
Abstract
Background
Maxillofacial trauma is a critical subset of polytrauma that impacts both functional and esthetic outcomes. Timely and structured intervention by oral and maxillofacial surgeons is paramount for optimal recovery.
Objective
To present a departmental model for managing maxillofacial trauma through integrated infrastructure, hierarchical treatment strategies, and continuous innovation.
Methods
A retrospective and descriptive overview of infrastructure, patient demographics, treatment strategies, innovation, and research from a high-volume maxillofacial trauma unit over a defined time period.
Results
The department managed a significant and increasing caseload with year-on-year growth in trauma admissions. A tiered management approach—conservative, minimally invasive, and surgical—was employed. Innovations such as indigenous fixation devices and endoscopic techniques enhanced outcomes. The department also contributed substantially to research, patents, and community outreach.
Conclusion
A multidisciplinary, innovation-driven model with layered treatment protocols and academic integration can optimize maxillofacial trauma care in both urban and tertiary care centers.
Introduction
Maxillofacial trauma presents unique challenges due to the complex anatomical, functional, and esthetic components of the facial skeleton. Emergency management of airway compromise, hemorrhage, and disfigurement requires coordination between surgical specialties and robust infrastructure. This article presents a departmental model from a high-volume tertiary care center in India, illustrating the integration of clinical excellence, innovation, and research.
Infrastructure and Clinical Setup
The department is comprehensively equipped to handle all aspects of maxillofacial trauma care, functioning as a high-efficiency unit within the broader hospital trauma system. It features round-the-clock trauma response teams, ensuring immediate evaluation and stabilization of patients upon arrival. Dedicated operating theaters support both general and local anesthesia, enabling flexible surgical planning for a wide range of trauma cases, from minor lacerations to complex fractures (Figures 1-3). The presence of specialized oral and maxillofacial surgery (OMFS) wards (Figures 4 and 5) allows for condition-specific monitoring and treatment, staffed by clinicians trained in the nuances of facial trauma management. Inpatient facilities are structured to accommodate both short-term and extended recovery periods, with close clinical supervision, while the postoperative care units are designed to support early rehabilitation and minimize complications. Together, these resources enable the department to deliver prompt, coordinated, and evidence-based surgical interventions, reinforcing a model of multidisciplinary trauma care that emphasizes both efficiency and patient-centered outcomes.
Trauma Unit (General Anesthesia (GA) and Local Anesthesia (LA)); General Anesthesia Operating Theater (OT); Local Anesthesia OT.

Forty-bed Oral and Maxillofacial Surgery (OMFS) Ward; Special Surgical Ward (Trauma Center).

Patient Demographics and Caseload
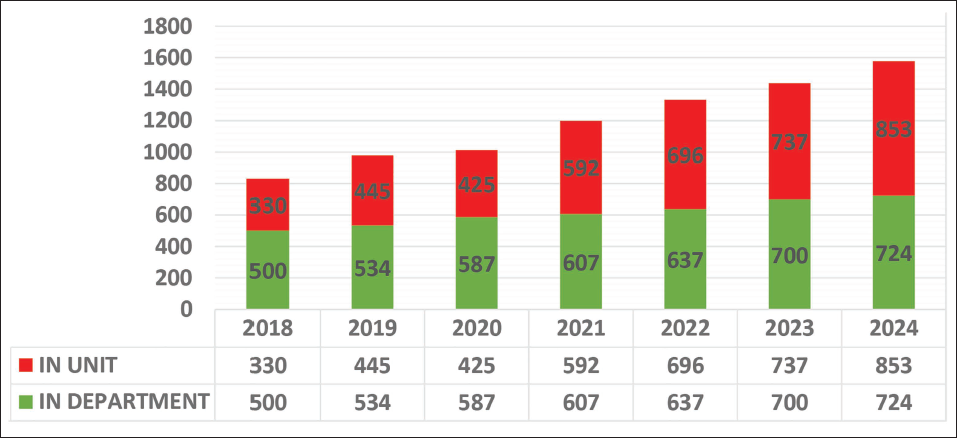
Over the past several years, the department has observed a significant and sustained increase in the volume of trauma admissions, with internal records indicating an approximate 100% rise (Figure 6) in maxillofacial trauma cases requiring hospital-based intervention. Figure 6 reveals an approximately two-fold (100%) increase in patient numbers over this period. Despite this significant rise, we have consistently managed to admit around 91% of all cases for treatment and further surgical procedures. Despite a two-fold increase in the number of patients, our trauma unit has successfully provided treatment for approximately 50% of all maxillofacial trauma cases reporting to us (Figure 7).
Chart Illustrating the Number of Maxillofacial Trauma Patients from 2018 to 2024. Note the 100% Increase in Patient Numbers.
