
Abstract
Behavioral health crises among youth are increasing, and schools are well positioned to decrease use of Emergency Rooms and increase access to community-based care. Mobile crisis intervention (MCI) teams have been shown to reduce rates of hospitalization and strengthen connections with community-based resources. Yet, there are few studies examining the lived experiences of families and professionals engaging in inter-agency collaboration, specifically regarding proactive efforts in crisis situations. Using framework analysis, researchers coded and contrasted various perspectives to identify practice interventions. Using snowball sampling recruitment methods, focus groups were conducted with school-based behavioral health providers (n = 12), MCI clinicians (n = 4), and caregivers (n = 14) to elevate the voices of individuals most frequently involved in MCI. Participants, who mostly self-identified as White from one Northeastern state, engaged in recorded interviews that were coded and contrasted using framework analysis. This step-by-step analysis of qualitative data collects themes, compares findings from different participant groups, and organizes information in a matrix format. Though the interview sought to identify strengths and challenges, two overarching themes were identified: (a) systemic facilitators and barriers, and (b) interpersonal facilitators and barriers. Categories and subcategories were also identified, providing deeper insight into participants’ experiences. Results demonstrated a need to forge and improve connections between mental health MCI and school-based teams. Practice, research, and policy implications are addressed to better meet the needs of youth and families by providing high-quality, timely, integrated, and comprehensive emergency services.
Introduction
Recently, the number of youth experiencing behavioral health crises has skyrocketed (Krass et al., 2021; Leeb et al., 2020). Kalb et al. (2019) identified a 28% increase in pediatric emergency room (ER) visits for mental health challenges, with even larger increases among adolescents (54%), African American (53%), and Hispanic patients (93%). Across the nation, ERs are not equipped to meet the rising needs of youth in crisis. While youth with behavioral health emergencies spent about 3 hr in the ER, only 16% were seen by a mental health professional (Kalb et al., 2019). ERs are often “characterized by a lack of privacy, overstimulating environments, exposure of patients to other psychiatrically and medically ill individuals,” contributing to detrimental conditions for youth (Hoge et al., 2022, p. 1226). These problems were exacerbated by the COVID-19 pandemic. In 2020, ER visits for mental health had increased by 24% for school-aged youth and by 31% for adolescents (Leeb et al., 2020). The pandemic increased youth utilization of the ER for mental health needs, which highlighted pre-existing barriers to adequately treating youth in crisis. The small number of pediatric patients seen by mental health providers in the ER, compounded by adverse ER settings which are potentially harmful to youth, emphasize the need to explore alternative options for youth in crisis (Hoge et al., 2022; Kalb et al., 2019).
Mobile crisis intervention (MCI) is a community-based, multi-disciplinary service that provides coordinated response to youth in crisis due to behavioral health needs as well as coordination and referrals with local community providers and has been shown to reduce hospitalizations (O’Brien & Gulley, 2022). MCI offers in-person, crisis intervention and support for youth experiencing psychiatric emergencies in their home, school, or other community setting that is available 24 hr/day, 7 days/week. They offer in-person support across multiple settings (i.e., home, school, community settings, daycare, etc.). MCI services are state-sponsored, with the goal to provide stabilization and de-escalation care in the form of risk assessments and safety planning, as well as connect families with referral to community services (CBHI, 2015). When a youth is having a behavioral health crisis at school, the staff can call for assistance, and mobile crisis clinicians will come to the school buildings to provide in-person support. This can look like performing a risk assessment, de-escalating a student, transporting them to the ER, and/or making an appropriate referral (e.g., to inpatient hospitalization, outpatient therapy, etc.). Overall, the literature establishes MCI as an incredibly effective intervention that also acts as a preventative mechanism for hospital visits (Fendrich et al., 2019). Some findings indicate that MCI is rated favorably by family members of those in crisis, and that 74% of MCI clients felt better able to cope with future crises (Ligon & Thyer, 2000; Vogel-Stone, 1999). MCI has been shown to reduce healthcare costs, ranging from 23% (Scott, 2000) to 79% (Bengelsdorf et al., 1993), by decreasing the use of more intensive services. Moreover, mobile crisis also provides a successful linkage to after-care for suicidal patients 70% of the time, compared to 30% of patients who were not using MCI (Currier et al., 2010).
Most calls to MCI for youth relate to risk for suicide or harm to self (Alexander & Zealberg, 1999; Goldman, Looper, et al., 2023) and involve adolescents rather than younger children (Vanderploeg et al., 2016). The expected outcomes of MCI include minimization of police involvement and unnecessary use of force, appropriate utilization of ER, cost savings, stigma reduction, care coordination between agencies, early identification and prevention of illness, and accessibility (Martin, 2005; Zealberg et al., 1993). The benefits of MCI can also improve services within educational settings, as pediatric psychiatric ER visits are most likely to occur during the school day, and often relate to stressors within the school context (Soto et al., 2009). Studies have shown that schools are more likely to inappropriately refer students to the ER, with almost half of referrals considered “avoidable” (Grudnikoff et al., 2015; Holder et al., 2017; Soto et al., 2009), and as only one out of ten school risk assessments lead to hospitalization (Crepeau-Hobson, 2013). These advantages are most noteworthy for ethnically and racially diverse youth living in poverty with ongoing behavioral health concerns. A recent review by Oblath et al. (2022) identified that 95.6% of the youth who encountered MCI services were publicly insured, were existing patients (60.2%), and were from ethnically and racially diverse backgrounds (37.9% involved Black youth, 26.2% with Latino youth, and 17.7% with White youth).
