
Abstract
Diagnoses of cancer at later stages contribute to racial/ethnic disparities in cancer survival, with African Americans/Blacks and sometimes Hispanics experiencing poorer 5-year survival rates for breast, cervical, colorectal, lung, and prostate cancers. Interventions that promote early detection and cancer prevention are critically needed to reduce racial/ethnic disparities in cancer survival. The purpose of this study was to develop the Pathways to Cancer Prevention and Screening training program to educate community health workers (CHWs) on cancer prevention and screening guidelines; and cancer screening referrals for breast, cervical, colorectal, lung, and prostate cancers. We examined pre- and post-training changes among CHWs in (a) cancer prevention and knowledge overall and by sub-category: cancer knowledge, screening, and preventive lifestyles; (b) cancer fear and fatalism; and (c) comfort discussing screening guidelines. In an urban area using a quasi-experimental design, we recruited 47 CHWs, with 44 who completed pre- and post-assessments. Statistically significant changes that suggest improvement in mean cancer knowledge prevention scores overall and by sub-categories: cancer knowledge, cancer screening, and preventive lifestyles. Improvements in cancer fear and fatalism were marginally significant, and comfort in discussing cancer screening guidelines significantly improved from pre- to post-assessment. Pathways to Cancer Prevention and Screening is a feasible way to improve knowledge of cancers, and screening guidelines for breast, cervical, prostate, lung, and colorectal cancers. Investing in CHW workforce development can improve the quality of one-on-one education to clients with increased risk for five of the most prevalent forms of cancer.
Introduction
For African American/Black (henceforth Black) and Hispanic American people, a cancer diagnosis is often associated with more advanced cancer (Giaquinto et al., 2022; Miller et al., 2018). In a population-based study of Black and White people in the Surveillance Epidemiology and End Results (SEER) database, Virnig et al. (2009) found that White people were diagnosed at earlier stages than Black people in 31 out of 34 tumor sites. These sites include the leading five cancer types—female breast, cervix, colorectal, prostate, and lung cancers (Virnig et al., 2009), and critically impact racial disparities in cancer survival throughout the United States (Giaquinto et al., 2022). A statewide analysis of health and demographic patterns reveals pronounced racial disparities in Wisconsin, with Black and Hispanic women showing lower 5‑year breast cancer survival rates and Black residents experiencing poorer colorectal cancer survival compared with White residents (Beyer et al., 2016). Systemic barriers, such as low socioeconomic status, clinic access, uninsured/under insured, quality of screening for various cancers (e.g., mammogram), and transportation, drive many of these disparate outcomes in the early detection of cancer (Giaquinto et al., 2022; Miller et al., 2018). Interventions that address these barriers through providing referrals for early detection of cancer can improve access to cancer screenings and provide education on cancer prevention.
Training the community health worker (CHW) workforce on early detection and cancer prevention is one way to work toward addressing some of the systemic barriers faced by communities that are disproportionately burdened by lower cancer survival rates. As trusted members of the community, CHWs are non-clinical public health liaisons who facilitate access to services and resources that relate to health and other basic needs (Balcazar et al., 2011; Battaglia et al., 2022). With deeply rooted connections and trust among the communities, CHWs have the potential to engage communities with cancer education, awareness, and screening (Murayama et al., 2017). This role does not typically require a formal education, and the standard occupational classification categorizes CHWs under Community and Social Service Occupations (Battaglia et al., 2022). CHWs engage individuals from historically disadvantaged backgrounds and lower incomes to increase breast, cervical, and colorectal cancer screenings among medically underserved populations (Islami et al., 2022) and often share the racial/ethnic background of the people they serve (Murayama et al., 2017).
Literature Review
There is a growing body of research demonstrating the use of CHWs in cancer screening uptake. For example, a recent systematic review of 76 studies showed that CHWs were used to improve breast, cervical, and colorectal screening (Okasako-Schmucker et al., 2023). In addition, the Cancer Prevention and Screening Taskforce (CPSTF) has found substantial evidence that CHWs increase cancer screening rates through various interventions. Collectively, these studies show that CHWs engage in some common strategies to improve screening uptake, such as including educational interventions to increase awareness of cancer screening; reducing barriers to clinic accessibility by connecting clients to services for transportation; translating services into clients’ native languages; and coordinating access to childcare (Islami et al., 2022). Through these common strategies, CHWs enable advocacy for the wellness of medically underserved communities (Murayama et al., 2017). However, little is known about training CHWs on multiple cancer types and cancer prevention.
