
Abstract
Every day, people struggle with mental health challenges; one in five people will experience a mental illness in their lifetime. Innovative approaches to strengthen the public mental health strategy warrant careful deliberation. This article reintroduces and explores the conceptual framework of mental hygiene. The concept of mental hygiene was originally introduced in the early 20th century, with the aim of preventing and treating mental illness and milder mental disorders. The movement lost its momentum shortly thereafter and the concept went largely ignored since then. Mental hygiene is a form of preventive maintenance that can be likened to other hygienic practices. Through the plasticity of the brain, mental training activities can foster healthy cognitive patterns that are conducive to well-being. The article offers a brief overview of some of the mental hygiene practices one can engage in, on a daily basis, to support well-being and assist in preventing mental health issues. Such mental training behaviors may potentially reduce ubiquitous human tendencies to ruminate and mind-wander without awareness, which when in excess correlate with increased activity of the default mode network and susceptibility to the pathogenesis of mental illness, along with impeding human flourishing. The article advocates for the routine engagement in healthy mental hygiene to become a global recommendation.
In 1922, the National Council for Mental Hygiene (NCMH) was established in hopes of preventing and treating mental illness and milder mental disorders (NCMH, 1930). It was seen as a valuable movement that aimed to rectify the social problem of mental illness in the community. Although supported by various experts in psychology, World War II (WWII) changed the landscape of how mental disorders were perceived. Mental illness was framed as a detriment to society and threatened the well-being of healthy people. During the war, it was alluded that entire nations were capable of exhibiting symptoms of mental illness (Toms, 2010), making them dangerous and threatening. Post war, the mental hygiene movement lost its momentum. A few decades later, the assessment and treatment of mental illness became commonplace, with its impetus stemming from new research into mental disorders (Toms, 2010) and the deinstitutionalization movement of the 1950s and 1960s (Rodrigues et al., 2016).
Although the concept of mental wellness is anything but novel, there has been a deficit in attention given to the idea of mental hygiene, especially after WWII. Alarmingly, one in five Canadians will experience mental illness in their lifetime, most commonly anxiety disorders and depression (Canadian Mental Health Association [CMHA], 2017). Mental illness is the single most disabling group of disorders for youth worldwide, and is one of the most substantial costs to Canada, with an estimated Can $50 billion a year (Mental Health Commission of Canada [MHCC], 2012), being spent on health care costs, lost productivity, and reductions in health-related quality of life (Smetanin et al., 2012). Reinstating the mental hygiene movement may in fact aid in alleviating some of these systemic burdens.
In recent years, various organizations such as the MHCC have helped lay the groundwork for substantial changes to the way Canadians think and deal with mental illness. Its 2012 report, Changing Direction, Changing Lives: The Mental Health Strategy for Canada, proposes concrete steps for various stakeholders to implement structural changes related to the multidimensional factors (e.g., determinants of health, [de]stigmatization, access to mental health care) that foster mental health. This report also reflects the goals that were outlined by the original mental hygiene movement founded by Adolph Meyer in the early 20th century (March & Oppenheimer, 2014). In addition to their aim of fostering healthy ways of living, this movement sought to improve socioeconomic factors that affect and contribute to mental illness (March & Oppenheimer, 2014).
Concept of Mental Hygiene
Hygiene can be defined as a science of the establishment and maintenance of health or as conditions or practices (as of cleanliness) conducive to health (Hygiene, 2018). Different forms of hygiene have historically been, and currently are, promoted by public health officials and organizations, encouraging individuals to adopt certain daily practices. For example, the Canadian Dental Association (CDA, 2018) recommends brushing twice daily, for a minimum of 2 min each time, to prevent gingival disease and to encourage oral health-promoting behaviors. Similarly, the Sleep Foundation (2021) recommends 7 to 9 hr of sleep per night for the average adult, along with the avoidance of nicotine, alcohol, or caffeine prior to bedtime as part of sleep hygiene. The Heart and Stroke Foundation of Canada (2017), as well as the World Health Organization (WHO, 2017), recommends 150 min per week of moderate to vigorous physical activity (PA) to promote cardiovascular hygiene. Hand hygiene recommendations have also been instrumental in reducing communicable diseases (WHO, 2009).
Currently, there is no equivalent recommendation vis-à-vis mental health. The CMHA (2016) has commented, “Mental health is key to our well-being. We can’t be truly healthy without it. It involves how we feel, think, act, and interact with the world around us” (p. 1). In light of this reality, the general population faces limited guidance in fostering healthy cognitive patterns and in avoiding maladaptive habits of thought. Most recommendations given to promote mental health for the individual include PA, good sleep hygiene, a balanced diet, and maintaining healthy social relationships (Government of Canada, 2016). These recommendations are not to be underestimated in their importance; however, there is little attention given to the myriad of evidence that suggests how, through the plasticity of the brain, individuals can train themselves to foster healthy cognitive patterns that contribute to mental well-being (Ramirez-Barrantes et al., 2019).