Community Collaboration at the Mesosystemic Level
Schools play a particularly important role in mental health service delivery for youth, as the majority of children receiving services occurs within the school setting, and this finding has been corroborated through studies and meta-analyses for more than 25 years (Bradshaw et al., 2008; Duong, et al., 2021). Studies have also shown that 40% of all youth mobile crisis referrals are made from schools, though schools are more likely than outpatient clinicians to inappropriately refer students to the ER (Fendrich et al., 2019; Grudnikoff et al., 2015; Hoge et al., 2022; Holder et al., 2017). Thus, a partnership between districts and MCI agencies is critical and highlights the need for effective cross-sector collaboration. Yet, many systemic efforts tend to focus on the individual navigating one organization, while children and families bridge multiple organizations across systemic levels within the ecological framework (Bronfenbrenner, 1977, 1979). Each layer of the ecological system influences the individual, and the relationships within the systems generate reciprocal and ever-changing influences on a child’s social, behavioral, and academic development. Thus, the individual is greatly influenced by those at the closest, microsystemic level, such as family, peers, teachers, etc., as they have direct interaction with the person. Interactions at the mesosystemic level involve relationships between community agencies, such as educational institutions and health services, and community-based partnerships that bridge these levels can support students in need of behavioral health services, decrease problem behaviors, and improve adaptive functioning within the school environment (Pearrow et al., 2021). However, on a systems level, collaboration between school and community providers can be challenging due to variable funding mechanisms, oversight, training programs, privacy and confidentiality concerns, and licensing (Doll et al., 2017). Nonetheless, together, MCI and districts have the potential to meet the needs of children and families in crisis by providing high-quality, timely, integrated, and comprehensive emergency services.
The current study seeks to advance the research by focusing on the collaboration between districts and MCI agencies and highlights the lived experiences of caregivers, school staff, and mobile crisis clinicians navigating emergency crisis response (i.e., MCI). The investigation occurs in the context of the state’s mental health system procedural efforts to enhance access to MCI teams and community-based supports as a strategy to reduce boarding of youth in crisis. As such, research questions included the following: (a) What are the current strengths of MCI and school team collaboration? (b) What are the current challenges of MCI and school team collaboration? (c) What do community members view as best practices for MCI and school team collaboration? Findings will examine policy implications as well as generate recommendations for tools and resources that can enhance partnerships across agencies.
Method
As the current study was conceptualized as a descriptive examination of youth mobile crisis practices, a qualitative study process was determined to best meet the objectives to understand the challenges and opportunities from the perspective of those most impacted. As such, participants from various roles and agencies, as well as the caregivers of these youth, were recruited and interviewed to explore their experiences with mobile crisis, and with one another before, during and after mobile crisis intervention.
Participants: Setting and Recruitment
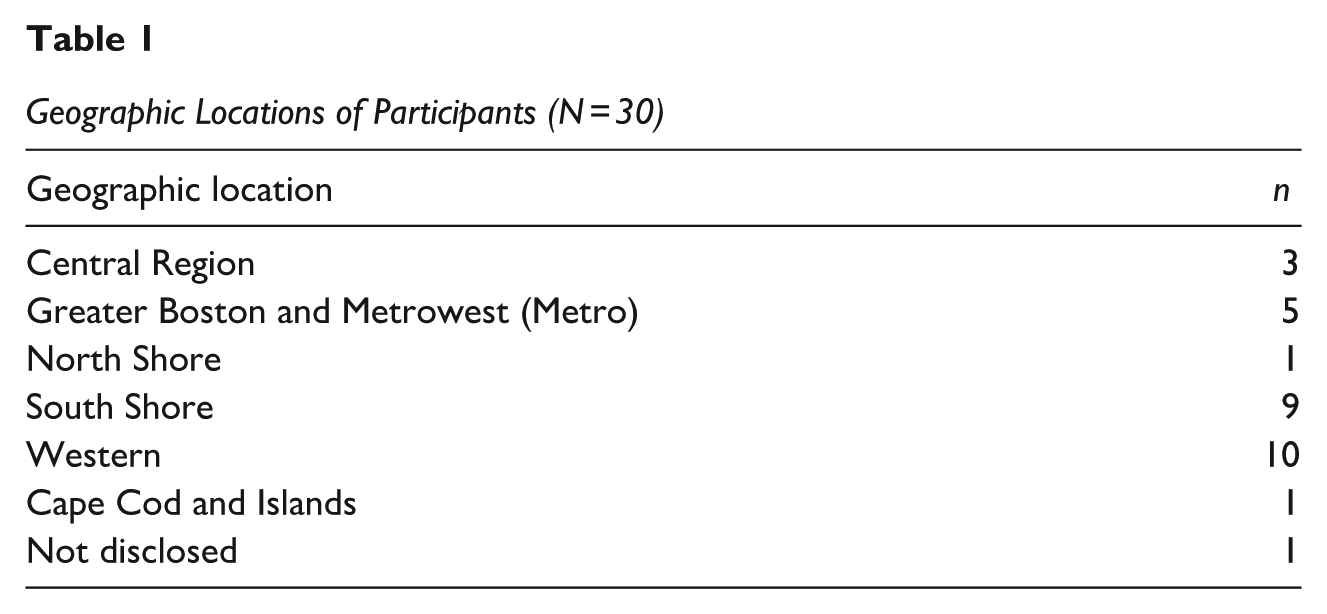
Participants included 30 mental health professionals and caregivers, and more specifically, individuals identified as school-based professionals (n = 12); MCI providers (n = 4), and caregivers (n = 14) from a Northeastern state in the United States. To be eligible, participants had to have relevant firsthand experiences supporting youth in crisis, such as MCI provider, school-based professional, relative of a youth who received services, and/or school or community leaders. Please see Table 1 for geographic representation of participants, and Table 2 for demographic characteristics of the participating school districts and their accompanying communities.