While previous work has discussed improving screening uptake, few have included lung and prostate cancer screening. In addition, cancer prevention has been rarely included as a training component for CHWs (Okasako-Schmucker et al., 2023). We build on this body of work, by focusing on each of the five most prevalent cancers including lung and prostate cancers, as well as cancer prevention. A focus on both screening and prevention supports the National Cancer Plan’s goal to eliminate inequities in cancer risk factors and mortality through equitable access to prevention, treatment, and survivorship care (National Cancer Institute, 2025).
CHWs are being increasingly integrated into the oncology workforce to connect historically marginalized communities to healthcare providers and services (Battaglia et al., 2022), but less is known about how to train CHWs on the screening and prevention of multiple cancer types. When CHWs are educated about cancer prevention, they provide relevant materials to their clients, it also creates an increased demand for screening services in their shared communities (Islami et al., 2022). Mobilizing resources and equipping CHWs with cancer prevention knowledge is a proven way to address the imbalanced prevalence and persistence of cancer mortality in medically underserved communities. Through training a diverse CHW workforce, it will increase access to cancer prevention and screening resources among the underserved.
Study Purpose
The purpose of this study is to explore ways to mitigate declines in screening uptake after the COVID-19 pandemic. Our objective was to train a diverse group of CHWs on multiple cancer types to reach a larger demographic of clients. We describe the process of teaching CHWs about breast, cervical, colon, lung, and prostate cancers; connecting clients to cancer-related community resources; and referring clients to relevant cancer screenings.
Method
Participants and Setting
This study included a purposive sample of CHWs recruited through UniteWI, a care coordination agency, between February 2022 and February 2023. Participants were contacted through email and letters describing the study’s purpose, procedures, time commitment, data collection, and the voluntary nature of the study. Our inclusion criteria for CHW participation in the Pathways to Cancer Prevention and Screening Training and survey were as follows: (a) age >18; (b) completed Pathways community HUB institute CHW Training; or (c) will complete Pathways community HUB institute CHW Training; or (d) currently practices as a medical professional (e.g., pharmacist); and (e) have current HIPAA certification.
Intervention
The Pathways to Cancer Prevention and Screening training is a 16-hr hybrid training (4 hr for 4 days) for CHWs developed collaboratively between the CHW organization, and faculty at two Midwestern Universities. Participants were encouraged to attend in person, but an online option was available via Zoom for those who could not attend in person. Community members, a breast oncologist, and experts in cancer prevention and control collaboratively developed this training. The training development process involved biweekly meetings, where we outlined what CHWs should know to provide one-on-one guidance for cancer prevention and cancer screening referrals. We also leveraged the expertise of our colleagues in lung, prostate, colorectal, and cervical cancer to provide the most up-to-date information on screening guidelines. The training consisted of lectures, hands-on activities, and role playing. The facilitators included a breast oncologist and a community outreach director. We also identified curricula focused on breast cancer and cancer awareness with similar goals from reputable sources to adapt some of these materials. The training included information on each of the five cancer types and focused on six areas: (a) health behaviors to promote cancer prevention; (b) risk factors, diagnosis, and general treatment guidelines for breast, colorectal, lung, prostate, and cervical cancers; (c) current cancer screening guidelines for breast, colorectal, lung, prostate, and cervical cancers; (d) strategies to address barriers to cancer screening, including tools to navigate barriers to early screening; (e) strategies to address cancer fear and fatalism; and (f) hands-on training for HUB Pathways software on the Cancer Prevention and Screening electronic protocol.
These six areas were offered because it gives CHWs a basic understanding of the disease, how to prevent it, and the screening process. In developing the training materials, we were give permission to leverage some of the structure and content ideas offered through Cancer Clear & Simple (Fredrick et al., 2022) and Rodriguez and colleauges (Rodriguez et al., 2020). Each set of cancer educational materials included a curriculum, facilitator guide, and educational handouts. CHWs received our adapted curriculum binder, as well as a laminated card with updated cancer screening guidelines as resources.
