
Abstract
Background:
Raising public awareness of palliative care has been identified as a priority within research literature on public health approaches to palliative care and within policy documents from many countries, including Canada. However, there is a lack of clarity about what this entails.
Objective:
To develop conceptual clarity and move from the broad goal of “raising public awareness” of palliative care to more clearly defined outcomes and priorities.
Design:
Group concept mapping is a participatory mixed methods approach that combines qualitative and quantitative analysis. Trochim’s six phases of concept mapping methodology were followed.
Methods:
Convenience sampling was used to invite participation. Participants were asked to brainstorm as many ideas as they wanted in response to the prompt: “Good public awareness of palliative care means . . ..” A master list of these ideas was then shared with participants and they were asked to: (1) sort the responses into groups and (2) rate each response on a Likert scale of 1–5 in terms of importance. Statistical analyses were conducted to compile the data into a point map and a range of cluster maps. Participants selected the best-fitting cluster map.
Results:
Nineteen people participated in the group concept mapping exercise. Eighty-four unique statements were generated in response to the prompt, and participants selected a seven-cluster map as best fitting the data. The seven clusters represent components of good palliative care public awareness and were assigned the following labels: (1) understanding palliative care; (2) knowing how to access palliative care; (3) planning ahead; (4) community support for palliative care; (5) caregivers are supported; (6) comfort talking about death and dying; and (7) palliative care is normalized.
Conclusion:
As a participatory mixed method, group concept mapping offers a novel approach to providing clarity and supporting action planning. It has been instrumental in refining activities to improve public awareness of palliative care in Alberta, Canada, and may be useful to others undertaking similar initiatives. Addressing these domains is a promising means of improving public awareness, understanding, and ultimately uptake of palliative care.
Plain language summary
Why this study was needed: Experts say it is important for people to know more about palliative care – the type of care that relieves the symptoms and stress of living with a serious illness. But what raising awareness of palliative care really means is not clear. What we wanted to do: We did this study to describe in more detail what good public awareness of palliative care actually means. What we did: We asked a group of people to help us by sharing their ideas about what good public awareness of palliative care means. We did this using a method called group concept mapping. -First, the people in our study gave us lots of ideas in response to the question: Good public awareness of palliative care means. . . -Then, they helped sort the ideas into groups and rated how important each one was. -We used this information to create maps (pictures) showing how the ideas were grouped. -The people in our study then chose the version of the map they felt was the best fit. What we found: -Nineteen people took part. -They came up with 84 different ideas. -One map with seven themes (groups of ideas) was chosen. These themes show what the people in our study believe makes up good public awareness of palliative care: 1. People understand what palliative care is; 2. People know how to get palliative care; 3. People plan ahead for future health needs; 4. Communities support people who need palliative care; 5. Caregivers (like family and friends) are supported; 6. People are comfortable talking about death and dying; 7. People see palliative care as a normal part of healthcare. Why it matters: This study helped create a clearer picture of what good public awareness of palliative care actually means. We used the results to help plan our palliative care public awareness project in Alberta, Canada. This study could be useful for people working in other places too. Focusing on these seven themes may help people better understand and get palliative care.
Introduction
Palliative care is effective at reducing suffering and improving quality of life for people with serious illnesses and those close to them. A growing body of research suggests that patient outcomes improve when palliative care is provided early in the disease trajectory.1–3 In 2014, the World Health Organization called palliative care “fundamental to improving quality of life, well-being, comfort and human dignity.” 4 However, many who could benefit from it do not have access to it, and there is also evidence that inaccurate public perceptions of palliative care mean it is under-utilized even when available. 5
Recommendations to improve access to palliative care involve changes in policy, health systems, and clinical education. Improving public awareness of palliative care is also identified within the research literature as a necessary component of improving access to, and uptake of, palliative care.6–12 Recent policy documents from many countries, including Canada, call for public awareness campaigns and education about palliative care.13–16 However, there is a lack of clarity about what it means to raise awareness of palliative care, or what good public awareness entails.17,18
The Covenant Health Palliative Institute, Alberta, Canada, has a mandate to increase palliative care capacity and advocate for a robust national palliative and end-of-life care system. In late 2020, the Institute received funding from the Government of Alberta to increase public awareness of palliative care in the province of Alberta (total population ~5 million) through the Palliative Care Public Awareness Project. The project ran from August 1, 2020 to September 30, 2025 and incorporated a public health palliative care approach, partnering with community-based organizations from diverse sectors to help with awareness-raising activities. A public health approach to palliative and end-of-life care asserts that death, dying, loss, and care is everyone’s responsibility 19 and brings health promotion ideas to palliative care, encouraging the public at large to adopt practices to improve quality of life and end-of-life care outcomes. 20 The public health palliative care approach recognizes the community as an equal partner in caring for people living with serious illness and through end of life.19,21 Community-based organizations are uniquely positioned to connect with people where they live and complement health services in caring for people facing serious illness and therefore are key partners in awareness-raising initiatives.
