
Abstract
Background
N-of-1 designs involve randomising an individual between treatments and recording outcomes over several timepoints. They are rarely used in mental health research. This research aims to explore the reasons behind this, identifying both opportunities and barriers to their implementation.
Methods
A cross-sectional qualitative study was conducted to explore healthcare professionals’ and trial app developers’ views on N-of-1 trials in mental health. Data were collected through semi-structured interviews and analysed using framework analysis, informed by the Theoretical Domains Framework.
Results
We conducted interviews with nine participants, including three psychiatrists, two mental health nurses, two other health professionals, and two people who were involved in developing apps for research in mental health to explore perspectives on N-of-1 trials in mental health. We generated three key themes: (1) N-of-1 trial designs are appropriate for very specific combinations of patient populations, interventions and settings in mental health. (2) If used appropriately, N-of-1 trials have the potential to inform treatment choice, improve outcomes and empower patients. (3) Improved knowledge and understanding of N-of-1 trials is needed among clinicians, patients and the wider research system to facilitate the use of this trial design in mental health.
Conclusions
Our findings suggest a potential role for N-of-1 trials in mental health, specifically for patients with stable chronic conditions and for interventions that can be safely discontinued and re-started. N-of-1 trials could inform treatment choices, improve outcomes, and empower patients. However, significant barriers to implementing this trial design exist within the current UK health and research system.
Keywords
Introduction
It is common to hear that a treatment ‘does not work’ for a certain person, or that it works differently for different people.1,2 Anecdotally, the present authors have frequently heard such claims based on informal self-experimentation, such as, ‘I took this treatment for 2 weeks and felt awful; then stopped taking it and felt better.’ Anecdotal evidence like this is often used to support claims that a treatment does not work. In this context, N-of-1 trials offer a more rigorous basis for understanding the effects of a treatment on a given person. They include devices such as randomisation and replication that facilitate making causal claims about treatments.
N-of-1 trials are an underused experimental design
3
whose essential feature is randomisation of a single individual between two or more treatments over several time points. After an initial randomisation, the patient’s outcome is measured at a defined time point, after which the second randomisation occurs, and so on. In practice, randomisation is typically arranged in blocks (sometimes referred to as ‘cycles')
4
so that a treatment cannot be repeated before each treatment has been assigned in that block. For example, an N-of-1 trial with six treatment periods and two treatments would be split into three blocks of two. Each block consists of A first and B second, or B first and A second (where ‘A’ labels existing treatment and ‘B’ a new treatment). There are
In N-of-1 trials, the individual is randomised multiple times, meaning we learn about an average treatment effect across the times. That is, N-of-1 trials inherently target a different estimand to parallel-group trials. Although seasoned researchers tend to roll their eyes at promises of ‘personalised’ or ‘individualised’ medicine, an N-of-1 trial does provide this, albeit saying little about other individuals. The purpose of this article is not to review the theoretical justifications for N-of-1 trials, nor document their development; there are many excellent resources that already do this. Mirza et al provide an interesting overview of the historical development and context of N-of-1 trials 5 . Since they were first proposed in medicine by Guyatt et al 6 there have been many subsequent developments, including the development of reporting standards7,8 and the concept of aggregate N-of-1 trials9,10. A comprehensive overview and list of resources can be found on the Stats-of-1 website. 11
N-of-1 trials have been used in many fields. A recent review by Hawksworth et al. found 74 N-of-1 trials, used across many different health/disease areas. 3 Chatters et al. provided 22 structured points to appreciate about N-of-1 designs to help decide whether an N-of-1 trial is viable and appropriate. 12 Generally, N-of-1 designs are most useful and straightforward for conditions that are stable over time, with intervention that is expected to have a quick but temporary effect, and for outcomes that can be measured quickly.
This project was inspired by conversations where it was clear that people often experiment on themselves in an ad hoc way, sometimes with interventions that they claim to improve or otherwise affect their mental health. Such interventions for mental health suggested that they could be more rigorously understood using N-of-1 designs.
Hawksworth et al.'s review found very few N-of-1 trials had been used in the area of mental health/illness. 3 A systematic review of N-of-1 trials for depression found five eligible studies, all of which evaluated the effects of pharmacologic treatments, and found heterogeneous treatment effects that could personalise treatment selection for individual patients. 13 The authors reported a paucity of information on implementation challenges such as cost, time, and clinicians views on the usefulness of N-of-1 trials, which may hinder uptake of the trial design. Another systematic review looked at the use of N-of-1 trials in schizophrenia 14 . This found six studies meeting the inclusion criteria, investigating pharmacological, psychological and physical interventions. A search of https://clinicaltrials.gov revealed a number of registered N-of-1 trials in the area of mental health, including light therapy for depression 15 ; a personalised lifestyle intervention for depression or anxiety 16 ; open-label placebo aiming to alleviate side-effects from anti-depressant discontinuation 17 ; and gratitude journalling, mindfulness meditation, random acts of kindness, physical activity and laughter therapy for stress, cognitive focus and happiness 18 . However, none of these studies seem to have published results at the time of writing (except for baseline characteristics), despite having been completed more than a year ago.
Implementation science to identify barriers and facilitators to the adoption of N-of-1 trial design in mental health has the potential to help us better understand the potential role of this trial design, and what is needed to facilitate its use.19–21 It provides theoretical frameworks to better understand the challenges associated with implementation. 22 One of these frameworks is the Theoretical Domains Framework (TDF). 23 TDF is widely-used within implementation science and has been validated in numerous studies 24 on a variety of topics. It synthesises constructs from many behaviour change theories into 14 domains, including knowledge, skills, beliefs about consequences, social/professional role and identity, social influences and environmental context and resources.
This project sought to understand the views of stakeholders including health professionals who treat people with mental health conditions, ethics committee members and developers of mental health apps around the appropriateness, opportunities, barriers, and facilitators to use of N-of-1 trials in mental health. We aimed to talk to mental health professionals about the scope for N-of-1 trials in mental health research because they could play a role in using or encouraging use of N-of-1 trials to better understand how a treatment works for an individual. Given that N-of-1 trials exist, and could sometimes be appropriate, we wanted to learn about the situations and treatments in which they may be used, the barriers, and whether these are surmountable.
Methods
We conducted a cross-sectional qualitative study of the views of health care professionals who care for people with mental health conditions within the UK National Health Service, and trial app developers, around the use of N-of-1 trials in mental health. Our completed SRQR checklist can be found in Annex 1. Data were collected using semi-structured interviews and analysed using framework analysis approach. 25 The study was informed by the Theoretical Domains Framework, 23 and we employed a critical realist perspective, taking the viewpoint that research outcomes are influenced by the context in which the research takes place, including the background of the research team. 26 Further detail about our methods and results can be found on OSF. 27
Sampling and recruitment
We used a purposive approach to sampling, aiming to recruit three categories of participants: • Health care professionals involved in treating people with mental health conditions in the UK (including those who specialise in mental health, e.g. psychiatrists and mental health nurses, and those who are not specialists in mental health, e.g. General Practitioners and other medical professionals) • Research Ethics Committee members • People involved in developing interventions/and or applications for mental health
Our sampling frame included a range of characteristics in addition to role (described above): • Years of experience (1–5, 6–10, >10) • Whether they have experience of N-of-1 trials (yes or no) • Whether they conduct research as part of their current role (yes or no)
Interviewees had to be above the age of 21, and able to give informed consent.
