
Abstract
Background:
The rising prevalence of kidney failure is a global concern. Individuals with kidney failure experience increased symptom burden, reduced quality of life, and increased healthcare utilisation. Kidney supportive care (KSC), a palliative-aligned approach that emphasises comfort, dignity, and holistic support for patients and families is offered as an alternative to dialysis treatments. Little research has explored how patients and caregivers experience and decide on conservative kidney management and KSC.
Objectives:
To explore the lived experiences of patients with kidney failure and their caregivers in treatment decision-making for conservative kidney management.
Design:
A qualitative inquiry using an interpretative phenomenological approach was conducted.
Methods:
Semi-structured interviews were conducted with patient-caregiver dyads to understand patient and caregiver lived experiences in choosing conservative kidney management. Patients who were aged 21 or older with Chronic Kidney Disease Stage G5 (eGFR ⩽15 ml/min) and had chosen KSC, were recruited along with their caregivers. Semi-structured, in-person interviews were conducted with nine patients and eight caregivers. Interviews were transcribed verbatim. Two researchers performed independent coding and identified meanings and themes which alluded to the lived experiences of individuals under KSC and their caregivers.
Results:
Four themes captured the lived experience and decision-making journey: (1) lived reality of kidney failure, (2) navigating treatment decision making, (3) the role of family and healthcare providers, and (4) facing the future and perceived needs in supportive care. Decisions were influenced by personal values, comorbidities, age, clinician recommendations, fear of suffering, and witnessing others on dialysis. Most decisions involved collaborative discussions between patients, families, and clinicians. Participants expressed the need for enhanced continuity of KSC and community-based early palliative care access.
Conclusion:
Decisions to pursue conservative kidney management are multidimensional, shaped by patients’ values, social contexts, and healthcare interactions. Understanding these factors ensures informed choices and better support during the decision-making and care transition process to KSC. Findings highlight need to improve patient-provider communication and community support within an early palliative care-integrated approach.
Keywords
Introduction
Globally, there is a rising incidence of individuals diagnosed with chronic kidney disease (CKD). 1 CKD is characterised by the progressive decline in kidney function, culminating in kidney failure. Often, symptoms of CKD only presents in later stages. 2 Individuals with CKD stage 5 experience increased physical and psychological symptom burden, resulting in increased healthcare utilisation and reduced quality of life. 3 Besides physical symptoms, accompanying psychopathology such as anxiety and depression are commonly experienced. 4 Recognising the significant challenges faced by individuals with kidney failure and their caregivers, kidney supportive care (KSC) was developed as a care model to address multiple needs regardless of treatment modality, throughout disease trajectory. Core components of KSC include shared decision making, symptom management, advanced care planning, spiritual care, care at the end-of-life, and bereavement care. 5
Conservative kidney management (CKM) is a part of KSC, which is recognised as essential, person-centred care for patients who choose not to undergo kidney replacement therapy (KRT). 5 The International Society of Nephrology workgroup defines CKM as ‘care for people with kidney failure that focuses predominantly on providing kidney supportive care to promote quality of life but does not include KRT’. 5 CKM prioritises slowing disease progression and managing symptoms through a combination of dietary control and medication, as long as patient values and preferences are respected.5,6
One key domain of CKM within KSC is shared decision making amongst healthcare providers, individuals with kidney failure and their loved ones. 7 Families play a significant role in treatment decision making, often directly being involved in the process through being a messenger and intermediary between healthcare team and patient. 8 Current gaps identified in delivering effective CKM include insufficient information on prognosis and support, healthcare provider misconceptions on CKM, and limited integration into existing healthcare infrastructure.9,10 As CKM evolves, it is crucial to understand how patients and their caregivers perceive the illness burden, the nuances involved in their decision-making process and challenges they face when choosing CKM.
Limited research has been conducted on the perceived illness burden, decision-making process, and supportive care needs of patients who opt for CKM and their caregivers.11,12 Therefore, this study aims to explore the lived experiences of both patients and caregivers in navigating their decision for CKM. Understanding their needs will provide insights into shaping ongoing and future kidney supportive and palliative care interventions to improve the quality of KSC for patients and their caregivers.