Public awareness of palliative care has been defined using a variety of constructs ranging from term recognition 22 to self-described level of knowledge22,23 to actual knowledge of the World Health Organization definition of palliative care. 24 In light of this, we determined it was important at the outset of the project to develop conceptual clarity around what “good public awareness of palliative care” actually entails. Herein, we describe use of group concept mapping methodology to move from the broad objective of “raising public awareness of palliative care” to clearly defined outcomes and priorities to support action planning.
Methods
Design
Group concept mapping is a mixed methods approach in which participants generate ideas about a topic of interest and then structure these ideas through sorting and rating, resulting in a series of maps that visually depict the composite thinking of the participants. 25 This mapping technique is designed to help researchers and organizations define issues, undertake action planning, and guide program development and evaluation. 26 Group concept mapping has been used as a community participatory approach in research,27–29 where participants are included in the generation of ideas, analysis of the data, and interpretation of the findings. The method is well suited to the field of public health palliative care as it can allow patients, caregivers, and community members to act as partners in research rather than passive recipients of care. However, given that research has highlighted that “public health education is needed to increase knowledge about palliative care, promote its early integration and counter false assumptions,” 24 we chose not to engage the general public in defining good public awareness of palliative care. Instead, we engaged patients, caregivers, and the public at a later stage of our public awareness initiative in producing educational resources to address identified gaps in knowledge.
The six phases of group concept mapping as outlined by William Trochim 25 (Table 1) were followed.
Six phases in group concept mapping. 25

The project team that led this work consisted of two employees, M.S. and A.O., and one contracted expert (L.D.). We used Concept Systems Incorporated GroupWisdom™ software (Ithaca, NY, USA) to collect, sort, and analyze data. All participatory steps were completed in May–June 2021.
Recruitment, sampling, and tools
Prepare project (Phase 1)
Participants: A convenience sample of 27 individuals affiliated with the Palliative Institute were identified for inclusion in the concept mapping activity, anticipating that the actual number of participants would fall within the range of 10–20 recommended by Trochim. 25 To be included, we required participants to be employed by, or affiliated with, the Palliative Institute. We targeted these participants because they possessed a baseline familiarity with palliative care as well as a shared appreciation of the importance of developing good public awareness of it. We chose to exclude patients, caregivers, and other members of the public to reduce the risk of responses being shaped by widespread public misconceptions about palliative care. 24
Notably, a group concept mapping approach does not require a random sample of participants as the goal is “to achieve a broad sampling of ideas rather than a representative sampling of persons.” 30 While participants can be involved in all phases, primarily they are involved in generating and structuring ideas. In this project, we also involved participants in selecting the concept map that best represented the generated data.
Focus prompt: The following focus prompt was developed to elicit ideas relevant to the project aim: “Good public awareness of palliative care means . . ..” This prompt was chosen from a list of potential prompts brainstormed by the project team because of its alignment with our goal of articulating the desired outcomes for our public awareness project and facilitating project planning. We used a structured prompt to encourage participants to complete the sentence in a grammatically uniform way. 30
Data collection
Generate ideas (Phase 2)
Email invitations were sent to potential participants (by M.S.) with a link to the GroupWisdom software. We advised participants that this activity was voluntary, that they could participate in any or all phases, and that their individual responses would be kept confidential. Consent was implied by participation in the online exercise(s). Participants were asked to respond to the prompt by adding as many ideas as they liked and they could exit the site and continue later using a unique login. Individual responses were anonymous, but participants could see the list of ideas submitted by other participants. At this stage, we included a brief, three-question survey to gather data on participants’ professional backgrounds and personal experience with palliative care (Supplemental File). The idea generation phase was open to participants for 2 weeks.