Geographic Locations of Participants (N = 30)
Demographics of School Environments (N = 12)
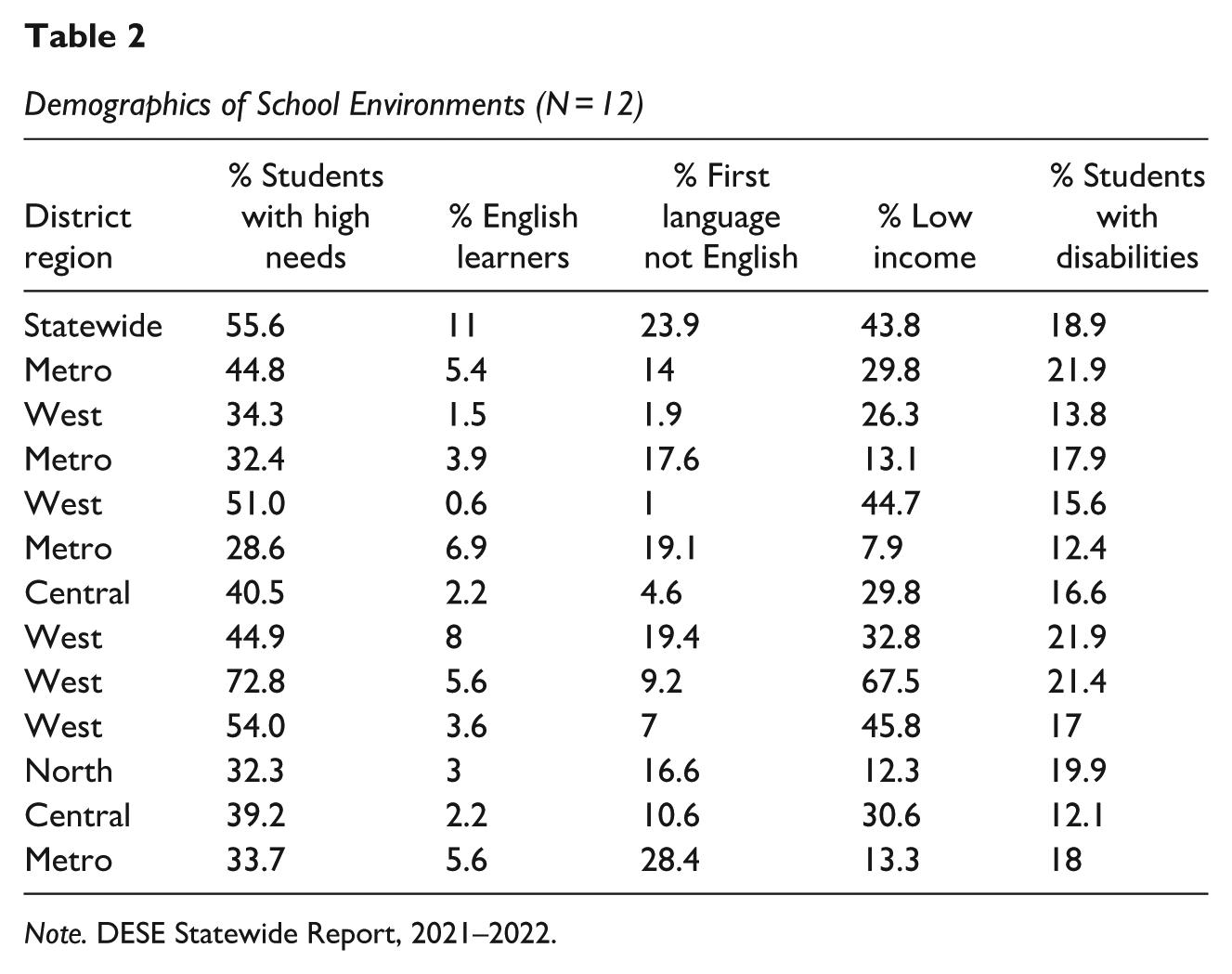
Note. DESE Statewide Report, 2021–2022.
School- and community-based professional participants were engaged in a number of roles across the two agencies, such as school social workers/adjustment counselors, school psychologists, district-based clinical director, and youth mobile crisis directors, and nearly every participant identified as White. One-third of the participants had between 7 to 10 years of experience, and half had more than 10 years of experience. Other participants had varied roles in schools, districts, or MCI agencies, and all were directly involved in crisis response. Overall, as demonstrated in Table 2, participants worked in communities that are diverse in race, ethnicity, language spoken, and socioeconomic status including rural, suburban, and urban (Massachusetts Department of Elementary and Secondary Education, 2022). Caregivers came from a range of regions and had experiences with seven different MCI organizations.