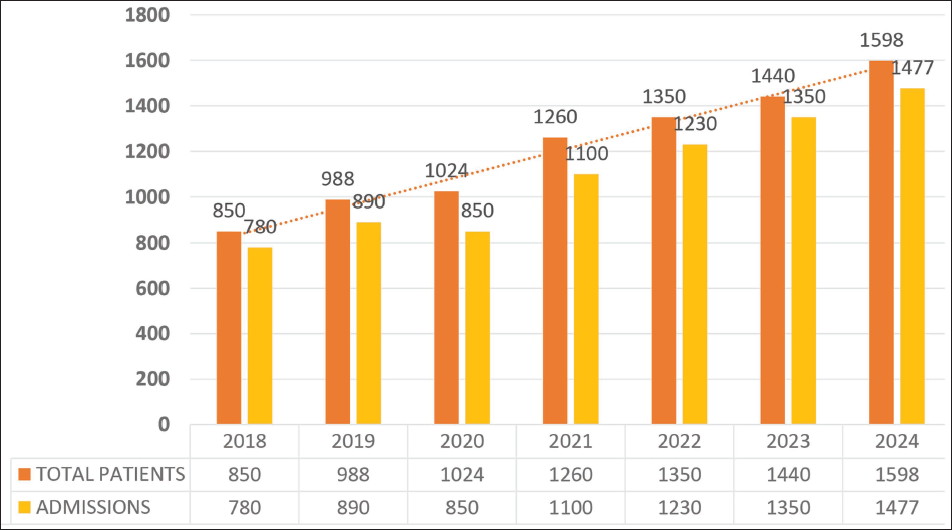
Chart Presents the Stratification of Patient Management Based on Their Treatment Location.
Notably, even during the COVID-19 pandemic in 2020, there was no decline in patient numbers, as our trauma center remained the sole operational facility providing essential treatment. This upward trend is reflective not only of changing patterns in trauma epidemiology but also of the growing recognition of the department as a regional center for specialized facial trauma care.
Upon presentation, all patients underwent a standardized and systematic initial assessment using the Advanced Trauma Life Support (ATLS)-based ABCDE approach, which emphasizes a prioritized evaluation of airway, breathing, circulation, disability, and exposure in the trauma center’s holding area.
We conduct comprehensive primary assessments in our OMFS trauma unit to ensure that no serious injuries are overlooked, hence our unit becomes a “Secondary Screen” (Figure 8a-8c). This protocol ensures that life-threatening conditions are promptly identified and managed, establishing a structured foundation for further diagnostic and therapeutic interventions.
Our Oral and Maxillofacial Surgery (OMFS) Trauma Unit Serving as a “Secondary Screen” for All the Trauma Patients Where All the ABCDE Assessment is Followed to Avoid Overlooking Any Missed Injury.

Anecdotally, cases with missed injuries were found, so a study was planned with 380 patients, where missed injuries in 7% cases were found. The findings of this study were later published, 1 highlighting a significant gap in pre-hospital trauma life support training. This training is crucial for ensuring timely and appropriate intervention, as its absence can lead to missed injuries that may result in increased patient morbidity and mortality.
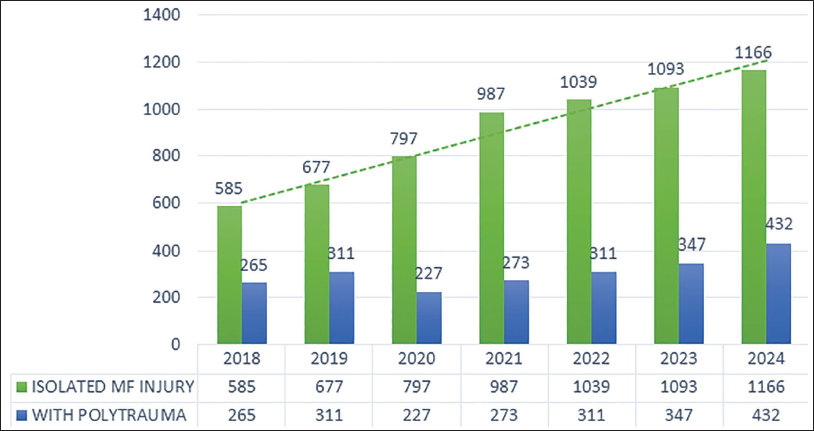
As a Level 1 trauma center, we handle a significant number of polytrauma cases. These patients typically sustain injuries involving multiple organ systems, necessitating a coordinated, multidisciplinary management strategy. In such cases, the involvement of various specialties, including neurosurgery, general surgery, anesthesiology, and critical care, was integral to comprehensive treatment planning and execution. Figure 9 compares the number of patients treated for isolated maxillofacial injuries with those presenting with polytrauma. Interdepartmental collaboration was essential not only during the acute resuscitative phase but also throughout the surgical and postoperative periods, ensuring that both maxillofacial injuries and systemic trauma were addressed in a cohesive and timely manner. This collaborative model exemplifies the department’s commitment to delivering high-quality, patient-centered trauma care that aligns with best practices and current clinical guidelines.
This Chart Compares the Number of Patients Treated for Isolated Maxillofacial Injuries with Those Presenting with Polytrauma. Approximately 45% of the Patients We Encounter have Polytrauma and Receive Coordinated Care with These Specialized Departments.
Emergency Management Protocols
The unit has demonstrated a consistent capacity to manage a wide spectrum of acute and often life-threatening maxillofacial trauma presentations, reflecting both the clinical expertise of the team and the efficiency of established emergency protocols.