Using the Information Power model, 28 we anticipated needing around 20–30 interviewees, given the narrow study aim and specific participant experience (but number of different types of participants we wanted to include), and application of established theory, and cross-case analysis approach.
We advertised the study to potential participants via email, social media, and professional networks. The adverts included a link to the electronic participant information sheet. Due to slower than anticipated recruitment, we amended our recruitment approach to include paid-for social media advertising on LinkedIn (including a short animation explaining the concept of N-of-1 trials) and allow for snowball sampling.
The electronic participant information sheet contained a link to an electronic consent form and basic characteristics questionnaire for participants who wished to take part. This electronic consent form was created in REDCap within the UCL Data Safe Haven to ensure that potentially identifiable information was stored directly in a secure environment. The basic characteristics questionnaire was designed to inform our purposive sampling, allowing us to contact those who filled a gap in our sampling frame to arrange a suitable time for an interview.
Researcher characteristics and initial expectations
The research team brought diverse but complementary backgrounds in clinical trials methodology and qualitative research. AS is an experienced qualitative and mixed-methods researcher with over a decade of experience in clinical trials and a PhD in clinical trials methodology. She had no prior professional experience with N-of-1 trials or mental health research, but has conducted an N-of-1 trial on herself. She anticipated that participants would be unfamiliar with N-of-1 trials and expected to identify substantial barriers to their use, including time constraints, limited skills for design and analysis, and ethical concerns. She also expected that some clinicians might carry out informal N-of-1-type approaches in practice. GA and ST were PhD students in clinical trials methodology, both experienced in clinical trial operations and qualitative interviewing and analysis but new to N-of-1 trials and mental health research. Both expected mental health professionals to be positive about personalised approaches, but did not fully appreciating the complexity of applying N-of-1 designs in settings such as general practice or in populations with severe mental illness. TM is a senior statistician with over ten years’ experience in clinical trials methodology and personal experience conducting an N-of-1 trial on himself, though without prior involvement in qualitative research. He expected very limited awareness or use of N-of-1 trials in mental health and feared interviews might yield little insight due to participants’ lack of direct experience. He also anticipated that participants might enrol primarily out of curiosity rather than knowledge, yet hoped they would express enthusiasm and help clarify the potential scope and value of N-of-1 trials.
Data collection and tools
Interviews were based on a topic guide 27 informed by the Theoretical Domains Framework, which was pilot tested before data collection commenced. Separate versions of the topic guide were created for the three categories of interviewees (with an adjusted version produced when we recruited an interviewee that spanned two of the three categories). The topic guide was updated as interviews progressed to provide greater clarity where needed, including adding an explanation of what N-of-1 trials are, adding probing questions and links to further information. Iterative adaptation aligns with established qualitative approaches in which data collection and analysis inform one another, and does not compromise trustworthiness, which rests on transparency and a clear decision trail rather than rigid question standardisation 29 . Interviews were conducted online between December 2024 to March 2025. Interviews were recorded audio-visually in Microsoft Teams by authors GA and ST. Recordings and transcripts were then uploaded to the Data Safe Haven, and transcripts were checked, corrected and pseudonymised by the interviewers. All analyses were performed using the pseudonymised transcripts.
Data analysis
We used a Framework Analysis approach 25 to analyse our data, using NVivo version 14 to assist with indexing, sorting and data display. The first step involved familiarisation with the data, which included carefully reading the transcripts and making notes of thoughts and impressions, particularly around what people were saying that was relevant to the research question. Once we had conducted the first three interviews, the team individually read the transcripts and developed (independently) a list of concepts (potential codes) based on the data. We then held a workshop to construct version 1 of the framework. At this workshop, we each wrote each concept/code we had identified on separate sticky notes. We then grouped our concepts under the 14 domains of the Theoretical Domains Framework, using definitions based on those in the literature. 23 Where we were unsure where a particular concept belonged, we discussed it. Some concepts did not fit under any of the Theoretical Domains Framework. Where this was the case, we considered whether this indicated a new domain was required for our analysis framework. We also discussed the definitions of domains, adding examples of things we felt did or did not fit in the domain where needed for clarity. Based on this workshop we developed a codebook for version 1 of our framework.
The next stage of our analysis was indexing and sorting, labelling chunks of data with the relevant concepts from the framework we had developed. For the first three transcripts, each member of the team indexed two transcripts (meaning each transcript was indexed by at least two people). We then met to compare our indexing, discussing any challenges or uncertainty around the application of framework concepts, whether any definitions needed refining, and whether any codes needed merging. We also discussed proposed additional codes, deciding which ones to add to our framework. Based on discussion at this meeting, we created version 2.0 of our framework. GA and ST then re-indexed the first three transcripts using the new version of the framework, and indexed the subsequent three transcripts, so each transcript was indexed by a single person. Progress with data collection and indexing was discussed at weekly team meetings. GA and ST fed back that Version 2.0 of the framework was easier to apply and they did not feel any additional changes were needed at that stage. Indexing continued with single indexers until all transcripts were indexed.
The next stage of analysis was reviewing data extracts for each framework concept. Each member of the team was allocated items from the framework to review. This involved reading all the data extracts indexed to that framework item, considering whether they were all about the same concept, whether they needed to be moved to a different item, whether the framework needed to be refined in terms of amending labels or how they were applied, new items created, items dropped from the framework or merged with other items. Following this, we met to discuss the framework and potential changes to it. Where the reviewer was unsure about the indexing of a particular data item, these were discussed in the meeting. Following this, we created version 3.0 of the framework and applied it to the data.
We then proceeded to the charting and summarising stage of analysis. We created four framework matrices, each containing several framework domains as column headers, and each interviewee as a row. GA & ST created summaries of the data for each cell, summarising data from each interviewee related to the column header. Following this, all team members read all the matrices, reading down the columns rather than across the rows, thinking about the range of perceptions, views, experiences and behaviours described in each column, and differences between the interviewees. We sought to identify potential links between the columns, and elements contained within them. We then met to discuss our thoughts and reflections, including whether the columns in each of the four matrices belonged together. From this, AS drafted three major themes, attempting to summarise patterns of shared meaning within the data. These were discussed at a team meeting, including the content that fitted under each theme heading. An audit trail of our analysis was kept in the NVivo project.
Ethical considerations
This study was approved by the UCL Research Ethics Committee (study ID 28633.001) on October 22, 2024. All participants gave written informed consent to take part in this study before starting interviews.
Results
Participants
Participant characteristics.