Mental Hygiene for Mental Well-Being
Cognitive training activities, such as meditation and contemplative practices, have met resistance in being accepted as widespread recommendations for healthy mental hygiene (Van Dam et al., 2018). Some suggest these challenges have been related to terminological roadblocks (Dorjee, 2016). A clear consensus as to how to define such cognitive practices has been difficult to obtain, especially given the highly complex and much nuanced nature of the human brain. Nonetheless, many other approaches to training the mind exist, such as positive psychological interventions (PPIs), cognitive-behavioral therapy (CBT) exercises, and positive journaling, all of which have been documented to support mental well-being (Boiler et al., 2013; Porto et al., 2009; Smyth et al., 2018).
This article seeks to reintroduce the conceptual framework of mental hygiene, in which we explore the benefits of regularly engaging in mental training that facilitates psychological well-being. There has been significant progress in encouraging the public to maintain healthy personal, dental, and sleep hygiene as well as engaging in regular PA. The conceptual foundation of encouraging individuals to deliberately and intentionally tend to their minds on a routine basis, just as they would with any other hygienic practice, to facilitate mental well-being will be explored.
Building the Mental Hygiene Framework
Important to the mental hygiene framework is an understanding of its relationship to the two-factor model (TFM) of mental health. The TFM disputes viewing mental health as a single bipolar dimension in which mental health, essentially, on one end of the spectrum, is simply an absence of mental illness (Keyes, 2005). Rather, it proposes two correlated unipolar dimensions, one along the continuum of mental illness and psychopathology, and one along the continuum of mental health (Keyes, 2005). The optimal end of the continuum of mental health has been referred to with various terminologies such as flourishing, positive or complete mental health, subjective well-being, and happiness (Keyes, 2002). Thus, the absence of mental illness does not necessarily indicate mental health.
Important to the discussion of mental health promotion, the TFM highlights that disease prevention on its own is an incomplete strategy but rather needs to be inclusive of approaches that encourage and nurture human flourishing and well-being, which themselves serve as a highly protective factor to mental illness (Keyes et al., 2010). The theoretical foundation of the mental hygiene framework posits that it can exert influence on both dimensions via potentially malleable aspects of cognition. Consequently, not only can mental hygiene contribute to human flourishing, but it can also play a role in disease prevention and potentially serve as prescriptive behavior in the presence of mental illness. This is a common feature of hygienic practices in general; good sleep hygiene is essential to healthy human functioning. An absence of good sleep hygiene may increase the risk of mental deterioration, and it is likely to be one of various prescribed behaviors when managing individuals with mental health concerns. A similar analogy can be drawn from PA. Regular PA is an important aspect of maintaining physical health but is also considered important in disease prevention as is the case in preventing dyslipidemia and is prescriptive behavior in the presence of an illness such as type 2 diabetes (Booth et al., 2012).
Risk Profile
Although some activities have an inherent level of risk, there is minimal risk when engaging in mental hygiene, once the framework is understood. Studies have shown the many health benefits of physical exercise (Yancy et al., 2007); society collectively understands this and promotes the general population to engage in such behaviors (Makar & Siabrenko, 2018); yet, there are still risks to physical exercise. It has been reported that the relative risk of cardiac arrest during vigorous PA is 56 times greater than any other time of the day for men who do not participate in exercise often, and 5 times greater for men who exercise frequently (Haskell et al., 2007). With all the known benefits of exercise, despite these transient risks, along with the cost and infeasibility of medically screening all individuals prior to engaging in exercise, Haskell et al. (2007) explain how Asymptomatic men and women who plan to be physically active at the minimum levels of moderate-intensity activity set forth in the present recommendation (WHO, 2017) do not need to consult with a physician or health care provider prior to beginning unless they have specific medical questions. (p. 1089)
The same pattern follows in more specific clinical populations. In a study of 4,846 cardiac rehabilitation patients who engaged in aerobic exercise, one fatal cardiac arrest and two nonfatal cardiac arrests occurred (Rognmo et al., 2012). Although there was a fatality in the above-mentioned study, the majority of research on physical exercise reports a low risk associated with aerobic activity. Rognmo et al. (2012) concluded that aerobic activity for cardiac rehabilitation patients is still appropriate and recommended.