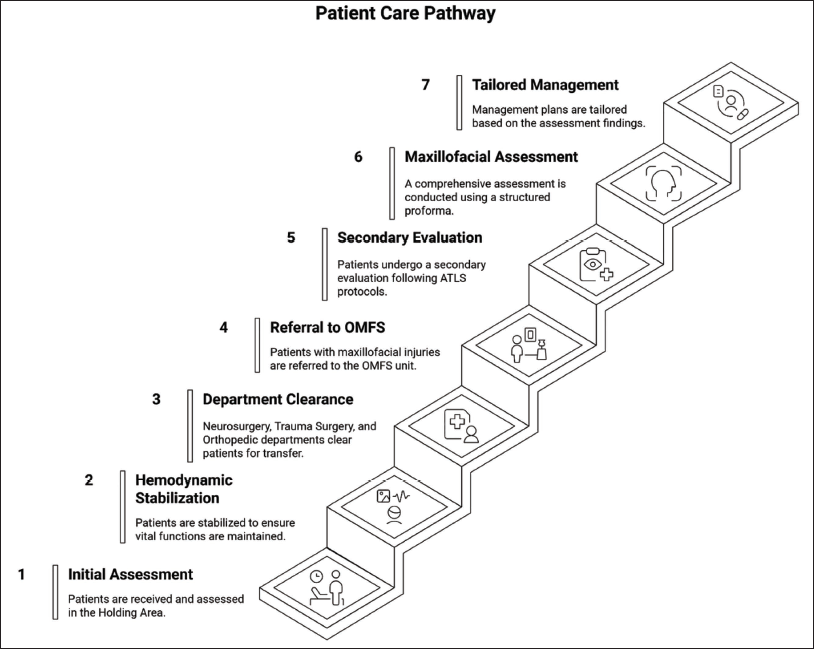
Patients presenting initially to the trauma center are first received in the holding area, where a preliminary assessment is conducted, and hemodynamic stabilization is achieved. Following clearance from the Neurosurgery, Trauma Surgery, and Orthopedic departments, individuals diagnosed with maxillofacial injuries are referred to the OMFS unit. Upon arrival, each patient undergoes a secondary evaluation in accordance with ATLS protocols, followed by a comprehensive maxillofacial assessment. This assessment includes the completion of a structured proforma, which has been adapted from an existing template to better suit departmental needs. Subsequent management is tailored based on the findings of this evaluation (Figure 10).
Figure Shows the Protocol Followed to Maintain a Forward Flow of the Patients with Maxillofacial Injuries.
Among the most critical cases successfully handled were those involving threatened airways complicated by active hemorrhage (Figure 11a), where rapid airway management and hemostasis were essential to prevent hypoxic injury or fatal outcomes. The department also managed complex and uncommon trauma scenarios such as bear maul injuries (Figure 11b), which often resulted in extensive soft tissue degloving (Figure 11c) and facial disfigurement. These cases posed significant reconstructive and infection control challenges, requiring immediate surgical intervention and staged repair strategies. Additionally, deep soft tissue injuries involving critical anatomical structures of the head and neck (Figure 11d) were addressed with precision, utilizing advanced surgical techniques to preserve function and esthetics while minimizing long-term morbidity.
(a) Maxillofacial Injury Threatening Airway. (b) Bear Maul Injury. (c) Degloving Injury. (d) Injury in the Throat Near Critical Anatomic Structures.

To guide the management of such high-stakes presentations, the unit implemented a case-based, algorithm-driven protocol that prioritized rapid assessment, stabilization, and the restoration of vital functions. This structured approach enabled timely decision-making in chaotic trauma settings and ensured that life-preserving measures were undertaken without delay. Each clinical pathway was tailored to the individual case while adhering to core principles of trauma care, including early resuscitation, airway protection, bleeding control, and infection prevention. The success of this protocol in managing both common and rare traumatic presentations underscores the department’s readiness and resilience in delivering high-acuity care in a multidisciplinary setting.
Hierarchical Management Approach