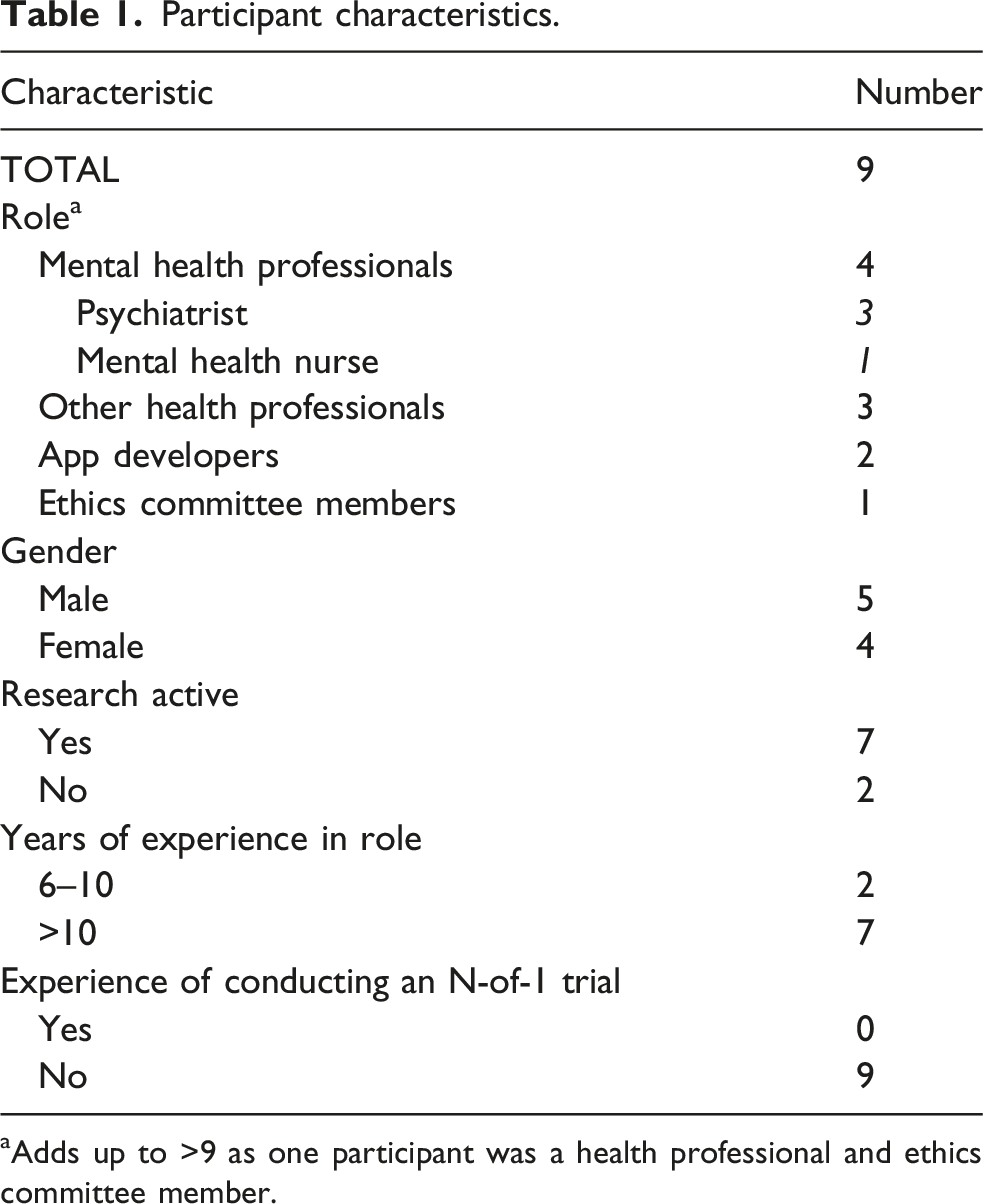
aAdds up to >9 as one participant was a health professional and ethics committee member.
Framework
The final version of our framework (version 3) 27 incorporated 11 of the 14 Theoretical Domains Framework domains. The Theoretical Domains Framework domains that were not included due to lack of relevant data were: motivation and goals; emotion; and behavioural regulation. In addition to domains from the Theoretical Domains Framework, our framework also included a domain on the Nature of N-of-1 trials, which includes data around the nature of N-of-1 trials and how that affects use or non-use of them in the context of mental health. It also includes advantages/benefits of N-of-1 trials (e.g. shared decision making, finding evidence of effectiveness, potential to improve decision making), and discussion around the nature of evidence N-of-1 trials give.
We developed three major themes, which are discussed in the sections below. Figure 1 shows how our themes relate to the domains of our framework. Across these themes we identified perceived barriers and facilitators.
27
Themes and framework domains.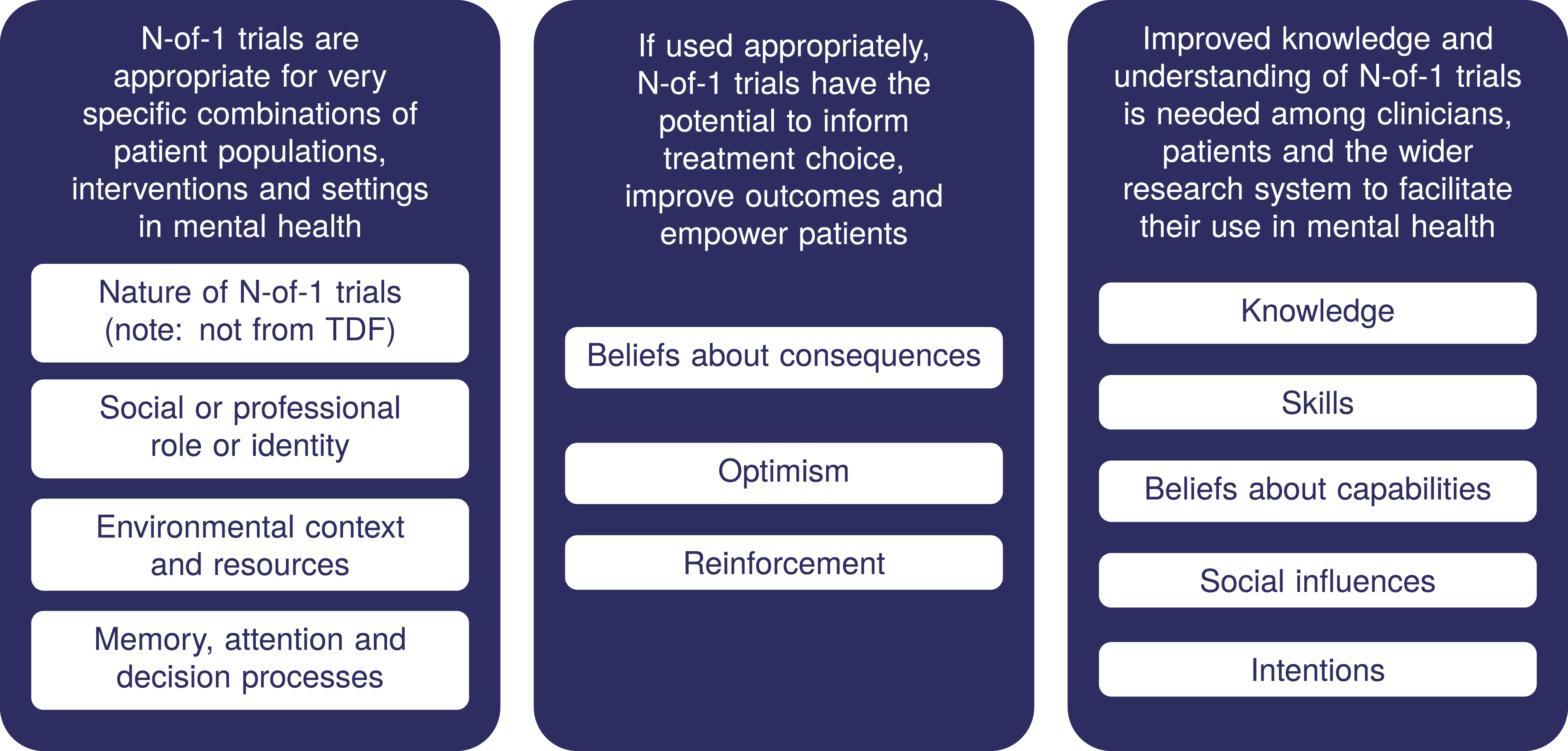
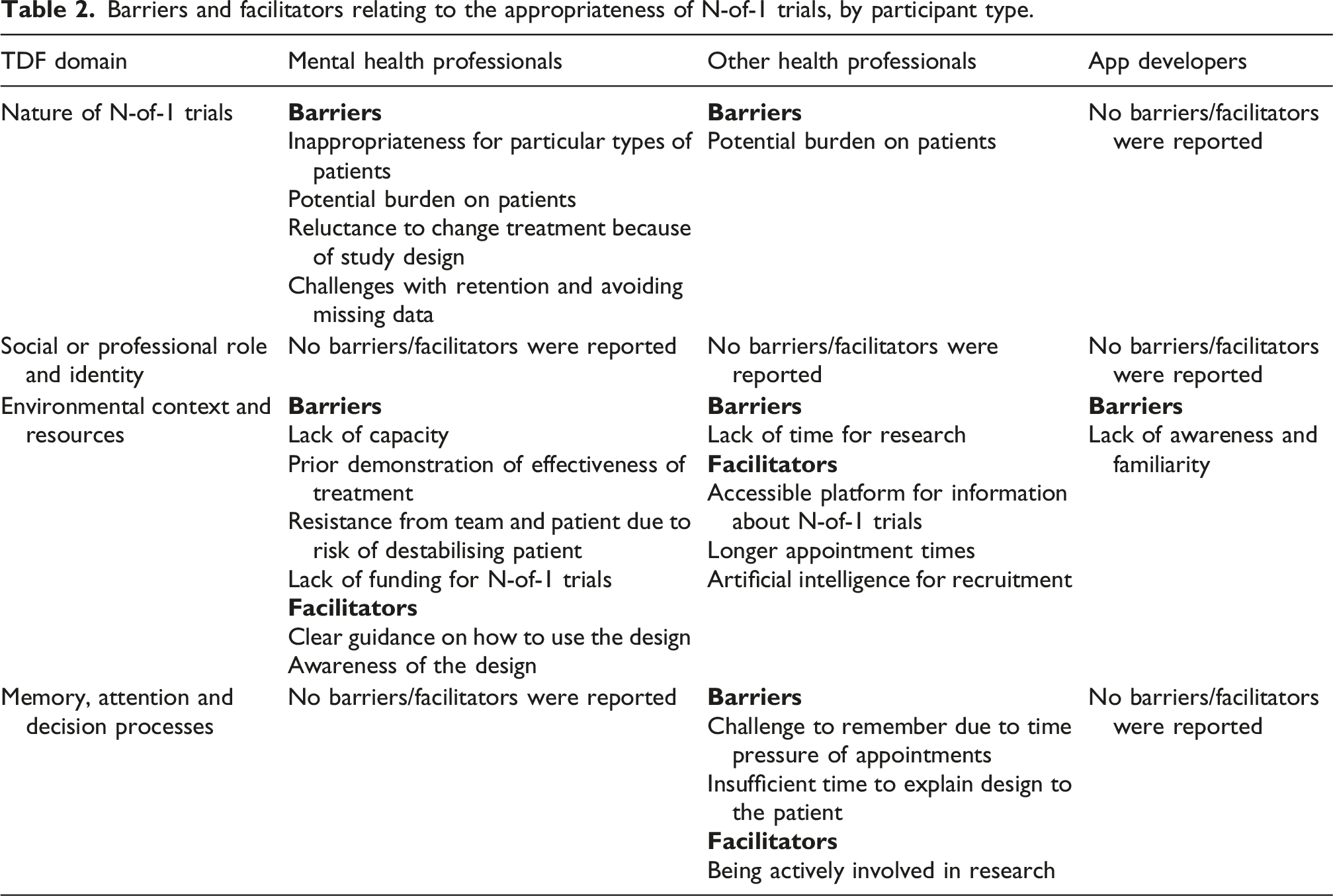
N-of-1 trial designs are appropriate for very specific combinations of patient populations, interventions and settings in mental health
Interviewees felt that N-of-1 trials could be appropriate for some specific types of mental health conditions, interventions and settings. It was seen as appropriate for people with stable chronic illnesses where treatment is not curative. Anxiety, obsessive-compulsive disorders, social phobias and depression were all named as potential conditions where N-of-1 trials could be