Modified snowball sampling was employed to recruit participants with efforts to ensure state-wide representation. Recruitment flyers sought individuals available for a 60- to 90-min interview or focus group to speak about their personal experiences related to mobile crisis response. Based on accessible networks, research team members generated a list of professional contacts and disseminated recruitment flyers to 44 individuals and agencies, including school-based behavioral health providers, special education directors, administrators in public, private, and regional school districts, state agencies, and nine statewide professional listservs. Flyers were also shared with a state-wide parent advocacy group that regularly interfaces with caregivers of children with behavioral health needs. Those contacted were invited to participate as well as share recruitment materials with their professional networks.
Data Collection Procedures
The individuals who responded to the recruitment efforts were asked to complete a brief screening form to ensure that they had first-hand experience of MCI/school collaboration. All participants who completed this form met eligibility criteria and were invited to participate in a semi-structured focus group and asked to “Describe your encounter with MCI crisis teams” to ensure appropriateness for participation. The protocol was developed based on previous research and was designed to elicit information about participants’ personal experiences pertaining to the strengths, challenges, and areas of growth for collaboration among school and MCI teams, specifically towards revealing appropriate proactive steps for improving collaboration. The protocol was shared with experts in the field, potential participants, and a parent advocacy organization to obtain feedback. In addition, questions were independently edited by multiple members of the research team to ensure clarity.
The protocol was organized into sections: strengths (i.e., best things about collaboration with MCI/schools), challenges (i.e., biggest challenges working with MCI/school crisis teams), hopes (i.e., most important practices for effective collaboration), and needs (i.e., training needs). The semi-structured protocol allowed for the researchers to ask follow-up questions when appropriate to enhance the breadth and scope of the discussion (Adams, 2015). All focus groups took place via Zoom and were conducted by two research team members: one notetaker and one facilitator. With consent, the focus groups were recorded and later transcribed verbatim to ensure accurate representation of interview content. Participants also received a small gift card of compensation.
In addition to the utilization of reflexive practices (discussed below), the following methods were employed to ensure credibility of current findings (Brantlinger et al., 2005). Multiple investigators independently coded data to ensure triangulation, as well as consistency across participants and focus groups. Discrepant cases were analyzed and addressed in debriefing sessions and ultimately were identified as outliers or incorporated in the analysis. All findings were shared with participants, who were invited to share their feedback. Collaborative work and peer debriefing were employed, with extensive documentation of all research activities.
Data Procedures With the Framework Analysis
Framework Analysis is an applied research technique that provides a step-by-step process for analyzing qualitative data thematically, comparing findings from different participant groups, and presenting information in a matrix format to be applied in practice (Goldsmith, 2021; Ritchie & Spencer, 1994). This structured—yet flexible—approach has two aims (a) to create an analytic framework informed by careful analysis of themes identified within the data and (b) to apply the created analytic framework to address the identified themes (Goldsmith, 2021). Framework analysis was chosen for the current project due its focus on applied research questions aimed at improving practice and policy, comparing themes from diverse participant groups, and its highly structured nature. Notably, this allowed researchers to actively listen to participants, rather than limit themselves to investigating hypotheses; thus, limiting potential biases. Below is an explanation of each stage of framework analysis, and this is followed by applying the stages to the interviews collected from this study.
According to Goldsmith (2021), the process consists of five stages, beginning with familiarization, where researchers review all data and record key ideas and major themes. This step includes reading transcripts and making a table with key themes and sample text associated with each stakeholder group. In the second stage, the researchers identify themes for the analysis and identify abstract concepts, which can include both major themes, concepts, and subcomponents which elaborate more specifically on these major themes. In the indexing stage, the framework is systematically applied to all the study data, and the original framework may be revised until all data are included in the framework. In the fourth stage of charting and summarizing, matrices of the data are developed, using rows and columns to represent different participant groups and framework components. In the final stage of interpreting and mapping, researchers describe emergent patterns and compare key learnings from earlier steps and make comparisons across participant groups and themes.
In the familiarization stage, research team members individually reviewed all data and recorded key ideas and major themes. This method allowed for the identification, comparison, and interpretation of themes in relation to both research questions and study participant narratives (Goldsmith, 2021). More specifically, the initial familiarization stage consisted of each of the researchers individually reviewing all transcripts and creating a table containing key themes and sample text associated with each participant. In the second stage of identifying themes, researchers compared each table to create a framework for the analysis and interpretation by comparing abstract concepts in a systematic manner. More specifically, each individual researchers’ themes and quotes were reviewed until agreement was reached on major themes, concepts, and subcomponents. In the indexing stage, the framework was systematically applied to all the study data, and the original framework was revised until all data were integrated. In the charting and summarizing stage, all participant quotes and themes were accounted for in a comprehensive matrix organized using rows and columns to represent different participant groups and framework components. All textual data (i.e., quotes) associated with each cell were summarized. In the interpreting and mapping stage, researchers described emergent patterns, compared key learnings from earlier steps, and made comparisons across participant groups and themes (Goldsmith, 2021).