A novice in aerobic exercise would be ill-advised to participate in a half marathon as their first PA. Similarly, individuals with minimal meditation experience may find a 5-day silent meditation retreat quite challenging for their mental experience and even perhaps destabilizing (Shapiro, 1992). Conversely, the person who has never participated in any aerobic activity would benefit from a brisk walk for 25 min a day, 6 days a week, thereby meeting the WHO’s recommendation of 150 min per week (WHO, 2017). In parallel, recommending 5 to 10 min of mental training, once a day, such as sitting with your eyes closed and focusing on breathing, comes with minimal risk. Shonin et al. (2014) elucidate this point when they explain that “both the classical meditation literature and empirical research findings appear to concur that when correctly practiced and administered, mindfulness meditation is a safe, non-invasive and cost-effective instrument for improving psychological health” (p. 391).
Hygiene in itself is not an intervention. Many meditation and contemplative practices are studied through a lens of intervention and compared in various trials to placebo, CBT, medications, or exercise (Goyal et al., 2014). The data obtained from these studies are instrumental in widening our perspective on how to approach mental illness and the usefulness of meditation; yet, when meditation is only studied in this context, we are unable to measure its effectiveness as a hygienic practice. Often when an individual has an infected tooth, they require a root canal, a dental intervention performed by a licensed dentist. In this instance, even excellent dental hygiene will be unable to resolve the dental issue. However, regular teeth brushing, as a preventive behavior, reduces the odds of developing a variety of dental disorders (CDA, 2019) and likely is an important practice for one with ideal oral health. This can be likened to practices involving mental hygiene.
When contemplative practices such as meditation are recommended from a hygienic perspective, it is not to imply that it is the best intervention in the presence of mental illness. When one is experiencing anxiety, depressive symptoms, or other psychological challenges, professional help in the form of psychotherapy, counseling, medications, physical exercise, or improving sleep hygiene may all be required to ensure a return to health. Meditation practices may not be sufficient on their own but can still be an appropriate adjunctive approach when viewed from a hygienic perspective. Van Dam et al. (2018) expressed concerns that the public may misinterpret that “meditation interventions can act as a replacement to medication for mental illnesses such as depression and bipolar disorder” (p. 48). Particular hype-filled slogans, such as “meditate, don’t medicate” (Annels et al., 2016), can be misleading in that people may interpret this message as meditative practices being interventional alternatives to medications. Despite promising data on mindfulness-based interventions for a variety of mental health issues and illnesses, Strauss et al. (2014) warn that we would caution against offering mindfulness based interventions (MBIs) as a first line intervention for people experiencing a primary anxiety disorder . . . findings from the current meta-analysis would suggest great caution if offering MBIs to this population as a first line intervention instead of a well-established therapy. (pp. 11–12)
Universality
This framework advocates the ubiquitous applicability of hygienic practices in general rather than a disease-specific approach. For example, evidence suggests that mindfulness and/or positive psychology exercises can be helpful for a wide range of psychopathologies such as anxiety or schizophrenia (Brown et al., 2019; Chien & Thompson, 2014; Hofmann et al., 2010; Kang et al., 2020; Tabak et al., 2015). Personal, dental, and sleep hygiene are equally important to both the flourishing human being and the individual suffering from major depressive disorder. Mental hygiene expands across the continuum of mental illness but also that of mental health. In a similar sense, the mental hygiene framework has a salutogenic orientation, while accepting the pathogenic model. Salutogenesis (Antonovsky, 1979) is the study of human health, which considers its causes and origins, and looks prospectively on factors that support well-being. This is in contrast to the traditional pathogenesis model that explores disease and its consequences analyzing retrospectively as to the causes (Becker et al., 2010). The theoretical basis for the universality of the mental hygiene framework is grounded in the salutogenesis model, which posits that humans are susceptible to entropy or degradation lest they actively pursue actions that create health and foster well-being (Becker et al., 2010). In an increasingly complex world and exponential growth in information sharing, the mental hygiene framework postulates that mental hygienic practices are an important strategy to prevent natural tendencies of engaging in rumination, excessive self-focused thinking, and suboptimal levels of positive feelings.
However, this framework reiterates and underlines the hygiene perspective, and does not advocate the discussed approaches as first-line interventions in the management of psychopathology. In reference to the previously mentioned PA analogy, an individual experiencing lower leg edema, along with chest tightness and shortness of breath, would be misled in thinking aerobic exercise is the first-line intervention for their current condition, rather than urgently accessing a cardiac specialist. Similarly, someone experiencing severe suicidal ideation would require urgent psychiatric intervention, rather than solely engaging in a mindfulness meditation practice.
General Targets of Mental Hygiene
Hygienic practices typically have generalized targets. For instance, there can be many varieties of specific dental problems, but overall dental hygiene targets the prevention of plaque buildup, cavity formation, and the minimization of gingivitis. Similarly, although each individual may have psychological challenges unique to them, mental hygiene aims to promote mental well-being by targeting common brain activities that have the potential to be detrimental when in excess.