useful. Conversely, mental health conditions which were short-term, where patients were critically unwell, at risk of suicide, or where potential participants lack capacity to understand the trial process or give informed consent were seen as less suitable. Some interviewees said they thought that patients who are treatment resistant, or who had previously tried multiple treatment options for their conditions, might be more appropriate, or more likely to agree to take part, in N-of-1 trials. I don't see N-of-1 trials having a role in the treatment of patients with chronic psychotic severe disorders, however, in other settings where I might be working, such as in anxiety disorders or phobia phobic disorders… I would be more likely to think it would be of benefit there. PS01, Psychiatrist For treatment resistant conditions, that's what I think… this might have potential because then you're exposing potential treatments to patients that already, like, showed that they don't respond to the current guidelines, which builds on the needs to… diversify approaches and provide different treatment options to the same patient in a standardized ways that then can be like evaluated and… reported and in a robust statistical way. PS03, Psychiatrist
Some pharmacological interventions were deemed unsuitable for N-of-1 trials because of the risk of side-effects or rebounds when switching treatment, and the risk of destabilising patients. While some viewed therapies such as talking therapies as more suitable for N-of-1 trials, others felt that interventions such as cognitive behavioural therapy might be inappropriate because the effect of the intervention might be long-lasting, beyond the intervention period, and unfeasible to wash-out.
