
Abstract
Black transgender women (BTW) are subjected to transmisogynoir, as intersectional minority stress and violence that increases their risk of negative well-being. The purpose of this study was to explore themes of intersectional violence and well-being in a group of BTW in Los Angeles, California, from their perspectives. Ten participants were interviewed, and data were analyzed using consensual qualitative research. This article focused on themes around transmisogynoir and (a) mental well-being, (b) social determinants of health, and (c) help seeking. Recommendations for BTW well-being interventions and future directions to promote BTW wellness are provided.
Keywords
Black transgender women (BTW) experience high rates of violence enacted at interpersonal, community, and systemic levels that manifest as denial of social and economic opportunities, social marginalization through discrimination, intimate partner violence, and murder (Human Rights Campaign [HRC], 2022). The roots of this violence stem from misogynoir, a term popularized by Bailey and Trudy (2018) referring to the unique, oppressive, and violent ways in which Black women are pathologized and unfairly treated at the interpersonal, social, and institutional levels given the interlocking and intersecting power dynamics and stigmatization (i.e., devaluing diverse groups; Dovidio et al., 2000) of race and gender. Yet BTW are exposed to a unique form of misogynoir, given that they are further marginalized due to cissexism (i.e., prejudice and discrimination directed toward transgender persons; Westbrook & Schilt, 2013). To account for this complexity, the term transmisogynoir, first coined by Julia Serano (2007) and critically expanded on by Krell (2017), refers to the violent, oppressive, and intersectional experiences that BTW are subjected to given interlocking systems of oppression rooted in anti-Blackness, sexist, and cissexist violence. Consistent with minority stress theory (Hendricks & Testa, 2012; Rich et al., 2020), transmisogynoir is a unique intersectional minority stressor stemming from social interactions at the interpersonal level and with systems/institutions that perpetuate violence through anti-Blackness, sexism, and cissexism (LaMartine et al., 2023; Millar & Brooks, 2021).
The impact and magnitude of transmisogynoir as violence is palpable, with BTW accounting for 69% of the victims of anti-transgender violence and two-thirds of murders of transgender people (HRC, 2022). In 2022 alone, there were 37 violent murders of transgender and gender-diverse persons, most of whom were BTW (HRC, 2022). Additionally, BTW contend with other experiences that result from transmisogynoir, including high rates of poverty, homelessness, sexual assault/violence, and mistrust of police and legal systems (James et al., 2017). The mental toll of transmisogynoir on BTW is substantial; data indicate experiences of violence are traumatizing to BTW (LaMartine et al., 2023) and associated with poorer health (Sherman et al., 2020).
In the context of the broader transgender literature, transgender women are exposed to high rates of violence and discrimination (Flores et al., 2021). Despite growing attention to the need for a focus on public resources and health care access for transgender persons (Arayasirikul et al., 2022), the unique forms of violence faced by BTW, specifically transmisogynoir, are not adequately covered in the broader transgender literature (Krell, 2017; LaMartine et al., 2023; Millar & Brooks, 2021). Thus, we argue that BTW are exposed to unique intersectional minority stressors—shaped by multiple experiences of violence and discrimination rooted in transmisogynoir—that affect overall well-being as discussed below.
Social Determinants of Health
Social determinants of health (SDoH) are defined as “conditions in the environment where people are born, live, learn, work, play, worship, and age that affect a wide range of health, functioning, and quality of life outcomes and risks” (U.S. Department of Health and Human Services, n.d.). Factors such as income, employment, and access to health care have distinct and heightened effects as social determinants that impact transgender persons (U.S. Department of Health and Human Services, n.d.). Additionally, institutional racism, discrimination, and violence are considered SDoH (Paradies et al., 2015). Experiences of racism, sexual/gender minority stress, and cissexism as SDoH contextualize health disparities experienced by socially minoritized communities as they reflect interconnected and bidirectional stressors that impact and threaten BTW well-being (Blosnich et al., 2017; Davis, 2020; Paradies et al., 2015), as shown in Figure 1.
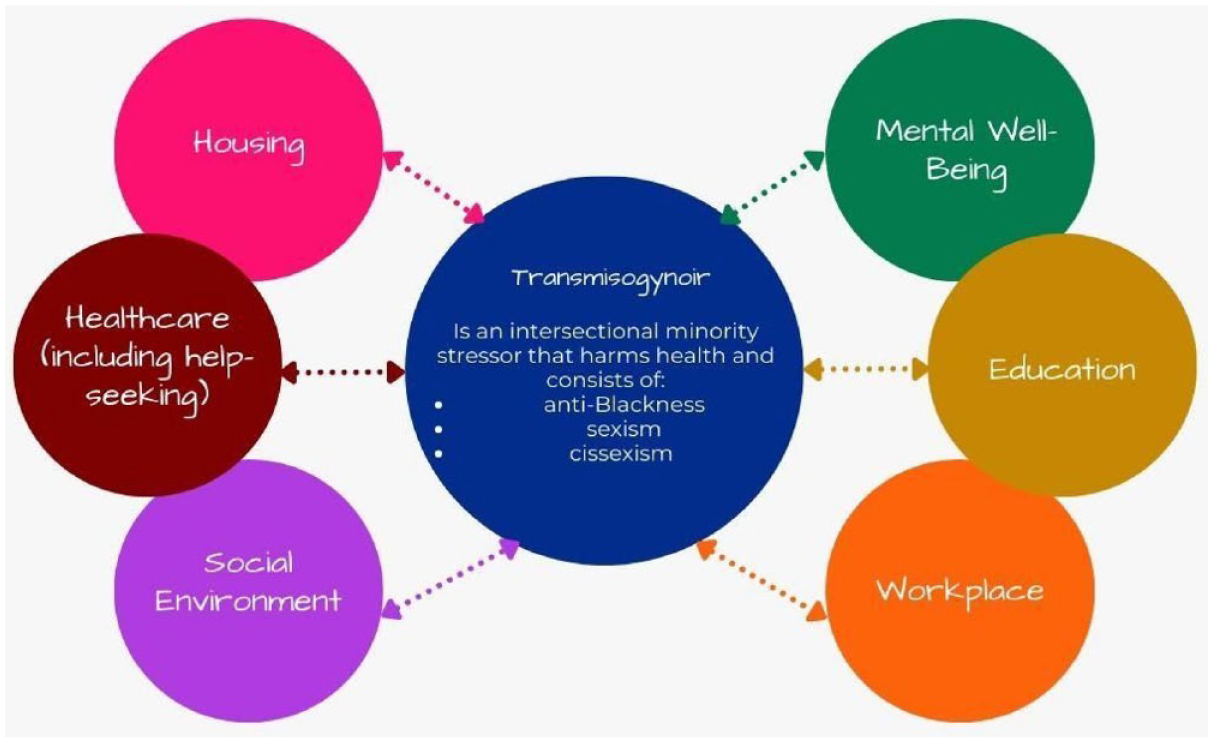
Conceptual Relationships of Social Determinants of Health and Transmisogynoir as Intersectional Minority Stress
Using a general SDoH framework to understand BTW well-being is not new. For example, in a qualitative study of BTW in the American South, Smart et al. (2020) found themes related to polyvictimization that stemmed from the family, their community, legislation barriers, and mistrust in health care systems (i.e., SDoH) that determined whether BTW engaged with health care. Similar themes were echoed in a sample of BTW when asked about their health care experiences in Maryland (Sherman, Balthazar, et al., 2022). Therefore, researchers understand that the social milieu—and the violence perpetuated within it—act as powerful determinants of BTW well-being. This is important to note given that for BTW, anti-Blackness, sexism, and cissexism uniquely intertwine as transmisogynoir violence (Bailey & Trudy, 2018; Wodda & Panfil, 2014).