Methods
An interpretative phenomenological analysis approach was adopted to explore the lived experiences of patients who opted for CKM and their caregivers. Interpretative phenomenology is a participant-oriented qualitative approach which allows researchers to understand and narrate the treatment decision-making process and their lived experiences with CKM.13,14
Setting and participants
Participants were recruited from the renal conservative care (RCC) clinic at Sengkang General Hospital, following the decision to pursue KSC without dialysis. The RCC programme is encompasses active symptom management, advance care planning, and psychosocial support provision, which is aligned with the KSC framework proposed by Davison et al. 7 Care is delivered through a multidisciplinary team comprising physicians, nurses, and medical social workers, each contributing distinct expertise to the holistic management of patients and their caregivers. Within this model, physicians conduct outpatient consultations for patients who have opted for CKM, with assessments covering biochemical parameters, symptom burden, care-related concerns, and the coping capacity of both patients and their caregivers. Medical social workers address the psychosocial dimensions of illness, including emotional adjustment, caregiver burden, advance care planning discussions, and the coordination of community support services. Notably, this patient population may not meet the eligibility criteria for home or inpatient hospice services, as qualification typically requires a documented prognosis of less than 1 year. For this study, participants were eligible if they were: (1) aged 21 or older, (2) diagnosed with end-stage kidney disease (eGFR <15 ml/min), (3) had decided on CKM, (4) receiving follow-up care at the RCC clinic, and (5) conversant in English, Mandarin, or Malay. Caregivers were included if they were aged 21 or older and provided informal care to the patient. Individuals with cognitive impairment were excluded. Recruitment was conducted by a medical social worker or research coordinator following physician consultation. In instances where only one member of a patient-caregiver dyad consented to participate, while the other declined, data collection proceeded with the consenting individual.
Semi-structured in-person interviews were conducted in English and Chinese between April 2023 and March 2025, using an interview guide containing open-ended questions on decision making and supportive care needs (Supplemental Appendix A). Interviews were conducted by social workers (L.W.L., L.S.P.) and a research assistant (C.S.Y.). Interviews lasted from 10 to 45 min and were audio recorded with informed consent.
Data collection and analysis
Interview data were transcribed verbatim on Microsoft Word. Each transcript was assigned a code (e.g. P1 for patient, C1 for corresponding caregiver). Chinese interviews were translated and cross-checked by another research team member. Quotes from Mandarin interviews were translated into English by a bilingual research team member fluent in both the source language and English. To ensure accuracy and preserve meaning, member checking was conducted with participants to verify that translated quotes authentically reflected their intended meaning. Two researchers (L.S.P., A.T.J.Q.) independently conducted idiographic thematic analysis for each case (transcript), coding for descriptive and emotional meaning. L.S.P. is a medical social worker with a postgraduate degree in palliative care, while A.T.J.Q. is a qualitative-trained postdoctoral nurse researcher. The researchers independently coded five transcripts and had initial discussions to align coding decisions. Convergent and divergent findings were identified across cases. Group experiential statements were formed after comparison across cases to articulate and summarise the lived experiences of patients choosing CKM. A third researcher (L.W.L., medical social worker) was also involved in theme development discussions. In phenomenological analysis, we aimed to approach data saturation in terms of data adequacy – to obtain insights that were sufficiently in-depth and nuanced to highlight the decision making for CKM. 15 As such, recruitment and data analysis took place concurrently. When the research team judged that data adequacy was reached, recruitment was halted. An audit trail of coding and theme development was kept on Microsoft Excel.
Researcher reflexivity was maintained through bracketing, documenting memos, and discussions. Conscious bracketing was employed as a reflexive strategy, whereby each researcher made deliberate and ongoing efforts to identify, articulate, and set aside preconceptions arising from their respective clinical backgrounds during data analysis. This was operationalised through reflective journaling, in which assumptions and interpretive inclinations were documented throughout analysis. Potential biases which included the nurse researcher’s familiarity with patient illness trajectories and the medical social workers’ experiential knowledge of patient-caregiver dynamics were surfaced and critically examined during regular team-based discussions. These discussions served as a forum for reflexive dialogue, where interpretive decisions were made transparent, competing interpretations of the data were debated, and consensus was reached through return to the primary data. Analytic memos were maintained throughout to document the reasoning underpinning coding and theme development, further enhancing the auditability of the analytic process.