Structure ideas (Phase 3)
In preparation for the “Structure ideas” phase (i.e., sorting and rating the statements), M.S. and A.O. synthesized the list of ideas to create a list of unique statements. Specifically, we removed duplicate ideas, split compound statements, edited some statements for clarity, and added statements from a review of the literature. We then invited participants to use the online software to structure the list of statements by sorting them into groups according to their own logic, and to rate the importance of each statement using a 1–5 rating scale, with 5 being the most important (Supplemental File). This phase was also open for 2 weeks. There were no missing data during the sorting and rating phase.
Represent ideas (Phase 4)
We used GroupWisdom software to analyze the structured data using multi-dimensional scaling and hierarchical cluster analysis. First, each statement was assigned a reference number, following which we used multi-dimensional scaling to create a two-dimensional data point map. Each point on the map represents one statement, labeled with that statement’s reference number. The distance between any two points on the map indicates how frequently those two statements were sorted together (i.e., the closer two points are together, the more frequently participants sorted those statements together). We measured the fit between the data point map and the sorted data using Kruskal’s stress value.31,32 This value varies between 0 and 1, where lower values indicate less stress (i.e., better conceptual fit).
We also calculated bridging values (0–1) for each statement on the data point map. Low bridging values (near zero) indicate statements that are often sorted with nearby statements, referred to as anchors. High bridging values (near one) indicate statements that are sorted with other statements far apart on the map. Referred to as bridges, these statements may reflect connections across concepts. 30
After creating the data point map, we applied hierarchical cluster analysis to see which data points were clustered together. We created a series of cluster maps, where clusters appear as shapes overlaying the data points, for group interpretation. Suggested cluster labels derived from the labels assigned by participants were generated by the GroupWisdom software.
Interpret maps (Phase 5)
A collaborative approach was used to interpret the maps and choose the best-fitting cluster model based on bridging values and subjective interpretation. 33 Participants met virtually to discuss a shortlist of promising cluster models and selected the best-fitting model via consensus. Finally, participants discussed labels for each of the clusters within the chosen model. Final labels were assigned by the project team.
Utilize maps (Phase 6)
The resulting concept map was used to conceptualize components of good public awareness of palliative care and to establish priority areas for project activities. Priority areas were identified by evaluating the concept map in relation to the project mandate, as well as by considering the programs and resources already available in Alberta and the resource gaps highlighted by community partners.
Statistical analysis
Fit between the data point map and the sorted data was determined using Kruskal’s stress value.31,32 This value varies between 0 and 1, where lower values indicate less stress (i.e., better conceptual fit). Bridging values (0–1) were also calculated for each statement on the data point map. Low bridging values (near zero) indicate statements that are often sorted with nearby statements, referred to as anchors. High bridging values (near one) indicate statements that are sorted with other statements far apart on the map. Referred to as bridges, these statements may reflect connections across concepts. 30 Hierarchical cluster analysis was then applied to see which data points were clustered together.
Results
Participants
Nineteen people participated in generating ideas and sorting the statements, and 18 people participated in rating the statements. The participants had diverse professional backgrounds: they included clinicians, researchers, administrators, and support staff, with academic backgrounds in health, sciences, and the social sciences/humanities (Table 2). Participants also had varying levels of expertise, from project staff with limited background in palliative care to clinical and research experts in the field. Forty-two percent of participants had < 2 years of professional experience in palliative care; 11% had between 2 and 10 years of experience in palliative care; and close to half (47%) had more than 10 years of experience. Most participants (74%) indicated that someone important to them had received palliative care within the past 10 years.
Participant demographics (n = 19).

Idea generation and synthesis
Participants generated 109 raw statements in response to the focus prompt, “Good public awareness of palliative care means . . ..” After removing duplicate ideas, splitting compound statements, editing some statements for clarity and including seven additional statements from the literature, the synthesized list included 84 unique statements (see Appendix), well within the recommended maximum of 100 statements for sorting and rating. 30
Data point map
The data point map generated through multi-dimensional scaling had a Kruskal’s stress value of 0.295, indicating good fit between the structured data and the data point map. 30 Generally, stress values between 0.05 and 0.35 are acceptable in group concept mapping. 34 This value is also consistent with a sample of 69 concept mapping studies, where the average stress value was 0.28 (SD = 0.04; range = 0.17–0.34). 35 Figure 1 shows the data point map, with each point representing one of the 84 statements generated.