Well-Being and Help Seeking
According to the World Health Organization (WHO), health involves not just the absence of disease or illness but also a complete analysis of physical, mental, and social aspects that contribute and factor into promoting well-being (WHO, 2018). As the WHO (2018) emphasized, mental health is also an important and necessary component of health. To this end, data presented in this section will take a broad definition of well-being (i.e., one that incorporates physical and mental health) to contextually understand the well-being of BTW. An important aspect of taking care of one’s health is help seeking, which refers to the actions that individuals engage in to get resources from other people, communities, or institutions, including primary care and mental health providers (Persson Tholin & Broström, 2018). Data indicate that differences exist in help seeking by race/ethnicity (Leong et al., 1995) and among gender-diverse persons, with evidence indicating that transgender people are less likely to seek help for their well-being compared to cisgender counterparts (Howell & Maguire, 2019). To this end, we will also discuss data on BTW help seeking in this section.
Some literature exists on the associations between intersectional violence (i.e., intersectional discrimination) and mental health symptoms (i.e., depressive symptoms, post-traumatic stress disorder (PTSD) symptoms, comorbid depressive and PTSD symptoms, general psychological distress) as well-being in BTW. For example, in a sample of majority BTW from the Sheroes Study, intersectional discrimination was positively associated with depressive symptoms (Jefferson et al., 2014). Moreover, using an innovative mixed-method study of intersectional violence and well-being, Sherman, Balthazar, et al. (2022) found that qualitative interviews of BTW in their sample experienced multiple types of violence, and narratives of participants revealed high endorsement of mental health symptoms. Moreover, Millar and Brooks (2021) examined psychological distress and found that Black transgender people were at higher risk for reporting mental distress as a function of intersectional violence, compared to White transgender persons. In a study examining violence in a large sample of BTW, Sherman et al. (2020) found that polyvictimization was positively and uniquely associated with depression and PTSD symptoms; however, the study lacked exploration into themes of transmisogynoir as a form of intersectional violence, despite the significant representation of BTW in the sample.
Other studies focus on intersectional violence (i.e., intersectional discrimination) in the context of SDoH, with findings indirectly relating to the well-being of BTW. For example, in a study of BTW in the San Francisco Bay Area, intersectional discrimination (conceptualized as an SDoH) was associated with increased odds of housing instability, a variable often associated with poorer well-being (Beltran et al., 2019). Moreover, Smart et al. (2020) found that SDoH (defined as family rejection, bullying, discrimination, violence, isolation, policy barriers, mistrust in systems, unstable employment, sex work, transportation issues, church antagonism, and substance use problems) emerged as a unique theme to contextualize the well-being experiences of the BTW sample living in North Carolina. In another qualitative study, Lacombe-Duncan et al. (2022) described the experiences of BTW in Detroit with regard to intersectional discrimination—in the context of housing, employment, income, education, and health care as SDoH—and their well-being. Results showed that experiences of exclusion within lesbian, gay, bisexual, transgender, queer, and/or questioning (LGBTQ+) communities, communities of color, and LGBTQ+-serving community-based organizations/programs harm the well-being of BTW. Similarly, among BTW living in New Orleans, intersectional discrimination experienced within housing and employment was reported by the sample; however, findings were not directly linked to well-being but instead were discussed within the framework of SDoH (Glick et al., 2019).
Among survivors of violence, Sherman, Allgood, et al. (2022) found that BTW in the Baltimore and Washington, DC area who sought help from formal institutions were re-exposed to physical and verbal abuse from these resources. Some study participants reported positive and affirming interactions with these institutions when in the presence of LGBTQ+ staff, which often led to BTW receiving the help they needed to improve their well-being; however, others indicated threats to their confidentiality due to familiar persons (e.g., LGBTQ+ individuals or family members) working within those institutions, which made some BTW reluctant to seek help for their well-being. Most participants reported help seeking from formal resources, like emergency housing, health care, and legal assistance, and preferred to seek help from LGBTQ+ formal sources. The BTW in this study also indicated seeking help from same-gender peers. However, findings from this study with BTW indicate that barriers to help seeking exist like discrimination and stigma from society and institutions, a finding in line with the broader transgender literature.