While participants were generally positive about the potential of N-of-1 trials for some mental health conditions and interventions, the setting in which they should be carried out was unclear. One participant working in the primary care setting said they felt secondary care might be the more appropriate setting for N-of-1 trials. Running N-of-1 trials in primary care may be logistically challenging due to the short duration of appointments, and need for extra appointments for follow-ups. Within the secondary care setting, one psychiatrist suggested that N-of-1 trials could work if they are more embedded in clinical service delivery than clinical trials currently are. I would need a longer appointment to explain this sort of thing. So I'm, you know, I'm booked back-to-back pretty much every day in all the surgeries I go to. So I don't have a lot of time. So where would this extra time come from? And then it would, as I said earlier on, it would require longer term follow-ups with people. Then again. I wouldn't normally do so. Would I have the capacity to do that? NU01, Nurse (Primary Care) I think there needs to be an organizational shift. So that the N-of-1 trials are much, much, much, much more part of the clinical service delivery than the current trials are. PS03, Psychiatrist
Data collection for N-of-1 trials was perceived as being potentially burdensome for participants, with the risk of participant fatigue with repeated measures leading to missing data. Making sure data collection is short and simple, making sure that participants understand why it is important to complete the forms, and potentially offering financial incentives were all proposed as approaches to addressing this problem. So, for example, you give them some incentive for each data point collected and then a bonus at the end if they've collected the whole lot. That could be an option, and they [PPI group] felt that was ethical because you're paying people for their time and going over and above. PS02, Psychiatrist
Interviewees highlighted the need to ensure that potential trial participants understand the trial design, and what is involved. Several participants raised ethical concerns around having to switch patients who are doing well on a treatment, at the end of the treatment period in an N-of-1 trial. Transparency around this is important when explaining the trial to potential participants. Others highlighted the potential benefits of a trial design where the participant knows they will receive the intervention for at least some of the time, particularly in situations where people would be reluctant to join a standard trial where they might be randomised to the control arm throughout. I could not ethically destabilize very critically unwell patients on established multi-medicine regimes to enter them into N-of-1 trial for a psychotic disorder. I couldn't ethically justify that. PS01, Psychiatrist I guess the concern would be around the ethics of it. But then I guess if you're not entirely sure of a treatment decision in the first place, it may be not the same ethical dilemma. And I guess. yeah, the patient would obviously need to be fully consenting on board with it, but that would be the case anyway for research. NU01, Nurse
One challenge raised around conducting N-of-1 trials was the need for ethical approval; the complexity, work and length of time involved in this, in relation to a study which only has one participant. I'd love to use N-of-1 trial, but you've got to also remember if you're doing any research, i.e., N-of-1 would be considered research, you've then got to get ethics approval. An ethics approval on patients now in the NHS takes probably 6 months to a year. So you're putting in an enormous amount of work for very small number of patients. PS02, Psychiatrist
Barriers and facilitators relating to the appropriateness of N-of-1 trials, by participant type.
If used appropriately, N-of-1 trials have the potential to inform treatment choice, improve outcomes and empower patients
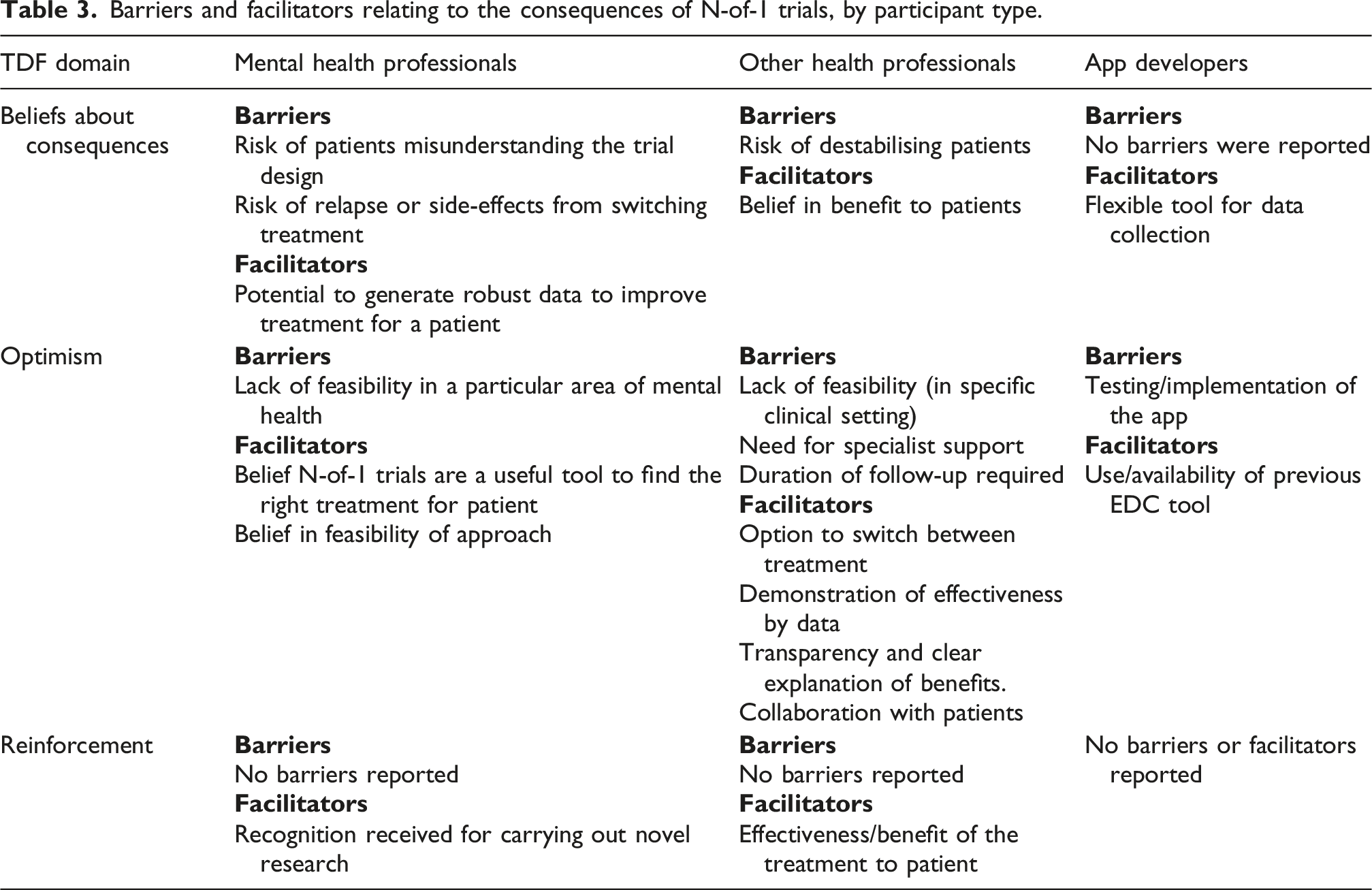
Participants identified potential benefits of N-of-1 trials, if used appropriately (see previous theme). Through providing robust evidence of the effectiveness of interventions for a particular person, N-of-1 trials were felt to have the potential to allow better informed treatment choices and improve outcomes. They may also help through educating health professionals on different treatment options and potentially making them more effective in their role. However, as discussed in the previous theme, if N-of-1 trials are used for interventions or health conditions that they are not appropriate for, there is a risk of destabilising patients. Interventions don't always work in people and the kind of average result of a study that you know not indicate that there's a difference. Or the product doesn't have any efficacy, but actually in a small number of people that might actually be really effective. So targeting people, I think we're quite on board with that. AP01, App Developer I suppose it could be a useful tool again if you were struggling to find the right treatment for a patient. And it would give you, you know, perhaps if you were used to always prescribing the same medication, it might give you more exposure to different ones that might provide a better effect for some people. So yeah, I suppose it's kind of educating yourself on different options. And giving different options to patients which might be better than the, you know, the first line standard that you might prescribe. GP01, General Practitioner