Conservative Management
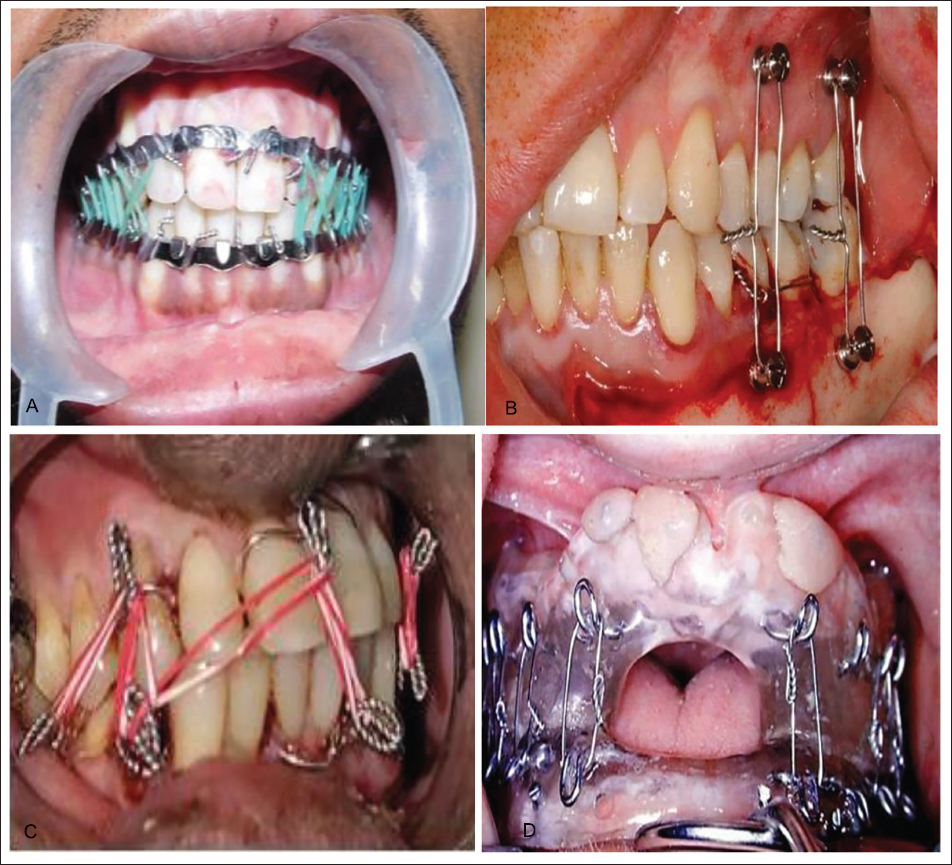
The department employs a comprehensive array of techniques and fixation devices to manage maxillofacial fractures, particularly those involving the mandible and maxilla, with an emphasis on stabilization, functional recovery, and minimally invasive approaches where appropriate. Conventional methods such as arch bars (Figure 12a) and intermaxillary fixation (IMF) screws (Figure 12b) remain foundational in the operative management of jaw fractures, offering reliable occlusal stabilization during the healing phase. Additionally, Ernst’s wiring techniques (Figure 12c) are utilized in specific cases to achieve secure and adaptable fixation, particularly in settings where dental support is limited or when rapid stabilization is required. Gunning splints (Figure 12d) continue to play a vital role in edentulous patients, allowing for effective immobilization of the maxillofacial skeleton while maintaining oral function and patient comfort.
(a) Intermaxillary Fixation (IMF) with Elastics. (b) IMF Screws. (c) Ernst Wiring Technique. (d) Gunning Splint for Edentulous Arches.
In keeping with the department’s commitment to innovation and context-specific solutions, the Solitary IMF Dental Cleat (SIDC)—a patented, indigenous device developed in-house—has been introduced as a novel alternative to traditional IMF methods (Figure 13). The SIDC represents a significant advancement in surgical convenience and patient safety, allowing for efficient application, reduced chairside time, and minimized mucosal trauma. Its use has been especially beneficial in cases where conventional IMF techniques are contraindicated or impractical due to anatomical limitations or comorbidities.
Clinical Pictures Showing the Use of Solitary IMF Dental Cleats (SIDC).

Minimally Invasive Techniques
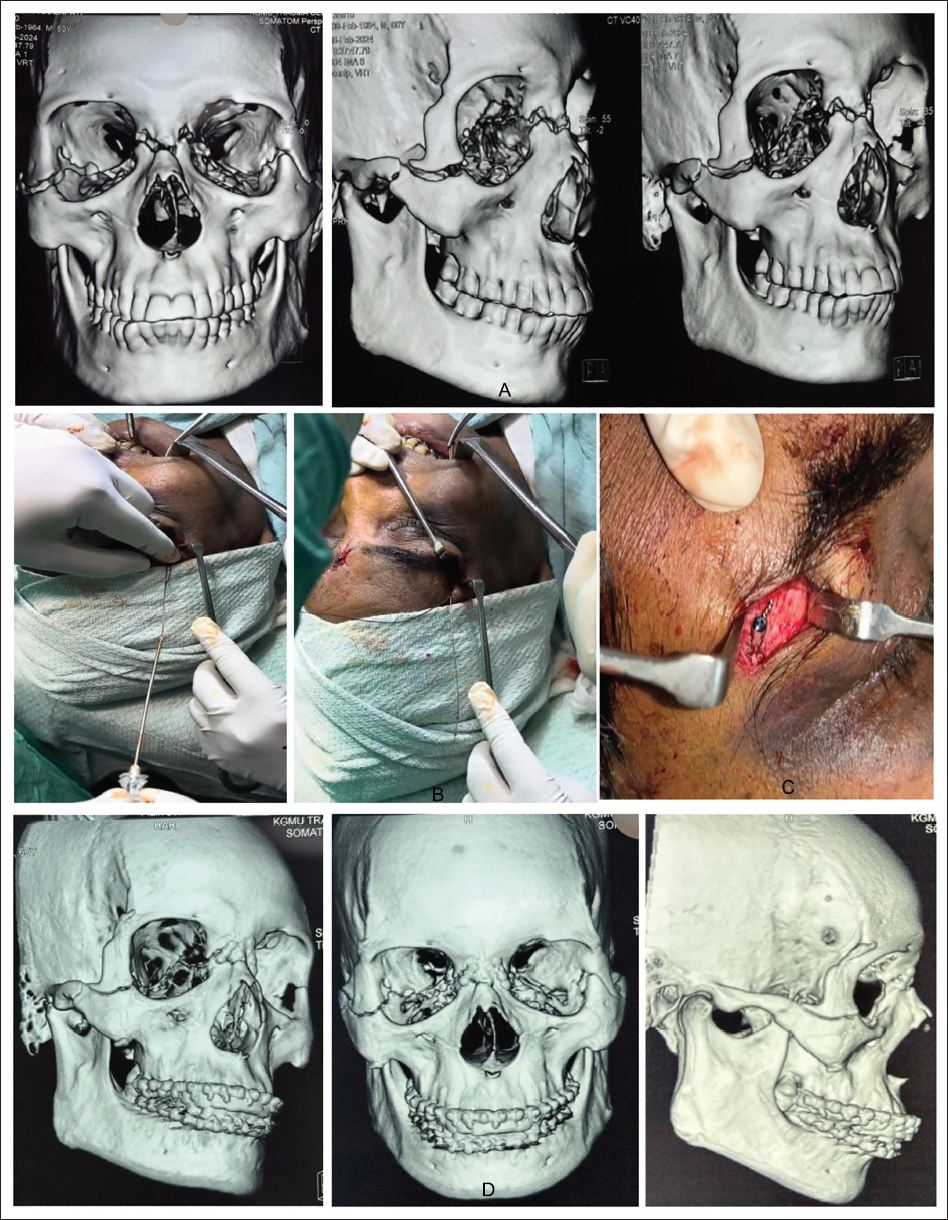
In the management of nasal fractures, suspension wiring in conjunction with open reduction and internal fixation (ORIF) has been effectively employed to provide stable anatomical alignment and facilitate optimal functional and esthetic outcomes. This technique allows for precise realignment of displaced nasal bones while minimizing soft tissue disruption, thereby promoting faster recovery and reducing postoperative complications. Furthermore, in selected complex or comminuted fracture cases, particularly those with vertical instability or midface involvement, suspension wiring techniques (Figure 14) have been employed to achieve additional support and alignment. These adjunctive measures enhance fracture stabilization in scenarios where plate fixation alone may be insufficient or where minimally invasive approaches are preferred. Overall, the department’s evolving fixation strategy reflects a balance between established practices and innovative solutions, guided by clinical judgment, patient-specific factors, and evolving surgical standards.
