
Abstract
Background:
While healthcare costs continue to grow, an aging population along with rising chronic diseases are increasing demand for high-quality end-of-life care.
Objective:
Our objectives include calculating hospital cost sub-categories, such as laboratory, medication, nursing, physician, and social counseling, and evaluating the economic impact of specialist palliative care (sPC) on overall hospital costs per stay and per day of severely ill and dying patients who died at a Swiss university hospital between 2016 and 2022.
Design:
Retrospective, observational cohort study with a control group.
Methods:
We used administrative cost data from the final hospitalization of patients who died at a university hospital in Switzerland. We compared hospital costs of patients receiving care, including sPC, with those of individuals receiving usual care (UC). We defined timely sPC referral as initiating within 3 days of admission. We used a generalized linear model—assuming gamma-distributed errors and with a logarithmic link function—adjusted by inverse probability weighting to adjust for patient characteristics differences.
Results:
Adjusted overall hospital costs per stay were higher for sPC (Swiss francs (CHF) 31,350 (95% confidence interval (CI) 28,590–34,854)) compared with UC patients (CHF 20,351 (95% CI 18,454–22,596)); mean ratio of 1.54 ((95% CI 1.34–1.77), p < 0.001). In contrast, adjusted overall daily costs were lower for sPC patients (CHF 400); mean ratio 0.87 ((95% CI 0.79–0.97), p = 0.005), mainly due to reduced diagnostic and medication costs. However, longer hospital stays (sPC 11 days vs UC 5 days) offset daily cost reductions. UC patients had nearly double the total costs of timely sPC referral patients (cost ratio 0.52, CI 0.46–0.58).
Conclusion:
To capture intended and unintended effects and avoid oversimplified cost debates, hospital cost analyses of sPC should examine detailed cost sub-categories rather than only total costs. Cost optimization could be reached by timely transfer of patients with sPC needs. Future studies should investigate barriers to transitioning patients across care settings to improve both quality and cost-effectiveness.
Plain language summary
As people age and chronic illnesses become more common, more people need high-quality care at the end of their lives or end-of-life care. Hospitals must provide end-of-life care, while also keeping costs manageable.
We examined hospital costs for patients who died at a university hospital in Switzerland between 2016 and 2022.
We compared two groups: patients who received specialist palliative care (sPC) and patients who received usual care (UC).
sPC focuses on
• relieving symptoms
• improving comfort
• supporting patients and families
We looked at hospital cost data, including expenses for staff; medications; laboratory; and other services, then we made adjustments for patient characteristic differences.
Since we found patients receiving sPC had longer hospital stays (11 days) when compared with UC patients (5 days), their total hospital costs per stay were higher (about CHF 31,000 for sPC vs. CHF 20,000 for UC).
However, patients receiving sPC showed lower daily hospital costs by around CHF 400—a lower cost mainly from receiving fewer diagnostic tests and taking less medications.
Our findings suggest that while sPC reduces the intensity and cost of care per day, the longer stays mean that overall costs per stay are higher.
Based on our study, we developed a few recommendations. To make the most of benefits from sPC, hospitals could combine it with timely discharge planning and good follow-up options, such as hospice, home-based care, or long-term care facilities.
Our recommended approach could improve patient comfort, maintain quality, and help manage healthcare costs more effectively, while supporting patients and their families at the end of life.