Alongside this, some participants felt it may also have benefits for the clinician-patient relationship, talking about N-of-1 trials allowing collaboration with patients, giving patients autonomy and empowering their decision-making. Conversely, there is potential for damaging the relationship between health professionals and patients if the trial design is not well explained. Other participants were concerned that it could negatively affect the clinician-patient relationship through undermining patients’ confidence in the treatment by expressing uncertainty about the effectiveness of the treatment being trialled. This issue is not unique to N-of-1 trials. In term[s] of collaboration with the patients, I think it really helps us to open up for a different perspective. Also the patient can feel more empowered in their decision making. ECNU01, Mental Health Nurse If you tell patients you're undertaking research, it inevitably means that there's no clear treatment that works. If it's research, why research something if you already know it works. So that could make the patient less confident in the treatment. PS02, Psychiatrist
The app developers were positive about the potential of N-of-1 trials, drawing connections between the design and current trends in research such as personalised medicine, adaptive trials and cross-over trials. As personalised healthcare is becoming more important, it seems like it's kind of the way forward. AP01, App Developer I'd love to think about the way that we might use N-of-1 in an adaptive trial, I think that is that is a really interesting question. AP02, App Developer
Barriers and facilitators relating to the consequences of N-of-1 trials, by participant type.
Improved knowledge and understanding of N-of-1 trials is needed among clinicians, patients and the wider research system to facilitate the use of this trial design in mental health
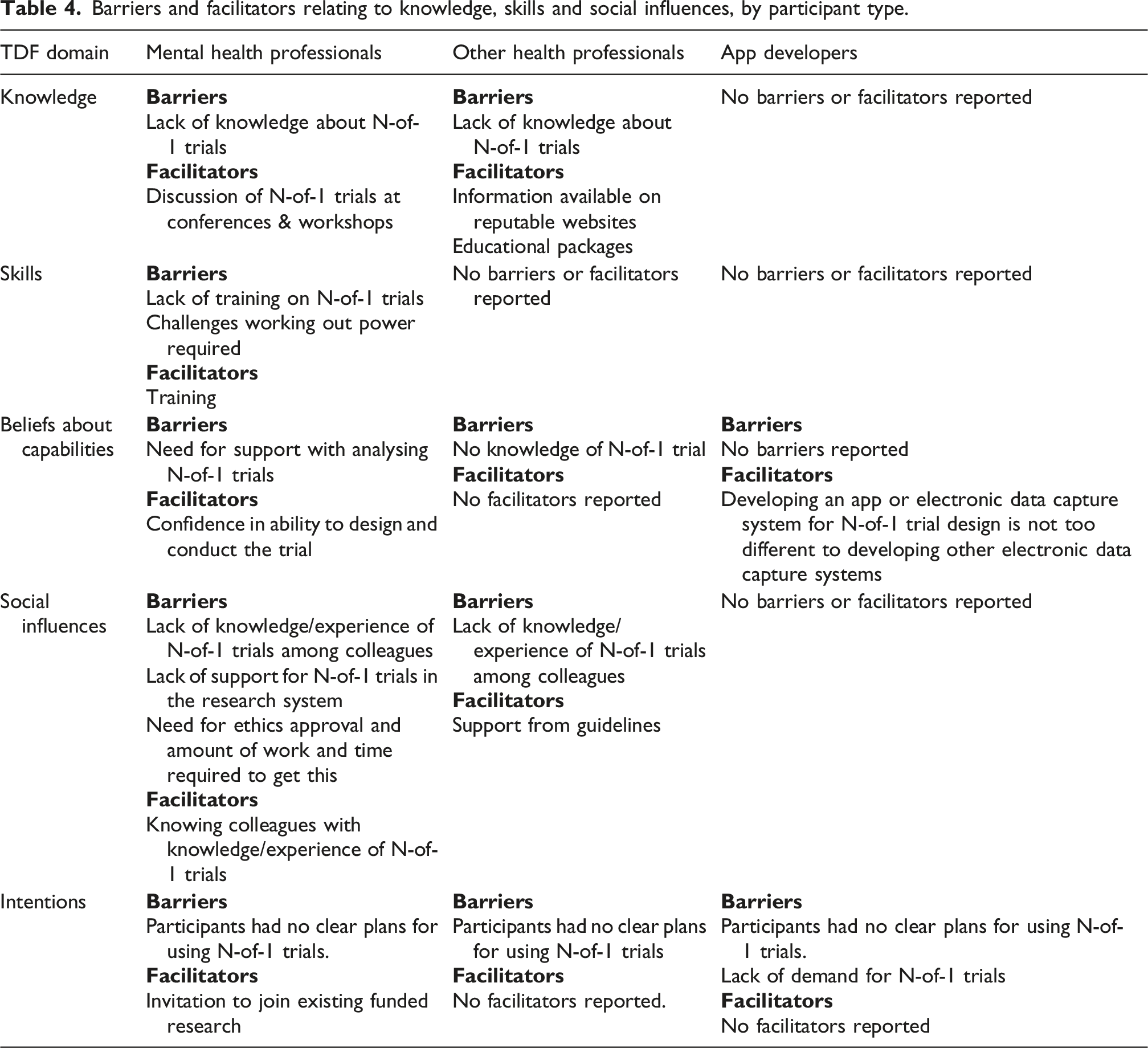
While participants were able to see the potential benefits of N-of-1 trials in mental health, none had intentions of using the design in the next year, nor a clear plan of how they would use it. The main barrier to the use of N-of-1 trials in mental health was lack of knowledge and experience of the design among the interviewees themselves, their colleagues and the wider research system. Most interviewees had heard of N-of-1 trials and were able to provide basic descriptions (often guesses). Most said they currently did not know enough about N-of-1 trials to be able to use the design and believed that their colleagues also did not know much about N-of-1 trials. I’m not familiar. I joined the interview just because I wanted to know a bit more. And I was curious to explore this. ECNU01, Mental Health Nurse and Ethics Committee Member I don't think many of them would have heard of it. Certainly not within the nursing staff. Some of the doctors potentially would. I've never come across anyone doing an N-of-1 trial in mental health. Ever. NU01, Mental Health Nurse
The sources of knowledge mentioned by the few participants who were more familiar with the N-of-1 trial design include conferences and workshops, papers, and colleagues with expertise in this area. None had experience of being involved in the conduct of an N-of-1 trial, and the Ethics Committee member had not been involved in reviewing any N-of-1 trials. When participants were asked where they would look to find more information on N-of-1 trials, most talked about web searches, looking for information from reputable sites. Some talked about wanting some kind of educational package to help them learn about the design and conduct of N-of-1 trials. Another approach that was thought would help people start to use N-of-1 trials was being able to learn from others who had carried them out. So I think some kind of educational package would be useful that you could direct people to, probably an interactive thing. I think something that people would be self-directed that people could do in their own time because everybody's busy kind of trying to attend training things, I think that just wouldn't work. So yeah, I think an online learning package, I know that, but I think an established place like the NIHR website where they do some training or for example in the NHS we do, we have like an e-learning for health program. OC01, Other Clinician
In terms of the skills required to carry out an N-of-1 trial, most of the clinical interviewees felt they would need additional training or support with designing and analysing N-of-1 trials. Some felt they could explain the design to patients, while others did not feel confident with this either. I think once I got my head round I wouldn't need help explaining it to a patient. NU01, Mental health nurse The design is quite different to any other trial design that I've had, I think the analysis I wouldn't even really know where to start with that and then the explanation to the patient. Yeah. I would need to figure out a way to explain that. OC01, Other clinician
The app developers we spoke to were more confident that they had the skills needed to apply the N-of-1 design, seeing the design as suitable for the platforms they use, and fitting with other trends in clinical research, but needing more help with designing the trial. So a bit more research, a bit more understanding and I think we'd be able to run at least a prototype level trial or feasibility study level trial. You know pilot, something like that. AP02, App Developer Designing a trial and designing how to extract the best outputs out of that or analysis is probably where we need help. AP02, App Developer