More specifically, Hereth (2021) explored the distinct barriers that transgender women experience in the context of victimization and help seeking, including cissexism, among transgender women in Chicago. Results of their qualitative study found unique experiences of victimization for transgender women, which deter them from seeking formal avenues of support (e.g., police, medical, or professionals). Critically, the sample was majority BTW, yet themes related to transmisogynoir were not reported in the context of victimization and help seeking. Guadalupe-Diaz and Jasinski (2017) examined themes from a sample of transgender women experiencing intimate partner violence. They found that most sought help from formal sources (e.g., police, legal action, shelters) and informal sources (e.g., help from family, friends, or coworkers); yet, when seeking support, they often encountered cissexism and gender discrimination in these interactions with formal and informal sources of support. Notably, while the sample had transgender women, only three were Black, possibly obscuring the unique forms of intersectional violence (e.g., transmisogynoir) faced by BTW. As shown above, when BTW engage in help-seeking behaviors, they are met with barriers from formal sources, including experiencing intersectional violence. Simply put, having access to resources is meaningless if the institutions and individuals that provide these resources perpetuate intersectional violence that further marginalizes BTW. Thus, there is a strong need to understand how help seeking plays out in the context of the well-being of BTW.
Current Study
As demonstrated above, BTW experience intersectional violence as transmisogynoir, which is associated with their well-being. As a framework, SDoH has been used to provide context to the unique blend of factors that impact and shape the well-being of BTW by producing health disparities. Furthermore, limited literature exists on help seeking in BTW. Due to the prevalence of chronic and unrelenting transmisogynoir as intersectional violence, this study centered on BTW from Los Angeles, California (L.A.). We focused on understanding the well-being of BTW and intersectional violence in L.A., given previously documented unmet needs reported by a clinic in the L.A. area (Sussman et al., 2015). Thus, our aim was to explore themes surrounding transmisogynoir and well-being among BTW.
Methods
The present study utilized consensual qualitative research (CQR), a qualitative approach that emphasizes team member collaboration to co-construct meaning from participant-reported experiences (Hill, 2012). CQR was selected because of its emphasis on “mutual respect, equal involvement, and shared power” (Hill et al., 1997, p. 523), which aligns with the values of the researchers. CQR prioritizes consensus between the research team and participants (Hays & Singh, 2023), which was particularly crucial in this study due to the lack of BTW on the research team. Further, CQR promotes power sharing among researchers and participants, which helps mitigate researcher bias stemming from researchers’ values, assumptions, and preferences (Hays & Singh, 2023). By acknowledging the impact of our personal and cultural backgrounds on data collection and interpretation, we can better honor and respect the perspectives of participants and achieve more effective research practices (Hays & Singh, 2023).
Planning the Study
While the lead researcher originally intended to investigate the experiences of violence among women of color broadly, preliminary review of the literature and the media (e.g., television, newspaper, and podcasts) suggested that transgender women were at increased risk for violence and repeated victimization. A thorough review of the literature confirmed that transgender women of color, particularly BTW, were disproportionately impacted by discrimination and violence compared to cisgender women. As a cisgender co-conspirator (i.e., going beyond mere support by taking proactive steps toward social change; Chang & Singh, 2018; Patterson, 2018) committed to action, the lead author proactively sought opportunities to gain a deeper understanding of systemic issues (e.g., transmisogynoir, racism, and classism) impacting BTW and examined how these institutional barriers overlap to create food, housing, and financial insecurities for BTW. While BTW were not involved in the creation of the study, the researchers sought feedback from multiple “cultural insiders” during the collection and interpretation of the data (Patterson, 2018, p. 147).
Sample
This study was approved by the institutional review board of a university that the authors were affiliated with at the time of the study. Participants were recruited from several LGBTQ+-serving organizations located in Los Angeles County (n = 9) and national listservs (n = 1). The primary author established contact with a community leader and was invited to various social events where she was given the opportunity to discuss her research. Eligible participants were between the ages of 18 and 65 years old, identified as transgender women of color, and agreed to participate in the study. Initial verbal consent was obtained from all participants prior to scheduling of interviews that took place at a time and location most convenient for each participant. At the beginning of each interview, the researcher briefed participants on the nature of the study, discussed potential risks and benefits of participation, and collected written consent from those wishing to engage with the study. Participants were compensated $24 for their time, the maximum allowed by the Institutional Review Board that did not require participants to complete a W-9 form for tax purposes. Additionally, the lead researcher made donations to two local organizations serving transgender communities and engaged in volunteering both before and after data collection.