Introduction
As populations continue to age and the prevalence of chronic diseases rises, the demand for high-quality, patient-centered end-of-life care is increasing. 1 Specialist palliative care (sPC) plays a critical role in addressing this demand by improving the quality of life for patients with life-limiting illnesses. It does so through comprehensive management of physical symptoms, psychosocial support, and facilitation of coordinated decision-making. 2
While the clinical benefits of sPC—such as better symptom control and higher patient satisfaction—are well documented, its economic implications remain an important and evolving area of research.3,4 A growing body of literature has examined the economic implications of sPC. Systematic and umbrella reviews indicate that sPC interventions are frequently associated with reduced healthcare utilization and lower costs, particularly through decreased use of intensive treatments and hospital services at the end of life.5 –8 However, findings vary substantially across healthcare systems, study designs, and outcome measures. In addition, many existing studies focus on overall healthcare expenditures, whereas relatively few analyses provide detailed insights into hospital cost structures or examine how specific cost categories contribute to overall hospital spending.6,7,9 Moreover, the timing of referral to sPC has been suggested to influence clinical decision-making, treatment intensity, and healthcare utilization during hospitalization.10 –12
In Switzerland, 37.2% of all deaths occur in hospitals, and referrals to sPC often take place late in the illness trajectory, frequently during a final hospitalization.13,14 University hospitals, which are central to the Swiss healthcare system, bear a large share of specialist and emergency care for patients with complex health problems, while also serving as centers for medical education, research, and training. These institutions face substantial operational and financial pressures from high personnel costs, advanced medical technologies, and needs for continuous infrastructure maintenance. Notably, healthcare expenditures peak at the end-of-life, making this period particularly relevant for cost analyses. 15 Understanding how the involvement of sPC referral during hospitalization relates to hospital resource use and cost patterns is therefore of particular interest.
Building on the findings of a previous 1-year study, 9 we now examine longer-term trends in a retrospective 7-year study. Specifically, we aim to assess whether hospital costs differ between patients who received sPC and individuals who did not during their final hospital stays. Furthermore, we investigate detailed hospital cost categories, such as medication, laboratory services, nursing, physician services, social counseling, and material costs (i.e., medical consumables and treatment-related supplies used during hospitalization), to better understand which components contribute most to overall expenditures for each group. As a secondary (sensitivity) analysis, we explore whether timely referral to sPC during hospitalization is associated with differences in hospital costs. Our goal is to generate robust empirical evidence to inform healthcare planning and reimbursement models for patients in the last phase of life and to better understand patterns of resource use associated with sPC in hospital settings.
Methods
Study design
After securing ethical approval (BASEC-ID: 2021-00253), we performed a retrospective observational cohort study based on administrative and clinical data from a large Swiss university hospital.
Setting
Our study was conducted at a Swiss university hospital equipped with 846 beds, accommodating over 57,000 inpatients per year and comprising 39 different clinical units.16 –18 The sPC unit within the hospital consists of ten beds and an ambulatory and in-house consultation service. It offers an interdisciplinary therapeutic approach (physiotherapy, nutrition counseling, social counseling, psychotherapy); full access to diagnostic and therapeutic measures (computed tomography, magnetic resonance imaging, chemotherapy, radiotherapy); and supports concurrent care. 19
In Switzerland, basic health care insurance is mandatory for all residents. Due to the basic insurance requirement, residents in need of inpatient sPC hardly experience financial barriers to access sPC. The standardized basic insurance package covers essential medical and pregnancy-related services, including both ambulatory and inpatient care, medications, and medical aids, assessed as necessary from medical and cost perspectives. Residents may purchase voluntary private or semi-private insurance to access additional benefits, such as complementary medicine, dental care, and private hospital rooms. 11
Hospitals are reimbursed for their services through a combination of public health insurance, government funding, and low patient out-of-pocket payments. Inpatient hospital services are primarily reimbursed through an activity-based funding mechanism using the Swiss Diagnosis-Related Groups (SwissDRG) system, whereby hospitals receive a fixed payment per case depending on diagnosis, procedures, and case severity.20 –22 Hospital sPC is part of a regional PC network offering 24/7 mobile sPC for home care and nursing homes; hospice care is not yet available to date.
Sample selection
An independent, in-house data department extracted administrative data from the last hospital admission of patients who died between January 1, 2016 until December 31, 2022. We considered patients discharged from the hospital and readmitted within 18 days as a single hospitalization according to SwissDRG (diagnosis-related groups). 23
We excluded patients from the study population if they refused to allow their health-related data to be used for research purposes and if they were younger than age 18. Moreover, we excluded patients if they died as a result of injury, poisoning, or other consequences of external causes, such as self-harm, assault, or accidents with transport vehicles, or were classified as other according to the International Classification of Diseases, 10th revision, and if death was a result of medical or surgical complications when the patient was otherwise healthy. We also excluded ambulatory patients with less than a minimum of one night at the university hospital and patients with missing cost data.