Researcher Reflexivity and Credibility
Over the course of the project, the research team consisted of two faculty advisors and five doctoral students, all of whom identified as cisgender, White females. The first author was a third-year doctoral student in counseling psychology, motivated to research this topic based on her experience as a special education teacher collaborating with MCI providers and her clinical work with youth and families in crisis. Authors held a range of experiences in school and counseling psychology at the doctoral level, practicing in school-based, community-based, and clinical environments. The positionalities, identities, and experiences may have impacted the team’s approach to this research, and they shared an ongoing commitment to the process of critically examining personal biases as it relates to this work. The authors were part of a graduate program grounded in the scientist–practitioner model, with public-health and equity-driven approaches.
Results
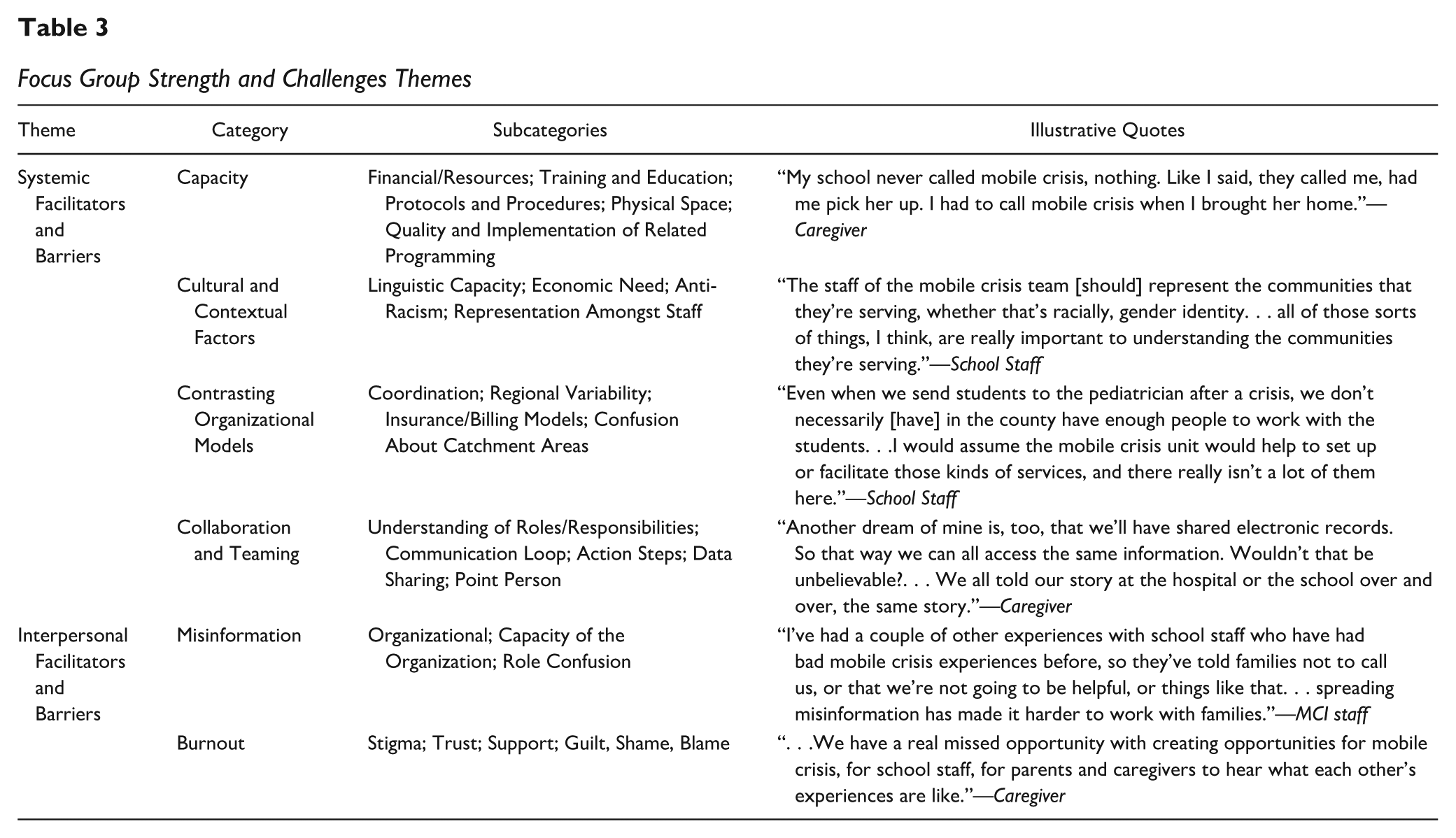
The framework analysis yielded two overarching themes of strengths and challenges, particularly as they relate to systemic and interpersonal barriers and facilitators of collaboration. Though questions specifically sought strengths, most of the discussions focused on the hurdles and barriers to partnerships across the education and emergency response systems. In this section, the primary headings reflect the themes, and the subheadings demonstrate conceptual categories that are more specifically defined in the subcategories. A detailed overview of findings can be found in Table 3.
Focus Group Strength and Challenges Themes
Systemic Facilitators and Barriers
Capacity
One facilitator of collaboration was the capacity of partners, such as the resources, training, and office space, as both school and mental health staff had varying procedures and preparedness to work together with youth in crisis. With few examples, the school personnel stated that MCI teams are voluntary, have good documentation practices, and that MCI clinicians arrive during school hours to support in handling a crisis. MCI providers indicated that collaboration and prevention efforts help mitigate crisis risk, particularly if there are established relationships across agencies. For caregivers, the benefits of having the MCI help connect families with resources in the community and supports throughout the crisis process was highlighted, as well as their accessibility across the state.