Suspension Wiring Technique. (a) Preoperative Computed Tomography (CT) Images. (b) Intra-operative Images. (c) Intra-operative Image Showing Screw Fixed for Anchoring Wire at Frontozygomatic Suture Region. (d) Postoperative CT Images.
For zygomaticomaxillary complex (ZMC) injuries, the department routinely utilizes Gillie’s temporal approach (Figure 15), a well-established and minimally invasive technique that permits direct elevation and repositioning of zygomatic fractures. This approach offers the advantages of reduced surgical morbidity, shorter operative times, and improved cosmetic results by avoiding visible facial scars.
Gillie’s Temporal Approach.

Integral to the surgical planning and evaluation process, comprehensive preoperative and postoperative imaging protocols are rigorously followed. High-resolution computed tomography (CT) scans and three-dimensional reconstructions provide detailed visualization of fracture patterns, aiding in precise surgical planning and implant placement. Postoperative imaging serves as a critical tool to confirm adequate reduction and fixation, ensuring the restoration of facial symmetry and function. The use of advanced imaging modalities throughout the treatment pathway underscores the department’s commitment to precision surgery and the achievement of superior esthetic and functional outcomes in maxillofacial trauma care.
Surgical Management
ORIF remains the cornerstone in the management of both mandibular and midface fractures, allowing for stable anatomical realignment and early restoration of occlusion and facial contour. The department routinely applies ORIF techniques tailored to fracture location and complexity, utilizing rigid fixation devices such as plates and screws to achieve optimal biomechanical stability (Figure 16).
(a) Open Reduction and Internal Fixation (ORIF) for Mandibular Angle Fracture. (b) ORIF for Zygomaticomaxillary Complex (ZMC) Fracture.
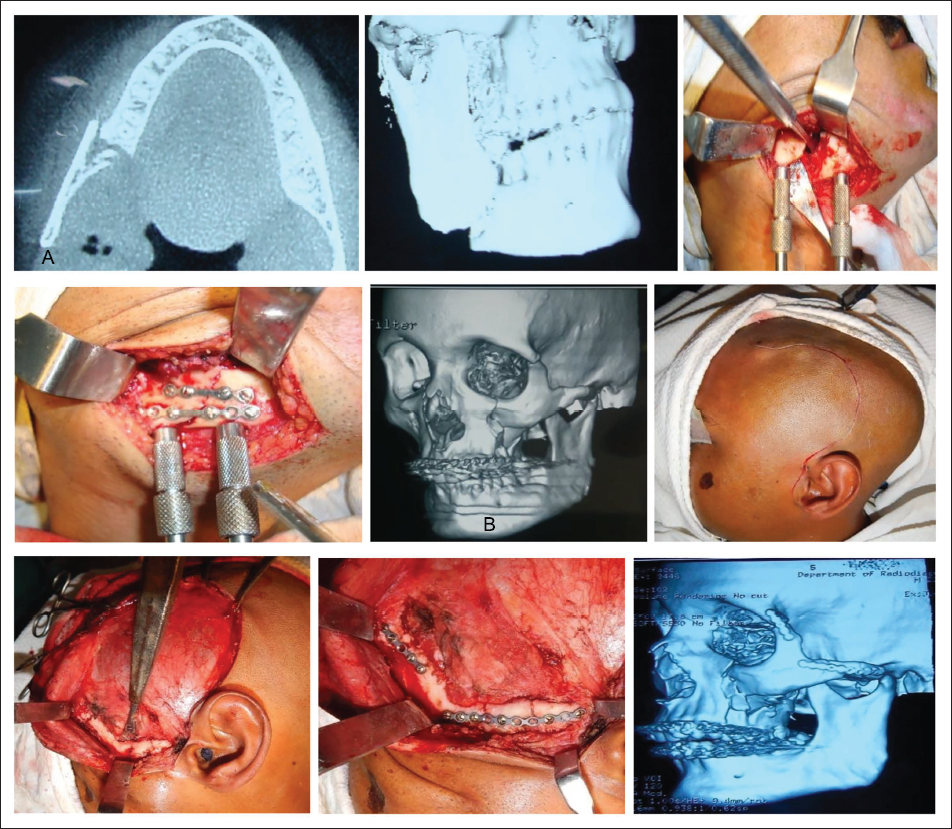
In particular, lag screw fixation has been effectively employed for subcondylar fractures of the mandible, offering the advantage of precise compression at the fracture site, which promotes faster healing and preserves temporomandibular joint function. This technique, when executed with careful attention to anatomical landmarks, minimizes postoperative complications such as malocclusion or joint dysfunction (Figure 17).