Results
We have approached 10 pairs of patient-caregiver dyads. Out of which, nine patients (90% acceptance rate) and eight caregivers (80% acceptance rate) were interviewed. Patients’ average age was 79.8 years old, while caregivers’ mean age was 61.4 years old. Most patients were married or widowed (n = 7), and were living with their spouse or children (n = 6). Caregivers were mostly married and lived with their spouse, or in a multigenerational household with their spouse, parents, and children (Table 1).
Participant demographics.

Four themes were identified (Table 2): (1) Lived reality of kidney failure, (2) navigating treatment decision making, (3) role of family and healthcare providers in decision making, and (4) facing the future-perceived needs in KSC.
Themes and subthemes.

Theme 1: Lived reality of kidney failure
Perceptions of own kidney function
Participants expressed awareness of their declining kidney function. They became cognizant of their physical health when their daily activities and physical function such as gait were severely affected – P10 was unable to ‘walk far because of breathlessness’. Some patients and caregivers only gained a clearer understanding of their kidney condition after being hospitalised.
It was last year that her kidney condition deteriorated. She was admitted and doctor told us that she may need dialysis. . . . (C11)
Other participants did not seem to be aware of when their kidney condition declined. P4 expressed uncertainty on his current kidney function: ‘Yeah, I got it at age 35. I got diabetes. I took only capsules. Now my doctor tells me to take an insulin injection . . . Diabetes or kidney, (I) don’t know’.
Impact of kidney failure on daily life
The symptom burden of declining kidney function significantly influenced patients’ physical functioning and activities of daily living. P6 noticed reduced appetite and lethargy. However, she was still able to ‘move around on (her) own, take bath, can dress up properly’. In comparison, P10 described frequent urination about ‘two to three times a night’, and became breathless if he had to walk far. P4 also mentioned that he suffered from severe pruritus which required specialist follow-up.
Caregivers were affected psychosocially. C3 described fear and anxiety in anticipation of physician consultations, fearing unfavourable news. As her father’s primary translator, she found it emotionally challenging to convey complex or distressing information sensitively: Every time when there’s a doctor’s appointment, I feel very down. I don’t know what I will hear from the doctor . . . Because for bad news, I may not share totally . . . you will be more careful, to filter these things. (C3)
Theme 2: Navigating treatment decision making
The cumulative burden of physical symptoms, functional decline, and emotional adjustment to progressive illness directly shaped how participants appraised their options and arrived at the decision to pursue CKM. Participants articulated the process of weighing risks and benefits of dialysis and opting for supportive care. Multiple aspects such as concerns over dialysis efficacy, practical losses involved, and patients’ values and preferences influenced treatment choice.
Viewing dialysis as a burdensome treatment choice
Patients and caregivers shared skepticism towards dialysis in controlling kidney disease progression, and associated it with accelerated functional decline and death. P1 witnessed ‘a few friends passing away shortly after starting on dialysis’ (translated from Mandarin). P6 viewed dialysis not as a cure, but solely to prolong life – ‘There is no guarantee how long it will last’.
Another key reason was the physical pain and side effects that they perceived dialysis may bring and expressed fear about it: (He) saw what my siblings went through . . . Very difficult after dialysis vomit, cannot sleep, cannot walk, going for holiday is also difficult. (P10)
Dialysis was viewed as financially impractical, due to the burden of treatment costs and lack of curative potential – ‘100% cure? Dialysis takes all the money, our money . . . must sell the house to pay for dialysis’ (P2).