In contrast, school and MCI providers discussed the barriers and limited bandwidth, availability, and expertise of behavioral health personnel trained to respond to crises. Caregivers reported difficulty accessing services across the state. In terms of physical capacity in school buildings, school personnel expressed lack of space to privately engage in crisis evaluation. Caregivers and school staff emphasized the need for increased capacity of clinicians in trauma-informed care, crisis protocol implementation, and broader understanding within schools about community-based crisis services. One mobile crisis team member stated: “I think having an opportunity to educate schools and school staff is a lot of them . . . . So if a kid makes a disclosure to a teacher, that teacher might think, ‘Oh, I need to call 911’. Rather than thinking, ‘Oh, there’s this other service where we might not have to deal with the trauma of an ambulance ride or the hospital and people showing up in uniforms.”
In terms of capacity following crises, caregivers expressed confusion and overwhelm regarding the re-entry process (i.e., student returns to school after an MCI encounter). They highlighted schools’ failure to implement safety plans, insufficient follow-up at school, and a lack of timely and meaningful communication with the school. Finally, MCI providers and school personnel expressed confusion about schools’ differential capacity to provide general education behavioral health supports and special education services.
Cultural and Contextual Factors
Several subfactors that connected youth to the context and cultural capacity of school- and community-employed providers, such as linguistic capacity, anti-racism efforts, and representation, were identified by participants. Across caregivers, school personnel, and MCI providers, there were overarching concerns emphasizing a lack of multilingual providers, and a dearth in available interpreters to support families. This prevented families, whose primary language was not English, from accessing services, resulting in increased stress. Caregivers and MCI providers discussed barriers to services including financial constraints, insurance, and geographic access. These factors created challenges to collaboration as it compromised providers abilities to effectively comprehend and assess the youth in the school context.
All participants suggested the need for providers to be trained to appropriately engage with students of diverse racial, ethnic, linguistic, and socioeconomic backgrounds. One school team member stated: “something very important. . .is that the staff of the mobile crisis team represents the communities that they’re serving, whether that’s racially, gender identity, all of those sorts of things are really important to understanding the communities they’re serving.”
Contrasting Organizational Models
The educational and mental health systems serve differing functions for the community, and as such, participants expressed a lack of collaboration, communication, and understanding of the role of each organization in responding to crises. Participants expressed varying experiences across different areas, including varied response times depending on region, differences in degree of MCI outreach, and variation in community resources’ availability (i.e., hospital beds, follow-up services). One school team member shared: “A lot of times [mobile crisis] takes a bit longer than the emergency services. . .If we call the crisis unit, they say they will be there in four hours. It’s 2:00. School ends at 3:00.” In terms of insurance and billing models, school teams explained that they may not be immediately aware of a student’s insurance status, which can affect a student’s access to higher levels of care and whether MCI can conduct a full evaluation. Finally, caretakers noted confusion about catchment areas, or geographic regions served by MCI teams and community mental health, and whether or not they align with the geographic area of school districts. Both school teams and MCI providers explained the difficulties that ensue when students in the same school district have different MCI providers.
Collaboration and Teaming
MCI teams indicated that a strength was when schools communicated beforehand and provided triage information sheets on children coming their way. This is one of the few strengths identified in the collaboration theme. Rather, confusion was reported about the differential roles and responsibilities of school providers, MCI providers, and caretakers. Caretakers described not knowing when MCI teams are called. School teams expressed confusion about the role of MCI versus their role, as well as roles within school and district teams when calling MCI. Similarly, MCI providers explained misunderstanding the schools’ challenges implementing their recommendations. Participants shared that communication seldomly occurs in a collaborative and proactive manner. One school staff member shared: “It would be nice to know, if I send [a child] out, what the recommendation was. . .it’s nice to hear that clinical opinion of, ‘Hey, this is why I made that decision.’ That way, when we’re working with the family again, we can help them through all of that.” Furthermore, school teams shared that it is unclear who is responsible at each point in the MCI encounter.
Fragmented data-sharing was also reported particularly as each agency has access to different information and guidelines around confidentiality. Caregivers highlighted that they must share their story repeatedly due to gaps in communication between providers, while both MCI and school professionals shared that it is unclear which information can and should be shared. One MCI provider stated: “The more information we have, giving us alerts and updates and having us come to meetings and really just getting us involved before we get to that point of total meltdown is really helpful for us.” All participant groups expressed a need for an appointed person to be a liaison to cultivate improved communication and mutual knowledge across systems while also remaining attuned to the parameters of confidentiality.
Interpersonal Facilitators and Barriers
MCI providers identified facilitators that collaboration and prevention efforts help mitigate crisis risk, particularly if there is an established relationship between providers across agencies. Moreover, caregivers indicated that across agencies, clinicians work well with children actively in crisis and advocate on behalf of families’ needs. However, the majority of participants focused on heightened interpersonal conflict, most often arising due to misinformation among providers and caregivers and contributing to high levels of burnout and staff turnover.