Images Showing Cases Where Lag Screw Fixation was Used to Manage Mandibular Condylar Fracture. (a) Pre-op Computed Tomography (CT) Images Showing Left Parasymphysis and Left Condylar Fractures. (b) Intra-op Images of Lag Screw Fixation Over Left Condylar Fracture. (c) Post-op CT Images. (d) Pre-op CT Images Showing Left Condylar Fracture. (e) Intra-op Image. (f) Post-op Orthopantomogram (OPG) Showing Lag Screw Fixation Over Left Condyle.
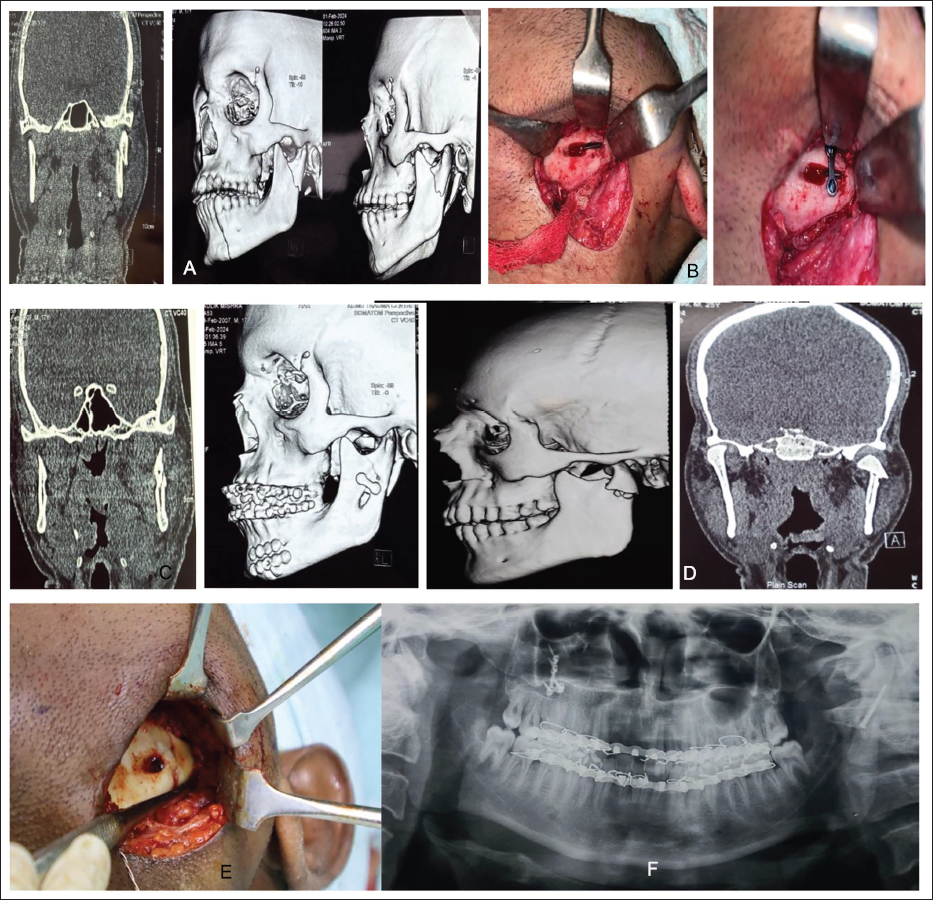
Management of panfacial trauma—a complex presentation involving multiple fracture sites across the upper, middle, and lower thirds of the face—requires meticulous surgical planning and execution. The department adopts a multi-point osteosynthesis approach (Figure 18a-18c) in these cases, strategically placing fixation points to restore the structural integrity and three-dimensional contour of the facial skeleton. This comprehensive method not only ensures mechanical stability but also supports the reestablishment of facial symmetry and esthetics. Postoperative monitoring of esthetic outcomes is an integral component of patient care, involving serial clinical assessments and imaging studies to evaluate bone healing, alignment, and soft tissue restoration. Through this multidisciplinary, protocol-driven approach, the department strives to optimize both functional rehabilitation and cosmetic results in patients suffering from severe maxillofacial trauma.
Images Showing Cases of Panfacial Fracture. (a) Pre-op Computed Tomography (CT) Images Showing Comminuted Zygomaticomaxillary Complex (ZMC), Naso-Orbito-Ethmoidal (NOE) Fractures Involving the Orbital Floor and Le Fort Fractures. (b) Intra-op Images Showing the Grafting of the Nasal Bridge Using Iliac Crest Bone Graft. (c) Post-op CT Images.