Once recruited participants were sent a survey link through REDCap to complete a pre-test on three sub-categories: cancer knowledge, cancer screening, and health/diet/physical activity up to one week before the training. Following the pre-test, participants attended a 16-hr hybrid workshop in-person or on Zoom completed over 4 days. At the end of the workshop, participants were sent a survey link through REDCap to complete the post-test on cancer knowledge, cancer screening, and health/diet/physical activity up to 1 week after the training. Participants who completed both assessments received a $50 store gift card. The University’s Institutional Review Board approved all the study procedures.
Table 1 shows participant demographics. The sample was individuals of predominately African American, followed by Asian and White backgrounds. The majority were non-Hispanic individuals, with one-quarter of the group were Hispanic individuals. Nearly a quarter of the group’s highest education was high school or equivalent (20%), while 16% completed an associate degree or 2-year certificate, nearly a third completed some college (32%), and over a quarter were either college graduates (16%) or completed graduate school or a professional degree (11%).
Descriptive Characteristics of Community Health Worker Participants at Baseline (n = 40)
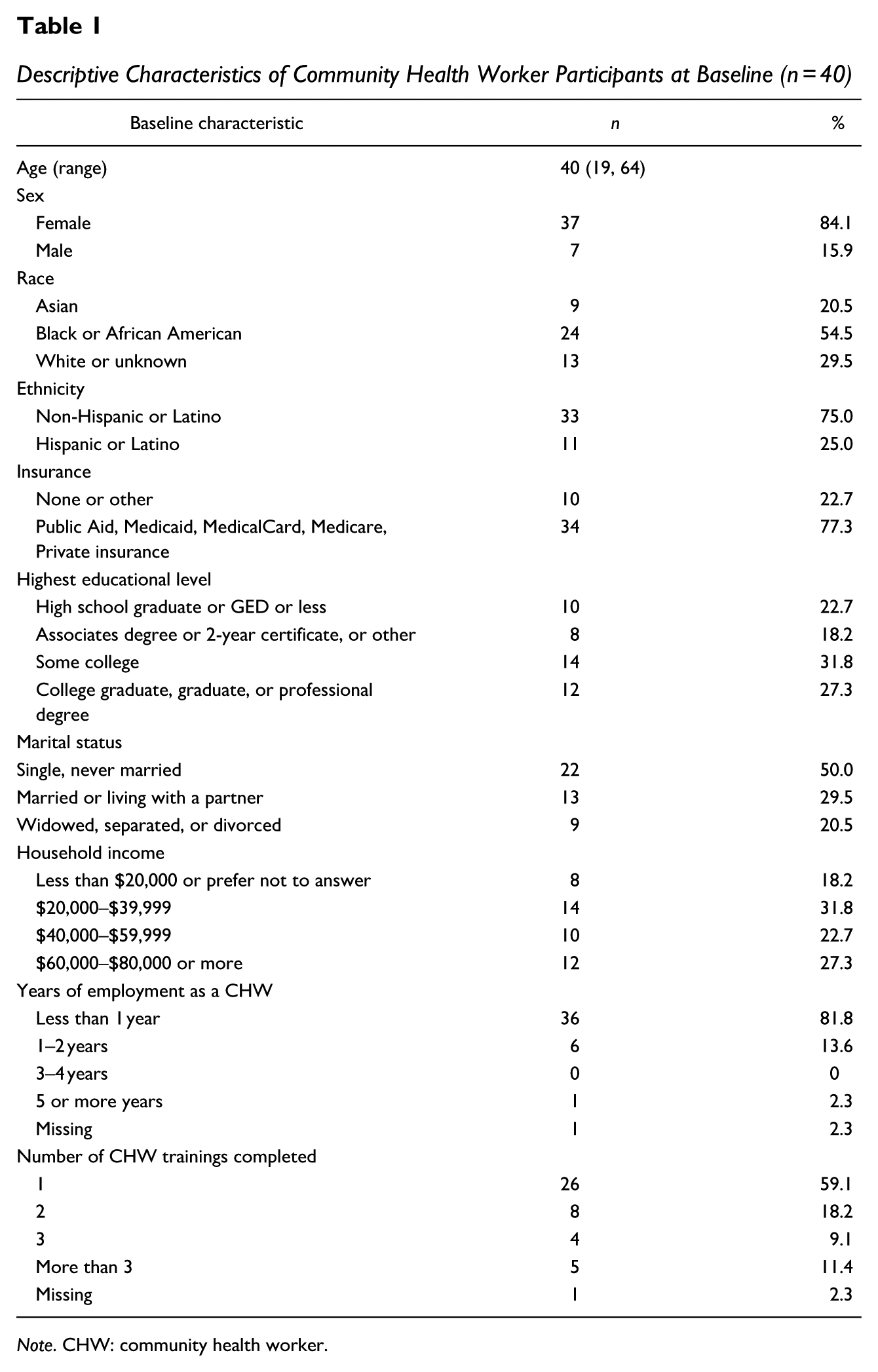
Note. CHW: community health worker.