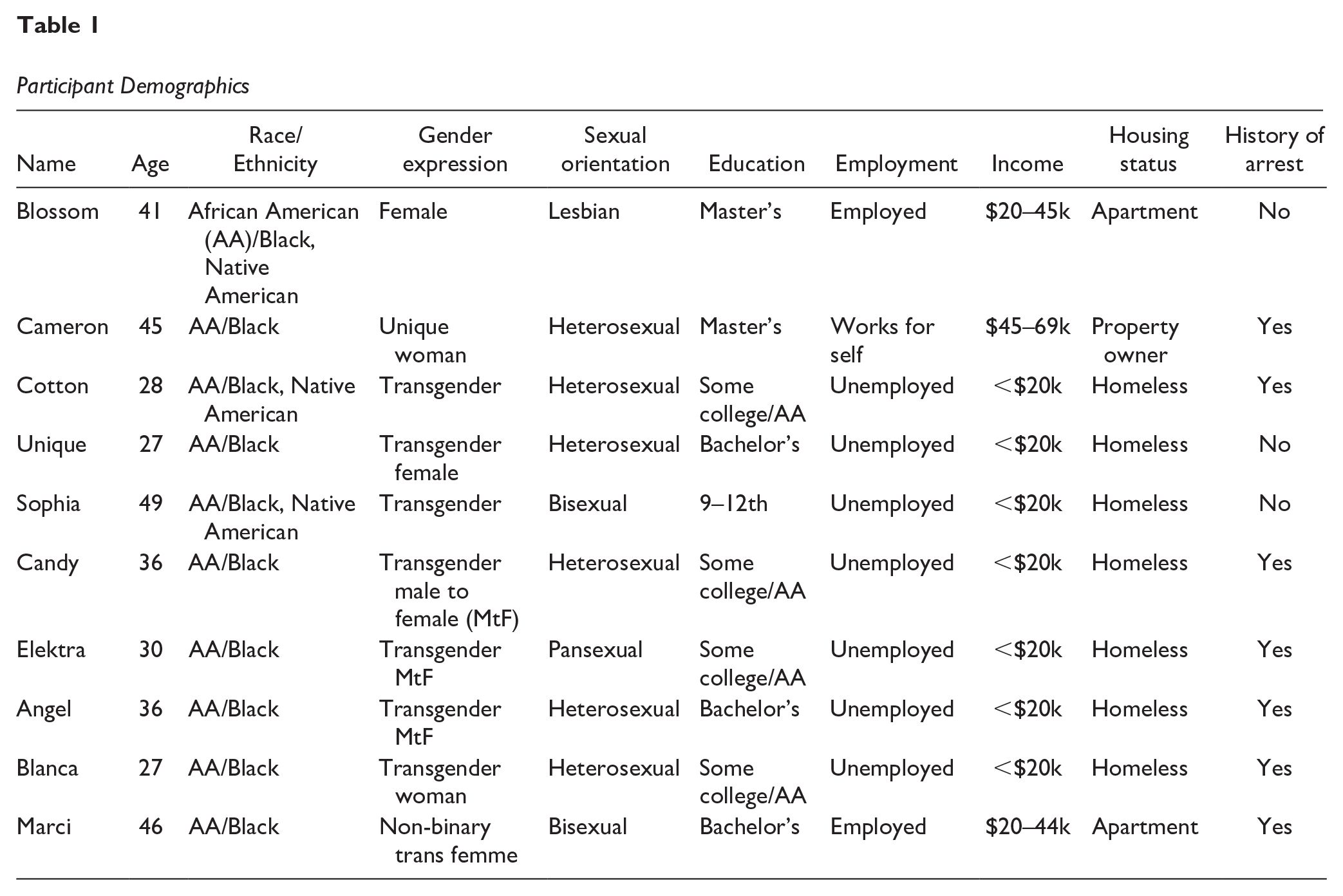
Participants ranged in age from 27 to 49 years old (M = 36.5; SD = 8.40). While the study was open to transgender women of color broadly, all 10 participants identified as Black or African American, with 3 participants also identifying as Native American. Overall, participants were highly educated, and two had master’s degrees in mental health–related fields. Despite their level of education, most participants were unemployed, deprived of adequate housing, identified as struggling with poverty, and had a history of arrest (see Table 1).
Participant Demographics
Researchers
The research team, composed of doctoral-level clinical psychology graduate students, was led by a Black, cisgender, heterosexual woman, who utilized the steps outlined by Hill (2012) to train the research team on the CQR process. The remaining members included a heterosexual, cisgender, Latina woman; a bisexual, cisgender, White woman; and a gay/queer, Chicano/Latino person who described their gender identity as existing along a spectrum, encompassing both cisgender and gender nonconformity. The auditor was a queer, cisgender, Asian American woman, and psychology professor specializing in LGBTQ+ populations. Both the lead author and auditor had previous experience with CQR methodology. While the lead researcher was experienced in interviewing survivors of racial violence, the rest of the team had varying degrees of violence training. None of the team members had prior clinical experience with BTW and relied on literature for guidance. The second author, a gay, cisgender, Latino man, has executive leadership experience in an LGBTQ+ organization and clinical experience working alongside BTW in health care.
Procedures
Participants who met eligibility completed a brief demographic questionnaire including age, race/ethnicity, occupation, socioeconomic status, sexual orientation, gender expression, housing status, level of education, and incarceration history. The lead author created the 25-item semistructured interview (see Appendix), which consisted of open-ended and follow-up questions adapted from previous research on discrimination and violence experienced by transgender people (e.g., Nadal et al., 2012; Singh & McKleroy, 2011). The interview protocol included questions about accessibility to care, past experiences with clinical providers, and a discussion on how “your experiences of being a transgender person of color influenced your mental health?” Probes were used to elicit or clarify responses to enhance understanding.
BTW were not involved in the development of the interview protocol. However, as suggested by Singh and McKleroy (2011), participants were asked to provide additional interview questions related to the study’s topic at the end of each interview to highlight additional aspects of their experiences and to inform future studies.
All 10 interviews were conducted during August of 2018 in a reserved room at a public library or at an LGBTQ+-serving institution. During the informed consent process, participants were told that interviews would be audio recorded, and the primary researcher explained how confidentiality would be maintained. For example, participants were randomly assigned a three-digit numerical code followed by their initials to create a codename. Codenames were later converted to pseudonyms, derived from BTW television characters, for increased identity protection. At the beginning of each interview, the lead researcher disclosed her positionality (e.g., race, gender, education, cultural background, and other aspects of identity that may influence her perspectives) to address potential power dynamics and to foster open/respectful communications. The semistructured interviews began with general questions about the participant’s gender identity and expression, which were designed to build rapport, before moving to more focused and specific questions about past experiences of violence and its impacts, and coping skills (Hill, 2012). Each interview lasted approximately 60 to 90 min (M = 77.5, SD = 10.19). At the end of each interview, participants were debriefed and provided a mental health resource sheet, contact information for the lead author, and a small honorarium in cash. For the purpose of expanding the sample, participants were encouraged to recommend others for interviewing. As suggested by Creswell and Poth (2016), snowball sampling, a type of convenience sampling, may be an efficient and cost-effective way to engage study participants from vulnerable populations.
The digitally recorded qualitative interviews were transcribed verbatim using Transcription Puppy, a paid transcription service, and the lead author crossed-check and edited the transcripts to ensure accuracy. All documents were securely stored on the lead researcher’s password-protected laptop to prevent unauthorized access. The data analysis process was conducted in accordance with the guidelines established by Hill (2012). Starting with the first interview, the research team coded each transcript independently before coming together to compare notes and codes. The domain list was co-created by the research team and further developed as it was applied to each transcript successively. When conflicting interpretations were presented, the team discussed the quote and reached consensus about the most appropriate code for the given statement. After coding all interviews, participants were invited to provide feedback (i.e., member checking) on the appropriateness of the themes identified and to ensure alignment between the participant’s interpretation and the interpretations of the research team (Hill, 2012). Due to structural barriers (e.g., transportation, limited Wi-Fi access, phone service, and disconnection), but consistent with recommendations by Hill (2012), 20% of the sample participated in member checking by reviewing the data. They did not report any discrepancies. Last, the auditor reviewed the final analysis and made recommendations that were subsequently addressed by the team.