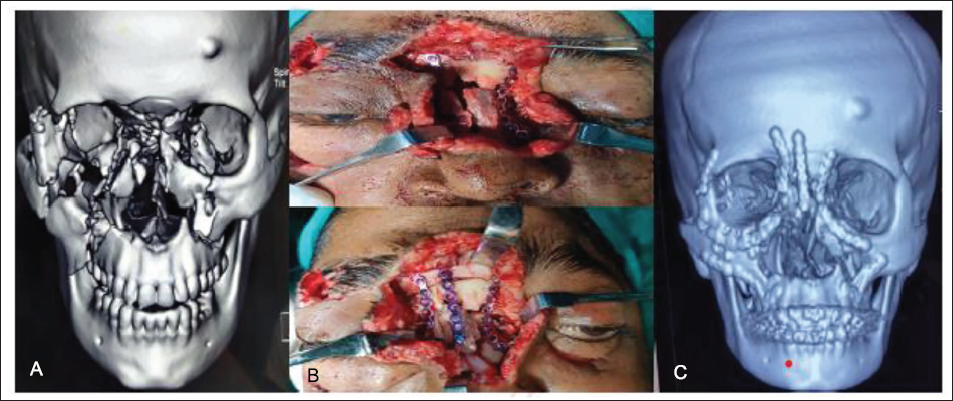
The department employs autologous bone grafting techniques for nasal reconstruction, particularly utilizing iliac crest grafts. These grafts provide robust structural support and are favored for their favorable contour and osteogenic potential, making them well-suited for the restoration of nasal framework defects following trauma or tumor resection (Figure 18).
Advanced Reconstruction and Innovation
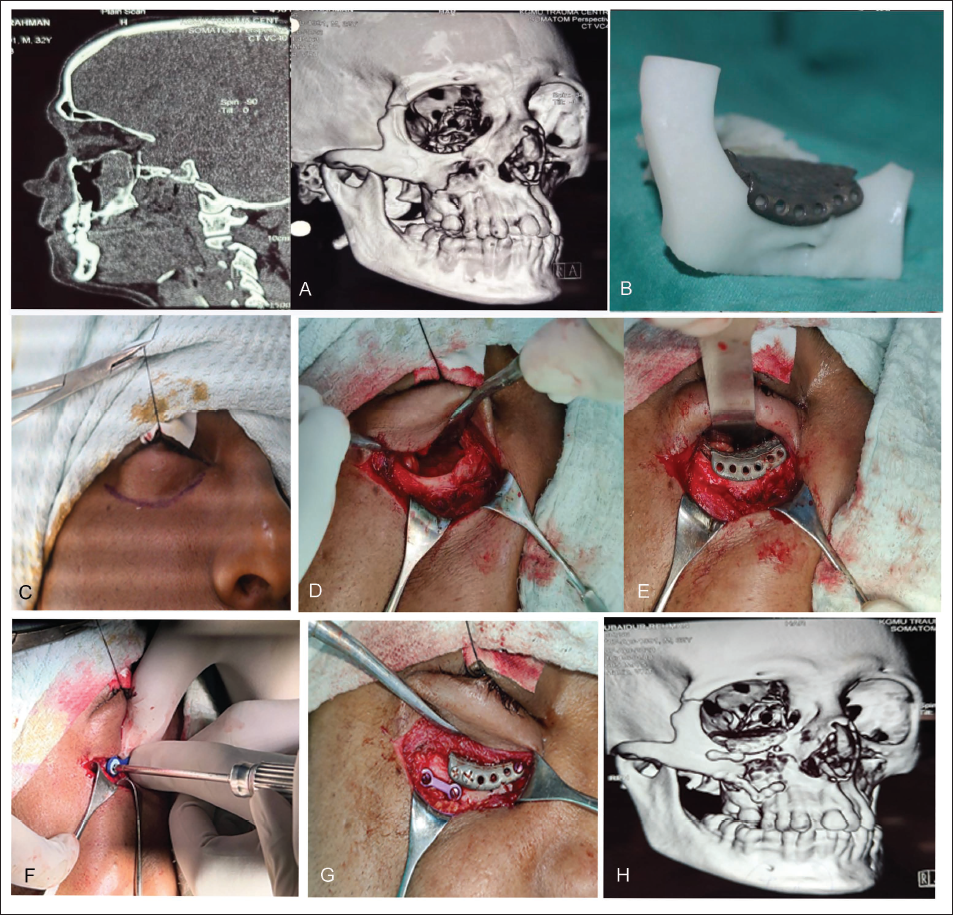
The department has integrated advanced reconstructive techniques to address complex maxillofacial defects, with a particular emphasis on orbital floor reconstruction. Patient-specific implants (PSIs) have been increasingly utilized to restore the intricate three-dimensional anatomy of the orbital floor with high precision (Figure 19). These customized implants, designed through preoperative imaging and computer-assisted modeling, enable an exact fit that closely replicates the native orbital contour, thereby improving both functional and esthetic outcomes. Complementing this approach, endoscopic-assisted reconstruction techniques (Figure 20) have been adopted to minimize surgical morbidity. The use of endoscopic visualization during orbital repair has been instrumental in reducing complications such as diplopia and ocular motility restrictions by allowing meticulous dissection and precise implant placement through less invasive corridors.
