
Abstract
This case report outlines the successful management of a large, chronic oroantral fistula (OAF) using a three-layer closure technique in a 55-year-old male who reported nasal fluid leakage several months after maxillary molar extraction. Imaging confirmed a large communication between the oral cavity and maxillary sinus. Surgical closure was performed under general anesthesia using nasal intubation. A cortical bone graft from the chin reconstructed the bony defect, followed by the placement of a buccal fat pad (BFP) and coverage with a buccal advancement flap. Platelet-rich plasma (PRP) was applied over the graft and soft tissue layers to accelerate healing and enhance tissue regeneration. Postoperative recovery was smooth, with complete resolution of symptoms and no complications noted during follow-up. This case emphasizes the effectiveness of combining autologous bone grafting, soft tissue coverage, and PRP application in managing large chronic fistulas, providing stable outcomes and improved healing in complex clinical scenarios.
Introduction
An oroantral fistula (OAF) is an abnormal, epithelial-lined connection between the oral cavity and the maxillary sinus. It most commonly develops as a complication after dental extractions, infections of the maxilla, or removal of cysts and tumors. 1 If an oroantral communication is not addressed promptly, it may epithelialize within 24-72 h, resulting in a persistent fistulous tract that can lead to chronic sinus infections. 2
OAFs most frequently occur in the maxillary premolar and molar regions. Typical symptoms include fluid regurgitation into the nose, altered speech resonance, difficulty in retaining liquids in the mouth, and a hissing sound during the Valsalva maneuver. While small defects (<3 mm) may heal on their own or with minimal suturing, larger fistulas (>5 mm) often require surgical correction. 3
The surgical procedure offers several options, including buccal flaps, palatal flaps, tongue flaps, and bone grafting. The choice depends on the size and position of the defect.
Autogenous bone grafts are recommended for wide OAF closure to achieve optimal outcomes. Grafts from various donor sites have been successfully employed in this procedure. Iliac crest grafts have been used for closing large OAF, 4 but this method requires an additional surgical procedure and may lead to considerable complications at the donor site. As a result, alternative sites are often preferred to reduce these issues. Common alternatives include the chin, 5 tuberosity, 6 ramus of the mandible, 7 and zygomatic bone. 8
The application of chin grafts in the treatment of OAF has yielded positive clinical results. Although chin grafts are widely utilized in various reconstructive surgeries, their specific role in OAF management appears to be infrequently documented and may be underrepresented in the current literature.
In managing large OAFs, along with soft-tissue flap and bone graft, the buccal fat pad (BFP) is also used, as it serves as an excellent reconstructive option due to its rich blood supply and ease of mobilization, promoting rapid tissue coverage. To enhance the healing process significantly, platelet-rich plasma (PRP), which is rich in growth factors, is also used. This also leads to faster regeneration and improved clinical outcomes.
This case report highlights the successful management of a large OAF using a three-layer closure technique (combination of chin graft, BFP, and buccal advancement flap) along with PRP. This method provided durable closure, promoted rapid healing, and yielded excellent functional outcomes.
Case Presentation
A 55-year-old male presented to the Oral and Maxillofacial Surgery Unit, Department of Dentistry, at a Government Medical Institute with complaints of nasal fluid leakage while drinking, persisting since the extraction of his maxillary left first and second molars at a private clinic 6 months ago. Despite consulting multiple clinics during this period, he had not received effective treatment, and ultimately reported to our center for further management. Clinical examination revealed a well-defined, round fistulous opening was observed in the maxillary molar region with healthy surrounding mucosa and an underlying bony defect (Figure 1a). There were no signs of acute maxillary sinusitis or discharge.
(a) Oro-antral Opening at Maxillary Molar Region. (b) Orthopantomogram. (c-e) Non-contrast Computed Tomography (NCCT) Scan Showing 14.1 × 10.2 mm Oroantral Communication in the Region of the Maxillary Second Molar.