Credibility and Trustworthiness
As suggested by Hill (2012), at the beginning of the study and during the coding process the research team engaged in various discussions around the biases and assumptions each member had about transgender women of color. This included beliefs about education, history of childhood sexual abuse, transgender identity as a fixed gender, societal acceptance of transgender individuals, the idea that transgender people have always existed, conflicts between family values and transgender identity, and religious teachings about transgender identity being an abomination. As encouraged by Patterson (2018), researchers reflected on their positionality and engaged in discourse around their social privileges. Furthermore, the team employed bracketing practices (i.e., suspension of preconceived notions), which serves as a checks and balances system and provides opportunities for researchers to reflect on how their own biases may influence study design and data interpretation (Hill, 2012). For example, during the early stages of the study’s development, the lead researcher engaged in multiple dialogues with the auditor regarding her social privileges and brainstormed strategies to reduce the likelihood of exploitation of the vulnerable participants. Similarly, before accessing any data, the research team performed a critical self-evaluation of their own expectations and the potential impact of their social privileges that could bias their ability to accurately analyze the experiences of marginalized persons. This was done to prevent any misinterpretation of the data. Moreover, researchers engaged in discussions around allyship and processes through which people have constructed and engaged in advocacy endeavors that ultimately harmed oppressed communities.
Further, the lead researcher enlisted feedback on the methodology and results from an independent colleague with no vested interest in the study. Peer debriefing was used to explore overlooked data, reduce potential researcher bias, and maximize rigor (Hill, 2012). The auditor played a crucial role in ensuring the validity of the data; verifying its accuracy; ensuring that the domains, categories, and core ideas accurately represented the participants’ narratives; and evaluating cross-analyses for accuracy and effectiveness (Hill et al., 1997).
Results
The data used in this study were collected as part of the lead author’s dissertation research, which aimed to investigate BTWs’ experiences of violence and coping strategies to mitigate the effects of repeated victimization. However, the current study will focus solely on themes related to transmisogynoir as intersectional violence as it relates to (a) mental well-being, (b) SDoH that influence BTW’s well-being, and (c) help-seeking behavior within the context of past health care experiences. For some themes, the intersectional minority stress against BTW occurred in the context of transmisogynoir. In the following section, we use the SDoH framework to better understand factors impacting BTW well-being.
Mental Well-Being
All participants (N = 10) endorsed mental distress that developed or was exacerbated by ongoing exposure to transmisogynoir endured on a daily basis. Repeated exposure to discrimination and violence can result in the internalization of harmful stereotypes or attitudes, causing individuals to accept and believe negative messages directed toward them. This can erode self-esteem and a sense of belonging and result in negative mental health outcomes including mood disorders (e.g., anxiety, bipolar, depression), PTSD, hallucinations, and substance use. For example, Blossom shared: I have had multiple mental health concerns [e.g., anxiety, depression, and PTSD]. I’m dealing with a lot of pressure and I’m struggling day to day . . . just having the amount of pressure of living, I’m dealing with the struggle day to day . . . There were times where transphobic messages came through and [I internalized them]. It made me depressed, lots of sadness; it was tough. I had a therapist who helped me deal with my PTSD that I had been struggling with since childhood.
Likewise, Blanca shared her personal struggles, including her mother’s history of anxiety, which she also experiences “sometimes, but I don’t—I try not to let it bother me.” She also identified as having a “gender dysphoria” diagnosis. Other participants alluded to experiences of stagnation, powerlessness, and emotional blockage. For example, Unique stated: I still have a lot of depression. I get depressed sometimes, I don’t know how to process or like move in general. And so, I just get stuck. And that’s where I’m at right now. I’m just stuck. And I really feel like it’s a big mental hurdle. I just can’t push over it.
For some, the “mental hurdle” also contributed to feelings of worthlessness and suicidal attempts. Per Angel, “I went through a storm and I became suicidal. I didn’t want to live because I didn’t think my life was worth living. But I overcame that and I don’t feel like that today.”
Some participants experienced additional challenges in accessing mental health resources and support, which may have exacerbated their symptoms. For instance, Blossom disclosed: “I’m a figure in my community—I’m always concentrating on the end game. I don’t always have enough—I don’t always have the ability to check in [on herself]. I don’t always have the opportunity to unpack all of my stuff. I don’t have the time or money.” Blossom’s sentiments highlighted the intersectional challenges she faces as both a Black transgender advocate and community member, navigating societal and systemic barriers such as discrimination, marginalization, and violence, which creates significant pressure and stress in her efforts to promote positive change. Moreover, participants also face barriers in accessing support from within the communities, as described by Unique “being a transgender woman of color and not being able to find a partner, being in my own community and yet being outcast. I feel alone and those things added to my depression. They make me lower my self-value.” Unique’s disclosure also highlights the insidious nature and personal and/or societal cost of mental distress that results in feelings of entrapment, disempowerment, and doom. The depression presumably impacted her ability to engage in her community, which in turn impaired her community’s ability to support her—resulting in increased depression.
Several participants discussed their experiences of living with serious mental illnesses, triggered and/or exacerbated by repeated victimization and accompanied by psychosis. For over 8 years, Marci utilized street drugs to manage her untreated auditory and tactile hallucinations, depression, and mania, further perpetuating her addiction. She elaborated: And it was like 8 years of this, hearing 12 voices, 8 voices touching me. Everywhere I went, I had to pretend everything was okay—when I was hearing voices in my head made me use the drugs more, cause I was self-medicating, which made me homeless . . . I developed schizophrenia . . . found out I was bipolar-depressive . . . these manic episodes of depression—which made me do the drugs more.