Mind Wandering (MW) and Rumination
MW and rumination have a ubiquitous tendency in the human experience (Mooneyham & Schooler, 2013) and are targets that mental hygiene aims to mitigate. Researchers have associated rumination and MW with a higher susceptibility to mental health issues and illnesses such as depression, anxiety, and attention deficit hyperactivity disorder (Anderson et al., 2008; Hong, 2007; Seli et al., 2015; Smallwood et al., 2007). Studies have suggested that the more time spent MW, the lower the levels of reported happiness. Research shows that the average person spends approximately 50% of their waking time MW (Killingsworth & Gilbert, 2010).
Although some have argued that MW has creative and functional components (Franklin et al., 2013), these typically only occur when the individual has a degree of awareness that they are engaging in the act of MW (Konjedi & Maleeh, 2017). Rumination, which overlaps with MW, is a process of uncontrolled recursive negative thinking that is primarily self-focused (van Vugt & van der Velde, 2018). Rumination has been shown to be a major predictor of depressive symptoms and of major depressive episodes (Takano & Tanno, 2009). It is correlated with various maladaptive cognitive styles such as self-criticism, pessimism, low mastery, and neediness (Nolen-Hoeksema et al., 2008). These two metacognitive patterns reflect a general tendency to think excessively and to overly self-focus without practical application. It has been demonstrated that one crucial difference between people who report being unhappy compared with their happy counterparts is the tendency to excessively self-focus (Lyubomirsky, 2001). Furthermore, longer periods of rumination have been negatively correlated with various measures of well-being (Harrington & Loffredo, 2011; Kompier et al., 2012; Luyckx et al., 2007). Rumination appears to exert influence on both dimensions of TFM. Its presence increases the likelihood of mental health issues and illness and hinders the pursuit of well-being. The impact of these metacognitions is further evidenced by neural correlates that have been identified in cognitive neuroscience (Gruberger et al., 2011).
Default Mode Network (DMN)
Cognitive neuroscience has produced many notable findings in mental health (Diamond & Amso, 2008), particularly relating to the DMN, a group of neural regions in the brain that when resting or nonattending to a particular task activate in unison (Berman et al., 2011). The structure of the DMN is composed of two main hubs: the posterior cingulate cortex and the medial prefrontal cortex, which link together a variety of subnetworks (Andrews-Hanna et al., 2010). It is suggested that this network is correlated with cognitive processes such as projecting oneself into the future, autobiographical memory, and theory of mind (Spreng & Grady, 2009). The DMN has become increasingly linked to self-referential mental activity, that is, the process of relating information from the external world to the self (Davey et al., 2016). This network is of particular interest as it is postulated to be the brain area that supports the human sense of self (Davey et al., 2016). DMN activity has also been associated with MW, rumination, and self-referential internal narration (Berman et al., 2011; Mason et al., 2007; Spreng & Grady, 2009). Other studies have demonstrated real-time functional magnetic resonance imaging (fMRI) data, in which participants reporting being in a state of MW corresponded with increased activity in the DMN (Garrison et al., 2013).
Research on the DMN continues and mapping out the functions of all the subnetworks is incomplete at this time. Nevertheless, we can derive a general framework from the current data that self-focused thinking, rumination, and MW without awareness are correlated with increased activity of the DMN. This research has implications for mental health. There are consistent findings to suggest that self-referential processing through the DMN plays a vital role in the development, persistence, and treatment response of serious psychopathologies, including major depressive disorder (Nejad et al., 2013).
The literature is rife with studies that have associated disorders of emotional dysregulation and other mental illnesses with DMN hyper-connectivity (Hamilton et al., 2011; Marchetti et al., 2012; Sheline et al., 2009; Whitfield-Gabrieli & Ford, 2012). An inverse relationship has been repeatedly demonstrated, in which higher reported levels of well-being are associated with decreased DMN connectivity (Luo, Kong, et al., 2016; Luo, Qi, et al., 2017; Shi et al., 2018). Neuroscience has laid out a general model that the more an individual thinks excessively in a self-focused manner via unaware MW and rumination, the more one is prone to a decrease in well-being, in turn, increasing the susceptibility to mental health issues and illness. Mental hygiene advocates that these underlying modifiable cognitive patterns require daily attention to minimize their frequency and produce the cognitive conditions conducive to well-being.
Expanding the Mental Hygiene Framework
The mental training activities outlined below are intended to create an initial platform of public recommendations that invite cross-disciplinary expert discourse, which would lead to formal mental hygiene recommendations for the public. Although the following practices alluded to in this article do not represent an exhaustive list of available mental hygiene activities, inclusion criteria were applied ensuring there were (a) significant evidence-based support for the activity to foster well-being, (b) robust safety profile, (c) potential cross-cultural application, and (d) scalability for equitable access. Other activities that did not meet all four criteria were excluded from this article. For example, although intensive meditation retreats demonstrate positive effects on well-being (Krygier et al., 2013), the safety profile for the general population is unclear and the cost/time requirements make them accessible to only a small proportion of the population; therefore, meditation retreats were excluded.