Misinformation
Inaccurate information, based on previous experiences or lack of updated training, leads to confusion on each agency’s procedures and services. School teams reported misunderstanding about the breadth of MCI services, and how MCI functions in terms of billing, funding, and insurance, which results in interpersonal conflict. Meanwhile, MCI providers often misunderstand the chain of command in schools, special education processes, availability of mental health resources, and family communication procedures. Providers described unclear delineation of responsibilities (i.e., calling families, following up, sharing data, etc.). This uncertainty related to funding streams, roles and responsibilities, and the availability of resources breeds interpersonal conflict, resulting in a lack of collaborative efforts and an increase in the sharing of negative experiences. As demonstrated by the clinician quote below, this leads to families not accessing or utilizing MCI services and discord between professionals.
Burnout
Participants discussed how stigma, lack of trust and support, guilt, shame, blame, and rigidity lead to the emotional toil of crisis response and burnout of providers and caregivers. Caregivers reported that schools often perpetuate stigma by not calling MCI, blaming caregivers for their children’s challenges (one participant commented “mental health problems are not parenting problems”), and faulting caregivers for not following through on recommendations and referrals. Meanwhile, the impact of this blame is cyclical, leading caregivers to share incomplete and disparate information with providers.
Caregivers described general lack of trust regarding providers’ competency due to failed interactions and not feeling supported in their own trauma. One parent discussed her child’s school team: “I was getting phone calls every afternoon about how they couldn’t handle [my child]. But they weren’t calling [mobile crisis]. They’re [school professionals] not trained in it [community-based crisis response resources]. . .it’s a lot of stress on a parent.” MCI providers similarly highlighted their frustration when families and schools challenge their decisions. School providers and MCI providers alike reported needing increased support from one another in facilitating follow-through, instead of the blame that so often arises (i.e., school providers blaming individual MCI providers for slow response time, etc.).
Finally, interpersonal rigidity was addressed by all groups of participants. Caregivers expressed the desire to be taken seriously by MCI providers. School providers shared that it can be difficult to change perceptions of MCI after negative experiences, and both school and MCI teams shared rigid thinking patterns (i.e., our organization is doing things “right” and our partner is doing things “wrong”). Overall, a lack of rapport between partners appeared to perpetuate blaming and burnout, thus deterring collaboration, as research has demonstrated that burnout by providers is associated with impaired emotional and physical health, a diminished sense of well-being, increased rates of anxiety, depression, sleep and memory problems, and ultimately, absenteeism and turnover (Morse et al., 2012).
Discussion and Implications
Aforementioned, the goal of this research was to uplift the voices of the partners most frequently involved during a mental health crisis event: mobile crisis clinicians, school professionals, and parents. When using a framework analysis approach, focus group findings highlighted two major categories of strengths and challenges to effective collaboration: (a) systemic facilitators and barriers and (b) interpersonal facilitators and barriers. Broadly, strengths were frequently bypassed in discussions with the focus shifting to systemic and interpersonal barriers, included contrasting organizational models, capacity, cultural and contextual factors, and teaming-related factors. Interpersonal barriers and supports included facets of relational interactions among involved parties. Participants frequently cited interpersonal conflict, largely due to misinformation and burnout. Implications include the need to formalize and strengthen proactive partnerships between MCI and school-based teams. Pre-crisis, during-crisis, and post-crisis procedures should be solidified, and mechanisms for increased leadership, communication, and data-sharing can ensure seamless communication. Achieving these goals may enable increased access to services for students and families, decreased involvement of emergency rooms and law enforcement, and time and cost savings for both organizations. To that end, researchers of this study developed an emerging toolkit based on identified themes and resources shared by participants. The efficacy of this toolkit will be examined in future research. Focus groups reinforced the pre-existing consensus that schools are under-equipped to handle crisis procedures; therefore, there is a call upon MCI providers to aid schools in maneuvering crises. The focus groups underlined barriers to MCI implementation and included implications for the school mental health field. As noted by Goldman, Ponce, et al. (2023), there is a need for standards in the face of contextual variability, and MCI programs need flexibility to adapt their services to best fit their population’s needs, physical environment, system components, financing mechanisms, and many other factors. With recognition of challenges, adaptations, and the continuation of exploratory research, gaps within literature and practice will be addressed. Below, we briefly discuss several of the identified policy and practice implications for immediate consideration.
School Providers and Administrators
Schools have a responsibility to support the health and well-being of students, which includes ensuring school staff are aware of crisis procedures (Bradshaw et al., 2008). One of the most striking results from the focus groups was that many school personnel reported feeling under-equipped to properly implement crisis protocols due to capacity limitations and lack of knowledge. District administrators and school leaders could provide training for school staff that involves necessary information about supporting students in crisis and collaborating with MCI.
Additionally, participants indicated that school crisis response teams should be formed prior to the start of the school year, and team members should be aware of their individual and collective responsibilities during crises. School providers may also benefit from pre-determined communication guidelines and scripts for partnering with all parties involved (i.e., language use when contacting families, information pertinent to share with MCI). Additionally, district administrators might address capacity and training concerns by allocating funds and adopting policies for mental health services for their students (U.S. Department of Education [USDOE], 2021).