We classified patients as receiving sPC if (1) they received treatment as part of an in-patient stay in the PC ward; (2) the patient’s attending physician requested a consultation and the patient was seen and evaluated by the sPC team at one or more visits; or (3) at least one set of recommendations was made by the sPC team for the primary team caring for the patient. Patients were classified as not receiving sPC (hereafter referred to as “usual care,” UC) if the above sPC criteria did not apply. A patient was classified as a long-term patient if their length of stay (LOS) exceeded 28 days, a threshold commonly used in previous studies to ensure comparability of results.24 –26
For a sensitivity analysis, patients were classified as either with or without care from the intensive care unit (ICU). Patients were classified as having ICU care if they spent at least one night in the ICU during their complete final hospitalization. For our main analysis, we excluded ICU patients because intensive care represents a clinically and economically distinct setting with substantially higher and more variable costs. 27 However, we included ICU patients in the sensitivity analysis to assess robustness. We also classified patients as timely sPC referral patients. We defined timely sPC referral patients as receiving sPC within the first 3 days of hospitalization. The three-day cut-off was based on existing literature28,29 and expert consensus. This timeframe reflects the early phase of hospitalization during which treatment goals and care intensity are typically determined in acute care settings. Involvement of sPC within this period allows the team to contribute to these decisions, whereas later referrals often occur after treatment escalation has already taken place.
Data and cost categories
We utilized administrative resource use and cost data recorded by hospital staff from the hospital’s clinical documentation and financial systems. The dataset provided detailed information at the most granular level available, including single-dose oral medications, minutes of service provision, treatments provided, and exact dates. Consequently, we considered the hospital costs incurred during the period from patient admission to patient death.
Our cost assessment adopted the perspective of the healthcare provider, capturing its real costs; the costs represent the actual unadjusted costs the hospital incurred to deliver services. No adjustments occurred for specific prices or years. We incorporated all hospital expenses without selecting or excluding specific types of care costs. Overhead costs were taken into account and distributed evenly. We report costs in Swiss francs (CHF).
To reflect all areas of hospital costs comprehensively, we categorized the cost data into seven distinct categories 9
Catering costs: includes food and beverages provided to patients.
Laboratory costs: covers internal and external laboratory analyses.
Materials costs: includes items such as cannulas, bandages, tubes, pumps, and implants.
Patient management costs: encompasses administrative services, such as medical controlling, patient registration, bed management, and archiving of patient records.
Pharmacy costs: includes all medications provided, such as oral drugs, transfusions, and other pharmaceutical supplies.
Room costs: measured based on room size (standardized price per square meter) and includes surcharges for private rooms and services like telephony.
Staff costs subgroups a. Nursing costs: services provided by nurses, medical technical assistants, and pharmaceutical technical assistants, measured in tacs® nursing minutes. The Swiss data method tacs® measures (in)direct nursing care time for monitoring and cost analyses.30,31 b. Physician costs: services provided by physicians across different clinics and hierarchical levels, based on a fixed number of effort points (Taxpunkte) that reflect the cost of each service.
32
c. Social counseling costs: includes psychological and social counseling services based on fixed number of effort points. d. Therapy costs: includes services from physiotherapists, occupational therapists, and music therapists based on a fixed number of effort points.
Statistical analyses
Patient characteristics are presented with median and quartiles (lower, upper) for continuous variables and frequencies and percentages for categorical variables. We compared PC and UC groups using Mann-Whitney-Wilcoxon or chi-squared tests for continuous or categorical variables.
The association of sPC with hospital costs was subsequently assessed based on inverse probability of treatment weighting using propensity scores. In a first step, the propensity scores were derived by a logistic regression with age, sex, marital status (binary variable; married; yes/no), nationality, insurance class (public versus private and semi-private; yes/no), type of illness (cancer; yes/no; cardiovascular; yes/no), and living in the community before admission (yes/no).