The study was conducted in a Midwestern City. According to the U.S. Census Bureau 2020 estimates, our county has a population of 939,489. The employment rate is 61.2%, the median household income is $55,347, and 17.8% live in poverty. The median age is 35.4 years. The racial and ethnic makeup of the county is nearly half non-Hispanic White (48.6%), a little over a quarter Black or African American (25.6%), and 4.9% Asian (non-Hispanic). About 16.3% of the population are Hispanic (White, Multiracial, Black or African American, or Other). The age-adjusted cancer mortality rate from 1995 to 2020 is 169.3 (mortality per 100,000 population), which far exceeds the Health People 2030 cancer mortality rate goal of 122.7 per 100,000.
Measures
Demographics
Participants provided information on age, marital status, race/ethnicity, gender, the highest level of education, length of time in employment as a CHW, number of CHW trainings completed, annual income, and insurance status.
Cancer Prevention Knowledge Questionnaire
An adapted version of the Cancer Clear & Simple cancer prevention knowledge measure was used (Fredrick et al., 2022). The adapted measure is an index of 18 items related to cancer knowledge, cancer screening, and preventive lifestyles (i.e., health, diet, and physical activity). The adapted measure added questions on cancer screening, and preventive lifestyles are recorded as True/False. Each item answered correctly was scored as one point for a total of up to 18 points. Higher scores reflect increased knowledge.
Powe Cancer Fatalism Inventory (PFI): It is a 15-item inventory focused on fear, pessimism, and sense of inevitability of death and predetermination. Respondents responded yes or no to statements and scores ranged from 0 to 15 (Powe, 1996). PFI is widely cited and used in cancer-related research, especially among minority and underserved populations. The reported Cronbach’s alpha values (≥.80) are generally strong across multiple studies, supporting reliability (Keller et al., 2024).
Knowledge of ACS Diet and Physical Activity Guidelines
A four-item index was created for this study to assess knowledge of the American Cancer Society diet and physical activity guidelines. Responses are recorded as True/False. Each correct item was scored one point, for a total of up to four points. Higher scores reflect increased knowledge of guidelines.
Comfort With Discussing Screening Guidelines
A 10-item index measure to assess CHW comfort level in referring clients for cancer screening tests, answering questions regarding cancer screening, and conducting an education session with a participant. Participants rated their comfort with discussing screening guidelines on a scale from 1 to 10. Responses ranged from 1 = very uncomfortable to 10 = very comfortable. This measure was taken from a sample of healthcare professionals that were trained to improve cancer screening referrals (Bryan et al., 2015).
Cancer Screening and Cancer Diagnosis History
Items asked the CHW about their cancer screening uptake mammogram; pelvic exam/pap smear; colonoscopy; and blood stool test, as well as if they had ever been diagnosed with cancer, and if so, what type. Participants responded yes or no. The measures were created for this study. These items were included to understand the extent to which CHWs have experienced cancer screening and diagnosis, which could inform their knowledge of cancer screening, diagnosis, and treatment.
Research Design
We conducted this pre and post study using a quasi-experimental design with a single group of participants who completed the Pathways to Cancer Prevention and Screening training. Quantitative survey data were collected to examine changes in cancer knowledge, cancer screening, health, diet, and physical activity.
We calculated a cumulative score from the Cancer Prevention Knowledge Questionnaire across three categories (cancer knowledge, cancer screening, health, diet, and physical activity) using a pre- and post-test design. Correct answers given by participants for cancer knowledge (e.g., Cancer is one disease [True or False]), cancer screening (e.g., The goal of cancer screening is to find cancer before it grows and spreads [True or False]), and health, diet, and physical activity (e.g., Physical activity lowers your chance of getting cancer [True or False]), were summed to create a Cancer prevention knowledge score variable for each participant. In addition, we calculated the change for fear and fatalism, which was the sum of all belief questions answered positively. Data were analyzed using R software (R Core Team).