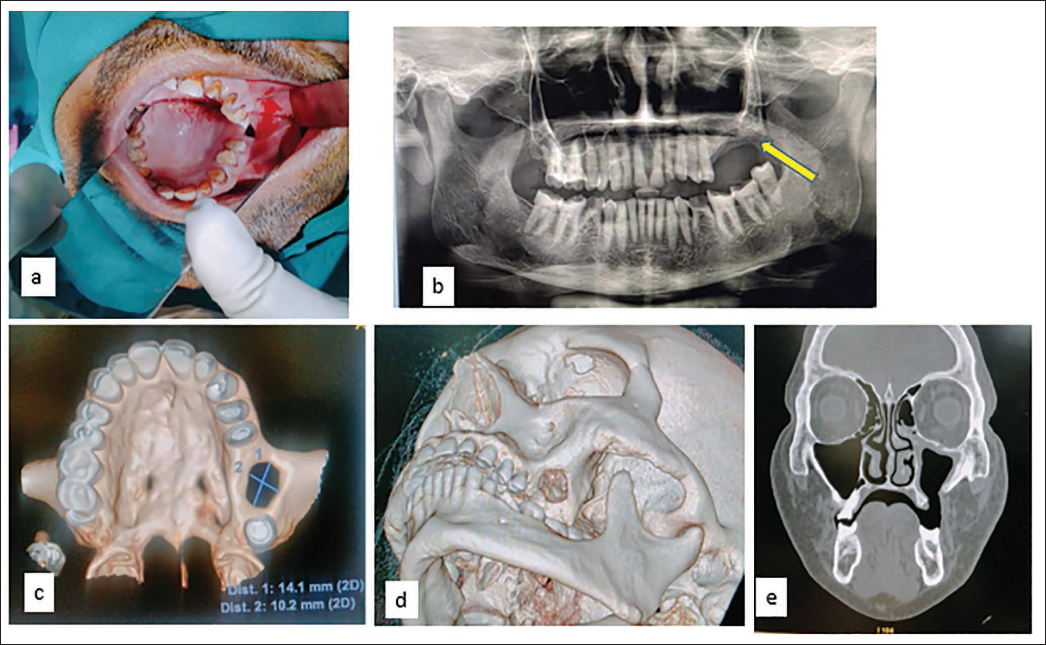
An orthopantomogram (Figure 1b) and non-contrast computed tomography (NCCT) scan (Figure 1c, 1d, 1e) were performed. The NCCT revealed a 14.1 × 10.2 mm oroantral communication in the region of the maxillary second molar, confirming a chronic OAF. Based on clinical and radiological findings, surgical closure was planned under general anesthesia using nasal intubation.
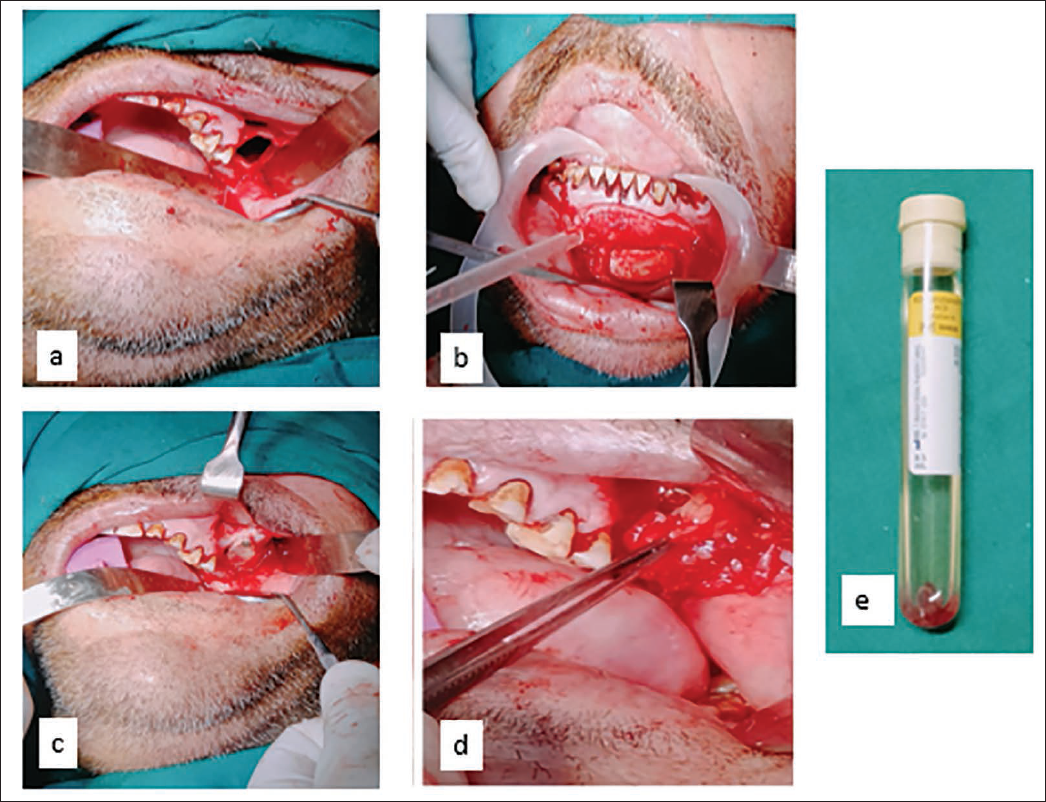
A buccal advancement flap technique was employed for a robust, multilayered closure. The fistulous tract was excised along with the surrounding epithelialized lining. A trapezoidal buccal mucoperiosteal flap was elevated (Figure 2a), and the periosteum was incised posteriorly to access the BFP, which was gently harvested by blunt dissection to cover the defect.