Meditation
Given the heterogeneity of meditation techniques, coupled with difficulties in measuring specific outcomes, meditation practices continue to be a challenging area to study, though research continues to grow on this topic (Van Dam et al., 2018). A meta-analysis of randomized clinical trials for meditation programs conducted by Goyal et al. (2014) reported a small to moderate reduction in multiple dimensions of psychological stress. Cognitive neuroscience has also produced notable findings in the examination of meditation and well-being. Multiple studies have demonstrated that experienced mindfulness meditators have less DMN connectivity than their novice counterparts (Brewer et al., 2011; Taylor et al., 2013). Mindfulness meditation involves focusing attention on the present-moment experience in a nonjudgmental way (Kabat-Zinn, 2003). The ability to watch the contents of one’s own mind dispassionately is a sense of self-awareness. Mindfulness meditation originates from eastern Buddhist traditions and has in recent decades become widely secularized, spanning across Eastern and Western cultures (Kirmayer, 2015). Researchers have demonstrated how engaging in mindfulness meditation makes the DMN less active than do self-referential internal narratives without awareness (Farb et al., 2007; Garrison et al., 2013). Furthermore, other variations of meditation techniques (e.g., focused attention, loving kindness) have also produced similar outcomes of decreased DMN activity (Brewer et al., 2011; Tomasino et al., 2012). Correlated to these findings is a growing body of evidence that mindfulness techniques are helpful in reducing the tendency to ruminate, which impacts psychological wellness (Deyo et al., 2009).
This is not to confuse the matter in dictating that any MW is harmful and ought to be completely eliminated, which is both impractical and unrealistic as a recommendation. MW and mindful awareness are not completely compartmentalized and separated processes but rather have a nuanced overlap (Vago & Zeidan, 2016). Vago and Zeidan (2016) describe this as “positing an overly simplistic polarization of mind-wandering as bad and mindfulness as good” (p. 108). They explain, building on existing efforts to introduce a more nuanced perspective on the relationship between mindfulness and mind-wandering, we describe a potential neurocognitive framework in which mental training associated with mindfulness allows the practitioner to more skillfully gain volitional control, flexibility, and awareness over mind-wandering, evaluation and associated DMN activity without necessarily suppressing or avoiding the flow of mental content. (Vago & Zeidan, 2016, p. 108)
Essentially, as self-awareness is cultivated, MW is less likely to lead to excessive self-focused thinking or rumination and is rendered benign.
PPIs
Other forms of mental training have been shown to have remarkable benefits on subjective wellness; PPIs are an example of this training (Chakhssi et al., 2018; Sin & Lyubomirsky, 2009). PPIs are defined as intentional cognitive activities that help cultivate positive feelings, positive behaviors, and positive cognitions (Sin & Lyubomirsky, 2009). PPIs can include practicing gratitude by counting things for which to be thankful, writing about positive experiences, rehearsal of positive statements, best possible self exercises, and positive journaling (Boiler et al., 2013). Although the approaches may vary, they all share the common factor that with regular day-to-day practice, these deliberate and intentional exercises foster cognitive patterns conducive to well-being. PPIs have been widely studied and applied in non-Western countries, demonstrating their feasibility of being a global recommendation (Hendriks et al., 2018). A recent meta-analysis further validated that PPIs help increase well-being (Koydemir et al., 2020). Cohn and Fredrickson (2010) elucidate from their findings that “positive psychology interventions are not just efficacious but of significant value in participants’ real lives” (p. 355).
Self-Directed CBT
Besides PPIs, self-directed CBT exercises have been found to increase subjective well-being (Fava & Tomba, 2009). CBT, a treatment modality that aims to break patterns of maladaptive thinking and behavior (Espie et al., 2019), is an efficacious therapeutic approach for various mental disorders (Beck, 2005). Internet-based treatment protocols effectively delivered internationally attest to their cross-cultural applicability (Gentile et al., 2018). Similar to other mental training activities, regular engagement in CBT can measurably alter brain patterns by modifying dysfunctional neural activity related to various anxiety disorders (Porto et al., 2009). The usefulness of CBT can be expanded when it is considered as a mental hygiene practice. Self-directed exercises such as writing thought records (Dubord, 2011) or “play the script until the end” exercises, which may take just a few minutes at a time, have been demonstrated to support mental well-being (Chankapa, 2018). Espie et al. (2019) recently established how CBT offered in a self-directed digital format of 20-min sessions can have profound effects on well-being. Participants were asked to complete six sessions over a 12-week period, in which the focus was minimizing symptoms of insomnia to improve functional health and psychological well-being. The intervention group showed significant improvement in the latter two metrics as mediated by a reduction in their symptoms of insomnia. This large trial of 1,711 adults offers robust evidence on the potential of self-directed CBT to support human well-being.