To prepare the data for analysis, we assessed the data for missingness and checked to ensure that all statistical assumptions for the proposed analysis were met. Data were imported from REDCap, with basic cleaning including making R readable column headers and missing cell consistency for analysis. For response, for the repeated measures regression, three participants were excluded from the analysis because repeated measures ANOVA needs complete cases for estimation. Missing responses on the pre-test for scores were tallied as if answered incorrectly so as not to drop the subject from the larger analysis.
Homoscedasticity and error plots were visually examined to inspect for any major departures from the ANOVA assumptions. Covariates were checked to exclude high multicollinearity. Because repeated measures ANOVA was used for the analysis of this data, the data were subset to only participants who had both a pre- and post-event measurement.
Results
Table 2 shows pairwise t-test results on changes in cancer knowledge, screening, preventive lifestyles, fear and fatalism, and comfort. We combined scores from the Cancer Prevention Knowledge Questionnaire overall (F = 20.38, p < .001), cancer knowledge (F = 5.10, p = .029), screening (F = 9.35, p = .004), and preventive lifestyle subscales (F = 10.03, p = .003). Participants had statistically significant changes on the post-test using repeated measures ANOVA (F = 3.70, p < .01). We examined the effects of each of the scores alone and found significant effects from pre- to post- for knowledge, screening, and preventive lifestyles. The results of the pairwise t-test show that the event arm (post-event) had a significantly higher score than those in the pre-event arm. We conducted post hoc analyses on the 44 participants to test whether those with certification compared to those with certified and found no significant differences between pre and post scores. It is unclear whether the training workshop affected cancer fear and fatalism. Although fear and fatalism decreased from pre- to post-, the change was only marginally significant (F = 