Likewise, while imprisoned, Elektra was held in solitary confinement for 24 hr per day, and this triggered psychotic symptoms. She reported, “It was turning me into an animal almost like I was going crazy, like pacing the floors and hallucinating, seeing things, and like I will try and get out of myself, but I had to keep myself focused.” She was diagnosed with bipolar disorder and more recently schizoaffective disorder, due to the persistence of her auditory hallucinations. She elaborated: Recently in November last year . . . I was diagnosed as schizoaffective, because in April 2012 I started hearing voices within my head. Not from myself per se but others. It was like another keen sense . . . I don’t want it though. It irritates me. It’s really traumatic, disturbing, and I feel like I’m going crazy—feels like I’m insane.
While not entirely convinced that she has bipolar disorder, Blossom endorsed trauma symptoms including insomnia, hyper arousal, nightmares, fatigue, and anxiety. She shared: Bipolar disorder? No, cause I don’t have mood swings or the other components. I’m just primarily up all night. Um, so if I do fall asleep, I’m going to have all the hunger to relive all those things . . . a lot of times I would just become so tired and I would sleep for 12 hours. And I wake up numerous times, just cold sweats, screaming, and other things . . . it’s a really, really tough road. You’re just afraid all the time, and you can just feel everything kind of happening around you.
Likewise, Angel expressed uncertainty about her mental health, saying, “Sometimes I think I’m bipolar,” while also discussing the ongoing challenges of coping with the loss of her mother and the associated grief. She stated: I’m hurting and I’m in pain and somebody might say something out the way to me, and it may not even be that serious, but I may just go all in, just because—Uh, I don’t think that necessarily means I’m bipolar, of course that doesn’t mean I’m bipolar, but sometimes I feel like I am bipolar—just—I’m just—I have a temperament problem for sure.
Like many BTW, Angel often experiences multiple burdens in which they simultaneously face interrelated sources of distress or difficulties. Coping with the emotional pain of grief is a complex and prolonged process for Angel, while external circumstances may also jeopardize her safety and well-being, leading to increased stress and anxiety. This compounded burden can escalate psychological distress, ultimately leading to long-term consequences.
In some cases, participants reported current psychological difficulties resulting from repeated and ongoing distress. For example, Sophia stated: Mental health? I’m throwed off, yeah, I’m throwed off [i.e., crazy, insane, and in constant distress]. At times I feel like I’m cuckoo for Cocoa Puffs. I have a lot of mental problems including depression, nightmares, flashbacks, I can’t sleep or eat, I’m always scared, I get anxious, [and] I have a lot of PTSD. I have it all.
The provided examples elucidate the multiple challenges that BTW face, which, in various ways, are related to transmisogynoir that contributes to psychological distress. Participants described experiencing gender dysphoria, depression, bipolar disorder, and PTSD as well as specific symptoms such as suicidality, hallucinations, flashbacks, sleep disturbance, and internalized transphobia. In some instances, substance use was a way to cope with symptoms of mental illness. As reported by participants, a lack of access to mental health resources, dangerous social environments, neighborhood factors, and incarceration are just a few SDoH that exacerbated mental health issues in this sample.
Social Determinants of Health
Participants (n = 7) discussed difficulties in securing housing, receiving social services, and/or finding suitable employment; this also included instances of discrimination and marginalization faced by participants. For example, Angel recalled being profiled while waiting in line at a local homeless shelter for food. She noted: We were profiled from the moment we got in the line. One of the workers came and told us that the food was for homeless women only and then asked for our ID. I felt so humiliated and couldn’t believe that was happening.
Similarly, Cotton reported experiences of housing discrimination. She recalled: I applied for a house and . . . [was] told over the phone that it was available. When I arrived the guy realized that I was a transgender woman, [and] told me he would not be able to work with me. He’s a White man, but I understand why he didn’t want to rent to me.
Participants’ narratives illustrated the unique nature of intersectional minority stress and discrimination. Some participants noted the complexities associated with navigating both heterosexism within Black communities and anti-Black racism from White LGBTQ+ communities. For Elektra, intragroup marginalization has resulted in both mistrust of herself and her racial community. She shared: [I’ve been hurt so much by Black people] Now, I don’t know how to deal and live around my race and I don’t want to feel that way. I love my race. But so much trauma. It puts scars on your heart and PTSD in your mind, to the point where I’m not as trustworthy or easy going. I feel like a coward, I don’t make much eye contact with others, I stare at the ground. I’m not a social person. I’m very traumatized.
Participants were keenly aware of the impacts of societal stigmatization related to their intersecting social identities—they were often perceived as inferior to or “less than” cisgender women, and this made it harder for them to find and retain suitable employment. As a result of transmisogynoir and accompanied workplace discrimination, participants saw survival sex work as a viable source of income for them. Cotton explained: I started escorting at the age of 12 because I was homeless and broke. My family kicked me out, and I was living on the streets when I met this guy who promised me shelter. He got me engage in sex work, and I did it for some years.
BTW may also be subjected to workplace harassment and discrimination. Elektra recalled feeling negative and unwelcoming “vibes” from her cisgender coworkers of color. She reported feeling alone and rejected as her coworkers did not want to train, work, or interact with her (e.g., converse with her and/or eat next to her). Further, some even expressed outward disgust toward her; as such, she was fired shortly after being hired. She described: So she [manager] allowed me to get my first check and that following work week she just terminated me. And she didn’t even give me a reason. Like she just said, “Don’t come in tomorrow. And I’m gonna call your temp [agency].” I never heard from her again.
As explained by Cameron, even when work conditions are bearable, BTW are often undervalued and their contributions to the team go unnoticed. She recalled, “We never get any recognition for our work. It’s like they [employers] care more about calling themselves ‘diverse’ than about treating us daily. We are just a token.”
Participants’ examples illustrate the ways in which transmisogynoir as an SDoH was experienced by BTW in housing, accessing social services, and employment. In addition to experiencing transmisogynoir in general, it can be especially painful when this violence occurs within one’s racial community or from one’s own family. Such rejection can lead to additional factors that further threaten well-being, such as homelessness and survival sex work.