We collapsed levels of covariates with few entries (insurance class, type of illness, and stay before entry). For the continuous variable age, we used a flexible parameterization. The multivariable fractional polynomial model that best predicted the outcome variable was selected automatically. Our method preserves the continuous nature of covariates in a regression model even if the relationships are non-linear. We trimmed resulting stabilized weights—inverse probabilities of treatment established through the logistic regression—using the method by Stürmer et al. 33 based on the 1st and 99th percentiles. Inverse probability weights were evaluated by assessing covariate balance using a Love plot and the overlap assumption using an overlap plot (Appendix Figures A1 and A2).
Assuming a gamma distribution of errors and using a logarithmic link function, generalized linear models of the costs were subsequently estimated and adjusted by inverse probability weighting using the stabilized weights. We calculated potential outcome means, average treatment effect, and average treatment effect for the treated on this basis.
Bias-corrected mean differences with bias-corrected 95% confidence intervals (CI) calculated on 2,000 bootstrapped samples 20 were reported. p-Values were derived from bias-corrected point estimates and bootstrap standard errors using a normal approximation. The main analysis was made on the full data set, excluding ICU patients; ICU patients were included in the sensitivity analysis. As a sensitivity analysis, we examined the association of timely sPC referral by comparing patients receiving sPC within the first 3 days of hospitalization (timely sPC referral) with UC patients. All analyses were done using Stata 18 (Stata Corporation, College Station, TX, USA).
Results
Patient characteristics
Between 2016 and 2022, a total of 10,558 patients died in the hospital. Of these, 4316 (41%) met the eligibility criteria for inclusion in the study. We present a detailed flowchart of the study population in Figure 1. The primary analysis included 1839 non-ICU patients, comprising 1210 who received UC and 629 who received sPC. For the sensitivity analysis, we focused on patients who received ICU treatment: 65.7% of included UC patients received ICU care, compared with 20.4% of those in the sPC group. In total, the sensitivity analysis included 3526 UC patients and 790 sPC patients.

Inclusion flowchart for study population.
As shown in Table 1, the study population for the main analysis was predominantly male (57%), of Swiss nationality (91%), married (52%), and admitted to the hospital from home (69%). Over three-quarters of all included patients—75% in the UC and 80% in the sPC group—had only mandatory health care insurance, without additional private coverage. sPC patients were significantly younger (69 years vs 82 years, p < 0.001), had higher clinical complexity (case-mix index, 1.5 vs 1.1, p < 0.001), and more often with an oncological primary diagnosis (83% vs 27%, p < 0.001) compared with UC patients. Median LOS was significantly longer for sPC patients when compared with UC patients (11.0 days vs 5 days, p < 0.001). Moreover, 10% of sPC patients remained hospitalized for more than 28 days (long-term patients) compared with 2.3% in the UC group.
Baseline characteristics of usual care and sPC patients with and without ICU treatment who died between January 1, 2016 until December 31, 2022 in the university hospital.