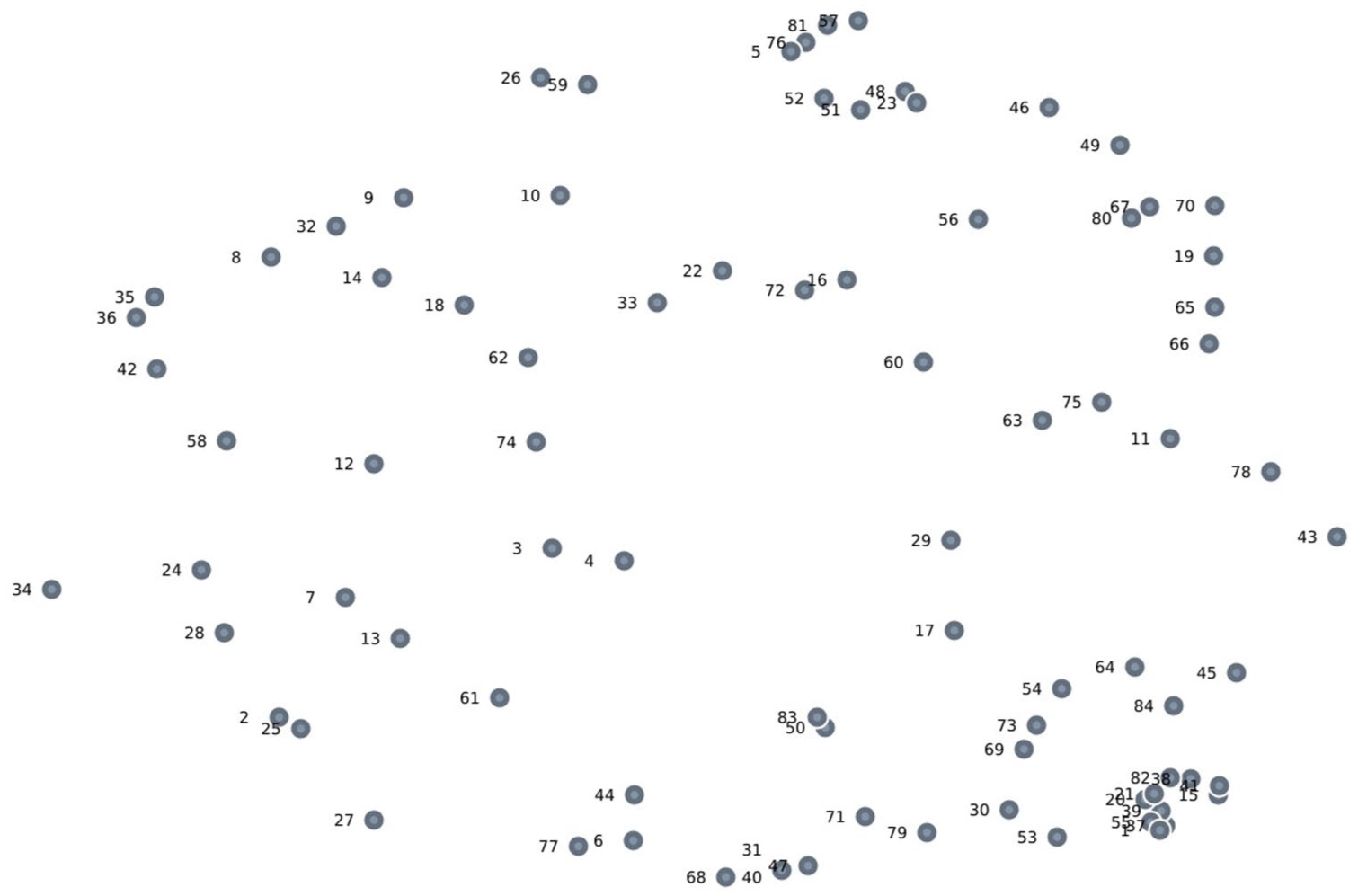
Data point map.
Concept map
The project team and participants met virtually to validate and discuss five cluster map options, ranging from four to eight clusters, resulting from hierarchical cluster analysis. Through consensus, the project team and participants selected a seven-cluster model as the best conceptual fit.