Prayer
Mental training for well-being can also be observed in religious behaviors (i.e., prayer). Although secularism is on the rise, particularly in Western nations, 84% of the world’ population identify as religious (Pew Research, 2017), and therefore, prayer is proposed as a mental hygiene practice with its potential cross-cultural reach. Studies on religiosity have not provided any conclusive findings that it has a positive impact on general well-being (Mishra et al., 2017); however, there have been a number of findings that suggest the regular practice of prayer is correlated with increased mental well-being (Abdel-Khael, 2010; Boelens et al., 2012; Lewis et al., 2008; Perez et al., 2011). Maltby and colleagues (1999) investigated various components of religiosity and mental well-being, and found that frequency of prayer was the dominant factor that correlated with improved psychological well-being. In a study of over 2,500 Americans, it was found that attending worship services, when accompanied by regular prayer, helped moderate the negative impact of life stressors on mental well-being (Rainville, 2018). Rainville (2018) explains how mental well-being was positively impacted “under conditions in which exposure to pro-social content at worship services is internalized through frequent private prayer” (p. 2153). The vital component in improving well-being is not religiosity per se but rather the intentional, regular, and deliberate mental training that takes place in the form of religious prayer. Perez et al. (2011) reported evidence that prayers of thanksgiving were linked to a decrease in rumination tendencies. No studies have examined the relationship between prayer and the DMN. However, using rumination as a proxy, this suggests prosocial prayer, like gratitude and thanksgiving, may have impacts on reducing excessive connectivity of the DMN. Furthermore, it is important to note that what emerges from the evidence is that the type of prayer is significant to the impact on well-being. Prosocial prayers, like praying for others, seem to be consistent with improved well-being, whereas prayers such as supplication or obligatory prayer have shown no impact (Possel et al., 2018; Whittington & Scher, 2010). Depending on an individual’s personal inclinations and beliefs, prayer as a way of internalizing prosocial content, which bears remarkable similarities to PPIs, may also be an avenue in which one might attend to mental hygiene.
Nature Exposure
In addition to mental hygiene practices that are traditionally considered contemplative or psychological, other valid approaches are also available. A growing body of evidence indicates the positive impact that exposure to nature can have on mental well-being (Berman et al., 2008, 2012; Hartig et al., 2003). This concept has been further supported by a longitudinal study reporting that urban-dwelling individuals tend to have increased mental well-being when there is more green space available (White et al., 2013). Similarly, Bratman and colleagues reported that a 50-min walk in a natural setting helped reduce anxiety and rumination, as well as increase working memory performance, when compared with controls who also did a 50-min walk, but in an urban environment (Bratman, Daily, et al., 2015).
Touching upon the DMN, research has shown that nature walks reduce rumination and neural activity of cortices in the DMN that are associated with anxiety (Bratman, Hamilton, et al., 2015; Zhu et al., 2017). This field of study continues to develop, and clarifying parameters of what types of nature setting, what frequency, and the specific measures that are impacted remains an ongoing endeavor. Despite the differences in the data on nature exposure, consensus data suggest that nature exposure is positively associated with mental well-being (Houlden et al., 2018). Deliberate and repeated exposure to nature on a regular basis may serve as a useful method to practice mental hygiene.
The Framework
As previously mentioned, practicing mental hygiene may occur through various approaches. There is evidence that demonstrates mental training behaviors like meditation and prayer, PPIs, CBT exercises, and nature exposure, when practiced regularly, lead to increased mental well-being. Figure 1 offers a graphical representation of the cognitive effects of engaging in mental hygienic practices.