Images Showing Use of Patient-specific Implant (PSI) for Orbital Floor Reconstruction. (a) Preoperative Computed Tomography (CT). (b) Planned Implant. (c-g) Intra-operative Images Showing Orbital Defect, Placement, and Fixation of PSI. (h) Postoperative CT Image.
Images Showing Use of Endoscopic Approach for Orbital Floor Reconstruction. (a) 30-degree Endoscope Inserted. (b) Orbital Defect. (c) Harvesting of Nasal Cartilage. (d) Preoperative Patient Image Showing Hypoglobus and Enophthalmos of Right Eye. (e) Postoperative Correction of Hypoglobus and Enophthalmos.

The department has introduced a new concept of total maxillofacial trauma management (TMTM), which involves the combination of cutting-edge implant technology and surgical methods, reflecting the department’s commitment to comprehensive, individualized patient care that prioritizes both functional rehabilitation and facial esthetics (Figure 21). Following this concept, the department offers patients complete management for facial bone fractures, alongside the simultaneous placement of dental implants to rehabilitate any tooth loss. This integrated approach ensures that both the structural integrity of the face and the functional restoration of the teeth are addressed in a single comprehensive treatment plan, promoting faster recovery and improved overall outcomes.
Images Depicting the Concept of Total Maxillofacial Trauma Management (TMTM). (a-b) Preoperative Computed Tomography (CT) Showing Right Condyle and Left Parasymphysis Fracture of Mandible with Loss of Maxillary and Mandibular Anterior Teeth. (b-e) Intra-operative Images Showing Open Reduction and Internal Fixation (ORIF) for Mandibular Fractures with Simultaneous Placement of Dental Implants. (f-g) Postoperative Orthopantomograms (OPGs) Showing Implant Placement and Rehabilitation of the Lost Teeth.
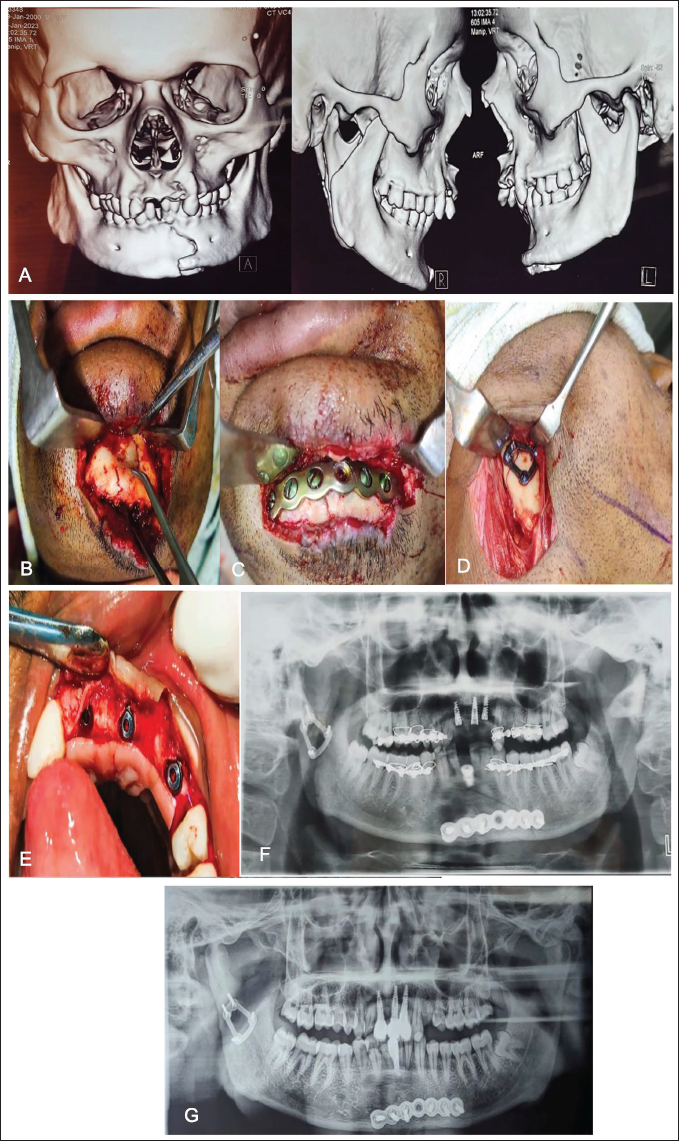
This concept is based on the rapid acceleratory phenomenon, which suggests that inflammation can actually accelerate the healing process. By leveraging this principle, we aim to stimulate the body’s natural healing mechanisms, enhancing recovery times and improving overall outcomes for patients with maxillofacial trauma.
Conclusion
Effective management of maxillofacial trauma is achieved through a tiered, multidisciplinary protocol that seamlessly integrates conservative measures, minimally invasive techniques, and surgical interventions tailored to individual patient needs. Grounded in a culture of innovation, digitalization, and rigorous research, the department’s model exemplifies a holistic approach to trauma care that optimizes clinical outcomes while advancing academic knowledge. By combining state-of-the-art technology with collaborative expertise across specialties, this framework not only enhances patient recovery and safety but also serves as a benchmark for trauma centers seeking to elevate both their clinical practice and scholarly contributions on a regional and national level.
Footnotes
Declaration of Conflict of Interests
The authors declared no conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Patient consent was taken in all the cases and none of image has any other source apart from them attained from the institutional setup.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.