With input from participants, the project team assigned the following labels to each of the clusters on the concept map: (1) understanding palliative care; (2) knowing how to access palliative care; (3) planning ahead; (4) community support for palliative care; (5) caregivers are supported; (6) comfort talking about death and dying; and (7) palliative care is normalized. Figure 2 shows the final concept map, with each cluster representing a domain of good public awareness of palliative care. The list of statements included in each cluster can be found in the Appendix.
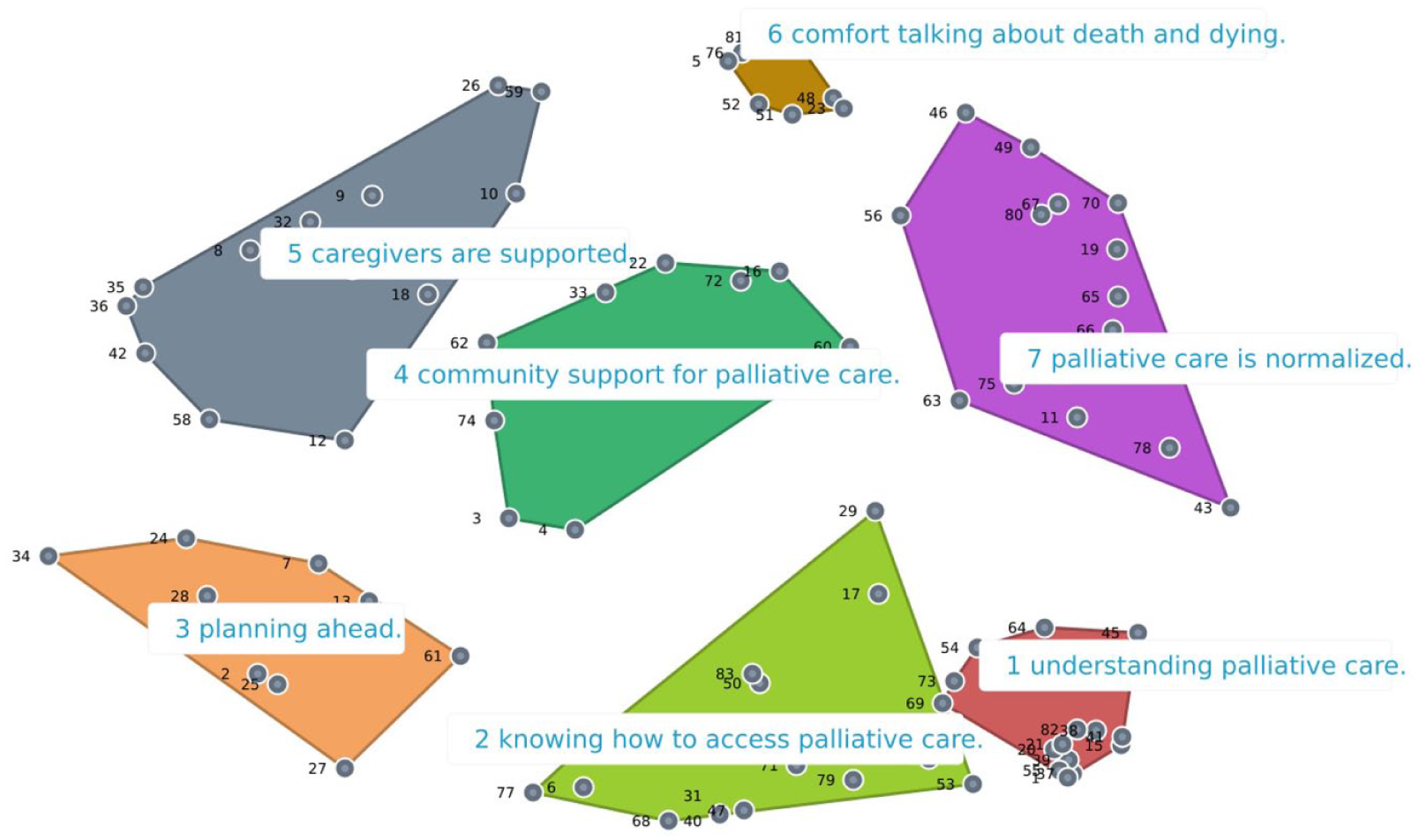
Final concept map: components of good public awareness of palliative care.