Simultaneously, a standard vestibular incision was made in the mandibular anterior region, and a cortical bone graft was harvested from the chin (Figure 2b). The graft was contoured to fit the defect and fixed in place using a 2.0 mm titanium screw (Figure 2c). Autologous PRP was applied over the graft to promote healing (Figure 2e). The BFP was then advanced over the graft, followed by repositioning of the mucoperiosteal flap, which was sutured with 3-0 Vicryl (Figure 2d).
(a) Buccal Mucoperiosteal Flap. (b) Mandibular Vestibular Incision to Harvest Chin Graft. (c) Chin Graft Fixed in Place Using a 2.0 mm Titanium Screw. (d) Buccal Fat Pad (BFP). (e) Autologous Platelet-rich Plasma.
This approach achieved a triple-layered closure, bone graft, BFP, and mucosal flap with PRP augmentation. Healing was uneventful, with no signs of infection or flap dehiscence. At 6 months follow-up, the patient remained asymptomatic, indicating successful closure of the chronic OAF (Figure 3).
Postoperative Photograph Showing Successful Closure of Oroantral Fistula (OAF).

Discussion
OAF most frequently arises as a complication following the extraction of posterior maxillary teeth, particularly molars, owing to the anatomical closeness of their root apices to the maxillary sinus floor. Incidence rates have been documented between 0.31% and 4.7%. 9 OAF closure requires careful consideration of several factors, including the size of the defect, the duration since its development, the presence of infection, and any foreign bodies.
Surgical repair of OAF can be technically challenging, particularly in cases of chronic or extensive defects. Long-term success is influenced not only by the surgical technique itself but also by anatomical and pathological considerations, including alveolar ridge height, vestibular depth, and sinus health. Preoperative management of any sinus or nasal pathology is essential to optimize healing and reduce recurrence.
In the present case, the primary objective was to achieve complete and secure closure of the communication between the oral cavity and the maxillary sinus, thereby preserving sinus drainage and preventing secondary infections.
To address the extensive defect, a three-layered closure was employed, as supported by Er et al. 10 and Weinstock et al., 11 who demonstrated that two-layer closures often fail to provide long-term stability in extensive defects and result in higher wound-dehiscence rates up to 20%. The reconstruction was carried out sequentially. Initially, a cortical bone graft harvested from the mandibular chin area was used to reconstruct the bony floor of the sinus. This was followed by the placement of BFP, selected for its rich vascularity, ease of mobilization, and capacity for rapid epithelialization. However, acknowledging the limitations of BFP alone in large defects, particularly due to volume constraints and postoperative shrinkage, a third layer was added using a buccal mucoperiosteal advancement flap. This ensured a tension-free, watertight closure and provided additional soft-tissue support. To further enhance soft-tissue healing, PRP was applied over the BFP. This bioactive scaffold supported angiogenesis and tissue regeneration, contributing to a favorable postoperative outcome. This comprehensive, three-layered approach allowed for effective closure of the OAF, restoration of the anatomical barrier, and long-term stability of both hard and soft tissues.
Conclusion
This case demonstrates that a structured, multilayered approach is highly effective for treating large, chronic OAF. Using a chin bone graft for skeletal support, a BFP for soft tissue coverage, and a buccal mucoperiosteal flap for final closure created a secure and durable seal. The additional use of PRP further enhanced healing by promoting tissue regeneration. Together, these components provided a stable reconstruction with an uneventful postoperative course. Successful OAF repair depends on strategically combining techniques tailored to the defect size to ensure optimal healing and long-term stability.
Footnotes
Declaration of Conflicting Interests
The authors declared no conflict of interest with respect to the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent were received and obtained, respectively, before initiating the study from all participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.