Value and preference-driven decision making
More importantly, participants were not willing to undergo significant lifestyle changes due to the huge time commitment of dialysis and strict schedule. Being on dialysis seemed akin to losing their independence and freedom. In one dyad (P3 and C3), both the patient and his caregiver (daughter) independently expressed an acceptance of mortality and a preference for quality over quantity of life, reflecting a convergent values framework that appeared to underpin their alignment with the CKM trajectory. The patient articulated a pragmatic acceptance of death as a part of the natural life course, rooted in his sense of having lived a full life: ‘Old already will die . . . nothing to worry (P3, translated from Mandarin). This sentiment was closely echoed by his caregiver, whose stated goals centred not on extending survival but on preserving the patient’s dignity and minimising suffering: I don’t need him to prolong his life. I just want him to live happily and not suffer much. (C3)
C3’s account reflected a nuanced understanding of her father’s personality, particularly his strong preference for autonomy, as it meant being confined to living around the dialysis schedule – ‘He cannot be as free as now, he may not be able to go downstairs to buy something’. Participants P8 and P12 emphasised maintaining personal control over treatment decisions, grounded in their perception that they themselves would ultimately bear the physical consequences of these choices: They want me to go for this and that even . . . Why don’t you just proceed with this? I said no . . . I’m the one who’s gonna face all the pain. (P12)
Concerns of declining functional status and increased care needs also shaped patients’ decisions: To her it just affects her quality of life further . . . My mum loves to travel, (dialysis) will stop her from being independent and going out on her own. (C6)
Religious beliefs emerged as a significant meaning-making framework through which participants interpreted their illness, negotiated their mortality, and arrived at treatment decisions that felt congruent with their values. Rather than functioning as a passive source of comfort, religious conviction actively shaped the cognitive and emotional architecture of decision making for some participants. P6 believed her lifespan and physical body was a gift – Her conviction that the human lifespan is divinely ordained reframed her decision not as resignation, but grounded in profound gratitude for what she perceived as an already extended life: ‘Our age and lifespan is up to 63. Now I am 74. I am given a bonus already. I am thankful to God . . .’. She believed that the dialysis catheter was invasive, and preferred to ‘leave the world with the beautiful body that God created (her) in’. The influence of religious belief extended beyond the patient to shape caregiver experiences and their capacity to accept the illness trajectory. C5 expressed that religious influences in her mother’s life allowed her to be more accepting towards death: ‘She will pray to Jesus . . . it gives her some comfort that somebody is looking after her’. Across these accounts, religious beliefs functioned simultaneously as a personal framework for decision making, a source of emotional sustenance, and a relational resource that supported both patients and caregivers in navigating the uncertainties of advanced illness.
Theme 3: Role of family and healthcare providers in treatment decision making
Treatment decision-making processes were also influenced by family dynamics and interactions with healthcare providers. While most participants engaged in open communication and collaborative decision making with their clinical teams, the findings also revealed that family relationships introduced layers of complexity that extended beyond the initial treatment choice. Specifically, tensions within family units including disagreements between caregivers, the exclusion of patients from decision making by well-meaning relatives, and ambiguity around designated proxy decision makers generated uncertainty around anticipated downstream decisions, particularly those concerning resuscitation and end-of-life care. These findings highlight that the relational dimension of CKM decision making does not conclude with the choice to forgo dialysis, but may continue to evolve as the illness progresses and more immediate end-of-life decisions approach.
Collaborative decision making
Generally, patients and caregivers expressed that they were involved in collaborative decision making through open communication with the healthcare team. This allowed patients and caregivers to be fully aware of the risks and alternative treatment options to make an informed decision. For patients with larger families, efforts were made to discuss treatment options via family chatgroups or in-person. Treatment decisions were characterised by shared family-based deliberation, and they felt well supported by the healthcare team in terms of informational needs: We talk to the doctor then we kind of vote in our chat group . . . The doctors are good, they give us a lot of information and give us options . . . they give us the best advice considering her age. (C5)
C5 emphasised efforts to involve her mother in the decision-making process through relaying information from the physician, ultimately leaving the decision to patient – ‘We discuss among ourselves, we talk to her . . . let her understand, then she will be the final one to (decide) . . . If she says no, we say okay’.