As N-of-1 trials were so little talked about or carried out in the area of mental health, some participants were unsure how they would be regarded by clinical colleagues, which could pose a barrier to their uptake. Only one interviewee had attempted to use N-of-1 trials in the past, putting in funding applications, which had been met with resistance both from clinical trials units and research funders. The things I would like to know before doing an N of one is, is how it's regarded in the in the space that we're in, right? So would it be something that people would go oh, that's interesting. What an interesting approach you've taken there. Or would it be something that they would think was just a fad or you know, something like that, that I couldn’t answer that at the moment. AP02, App Developer So if the leaders of departments and statistics are saying that N-of-1 trials aren't valid it's very hard to swim against the current you know. PS02, Psychiatrist I've been previously a member of [major funding panel] and whenever you know someone suggested a N-of-1 trial, I think we had one application and as well as ours, and on both occasions, people said no, it's not a randomised control trial and that was you know, so it wasn't even considered. And I think that's an error of judgement actually, but I'm a convert. PS02, Psychiatrist The UK [has] really been a bit slow to take up the mantle of leading on N-of-1 and maybe having a unit setting up funding format and for funding bodies to have maybe dedicated funding, that's where I would do it. PS02, Psychiatrist
The influence of patients’ expected reactions to the offer of N-of-1 trials was unclear, as often interviewees recognised that the design would appeal to some participants and not others. One mental health nurse, while anticipating that many of her patients would not want to take part in an N-of-1 trial, felt that it was not the role of clinicians to decide in advance on the patient’s behalf. Those who have characteristics of novelty seeking, probably they would be more interested in an N-of-1 trial in which they would be exposed to different, you know, like treatments. Whereas those who are more concerned or suspicious probably they would face more barriers. PS03, Psychiatrist I think if the opportunities are there, people should be offered it and it's their decision then if they want to take part or not. You know, I think too often clinicians are the gatekeepers… It should be easier for patients to access research studies without having to go through clinicians. NU01, Mental Health Nurse
Barriers and facilitators relating to knowledge, skills and social influences, by participant type.
Discussion
Based on our findings from interviews with health professionals who care for people with mental health conditions, and mental health app developers, we believe there is a potential role for N-of-1 trials in mental health. This role is quite specific: in people with stable chronic illnesses where treatment is not curative, who have capacity to understand the trial design, for interventions that are not expected to have long-lasting effects or cause problems when discontinued, and in settings where participants can be followed-up for the duration of the trial. In scenarios where these conditions are met, N-of-1 trials have the potential to inform treatment choice, improve outcomes and empower patients. However, we found substantial barriers to using this trial design in the current UK health and research system. We found low levels of knowledge and familiarity with the N-of-1 design, with none of our participants having been involved in the conduct of N-of-1 trials, and one being aware of colleagues using this type of trial. The one participant who had attempted to get funding for N-of-1 trials had met with resistance from both research funders and researchers. Participants also anticipated the workload involved in getting ethical approval for such small trials being a formidable barrier. If N-of-1 trials are to achieve their potential benefits in the context of mental health, considerable effort is needed to improve knowledge of the trial design among health professionals, researchers and those involved in funding and ethics decisions.
As part of this work we carried out a PPI workshop involving people with lived experience of mental health challenges. The PPI participants’ concerns were perhaps more sobering than some of those noted in interviews. The following challenges were noted: • That mental health issues often arise in the context of or are exacerbated by other health problems. • Participants would be unwilling to risk switching treatment when outcomes are good or, conversely, staying with current treatment when outcomes are bad. • Similarly, allocation concealment (not knowing the upcoming treatments until the treatment period begins) would pose a problem for participants. • N-of-1 trials would be inappropriate for people with manic episodes. • Participants would entertain N-of-1 trials for lifestyle interventions (behavioural nudges, for example) but understandably not drug treatments that require titration or talking therapies.
There were also some positives regarding N-of-1 trials: • Data collection would be acceptable if there seemed to be a potential reward of learning which treatment/s “work”. • It seems safer to try a treatment on oneself than risk trusting results based on people who do not represent one.
And finally, some practical points: • Would need regular access to health professional monitoring progress, which is not always available. • Having an app or platform to record data, and this going directly to a GP, would be a motivator, though there is always concern about how your data might trigger care decisions.
Research team reflections on the project
Across the project, we collectively deepened our understanding of the practical, ethical, and methodological challenges of implementing N-of-1 trials in mental health. We found that N-of-1 trials were used even less frequently than anticipated and that the obstacles to their use in the area of mental health were more substantial than we initially appreciated. We observed consistent enthusiasm for the general concept of N-of-1 trials among participants, but this enthusiasm rarely translated into perceived feasibility in real-world practice. The use of framework analysis and the Theoretical Domains Framework supported us in identifying cross-cutting barriers and facilitators and fostered a shared understanding of the contextual factors shaping attitudes towards N-of-1 trials.