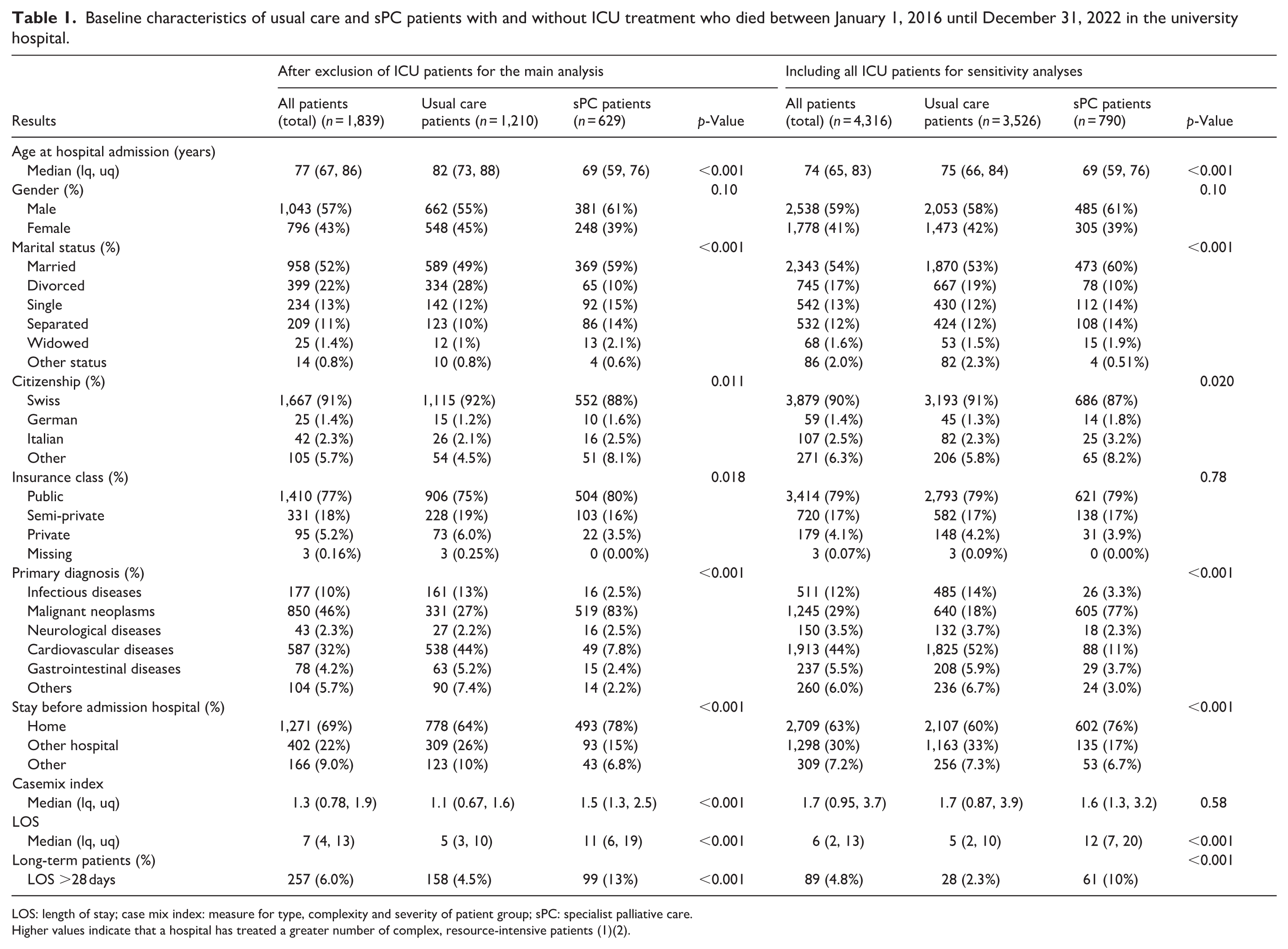
LOS: length of stay; case mix index: measure for type, complexity and severity of patient group; sPC: specialist palliative care.
Higher values indicate that a hospital has treated a greater number of complex, resource-intensive patients (1)(2).
Cost analyses
A summary of the key cost outcomes comparing sPC and UC across unadjusted and adjusted analyses is presented in Table 2. Adjusting cost for difference in patient characteristics was performed with inverse probability of treatment weighting which substantially improved the covariate balance between groups. Appendix Figure A1 shows the covariate balance between care groups before and after inverse probability of treatment weighting.
Summary of key cost outcomes comparing sPC patients and usual care patients.

ATE: average treatment effect; LOS: length of stay; PMD: potential mean difference; sPC: specialist palliative care.
p-Values were derived from bias-corrected point estimates using bootstrap standard errors and a normal approximation. Tests were two sided. Not corrected for multiple testing.