Importance ratings
Participants rated the importance of each statement on a scale of 1 (least important) to 5 (most important). Mean importance ratings for the seven clusters ranged from 3.80 to 4.07 (Table 3), suggesting that all clusters were considered important and each cluster was considered roughly equal in importance to the others. There was greater variation in the importance rating assigned to individual statements, from a low of 2.60 to a high of 4.66 (Appendix).
Average importance ratings of the seven clusters.

Application
The Palliative Institute used the concept map to develop a framework for our project activities by prioritizing four of the seven clusters for targeted intervention. The four areas we prioritized were: improving understanding of palliative care (cluster 1); building community support for palliative care (cluster 4); encouraging planning ahead (cluster 3); and increasing comfort talking about death and dying (cluster 6). Clusters 2 (knowing how to access palliative care) and 5 (caregivers are supported) were not prioritized because we determined them to be largely outside the scope of our project, which has a mandate to increase palliative care awareness among the general public prior to needing to access it. Additionally, we noted the presence of community organizations and programs working effectively in these areas, such as Caregivers Alberta and the Nav-CARE program (offered by a number of hospice and palliative care societies in Alberta). We interpreted the seventh cluster on the concept map, “palliative care is normalized,” as the end goal or outcome of improved public awareness of palliative care. After selecting four areas of focus, we conducted a global scan for educational tools and resources for public audiences, and selected a leading tool in each area to adapt and promote for use in Alberta in collaboration with community partners. These resources are all available free of charge at: https://covenanthealth.ca/about/centres-and-institutes/palliative-institute/compassionate-alberta/
Discussion
This study applied group concept mapping to reach conceptual clarity around what constitutes good public awareness of palliative care. On our concept map, clusters 1 (understanding palliative care) and 2 (knowing how to access palliative care) are closely related but distinct domains. Statements falling into cluster 1 encompass familiarity with what palliative care is, what kinds of support it offers, and who can benefit from it (i.e., statement 82: “people understand you can benefit from palliative care right from diagnosis of a life-limiting illness”). Statements in cluster 2 relate to knowing how and where to access palliative care support and information (i.e., statement 44: “people are equipped to request palliative care from their health care team,” and statement 47: “people know where they can go to find more information about palliative care”). Notably, some statements in cluster 2 also overlap with cluster 3 (planning ahead), perhaps because understanding how palliative care is accessed may inform people’s advance care planning (i.e., statement 29: “being able to make informed decisions about what is best for you and your family at end of life,” and statement 30: “understanding the different care options at end of life.”)
Cluster 3 (planning ahead) mainly focuses on opportunities to integrate advance care planning and goals of care discussions into healthcare interactions (i.e., statement 24: “Goals of care discussions are a regular part of annual check-ups or as conditions change”). It also highlights estate planning as a place this should be integrated (i.e., statement 27: “that advance directives, identification of an agent, and goals of care are part of estate planning”) as well as the importance of general preparedness (i.e., statement 7: “people are well-prepared for death” and statement 28: “people have advance directives”).
Clusters 4 and 5 are related components of palliative care awareness, signaled by their proximity on the concept map. Cluster 4 (community support for palliative care) includes the idea that education and support are community-based – not confined to the health system (i.e., statement 74: “information, resources, and education are embedded in the community, not only in health care institutions”) as well as the vision that people are equipped to help members of their communities (i.e., statement 33: “family, friends and social networks understand some of the practical ways to help people who are dying or those who are caring for them”). Cluster 5 (caregivers are supported) includes social recognition (i.e., statement 9: “caregivers are acknowledged and celebrated”) as well as practical empowerment (i.e., statement 42: “having the confidence and skills to provide care for a dying loved one, in partnership with health providers”). There is some overlap between these two clusters, and some statements that appear in cluster five appear to better fit the cluster four label, and vice versa. This reflects the fact that participants grouped the statements and labeled the clusters according to their own logic before the final concept map and labels were determined.
Cluster 6 (comfort talking about death and dying) includes conversations between family and friends (i.e., statement 57: “we can talk about death and dying with our families, children, friends and significant others in an open and honest way”) as well as in the community at large (i.e., statement 5: “conversations about death and dying take place in a variety of community settings”). Cluster 7 (palliative care is normalized) includes statements such as, “palliative care is accepted as a normal part of a treatment plan” (statement 65) and “no stigma is attached to it” (statement 70). In both domains, the goal is to make conversations about death and palliative care, respectively, more common and comfortable, in interpersonal relationships, clinical interactions, and society at large.