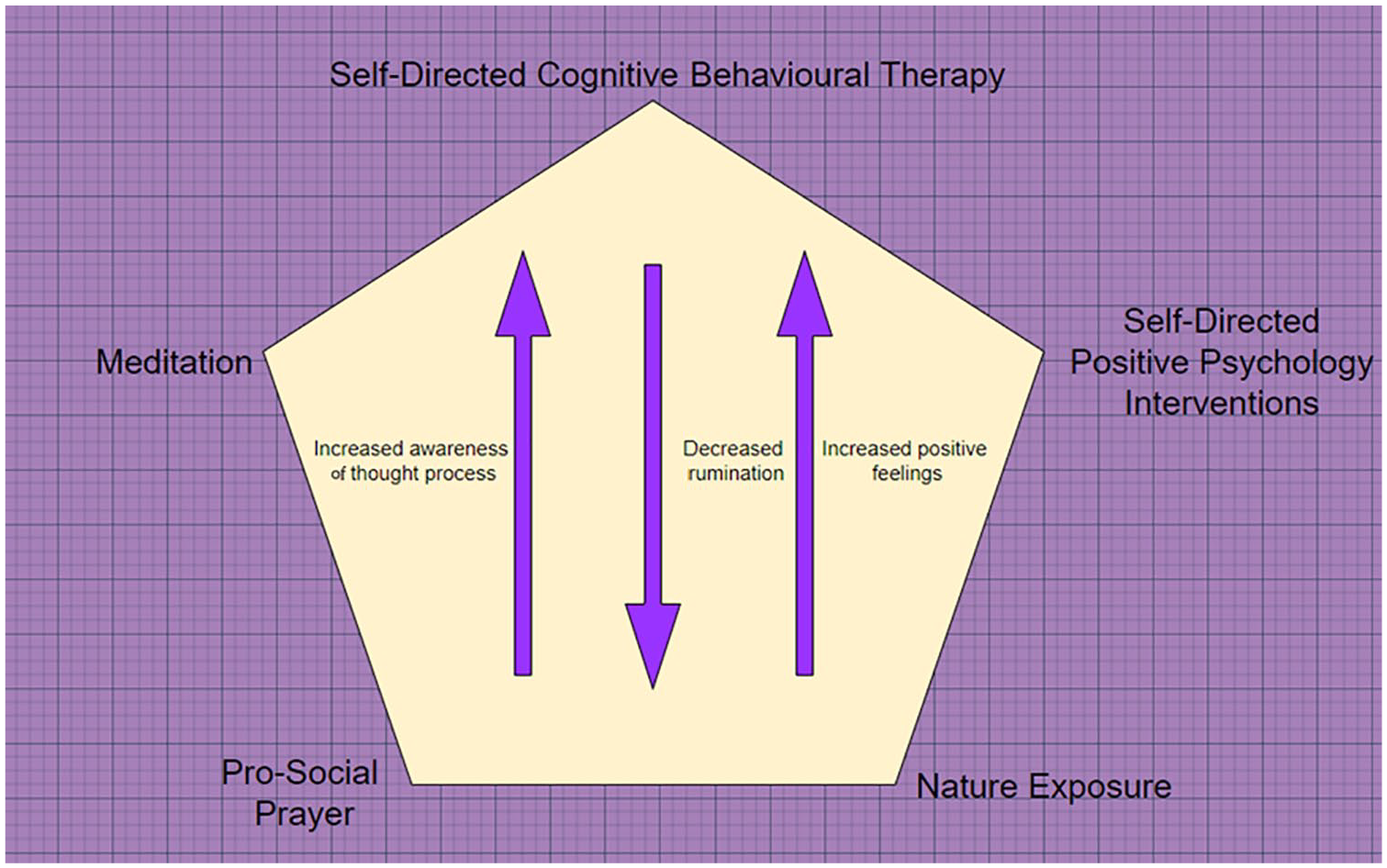
Graphical representation of the cognitive effects of engaging in mental hygienic practices.
The mental hygiene framework encourages self-directed practices in an attempt to increase an individual’s positive feelings, decrease the tendency to ruminate, and increase awareness of one’s own thought processes. This is congruent with Romano and Hage’s (2000) definition of prevention as cited in the American Psychological Association’s (APA, 2014) “Guidelines for Prevention,” which includes stopping or delaying problem behaviors and their impact, concurrently promoting knowledge, attitudes, and behaviors that promote well-being at both the individual and macro levels of communities and institutions.
The framework generally avoids specifying which mental hygiene practices are recommended for various mental health issues, leaving these to be determined by the individual experiencing mental illness but also in collaboration with the expertise of clinicians. Consensus data seem to suggest that prosocial prayer and PPIs are more impactful on nurturing positive feelings, whereas CBT and meditation tend to exert influence on increasing awareness of thought processes, as well as decreasing the tendency to ruminate (Querstret & Cropley, 2013). Nature exposure seems to help both nurture positive feelings and reduce rumination (Bratman, Hamilton, et al., 2015; Korpela et al., 2017). Furthermore, these practices are not entirely mutually exclusive, often overlapping one another. For instance, a walking meditation can be done during nature exposure, or a loving-kindness meditation may be difficult to distinguish from PPIs like gratitude exercises (Hendriks et al., 2018). Discussion surrounding other suitable practices remains an open forum for expert discourse to further refine mental hygiene recommendations so that they are clear, easy to understand, safe, and evidence-based.
