these issues. This supports the contention that dhat syndrome is based more on cultural expectations than on geographical or religious affiliations. 2
From a clinical point of view, dhat syndrome patients showed significantly greater depression and anxiety, as quantified by HAM-D and HAM-A scores, respectively. This corroborates previous research that suggested greater emotional distress, including guilt and suicidal thoughts, among dhat syndrome patients. 15 Sleep disturbances, specifically early insomnia, were also more common, indicating a ruminative and hyper-aroused psychological state that is typical of somatoform and anxiety disorders. Somatic symptom burden was high in the dhat group. 16 Patients complained of back pain, gastrointestinal distress, headache, and tiredness on a regular basis. These results are consistent with the prior literature, indicating that somatization is at the core of the dhat syndrome construct and might mask the underlying psychiatric illness. 17 These somatic complaints tend to first make patients seek care from nonconventional medical systems such as homeopathy, Unani, or Ayurveda, and this contributes to a delay in psychiatric consultation. 11
Sexual dysfunction was significantly more pronounced in dhat syndrome patients, as indicated by ASEX, covering reduced libido, difficulty with arousal, erectile dysfunction, and low satisfaction. 18 Previous research has identified similar trends, with participants blaming general weakness, tiredness, and poor sexual performance on semen loss, which worsens performance anxiety and guilt. 16 The perception that semen is an essential fluid whose loss is incapacitating and is responsible for avoidance behaviors and negative self-evaluations of masculinity and virility. 19
Functionally, patients with dhat syndrome scored significantly lower on the SOFAS, reflecting compromised social and occupational functioning. Such impairment can be due to both somatic preoccupation and the psychological effect of sexual guilt and anxiety. 2 The person may isolate themselves from society or underachieve in the workplace due to fear of stigmatization and internalized pain. QOL, as measured by WHOQOL-BREF, was also significantly lower in patients with dhat syndrome on various domains such as physical health, psychological, and social relationships. Previous research also suggests that dhat syndrome patients have lower general well-being and have tremendous difficulty in having functional relationships. 20 The present findings reaffirm that the distress among these individuals goes beyond the psychological to involve fundamental life areas, causing their subjective QOL to be seriously affected.
Dhat syndrome is a culturally influenced, yet clinically significant, form of somatization and sexual health anxiety that amplifies the load of depressive illness. Although it is omitted from formal diagnostic criteria, its significant impact on mental health, sexual function, social roles, and QOL requires greater public health and clinical consideration. Early detection, culturally sensitive psychotherapeutic interventions, and multi-faceted public education are needed to reduce the effects of dhat syndrome and ensure holistic mental healthcare.
Limitations
The research was conducted in a single tertiary care center, because of which the findings may not be generalizable to other settings, especially in rural or primary care settings. The data was collected using self-report and interviewer-administered scales, which may make the data vulnerable to social desirability or reporting bias, especially on sensitive issues such as sexual functioning. Additionally, the relatively small sample of dhat syndrome patients could restrict the statistical power available for subgroup analyses.
Directions for Future Research
The clinical characteristics of depressed patients with comorbid dhat syndrome are highlighted in the current study. There is a dire need for culturally sensitive diagnostic and treatment approaches to be designed and standardized for the management of these symptoms. Future studies should use longitudinal designs to explore causal relationships and investigate other comorbid or extraneous variables that may play a role in the manifestation of dhat-like symptoms in people diagnosed with depression.
Conclusion
In conclusion, dhat syndrome markedly worsens the clinical picture of depression in young men, adding to increased psychological distress, burden of somatic symptoms, sexual dysfunction, and functional impairment. Its close linkage with decreased educational status emphasizes the importance of poor sexual literacy and culturally determined misconceptions in the illness behavior. Although it is highly embedded in cultural beliefs, dhat syndrome has real psychiatric implications that require clinical consideration.
Successful management of the condition demands an approach that includes culturally sensitive assessment, focused psychoeducation, and evidence-based psychotherapeutic intervention. Early detection and destigmatization are imperative to enhance help-seeking behavior and clinical outcomes. Longitudinal studies should be the focus of future research to study the course of dhat syndrome and to evaluate the effectiveness of individualized interventions. Moreover, there is an urgent need for the integration of culture-bound syndromes into medical education and public health policy to raise awareness and provide comprehensive, context-sensitive mental health care.
Footnotes
Authors’ Contribution
AND contributed toward initial ideation. AND and PJ contributed to data collection and study conduction, AT, BG, and SSK contributed to study supervision and guidance. All authors contributed to the writing of the first and final drafts.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Institutional Ethics Committee of King George’s.
Medical University, U.P., Lucknow, on 16/09/2023 Ref. code – XX-PGTSC-IIA/P31.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
All participants provided written informed consent prior to participating.
Statement
The manuscript has been read and approved by all the authors, the requirements for authorship have been met, and each author believes that the manuscript represents honest work.