This exercise is, to our knowledge, the first utilization of group concept mapping in the area of palliative care public awareness, although it has been employed elsewhere in the field of palliative medicine.36–38 The seven components of good public awareness of palliative care highlighted on the concept map align with many of the global trends in palliative care policy and research. For example, the “planning ahead” cluster aligns with extensive literature stressing the importance of patient preparedness through conversations about care preferences with family members and healthcare providers, which is reflected in the range of tools and resources developed to support this.39–41 The cluster, “community support for palliative care,” emphasizes the importance of building social connections and “networks of care” around people living with serious illness, a central objective of the Compassionate Communities movement.20,42 Researchers and organizations involved in this movement have highlighted how partnerships between communities and the healthcare system improve quality of life.43,44 What makes the concept map the Palliative Institute produced particularly valuable is the way related but distinct concepts are organized and represented visually.
Limitations of this exercise include the small sample size and convenience sampling method. Additionally, validity of the focus prompt and the instructions for sorting and rating statements were not assessed. We did not conduct a sample size calculation for the study, and although a larger number of participants might produce different results, our sample size (n = 19) is within the recommended range for group concept mapping. 25 We acknowledge that limiting participation in this study to professionals affiliated with the Palliative Institute might have missed important perspectives that could have been provided by people who have benefited from palliative care, such as patients, caregivers, and bereaved caregivers. Future studies could be conducted to include these populations. The consensus around the seven-cluster map as the preferred map is subjective, as was the labeling of each cluster. Future research involving a larger sample size, different recruitment methods, or validity testing of the focus prompt could help validate or refine the seven clusters we identified – or produce a different map entirely. Additionally, given that our study took place entirely online, it is possible that a different method such as a group brainstorming session may have generated different results (e.g., with participants building off of each other’s ideas, or participants hesitating to share their ideas in a group setting). That said, the map generated has proved useful to this project and resonates with the research literature and activities undertaken by many other organizations working to improve public awareness of palliative care.
Conclusion
Structured group concept mapping was an effective mixed methods approach that enabled the Palliative Institute to clarify and define the scope of a project to raise public awareness of palliative care and identify areas for intervention. Other organizations that share this aim may benefit from considering these seven key components of good palliative care public awareness and assessing which domain(s) represent gaps or needs within their communities or target audience. Future research is warranted to determine whether implementing interventions to support each of these seven domains ultimately improves palliative care uptake.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524261451439 – Supplemental material for Using group concept mapping to conceptualize “good public awareness of palliative care”
Supplemental material, sj-docx-1-pcr-10.1177_26323524261451439 for Using group concept mapping to conceptualize “good public awareness of palliative care” by Mary-Ann Shantz, Abisola Omoniyi, Lynn Dare, Patricia Biondo, Melanie Doiron and Louise Kashuba in Palliative Care and Social Practice
Supplemental Material
sj-docx-2-pcr-10.1177_26323524261451439 – Supplemental material for Using group concept mapping to conceptualize “good public awareness of palliative care”
Supplemental material, sj-docx-2-pcr-10.1177_26323524261451439 for Using group concept mapping to conceptualize “good public awareness of palliative care” by Mary-Ann Shantz, Abisola Omoniyi, Lynn Dare, Patricia Biondo, Melanie Doiron and Louise Kashuba in Palliative Care and Social Practice
Footnotes
Appendix
The following tables show the synthesized list of 84 unique statements generated in response to the prompt, “Good public awareness of palliative care means . . .,” grouped by cluster, with mean importance ratings for each statement.
Acknowledgements
We gratefully acknowledge the advice of the Palliative Care Public Awareness advisory committee and the contributions of Dr. Konrad Fassbender.
Ethical considerations
Ethical review and approval were waived for this study by the Health Research Ethics Board of the University of Alberta as the public awareness project activities were deemed to fall under the category of quality improvement.
Consent to participate
Participants were advised that this activity was voluntary. As participation was all online, consent to participate was implied by the action of logging into the GroupWisdom software and completing the concept mapping activity(ies). Participants were not compensated for taking part in the study.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors disclose receipt of funding from the Government of Alberta to support this quality improvement initiative [grant number 010831].
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The authors confirm that the data supporting the findings of this study are available within the article and its Supplemental Materials. The study protocol can be obtained from the corresponding author* upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.