As a team with differing levels of prior experience in qualitative research, clinical trials methodology, mental health research, and N-of-1 designs, our combined perspectives inevitably shaped aspects of data collection and interpretation. Team members new to N-of-1 trials may have encouraged participants to elaborate on uncertainties or foundational concepts. Initial expectations, such as anticipating low familiarity with N-of-1 trials or expecting positive views on personalised approaches, may also have subtly influenced the framing of questions and early interpretations. However, our collaborative analytic process, regular discussion of potential themes, and use of a structured framework helped counterbalance individual assumptions and support a more reflexive and transparent interpretation of the data.
How our findings relate to the wider literature
This article began by quoting a description of N-of-1 trials as “underused”. Our findings have shown that the design appears to be unfamiliar to people familiar with parallel-group trials in mental health. However, some very influential experiments involved N-of-1 designs. 27
Our finding that stakeholders believed N-of-1 trials could help inform individual treatment choices align with the results of the systematic review of N-of-1 trials for depression. 13 Two of the studies in the review were in people with treatment-resistant depression, which again aligns with our findings suggesting the treatment-resistant setting might be particularly appropriate for this trial design. The review of N-of-1 trials in schizophrenia concluded that N-of-1 trials are feasible and potentially valuable for a range of interventions in schizophrenia, 14 which is perhaps more positive about the potential of N-of-1 trials in this setting than our participants were.
Relatively little implementation science work has been done looking at the implementation of specific trial designs or trial methodology developments. One study used the Consolidated Framework for Implementation Research, the COM-B framework and Behaviour Change Wheel to look at uptake of four trial methodology developments in clinical trials units in the UK. 20 This did not look at a trial design, but at an issue within the design of trials (progression criteria for internal pilot studies) alongside three other methodology topics. They identify three potential solutions to improving the uptake of trial methodology: improving awareness of trial method research findings; reducing effort required to implement those findings (e.g. through provision of templates, software, case studies of implementation); and changes to culture within clinical trials units towards implementing new methods (supported through the provision of funding to allow the time required for this). 20 These findings chime with ours around the need for improved awareness of N-of-1 designs and training; more published examples of successful implementation of these designs in mental health, and the need for changes to research system to facilitate use of N-of-1 designs (through better understanding of the design among clinical trials units, ethics committees and funders).
Strengths and limitations
We applied an established, validated implementation science theoretical framework (the Theoretical Domains Framework) to inform our topic guide and analysis. Our study is the first (to our knowledge) to apply the Theoretical Domains Framework to a question around implementation of a trial design. The data we collected were rich, and from a variety of perspectives, including psychiatrists, mental health nurses, other health professionals and mental health app developers. However, we recruited fewer participants than planned. Only one participant interviewed had prior knowledge of N-of-1 trials and no-one had experience of running an N-of-1 trial, meaning we were unable to explore issues that might arise in the course of conduct of an N-of-1 trial in mental health. This meant some of our interviews were shorter than anticipated (22–47 min), as some of the questions were only relevant to those with experience of conducting N-of-1 trials. Only one participant was an ethics committee member, so we were unable explore this aspect as much as we would have liked. These challenges limit the breadth of our findings, and meant we had to focus on what people anticipated would be barriers and facilitators to conducting N-of-1 trials in their setting, rather than actual experience of this.
Future challenges
Important questions remain around the regulatory and ethical aspects of N-of-1 trials. We are not trying to encourage people to experiment on themselves, without consulting their clinicians. There are risks associated with any trial, and proper clinical oversight is needed to ensure patient safety. Currently, in the UK, most clinicians are not in a position to offer this support to patients who would like to use N-of-1 trials to find the best treatments for themselves, due to lack of knowledge and training, and an unsupportive research system. Better education of health professionals around N-of-1 trials could help them support patients who may be able to benefit from this truly personalised approach to treatment. A digital platform that can guide clinicians and patients to design, conduct and analyse appropriate N-of-1 trials of low-risk interventions may be a useful starting point. More published examples of where N-of-1 trial design has been used in practice in mental health would be helpful.
Conclusion
Our findings suggest that, although N-of-1 trials are seldom used in mental health, there is a potential role for this design in mental health in specific circumstances, for people with stable, chronic conditions, and where interventions can be safely discontinued and re-started. In these contexts, N-of-1 trials may offer a structured way of informing treatment choice, improving outcomes and, in some cases, supporting patient empowerment. At the same time, the barriers we identified, including little awareness of N-of-1 trials among clinicians and researchers, uncertainty around analysis and design, and practical challenges related to ethics and research infrastructure, highlight that substantial work is needed before such trials can be routinely implemented in mental health settings.
Our study provides an initial step towards addressing these challenges by outlining where the design may be most appropriate and by identifying the knowledge, skills and system-level supports required to make its use feasible. Future work can build on these findings by developing accessible training and guidance for clinicians, researchers and ethics committees; publishing results from N-of-1 trials conducted in mental health contexts to provide examples others can learn from; and exploring streamlined ethical and operational pathways.
As interest in personalised and patient-centred approaches continues to grow, our results offer a foundation for understanding how N-of-1 trials might be used more effectively and safely within mental health, and what is needed for them to become a realistic option within clinical and research practice.
Supplemental material
Supplemental Material - N-of-1 trial designs in mental health: A qualitative study of their appropriateness, and barriers and facilitators to their use
Supplemental Material for N-of-1 trial designs in mental health: A qualitative study of their appropriateness, and barriers and facilitators to their use by Annabelle South, Shiva Taheri, Gideon Asamoah, and Tim P. Morris in Research Methods in Medicine & Health Sciences.
Footnotes
Acknowledgements
The authors wish to acknowledge our colleagues Grisma Patel, Kate Sturgeon and Sophie Merrick for their support with this project. We would also like to thank the PPI contributors and study participants for sharing their experiences and views on the topic. Please note that acknowledgement of the above individuals does not imply their endorsement of this paper.
Ethical considerations
This study was approved by the UCL Research Ethics Committee (study ID 28633.001) on October 22, 2024.
Consent to participate
All participants gave written informed consent to take part in this study before starting interviews.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the NIHR/MRC Trials Methodology Research Partnership. The salaries of TPM and AS were funded through Medical Research Council core funding (MC_UU_00004/09).
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AS, ST & GA declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. TPM has received consultancy fees from Novartis Pharma AG, Bayer Healthcare Pharmaceuticals, Alliance Pharmaceuticals, Gilead Sciences, and Kite Pharma, and owns shares in Novartis Pharma AG.
Data Availability Statement
The anonymised transcripts that support the findings of this study are available via a controlled access approach in line with the Innovative Clinical Trials Unit at UCL Data Sharing policy https://mrcctu.ucl.ac.uk/our-research/other-research-policy/data-sharing/![]() Initial enquiries about the availability of the data should be addressed to the corresponding author.
Initial enquiries about the availability of the data should be addressed to the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.