Complexities in family involvement
Some caregivers were averse to being involved in the decision-making process as they expressed fear of making a ‘wrong decision’. To them, having to decide between dialysis and CKM seemed like a life and death decision that was too heavy a burden to bear: It is his body and he needs to decide . . . I can be blamed for it if I convince him to do dialysis and it is not good for him. (C12)
For caregivers who were proxy decision makers or main spokespersons, care decisions could be further complicated by challenging family dynamics. Although P6 and C6 have expressed support for the CKM trajectory, divergence was identified around the practicalities of advance care planning, the boundaries of decision-making authority, and the interpretation of the patient’s psychological state. C6 reflected on navigating unanswered questions about her mother’s resuscitation preferences and the prospect of having to make proxy decisions without clear guidance: I want her to make the decision, and not me and my brother when she is lying on there and make a decision for her. (C6)
At times, family may choose to exclude patients in the decision-making process with the intention of shielding them from potential distress. C7 described intentionally withholding information from her mother in efforts to alleviate worries about her health condition: She knows nothing, we do not want her to know . . . Even how weak her heart, how bad is the kidney she doesn’t know . . . Makes her more worried, more anxious. (C7)
Physician-directed treatment
Physicians were perceived to be highly directive in communicating treatment choices, whether it was to consider dialysis or CKM. When physicians communicated the need for dialysis, some patients expressed emotional distress and resistance due to conflict with their preferences and concerns of reduced quality of life. One patient’s direct observation of a relative who had undergone dialysis yet died within 2 months led him to question the value of the treatment in altering the illness trajectory, an experiential conviction that ultimately outweighed the physician’s clinical recommendation Doctor said I MUST do dialysis, but my relative did it and still passed away after two months. (P10)
Mistrust towards healthcare providers represented a further barrier to the acceptance of clinical recommendations. For one patient, scepticism was rooted in a past negative experience in which his own clinical judgement, or that of his family, had proven more effective than medical advice, intensifying his reluctance to follow recommendations for dialysis: ‘I don’t trust doctor ah. Doctor said, cut my leg. In three days, my daughter just put water on my leg and (it was cured)’ (P2).
In contrast, physician directiveness was not uniformly experienced as coercive or unwelcome. In cases where patients were deemed medically unfit for dialysis, a clear and unambiguous clinical recommendation appeared to simplify and validate the decision-making process for caregivers. One caregiver described the decision as straightforward, because the physician’s assessment aligned with and affirmed the family’s own observations of the patient’s deteriorating condition: ‘Not (a) difficult decision, because doctor already says (her condition is very bad) . . . we also agree with the doctor’ (C11).
Theme 4: Facing the future-perceived needs in CKM
Participants emphasised need for stronger care continuity in the community and improved communication after opting for CKM.
Care continuity in the community
Caregivers anticipated potential emergence of physical symptoms as kidney function declined over time and expressed a need for ongoing support even without active treatment. Home visits and check-ins were seen as assurance and stability: At least check in between their consultations, just make sure her lungs are not infected, and her well-being is still okay. (C5)
Some patients received community follow-up, and caregivers like C12 called for more emotional and moral support to reduce isolation. P6 valued daycare services for offering both encouragement and social interaction: I go to this therapy . . . (daycare staff) give me very encouraging talks . . . this gives me a chance to get out of my house at least once or twice a week. (P6)
Caregivers also described uncertainty around the illness trajectory and the transition to palliative care. They felt unprepared and lacked knowledge about available support: What if the kidney fails. Fully fails one day? We don’t know what to do and don’t know what to expect. (C10) I need to know about the conservative care . . . is there a period where it will stop and palliative care will take over? (C6)
Need for enhanced healthcare provider-patient communication
Patients and caregivers had mixed experiences in communicating with their healthcare providers. Some caregivers valued the healthcare team’s efforts to ensure patients’ preferences were communicated. Specifically, medical social workers actively facilitated end-of-life discussions and preferences with patients, a conversation that caregivers found difficult to hold given the emotional weight of such interactions. This was reflected in the account of caregiver C3, who expressed appreciation for the structured professional support in navigating these discussions: I appreciate all these social workers trying to find out. Your last breath, (it’s not) easy for me to ask as family. (C3)
While patients generally acknowledged a degree of accessibility to their renal physicians through the RCC clinic, as illustrated by one patient who noted that he could request an appointment whenever concerns arose (P3), this access did not uniformly translate into satisfactory communication experiences. A contrasting account from another patient highlighted significant gaps in the quality of clinical communication, particularly with respect to empathic engagement and the clarity of information provided regarding treatment options. This patient recounted feeling dismissed and poorly informed during a consultation, expressing confusion over the repeated emphasis on dialysis in the absence of a clear rationale: The last time I saw (the doctor), he keeps telling me that I am in a very bad stage. Is dialysis the only cure? But it is not a cure right? Why do you insist that I must? And he refused to look and talk to me . . . . (P6)
This account is particularly salient in the context of CKM, where patients have made an informed decision to forgo dialysis. The disconnect between the patient’s expressed preferences and the physician’s communication approach underscores the need for patient-centred dialogue that affirms and respects the chosen treatment trajectory, rather than revisiting or implicitly undermining it.