Overall hospital costs per stay of patients receiving sPC versus UC
In unadjusted analysis, overall costs per stay where higher for sPC patients (CHF 32,463 95% CI (29,981–35,229)) when compared with UC patients (CHF 18,047 95% CI (16,764–19,732)) with a mean ratio of 1.80 (95% CI (1.60–2.02), p > 0.001) and a mean difference of 14,416 CHF (95% CI (1428–17,634); Table A1). As these represent simple comparisons, they may reflect underlying differences in patient characteristics and selection into sPC.
After applying inverse probability weights to adjust for patient characteristics, the cost gap between the two groups decreased but remained present. Overall adjusted costs for patients receiving sPC were higher over the whole stay (CHF 31,350, 95% CI (28,590–34,854)) compared with UC patients (CHF 20,351, 95% CI (18,454–22,596)) with a mean ratio of 1.54 (95% CI (1.34–1.77), p > 0.001) and a mean difference of 11,000 CHF (95% CI (7,490–14,718); Table 3).
Adjusted overall potential mean hospital costs per stay of usual care and sPC patients using propensity score model (ICU patients excluded).

ATE: average treatment effect; PMD: potential mean difference; sPC: specialist palliative care.
p-Values were derived from bias-corrected point estimates using bootstrap standard errors and a normal approximation. Tests were two sided. Not corrected for multiple testing.
In the adjusted analyses of individual cost categories, laboratory costs (−15%) and pharmacy costs (−17%) were lower in the sPC group compared with the UC group. All other cost categories showed higher costs in the sPC group, with the most pronounced ones nursing (+93%), social counseling (+89%), therapy (+76%), and catering (+48%) costs.
Daily hospital costs of patients receiving sPC versus UC
In unadjusted analyses, sPC patients showed lower costs per day (CHF 2,423, 95% (CI 2,335–2,526)) than UC patients (CHF 3,107, 95% (CI 2,904–3,328)) with a mean ratio of 0.78 (95% CI (0.72–0.85), p > 0.001) and a mean difference of −684 CHF (95% CI (−923 to −450); Table A2). As above, these crude comparisons may reflect differences in patient characteristics between groups.
After applying inverse probability weights, overall costs per day in the sPC group (CHF 2,607, 95% CI (2,415–2,931)) were lower than in the UC group (CHF 3,007, 95% (CI 2,827–3,189)), with a mean ratio of 0.87 (95% CI (0.79–0.97), p = 0.005) and a mean difference of −400 CHF (95% CI (−664 to −108); Table 4).
Adjusted potential mean of hospital costs per day of usual care and sPC patients using propensity score model (ICU patients excluded).

ATE: average treatment effect; PMD: potential mean difference; sPC: specialist palliative care.
p-Values were derived from bias-corrected point estimates using bootstrap standard errors and a normal approximation. Tests were two sided. Not corrected for multiple testing.
For almost all cost categories, adjusted daily costs were lower for sPC compared with UC patients: laboratory (−51%), material (−31%), patient management (−56%), pharmacy (−38%), and physician costs (−33%). Daily nursing (+23%) and therapy (+33%) costs were higher in the sPC group when compared with the UC group. Catering, room, and social counseling costs did not differ between groups (Table 4).
Sensitivity analyses
For the sensitivity analysis, we included all ICU patients. The median case-mix for UC patients was higher by 0.6 points to an index of 1.7 and was higher than for sPC patients with an index of 1.6 points. Differences in cost categories between patients receiving sPC and individuals receiving UC became more pronounced. Specifically, sPC patients incurred lower diagnosis-related costs, with reductions of 69% for daily laboratory expenses, 66% for daily material costs, 68% for daily pharmacy charges, and 64% for daily physician services compared with UC patients. The mean cost ratio for overall costs per stay dropped by 0.36 points to 1.18 when ICU patients were included, compared with the ratio observed when ICU patients were excluded. Overall adjusted costs per day of the sPC group (CHF 3,360, 95% CI (3,127–3,802)) were lower than for the UC group (CHF 6,509, 95% CI (6,271–6,756)) with a mean ratio of 0.50 (95% CI (0.46–0.54), p < 0.001; Table 1 includes baseline characteristics and Tables A3 and A4, the cost overview).