3.70, p = .061). Table 3 shows the CHWs’ comfort in discussing cancer screening guidelines with clients. The pairwise t-test showed that the post-workshop group had a significantly higher score than the pre-workshop group. With the exception of following up with physician offices on screening referrals (F = 2.07, p = .158), there were significant improvements in each of the individual components: referring clients for cancer screening tests (F = 20.49, p < .001), answering clients’ questions (F = 14.15, p < .001), counseling clients on barriers to cancer screening (F = 10.56, p = .002), conducting an education session with a client (F = 18.79, p < .001), reminding clients to complete cancer screening (F = 6.01, p = .019), providing primary physician referrals to clients (F = 5.30, p = .027), referring clients to a low-cost screening program (F = 7.42, p = .010), keeping client records in Pathways on cancer education and screening (F = 19.29, p < . 001), and educating clients in cancer screening guidelines (F = 12.17, p = .001). Participants scored an average of 9 or 10 out of 10 across all 10 domains. CHWs had to score an average of seven or higher in the overall comfort score to be included in the study.
Pairwise t-Tests on Change in Cancer Knowledge, Screening, Preventive Lifestyles, Cumulative Cancer Preventive Knowledge, and Fear and Fatalism
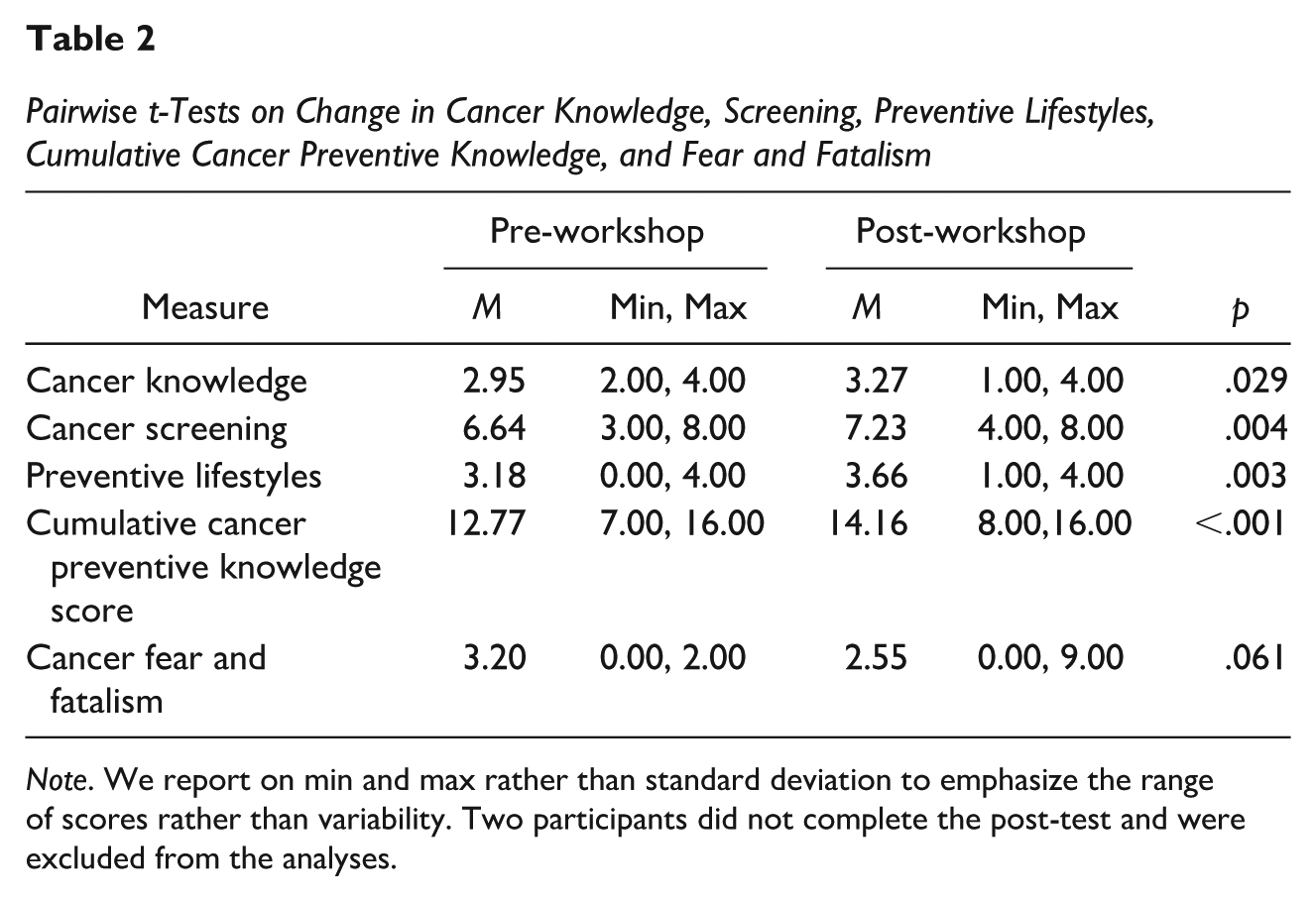
Note. We report on min and max rather than standard deviation to emphasize the range of scores rather than variability. Two participants did not complete the post-test and were excluded from the analyses.
Comfort in Discussing Screening Guidelines Among Community Health Worker Participants
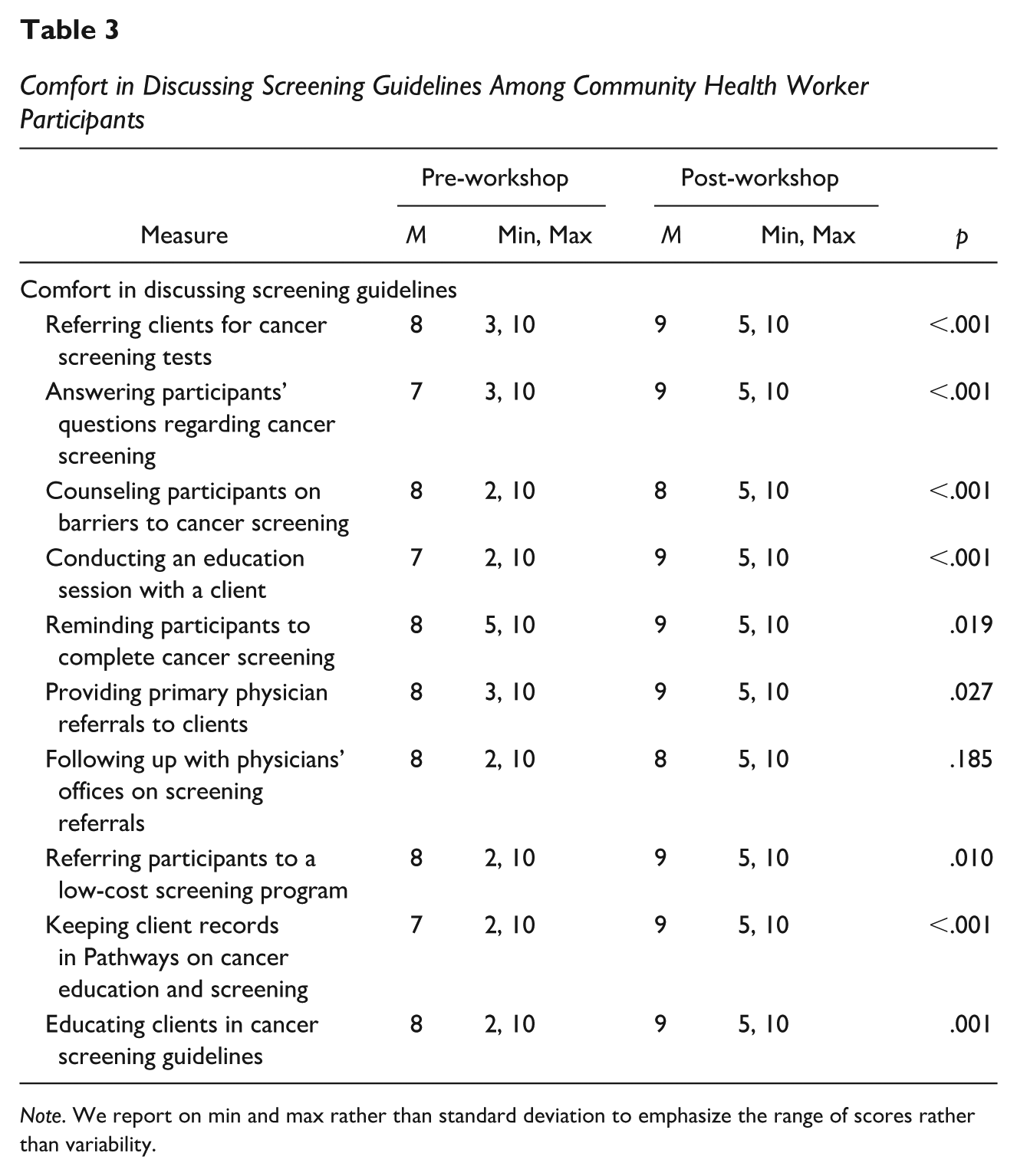
Note. We report on min and max rather than standard deviation to emphasize the range of scores rather than variability.
Discussion