Seeking Help Within Health Care
Collectively, the sample (N = 10) reported regular and positive help-seeking behaviors: Seven participants received health care services within 3 months of the interviews, two received care within 12 months of the interviews, and one indicated that it had been over a year since she last sought health care service. Further, when asked to rate their level of comfort with health care providers, participants generally responded positively. For example, Blossom had her provider’s personal phone number and felt like she could call her “If anything happens; I feel very comfortable with her. It’s really hard to find someone that you’re comfortable with.”
While this sentiment was echoed by Cameron, Angel, and Blanca, Candy was indifferent. Despite having had both negative and positive encounters, she did not feel comfortable with any particular provider. She reported, “I haven’t had a bad experience with a provider here—I mean, I’ve had rude service at the hospital when they refused me care, but not my doctor.” Likewise, Blossom recalled a time she went in for routine testing for sexually transmitted infections and was treated by a doctor who was in a “really rough mood.” She stated, “I was probably the hundredth test he had done that day and was probably tired. He apologized and told me that he was having a bad day. I told him I understood.” Participants also reported instances in which their health care providers breached their confidentiality. For example, Cotton shared that the therapist she was seeing at a local community center “crossed the line when she was telling one of my girlfriends my business . . . [I did not report it] because I understood intentions . . . she thought she was protecting me. But she crossed the fucking line.” Relatedly, Elektra and Marci also experienced past mental health providers as unsupportive and invalidating and showing very little empathy and regard. For example, Elektra noted, [My psychiatrist] was a smack. You know he didn’t love his craft. He was in for the money—he didn’t care about my problems. He didn’t care about my ass, [the] psychological warfare [endured], mental anguish, or my disability. He will put me on psych meds that won’t help me. I was just like a guinea pig to him, and it was hurting me more than helping me.
While some participants reported a history of mental health treatment to better manage their symptoms, other participants reported that, despite the various impairments they struggle with, they have not sought professional treatment due to mistrust, fear, or lack of resources. For example, Candy noted: I’m too prideful—when I lost my mom, it was tough for me and I needed help. I started going to grief counseling and it helped a little but I didn’t stay. To be honest, I’m hurting and I’m in pain, but it’s also hard for me to trust.
Despite her fears that she “might do something stupid [harmful] in my lowest of low,” Candy decided to forgo professional interventions due to mistrust. She reported that when she’s feeling low, she conducts her own “evaluations and provide my own treatment.” Still for others, the decision to forgo therapeutic interventions was driven by shame, stigma, and internalization of the Strong Black Women stereotype. For example, Blanca expressed: I get anxious sometimes. I try not to let it bother me. When I was younger, [my mother] had anxiety all the time, and I remembered her sitting by herself sometimes and she [used] an adult coloring book for stress relief . . . my mom never sought help for anything. She took care of it all by herself [with] no complaints. I’m like that. I manage on my own.
Although they reported negative encounters, most participants reflected on at least one corrective health care experience that helped them rebuild trust in providers thereby reinforcing help-seeking behaviors. Participants described providers as knowledgeable and understanding, and, as noted by Blanca, they “asked questions and went out of their way to make sure that I understood everything.” Participants were especially struck by the professionalism exuded by providers with limited experience working with transgender women. They were described as communicative and proactive in their attempts to create a safe space. Cotton recalled overhearing her health provider outside of the examination room. “I will never forget that man. He was preparing himself to try and take the little time, the little gesture to get to know how to communicate with me . . . most doctors won’t do it. They have a tendency to misgender you.” Last, as illustrated by Marci, having knowledge of the transgender community also contributed to participants’ overall positive experiences. Marci noted “From the first encounter, he was very knowledgeable about the LGBT experience. He knew that there were things within my community that the straight community didn’t go through.”
In the context of access to health care as an SDoH, participants demonstrated a willingness to engage with health care systems, despite negative encounters. While most had received health care in the past year, participants provided information on various barriers to help seeking including mistrust, stigma, invalidation by providers, and lack of resources that hindered access to high-quality/affirming health care. Participants also provided examples of what helped them re-establish trust in providers such as showing an understanding about the transgender community, including not misgendering patients.
Discussion
Despite widespread evidence of discrimination, violence, and health disparities experienced by BTW, they are rarely centered in research studies (James et al., 2017). To this end, our study explored themes of transmisogynoir as a unique intersectional minority stress impacting the well-being of BTW. Results showed the unique themes surrounding mental health, SDoH, and help seeking in the context of health care for BTW. Importantly, the SDoH framework illuminated the important role of the context in which BTW exists. Despite being highly educated, the BTW in this study faced poverty and unstable housing.
The results from this study highlight that BTW experience mental health challenges (e.g., depression, anxiety, PTSD, psychosis, suicidality, and mania). Indeed, these results are consistent with the U.S. Transgender Survey, which found high rates of mental health issues associated with gender minority stress (James et al., 2017). Participants in this study spoke of past traumas that they believe had lasting impacts and ongoing challenges that impacted their well-being, consistent with the broader transgender literature (Hereth, 2021). Substance use was one way that was utilized to cope with symptoms of mental illness. They also indicated that they sought mental health services but sometimes faced barriers including not being able to prioritize their well-being.
Experiences of intersectional discrimination have been linked to SDoH (Beltran et al., 2019; Glick et al., 2019). Participants reported that intersectional minority stress shaped their access to housing, employment, and medical care. Unfortunately, participants faced gatekeepers who prevented them from accessing resources such as food at a homeless women’s shelter. They also described experiences of discrimination that impact their ability to stay employed or to secure housing. Using an SDoH framework to consider health disparities in BTW helps us to see the importance of dismantling systems of oppression. Advocacy for housing, employment, and legal protections can improve BTW well-being (Glick et al., 2019).