Discussion
From our study, we identified that treatment decision making was mostly driven by individual values and preferences, with influence of family and healthcare providers. While existing literature has documented patient and caregiver perspectives on CKM, our findings extend this body of work by foregrounding the deeply sociocultural and biographical nature of treatment decision making in this population. Consistent with Lightfoot et al. (2025), 32 participants in our study valued clear information and honest communication from clinicians in arriving at their decisions. However, our findings reveal that clinical information alone was rarely the primary or singular driver of the decision to pursue CKM. Rather, treatment decisions were shaped by a constellation of factors including religious belief, culturally situated understandings of death and suffering, witnessed illness experiences of significant others, and a biographical sense of having fulfilled one’s life roles and responsibilities. This aligns with the broader serious illness literature, which recognises that medical decision making is an inherently values-laden process embedded within personal, relational, and cultural contexts. We apply the person-in-environment framework (Figure 1) to discuss our findings in relation to patient’s experience with kidney failure and decision-making process for CKM. The person-in environment framework consists of three levels (micro, mezzo, and macro), and considers how individuals decisions are embedded in their biological, social, and systemic contexts. 16
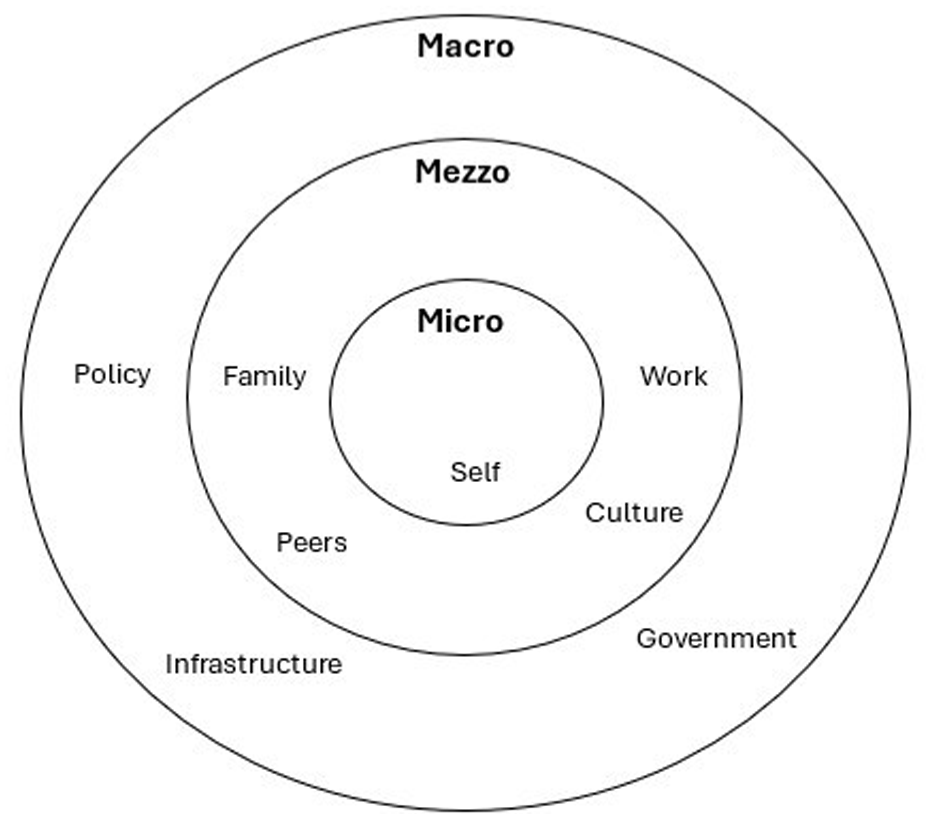
Person-in-environment framework.