Disseminating the Mental Hygiene Framework
The path to disseminating the mental hygiene framework as a public health strategy has valid antecedents on which to build. The WHO’s (2010) document titled Global Recommendations on Physical Activity for Health is a landmark in the public health initiative on a large scale. Successes of this framework were due in part to experts recognizing that promoting PA was more effective in general terms rather than promoting any one specific type of exercise (King, 1994). King (1994) argued that specific exercise routines and recommendations were often being accessed through health clubs, gyms, and fitness groups, where people already predisposed to exercise were more likely to access them. Alternatively, a simplified recommendation by public health officials, such as increasing moderate-intensity PA of one’s liking to about 30 min most days of the week, is more accessible to the wider public (King et al., 1995).
Similarly, mental hygiene practices are accessible through different forums like meditation classes, spiritual and religious groups, or therapy sessions. Although a benefit for those who participate, some practices are inherently limited in terms of accessibility to the wider public. Joining a mindfulness-based stress reduction class, for example, typically involves scheduling the class around your routines and priorities, and paying a fee upon the availability of the class. Similarly, accessing a mental health professional who might offer CBT or recommend PPI exercises is often prohibitive. In the United States, a 2010 survey found 47% of people with mood, anxiety, or substance use disorders who felt they needed mental health services could not access them due to cost or lack of insurance (Rowan et al., 2013). The mental hygiene framework is not a substitute to the relentless efforts still required to make mental health care more accessible to marginalized populations and low-income households, but is posited as a novel approach to engage the public in prevention and outreach, which is in line with equity and social justice (Vera & Speight, 2003). Mental hygiene practices such as 3 to 4 min of focused attention on breathing 2 to 3 times a day, or sitting down for 5 min a day to engage in positive journaling, are accessible to all. The WHO’s (2010) document provides general concepts of physical exercise to help simplify the communication of recommendations. Table 1 outlines a few of those recommendations and offers a proposed mental hygiene equivalent.
Mental Hygiene Recommendations Based on WHO Exercise Recommendation Model.

Note. WHO = World Health Organization; CBT = cognitive-behavioral therapy.
The recommendation of 10 min per day of mental hygiene was chosen as an arbitrary starting point guided by the literature. Most meditation studies usually involve 1 to 3 hr of training per week, spread either as one large training session or as a daily protocol (Goyal et al., 2014), some of which included 12 min of practice per day (Moss et al., 2012). Similarly, PPI studies often involve 4 hr of training per week for 8 to 12 weeks (Schotanus-Dijkstra et al., 2015). As previously mentioned, some CBT studies involve six sessions of 20 min over 12 weeks. Unfortunately, many of the study protocols do not necessarily offer sustainable practices for many individuals. Based on habit formation models, which suggest regular repetition to transition from reasoned action to habitual behaviors (Aarts et al., 1997), 10 min of mental hygiene on a daily basis is proposed.
The WHO’s global recommendations on PA have been instrumental in raising awareness of its importance. Awareness of the benefits of PA has been shown to be an independent factor associated with greater adherence to PA recommendations (Alkerwi et al., 2015). Developing large-scale mental hygiene recommendations for the public would require a similar process to the development of the WHO’s global recommendations on PA. Concrete steps are to (1) include expert group meeting, (2) define scope, (3) include content and target audience of recommendations, (4) include further compilations and assessment of scientific evidence, (5) include initial drafting of recommendation, (6) submit first draft to a peer-review process and obtain stakeholder input, (7) finalize draft, (8) submit final draft for further revisions, and (9) obtain approval by guideline review committee. Subsequently, implementing and disseminating the guidelines would involve complex processes such as social marketing, systems approaches, communication theory, and diffusion (King, 1994), steps that are beyond the scope of this article.
Conclusion
Population mental health is recognized as one of the greatest public health challenges of the 21st century (Fuhrer & Keyes, 2019). It is a complex, multidimensional challenge that encompasses many factors, some of which have been clearly identified, while others are still being determined. With this growing recognition, remarkable ideas and efforts have been initiated and implemented. Institutions and organizations are establishing efforts to reduce stigma, increase access to services that foster psychological well-being, and raise awareness around mental health issues and illness through campaigns like Bell Let’s Talk Day (Bell Media, 2019); agencies like the Ontario Telemedicine Network (OTN) are increasing access to mental health care by offering telehealth services (OTN, 2019); evidence-based research is promoting a recovery ideology and the profound effects of peer support (Campos et al., 2016); and governing agencies are working to implement further greening of urban spaces (Evergreen, 2004) and improve social support services. This challenge needs to be addressed from a variety of approaches. Encouraging a grassroots movement in which individuals deliberately train their minds on a daily basis to foster healthy cognitive patterns is warranted for consideration and further deliberation. Educating the public about mental hygiene, in a similar fashion as the WHO, may be a useful undertaking as part of a multipronged approach to strengthening the public mental health strategy.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.