Many of the BTW in the present study described experiencing rejection, discrimination, and violence from within their cultural groups. As an SDoH, these experiences of marginalization seemed to negatively impact their well-being. Mistreatment is experienced by BTW in spaces that ostensibly should provide safety and support. It is important to consider how this feeling of distrust toward one’s racial group can act as a barrier to support. BTW also experience rejection and violence from their own families, which causes trauma and creates vulnerability. Research shows that family support is a protective factor for transgender women (Jin et al., 2020).
Findings from our study point to the importance of environmental conditions as SDoH that negatively shape the well-being of BTW, like institutional oppression and discrimination as intersectional violence. Participants in the present study described negative experiences such as being refused care at a hospital and receiving rude treatment from health care providers. Participants also reported negative experiences with mental health care providers who breached confidentiality or were uncaring. While the findings from the present study focused on health care, previous research points to other oppressive institutions, such as schools, churches, and the criminal justice system, that BTW navigate (James et al., 2017).
Cumulative victimization has been identified as a barrier to help seeking in a study of mostly non-BTW (Hereth, 2021). Despite the negative experiences, participants also reported engaging in help-seeking behaviors. Most participants in this study reported receiving regular health care. Several participants reported positive relationships with their health care providers, which likely contributed to their ongoing engagement with health care services. Participants expressed appreciation for health care providers who asked questions instead of making assumptions, demonstrated some knowledge of the transgender community and practiced using correct language to not misgender their patients. These small gestures by health care providers do not go unnoticed and facilitate access to quality/affirming care. Many of our participants indicated that they notice and appreciate when providers make efforts to engage them as BTW.
Practice Implications
Current study findings have practical implications for health care practitioners. One way that health care practitioners can address experiences of intersectional violence is by integrating trauma-informed care into their work with patients (Substance Abuse and Mental Health Services Administration [SAMHSA], 2014). More specifically, a trauma-informed care framework can incorporate feminist theory to address the traumatic experiences of violence rooted in transmisogynoir that BTW face (LaMartine et al., 2023; SAMHSA, 2014). Moreover, given the intersectional violence reported by BTW, it is vital for interventions to address this directly. One example of this type of intervention was developed by Logie et al. (2019) with the help of African, Caribbean, and BTW in Canada, aptly named the TRANScending Love (T-Love), a non-pathologizing arts-based workshop that provided participants with the opportunity to share their experiences toward acceptance and feel connection and solidarity with other transgender women of color.
Given the myriad of negative experiences BTW have with health care and other systems, it is not surprising that there is distrust. This distrust is protective, yet it can also create more barriers to accessing quality care and delay in treatment. It is incumbent on health care providers to reduce barriers within the health care system in order to promote trust for gender-diverse persons. A practical example of this is the Trans Buddy Program, which provides referral lists of transgender-competent providers and accompaniment to appointments (Santora, 2021).
Research Implications
There are substantial issues with the lack of representation of transgender women in medical research outside of mental and sexual health (Chan, 2019); however, this invisibility is even greater for BTW. Often, BTW are characterized as “hard to reach populations” (Everhart et al., 2022). Yet BTW are not a “hard to reach population” if researchers connect with community organizations and engage in practices that are conducive to building trust for BTW that allow them to feel safe to share their narratives, including the strategies presented in this study. Moreover, for BTW, particularly those living with HIV, direct clinical services may be prioritized over research, given chronic psychosocial stressors (Everhart et al., 2022). Relatedly, there must be a representation of BTW in research (LaMartine et al., 2023; Santora, 2021).
Advocacy and Policy Implications
Findings from the current study have direct implications for advocacy and governmental policy that includes BTW. Using a community-informed approach, the Arming Minorities Against Addiction and Disease (AMAAD) Institute created the Black LGBTQ+ Action Coalition to understand and give voice to Black LGBTQ+ persons throughout Los Angeles County (AMAAD Institute, 2018). As part of the Community Advisory Board, Black LGBTQ+ community members were included to provide feedback to the L.A. County Department of Mental Health on the mental health needs, challenges/barriers, cultural strengths, inclusive spaces for Black LGBTQ+. Regarding legislation, California Assembly Bill (AB) 2521, or the Transgender, Gender Nonconforming, or Intersex Fund (California Legislative Information, 2022) earmarks dedicated funds for these communities to address several SDoH by providing funding to local community-based organizations focused on addressing these issues for transgender, gender nonconforming, and intersex persons, including for BTW. Moreover, California has established a LBTQ Health Equity Initiative, where funding is provided to organizations who serve LBTQ, including BTW, to address health inequities (California Department of Public Health, 2022).
Limitations and Future Directions
There are several limitations to this study. This study was originally conceptualized to focus on the experiences of transgender women of color, broadly rather than focusing specifically on BTW. As a result, the questions were not tailored to capture the unique experiences of BTW. Future research should collaborate with BTW from the early phases of study design. Additionally, researchers should be intentional in recruiting BTW participants and carefully craft interview protocol questions that specifically explore the experiences of BTW. We did not examine the vital role of resilience from these experiences of violence, as emerging data show that community building with LGBTQ+ communities of color helps foster resilience for BTW (Stone et al., 2020). Future studies should document how specific sources of resilience (i.e., individual, community) are related to themes of intersectional violence and well-being in BTW. In addition, future studies should include questions specifically about physical health to provide a more complete understanding of SDoH for this population.
Another limitation was the institutional constraints around how much participants could be paid. The lead researcher balanced compensating participants for their time and maintaining confidentiality by not increasing the honoraria amount, as this would require a tax form from participants. Therefore, future directions for researchers include understanding that unique SDoH exist that BTW face that should be accounted for prior to the design and implementation of a study, as these SDoH may impact data collection (e.g., fair compensation, transportation, and housing). Additionally, there are nonmonetary ways that researchers can demonstrate reciprocity to communities that they research, such as bringing the findings from research back to the community and providing services that directly benefit the community. In the context of this study, the lead author plans to collaborate with a community partner to carry out a needs assessment and intends to disseminate the current findings through presentations to community leaders.
Footnotes
Appendix
Authors’ Note
This project would not have been possible without our participants, the coding team (Matthew Alcala, Giselle Gomez, and Cassandra Lloyd) and community partners (especially Jazmunn Nichcala Crayton) who led to the success of our study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.