The cost differences became even more pronounced when focusing on patients who received a timely referral to sPC intervention compared with UC patients. The mean cost ratio for the total hospital stay dropped to 0.52 (CI 0.46–0.58), indicating that UC patients incurred almost twice the overall costs compared with timely sPC referral patients. Similarly, the mean ratio for daily costs per patient was 0.38 (95% CI 0.35–0.41). Across all cost categories—excluding catering and therapy— timely sPC referral patients consistently showed lower daily expenditures than those receiving UC. Timely sPC referral patients have a median stay 3 days longer in the hospital than UC patients (median 8 days vs 5 days per patient stay). Staying more than 28 days in the hospital, 5% of all timely sPC referral patients were long-term patients. Timely sPC referral patients also showed a lower median case-mix index (1.4 vs 1.7; Table A5 includes baseline characteristics and Tables A6 and A7, the cost overview).
Results were robust in a sensitivity analysis excluding long-term patients (LOS >28 days; Table A8includes baseline characteristics and Tables A9 and A10, the cost overview).
Discussion
Main results
In our 7-year retrospective analysis, patients receiving sPC incurred substantially lower hospital costs on a per day basis—13% less (CHF 400) when compared with patients receiving UC. However, the cost advantage did not translate into lower total hospitalization costs, owing to longer average LOS among sPC patients (+5.1 days). Our results are consistent with our earlier 1-year study, indicating that daily cost reductions associated with sPC are sustained over time, yet remain highly contingent on the availability of high-quality care settings outside the sPC department.
Nevertheless, these results diverge from prior studies reporting lower total costs among sPC patients.34 –38 One potential explanation for this discrepancy is the presence of a subgroup of long-stay sPC patients with elevated cumulative costs. These extended stays may be driven by the unavailability of appropriate, post-acute rehabilitative care facilities, limiting timely discharge from the hospital. Even though all patients in our cohort died in hospital, prolonged stays may still reflect system-level constraints, whereby patients remain hospitalized until death due to limited availability of appropriate discharge options (e.g., hospice or community care).
Further stratification revealed only timely sPC referral interventions—initiated within 3 days of admission—as associated with important overall cost savings. Notably, nearly half of all sPC patients (49.7%) received their first sPC intervention later than 3 days post-admission; patients exhibited prolonged hospital stays and higher total costs. Our findings highlight the need for the rapid identification of acute palliative care needs to adjust routine acute hospital management of patients early on and timely integration of sPC in hospital settings.
Our detailed cost breakdown into cost categories provides additional insight. sPC patients showed markedly reduced diagnosis-related daily costs—such as for laboratory services, medications, and physician interventions—by over one-third, with some categories reduced by up to 50%. Conversely, patient-related daily costs, including nursing and therapy, were higher among sPC patients, possibly reflecting the increased intensity of person-centered care. Nursing and therapy services possibly contribute to improved care quality for patients and their families. Including high-cost ICU patients further amplified the cost differences.
Comparison with other end-of-life care models
Our findings align with international evidence indicating that hospital-based end-of-life care is typically more expensive than care provided in hospices or at home. In a rapid review, Spencer et al. 39 reported hospital-based palliative care costs range from £10,000 to £64,000 in 2023 prices per hospital death. In comparison, the cost of hospice end-of-life care in 2023 prices ranged from £2000 to £21,000, while home- and community-based palliative care ranged from £900 to £21,000. 39 In 1983, Birnbaum and Kidder 40 found hospital-based hospice care per day was 44% more expensive than home-care hospice costs. Another report from 2012 from the organization “Marie Curie” 41 states that shifting end-of-life care from hospitals to community settings could reduce daily costs by as much as £280.