At the micro level, patients’ awareness of their kidney condition was intertwined with the symptom burden that they were experiencing. For some individuals, quality of life was prioritised over a life-sustaining treatment modality, despite experiencing the symptom burden of CKD. Treatment decisions were influenced by a desire to maintain their current lifestyle, religious beliefs, and perception that dialysis had limited benefit. Similar to previous studies, dialysis was commonly associated with negative outcomes such as loss of independence, driving patients to choose CKM.17,18 Additionally, poor understanding of dialysis as a treatment modality, especially in older adults,19,20 are a barrier to informed decision making. As symptoms often surface late in the illness trajectory, individuals may not have a good understanding of CKD progression. It is crucial to introduce pre-emptive and timely education to enhance understanding of illness. As treatment options may not offer survival benefits or improved quality of life, serious illness conversations should be initiated with individuals and their families in both pre-dialysis treatment decision making, and revisited throughout treatment to ensure that treatment decisions are aligned with individual values and preferences.21 –23
At the mezzo level, decision making is reinforced through the patient’s social network. This is salient in the Asian context, where the relational autonomy, collectivism, and family-centred decision making remain the cultural norms, 24 which in turn influences the extent to which individuals with kidney failure are involved in their own treatment decision making. For example, some elderly patients may choose to leave the decision to their children or physicians. In our study, most decisions were collaborative, with patients and caregivers demonstrating alignment in the decision to pursue CKM. Patients typically led the decision process, and their choices were respected and supported by family members. Some caregivers expressed relief at not bearing sole responsibility for treatment decisions. While other studies report that caregivers advocated for dialysis although finances and caregiving duties were a concern, 18 this was not reflected in our findings.
Nephrologist input was also a key factor in guiding patients’ decisions. However, clinical influence may unintentionally overshadow patient autonomy. Communication styles vary in treatment decision-making conversations amongst clinicians (both physicians and nurses), and are influenced by their perception towards dialysis and understanding of patient condition, sometimes resulting in patients being steered towards dialysis. 25 Nephrologists have expressed in past studies that it was challenging to balance patient’s autonomy with what they perceived as clinical best interest.25,26 These relational influences can support patient’s confidence or introduce stress and ambivalence if conflicting views exist. Conversations are also influenced by the manner in which clinicians communicate treatment options. Recent studies on renal treatment decision-making conversations amongst clinicians and patients reported that risks of dialysis were minimised and CKM options are posed or framed to individuals as a subordinate option. 27 Such communication patterns may inadvertently compromise patient autonomy and undermine the integrity of informed consent, particularly for individuals who may be open to or already inclined towards conservative management. Addressing this requires investment in structured communication training and the adoption of evidence-based conversational frameworks. The use of structured shared decision-making conversations, such as the three-talk model (choice talk, option talk, decision talk), offers a clinically validated approach to facilitating these conversations. Choice talk involves establishment of partnership between physicians and patients, informing that a decision is needed. Option talk involves the sharing of options and their pros and cons, while decision talk focuses on what is important to patients and caregivers, drawing references to their values and priorities in guiding decisions. 29 When used in conjunction with patient’s decision aids including information on both dialysis and CKM, this model has been shown to foster therapeutic collaboration and improve satisfaction with treatment decisions.28 –31
At the macro level, broader factors such as the availability of formal KSC services, healthcare financing and infrastructure significantly influence one’s decision for CKM. While resource limitations are evident in low- to-middle income countries, where kidney replacement therapy may be limited or less accessible, 28 attention to individual contexts and social inequities remain important. In Singapore, where financial assistance schemes and dialysis facilities are broadly accessible, social determinants of health – including socioeconomic status, health literacy, family support structures, and cultural beliefs, nonetheless play a meaningful role in shaping treatment preferences and should be systematically addressed in clinical planning. Participants’ accounts of the anticipated financial burden of kidney replacement therapy further highlight how economic considerations are not merely logistical, but integral to the lived experience of decision making. These findings point to the need for clinical encounters to move beyond information provision, towards more explicit engagement with patients’ social contexts and perceived financial concerns in order to facilitate informed and person-centred decision making.