The aim of our Pathways to Cancer Prevention and Screening Training was to teach CHWs about breast, cervical, colon, lung, and prostate cancer and how to connect their clients to cancer-related community resources; and refer clients to relevant cancer screenings. Our results show that the Pathways to Cancer Prevention Training is a feasible way to improve CHW knowledge of cancer prevention and screening, as well as comfort in discussing cancer and screening guidelines among CHWs—but not to reduce fear and fatalism.
Previous studies typically focus on breast, cervical, or colorectal cancer alone and do not include multiple cancer types in one initiative. In contrast, our study introduces cancer screenings for each of the major types of cancer, and prevention-oriented training. In particular, we tested general cancer knowledge that included information on three sub-categories: cancer knowledge, cancer screening, and health/diet/physical activity. We focused on teaching participants basic cancer information, such as what cancer is, and who is at risk (Fredrick et al., 2022; Rodriguez et al., 2020). We found significant changes in each of these sub-areas as well as improvements in the cumulative score. Although participant knowledge was high at baseline, participants still experienced significant changes post-workshop. None of the CHWs had previous experience working in an oncology setting or with cancer patients. However, during monthly check-in meetings, some of the CHWs attributed their high knowledge of cancer at baseline to their previous diagnosis of cancer among study participants or family members, and the receipt of cancer screening. Our study advances this literature by demonstrating significant changes in knowledge across five major cancer types: breast, cervical, colorectal, prostate, and lung cancer. Our finding is consistent with previous studies that focused on increasing cancer knowledge among CHWs for breast (Keating et al., 2014; Gu et al., 2019; Rodriguez et al., 2020; Wyatt et al., 2023), cervical (Wyatt et al., 2023), colorectal cancer (Boutsicaris et al., 2021; Whitaker et al., 2020), prostate cancer (Aristizabal et al., 2023), and lung cancer (Williams et al., 2021). However, what this study adds is that it included multiple cancer types of cancer, including lung and prostate, as well as cancer prevention.