MCI Providers and State Agencies
MCI providers largely reported capacity-related challenges and contrasting organizational models as major areas of difficulty. Increased funding could improve MCI providers’ capacity to serve more individuals at a faster pace, while concurrently reducing rates of burnout among providers (Substance Abuse and Mental Health Services Administration [SAMHSA], 2022). State agencies could develop guidelines that delineate the responsibilities of MCI providers before, during, and after crises in their partnerships with schools and caregivers. Additionally, state agencies might require school leadership and MCI leadership to meet annually to discuss crisis protocols, agree on communication and data sharing guidelines, establish relationships among respective providers, and provide information about organizational processes.
Improving Collaboration
The implementation of policies and practices at the state and district levels that address barriers to collaboration will be essential to improving MCI and school team partnerships. In Connecticut, there has been a statewide push for schools and MCI providers to sign a Memorandum of Agreement (MOA) to formalize their partnerships. These MOAs are signed by a school administrator and the leader of the MCI clinic, detailing roles and responsibilities including response time, development of crisis plan, expectations regarding communication, and providing space in the school. Providers in Connecticut report high levels of acceptability with this practice, though referrals to MCI continue to vary by school (Dubuque-Gallo et al., 2022). Continued refinement of these agreements are necessary, but formalization of collaboration is a strong foundational step.
School and MCI providers also identified a need for a designated team member at each agency to act as liaison between the school and MCI teams. These liaisons would act as the spokesperson for their respective teams and engage in both proactive and reactive communication. The school-based liaison could also be responsible for following up with caregivers post-crisis, and ensuring MCI recommendations for supporting the student in school are implemented properly. The MCI-based liaison might attend school meetings, collect triage sheets on high-risk students, and provide consultation and resources to help schools better support students with mental health concerns. These liaison personnel would be another product of formalized partnership and thereby improve accountability across systems.
Limitations and Future Directions
As with all research, there are limitations with this study and its findings. This particular study took place in Massachusetts and therefore, some findings may not be generalizable to other geographic areas. Focus groups were held in the summer of 2021, after the nation had experienced a global pandemic; thus, some participants’ perspectives may have been strongly impacted by the pandemic and co-occurring rises in youth mental health concerns (Kuntz, 2022; Murata et al., 2021). Another limitation included the dearth of prior research evaluating the effectiveness of MCI services for youth and the collaborative efforts between MCI and school teams (Dubuque-Gallo et al., 2022), thus restricting the findings to these unique participants. Both researchers and participants are primarily White and worked in various regions across the state, though the generalizability of these findings to other populations that come from communities that are historically under-resourced, marginalized, or linguistically diverse may be restricted. Thus, future research should specifically target demographically diverse youth and providers.
Finally, recruitment and the participant self-selection process may have influenced these findings. A larger representation of school district members participated in focus groups, which may reflect the proportionately larger sample sizes of districts. For example, there are roughly 20 mobile crisis agencies that provide crisis response services, employing far fewer staff than the 400 school districts. Moreover, there was a small, self-selected sample of MCI providers and there is a need to continue research with their perspectives. Caregivers who self-selected to participate in this study may have had more negative experiences with MCI and school teams which they wanted to highlight, which ultimately could impact findings. It may be beneficial to replicate this study with a larger sample size and an intentional effort to diversify the sample in regard to participant roles and identities.
Based on current findings, more research is needed to evaluate practices and interventions that alleviate the identified issues described above. For example, it would be beneficial to study organizations that have established effective collaborative models and examine what factors contribute to their success. Despite the aforementioned benefits of MCI and the clear need of integrated services, focus group members did not focus on the strengths of collaborative efforts despite prompting to do so. Although this speaks to the apparent frustrations experienced by both parties, and the need for improved collaboration, it may be beneficial for future studies to focus solely on the inherent strengths between this partnership. Finally, while this study was primarily focused on systems-level partnerships, and thus, centered the voices of caregivers and providers, future research must be replicated with youth themselves. Ultimately, youths’ experiences and voices must inform continued behavioral health emergency response efforts.
Conclusion
This study examined the strengths and challenges of inter-agency collaboration between MCI and school teams by elevating the voices and perspectives of those intimately involved in these events. Though the interview prompts focused on both strengths and challenges, our findings highlighted systemic and interpersonal barriers that impede effective collaboration. Results suggest that improving inter-agency collaboration between MCI and school teams may improve school’s capacity to meet youth’s behavioral health needs. Additionally, effective collaboration would allow for a wraparound approach to better support youth and their families. Future studies on this collaboration would be beneficial given the variance in organizational models for schools and MCI providers across the state, as well as the lack of existing research.
Footnotes
Ethical Considerations
This study was approved by the University of Massachusetts Boston IRB on April 1st of 2021 (Study Number: 2021036). Written and verbal consent were obtained by all focus group participants.
Consent to Participate
All participants in this study provided written electronic consent prior to participating. The PI and researchers were available to answer questions prior to consent obtainment. Participants were informed that participation is strictly voluntary, and they could leave the study at any point without consequence.
Author Contributions
The authors confirm contribution to the article as follows: study conception and design: A. Priest, T. Berkman; data collection: A. Priest, T. Berkman, K. Ruggeri; analysis and interpretation of results: A. Priest, T. Berkman, K. Ruggeri, D. Laenen, J. Osborn, K. Kurtz; draft manuscript preparation: A. Priest, T. Berkman, K. Ruggeri, D. Laenen, J. Osborn, K. Kurtz, M. Pearrow. All authors reviewed the results and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study received funding from Boston Children’s Collaboration for Community Health and the Massachusetts Department of Mental Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy and ethical restrictions.