Both patients and caregivers highlighted the importance of continued care beyond the hospital setting as a critical component of KSC. Access to community healthcare services plays a vital role in fostering confidence and reassurance for patients who have opted for CKM. Additionally, integrating upstream palliative care within KSC using an interdisciplinary, person-centred care approach can facilitate better management of emotional symptoms and practical issues among patients with advanced diseases. 29 Davison et al. recommends seven core components of comprehensive CKM: interventions to delay kidney disease progression, shared decision making, active symptom management, advanced care planning, psychological support, social and family support, and spiritual and cultural care. 7 Integrated nephrology and palliative care programs, delivered by an interdisciplinary team and encompassing core components of comprehensive CKM, have been well-received by patients and caregivers for their proactive and patient-centred approach, 3 and has been shown to reduce healthcare utilisation. 30
Implication on practice and research
Our study findings have significant implications for practice and research in KSC. While we acknowledge that decision making regarding CKM has been explored in prior research,31,32 this study is among the first to examine patient and caregiver perspectives on CKM and the factors influencing such decisions in an Asian context. Our findings affirm that treatment decisions are not determined by clinical indicators alone, but are shaped by a confluence of personal values, sociocultural influences, relational dynamics, and available resources. Clinical conversations around CKM should therefore extend beyond disease progression and treatment modality to encompass individual values and priorities, psychosocial needs, and practical circumstances of both patients and caregivers.
These findings point to three key practice implications. First, there is a pressing need for structured clinician communication training and the adoption of evidence-based conversational frameworks and decision aids that support balanced, values-aligned discussions around dialysis and CKM. Embedding serious illness conversations at appropriate clinical junctures can facilitate earlier and more informed decision making that is congruent with patient and caregiver values. 21 Second, given that optimal models of KSC remain to be established,33,34 future programme development should prioritise integrated symptom management, proactive psychosocial support, anticipatory planning for disease progression, and capacity-building for community-based care. Third, core components of CKM must be embedded within community health and social services with clear referral pathways, not solely confined to outpatient clinic settings. Seamless hospital-to-community transitions are essential to sustaining continuity of care across the illness trajectory. Future research should examine KSC programme designs that incorporate structured care pathways integrating hospital, community, and palliative care services to optimise outcomes for patients and caregivers navigating this complex illness experience.
Limitations
We acknowledge the following study limitations. First, although patient-caregiver dyads were recruited, the present analysis did not systematically examine the relational dynamics between dyad members. Opportunities to explore areas of agreement, discordance, and proxy decision-making roles, all of which carry significant clinical relevance in the context of CKM were not fully realised. Future research employing dyadic analysis frameworks would be well positioned to examine how patients and caregivers negotiate treatment preferences, the extent to which caregiver perspectives influence or diverge from patient wishes, and the conditions under which proxy decision-making occurs. Second, patients recruited were mostly independent in their activities of daily living, and caregivers were not involved in providing direct physical care. Thus, we were unable to explore experiences of individuals with advanced symptoms or caregivers who are physically caring for these patients. Third, participant age range was restricted. Majority of the patients were above 75 years old, thus the findings may not fully capture perspectives of a younger sample. Lastly, one-time interviews were conducted, thus changes in decision making over time were not studied.
Conclusion
As KSC continues to advance, more attention is required to integrate supportive models of care with structured pathways to essential healthcare services into the community for patients who have chosen CKM. Within the KSC model, access to informational support and clear communication between healthcare providers, patients, and caregivers is also warranted to inform decision making, particularly during critical care transitions approaching the end of life. Future longitudinal studies to investigate decision making throughout the patient’s trajectory will be useful in informing factors driving changes in treatment decision making alongside disease progression.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524261444755 – Supplemental material for Lived experiences and decision making among patients and caregivers choosing conservative kidney management: A qualitative study
Supplemental material, sj-docx-1-pcr-10.1177_26323524261444755 for Lived experiences and decision making among patients and caregivers choosing conservative kidney management: A qualitative study by Sing Ping Loh, Apphia Jia Qi Tan, Wan Ling Lau, Seow Yean Chiang, Lee Ying Yeoh, Swee Ping Teh and Priscilla Wen Yi Long in Palliative Care and Social Practice
Footnotes
Acknowledgements
The authors would like to thank the patients and caregivers for their valuable input and time to participate in this study. We would like to thank SingHealth Group Allied Health for supporting the publicaton fees.
Ethical considerations
Ethics approval was obtained from IRB board (2022/2692).
Consent to participate
Written informed consent was obtained from participants before commencement of data collection.
Author contributions
Funding
The authors received no financial support for this research. The publication fee was supported by SingHealth Group Allied Health.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data generated or analysed during this study are included in this published article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.