Many interventions emphasize screening awareness, but with recent changes in screening guidelines, new and updated trainings are warranted among CHWs. We focused on current cancer screening guidelines due to recent changes in the age of screening for colorectal cancer.
Few studies incorporate training on cancer prevention strategies, such as lifestyle modification, risk factor reduction, and early detection (Okasako-Schmucker et al., 2023). The National Cancer Plan prioritizes the need to reduce cancer incidence, and our focus on preventing cancer addresses a critical gap in the focus of CHW training (National Cancer Institute, 2025).
In contrast to previous studies, our study focused on changes in cancer knowledge among CHWs rather than increasing cancer knowledge among their clients (Bryan et al., 2015; Holt et al., 2019). Participants also experienced a significant change in comfort in discussing cancer and screening guidelines. Out of the 10 items included in the comfort score, participants improved the most in referring clients to cancer screenings, reminding participants about an upcoming appointment, answering participant questions regarding cancer, and educating clients on cancer screening guidelines. This finding is consistent with other studies that have shown that CHWs can play an important role in scheduling screening appointments and reminding participants to attend the appointment (Bryan et al., 2015; Holt et al., 2019). However, because many of the CHWs were already experienced as CHWs, many of them already felt comfortable discussing screening guidelines with clients. Based on our interactions with the CHWs, we believe that they were not aware of what the screening guidelines were before completing the training. We did not include a follow-up question to find out why they were comfortable discussing the screening guidelines without knowing what they were initially.
We did not find evidence to suggest that our training significantly reduced fear and fatalism. While participants did experience a reduction, it was not significantly different from baseline. This may be due to the low levels of fear and fatalism at baseline. A score of less than 5 on the Powe fatalism scale is considered low fear and fatalism. The mean fatalism score for participants was low both at baseline and post-workshop. We conducted some additional analyses to compare individuals who scored high versus low on fatalism at baseline and post-workshop but did not find a significant difference. Engaging CHWs with low levels of fear and fatalism may be an important aspect of conducting work in this field. This is the only study that we are aware of that have examined changes in fear and fatalism among CHWs.
Limitations and Future Directions
Our results reflect a small purposive sample of a diverse group of CHWs working in urban areas; these results may not be generalizable CHWs working in rural areas. Due to this small sample size, we did not stratify responses by any particular demographic characteristic, such as years of experience as a CHW. Future researchers may consider replicating this study in a large metropolitan area and stratifying on years of experience as a CHW to better understand the impact of this training on changes in cancer knowledge. In addition, our results explored changes in knowledge with repeated measures using a pre- and post-test design before and after the workshop. While we saw statistically significant changes, the absence of well-established, standardized measures for assessing cancer knowledge limits our ability to compare the effect sizes to comparable studies. Nonetheless, our findings did show improvements in cumulative scores for cancer knowledge although it was measured differently in previous studies. We also found that the comfort levels of CHWs increased, which may imply that they also felt more knowledgeable about cancer screening and prevention at the end of training.
Implications
The training in cancer prevention and screening guidelines not only increased their cumulative knowledge of cancer screening and prevention, but it also increased the CHWs’ comfort in educating clients on cancer screening guidelines, answering questions regarding cancer screening, and referring them to screening services. As trusted members of the community, these enhanced skills can help CHWs to normalize conversations regarding cancer prevention and screening in their communities, and contribute to the dissemination of accurate information on cancer screening and prevention.
Conclusions
This article can be used as a guide for other communities seeking to increase the uptake of cancer prevention knowledge and screening among CHWs. Based on our findings, we recommend that this model be replicated among CHWs to equip CHWs to promote cancer prevention behaviors and screening uptake across multiple cancer types.
Footnotes
Acknowledgements
The authors thank all of the participants for their time and effort put into this project.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Advancing a Healthier Wisconsin endowment at the Medical College of Wisconsin (Grant # FP41531). This project utilized REDCap supported by National Center for Advancing Translational Sciences, National Institutes of Health grant award 2UL1TR001436.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.