Results emphasize the main cost driver of sPC in hospitals is prolonged LOS, which is influenced by the availability of alternative care options within a care region. Inadequate capacity for transferring stable yet clinically complex patients to adequate and affordable hospice or long-term care facilities leads to avoidable hospital costs. Therefore, LOS may be a poor proxy for cost-evaluation studies unless contextualized by system-level constraints. Achieving a balance between cost-effectiveness and quality of care remains a central challenge for healthcare systems. 42
Our results support the notion that earlier discharge to community-based care—when medically appropriate—reduces costs while respecting patient preferences and maintaining care quality.
Practice implications
Providing high-quality care for patients with advanced, life-limiting illnesses requires well-coordinated, trans-sectoral collaborations within regional care networks. Central to such coordination is the seamless organization of services across institutional boundaries, coupled with avoiding institution-driven reimbursement models, such as payment per care setting, which tend to fragment care delivery and undermine efficiency. 43
sPC offers a paradigmatic example of network-based, trans-sectoral service provision. However, sPC can only be fully appraised when evaluated from a societal, healthcare system perspectives rather than from hospital-level perspectives. From a broader vantage point, relevant outcomes extend beyond direct costs of care to encompass improvements in quality, coordination, and smooth transitions of patients across care settings.
In Switzerland, such economic evaluation is currently hindered by a fragmented reimbursement system. Each sector—acute in-patient care, outpatient services, and long-term care—operates under distinct financing structures. Consequently, financial incentives and care responsibilities are largely confined to individual institutions, such as university hospitals, rather than shared across care networks. The structural fragmentation impedes coordinated care delivery and limits opportunities for cost optimization.44 –46
Addressing the gap requires a strategic expansion of community-based palliative care services. Strengthening patient transitions from hospitals to hospice or home-based care possibly reduces healthcare expenditures while better aligning with patient preferences. Notably, a representative survey found 72% of the Swiss population prefer to die at home.47,48 However, such a shift involves careful implementation to avoid transferring excessive care responsibilities to family members, which risks rendering substantial portions of healthcare labor and costs invisible. 41
Current capacity constraints require complementary measures. One promising strategy involves identifying patients earlier who may benefit from sPC during hospitalization. Timely referral and intervention enable more efficient allocation of sPC resources and promote continuity of care throughout the disease trajectory. While our study does not assess the quality of care, targeted investment in supportive care services potentially improves patient outcomes and optimizes healthcare resource utilization.
Limitations
We note several limitations. First, the generalizability of our findings is restricted by the single-center design focused on a singular university hospital. Cost structures and resource availability possibly differ across hospital types, such as private or non-profit and regions. Future research should include multicenter or international datasets to enhance external validity and inform policy debates, particularly around reimbursement models.
Second, our retrospective design carries inherent limitations, including the potential overestimation of costs, since sPC is often layered onto existing therapies. Furthermore, we did not differentiate between types of sPC interventions, such as ward-based versus consultation services, which possibly influence outcomes such as LOS. We did not differentiate between those groups, as our primary aim was to assess the overall association between sPC involvement and hospital costs. In our setting, both types of care are delivered by the same multidisciplinary sPC care team and are often part of a continuous care pathway, with some patients receiving both consultation and ward-based care during their hospitalization. However, future analyses separating sPC ward admissions from consultation-based sPC may provide further insights into potential differences in patient characteristics and outcomes.
Third, as the study spans a 7-year period, changes in clinical practice, hospital policies, or resource utilization over time may have influenced hospital cost patterns. Although the analyses adjust for observable patient characteristics, temporal changes in care delivery cannot be fully excluded.
Fourth, residual confounding and selection bias may be present. While we applied clear inclusion and exclusion criteria, unmeasured confounding factors—including psychosocial variables and in-hospital complications—potentially affected our results. Differences between the sPC and UC groups appear to be strongly linked to underlying diagnoses: patients with predominantly cancer-related conditions experience earlier hospital admission prior to death from stepwise functional decline, whereas individuals with primarily cardiovascular conditions more likely face sudden, acute deterioration. In addition, sPC patients tended to be younger and present with greater clinical complexity, as reflected by a higher case-mix index. The higher proportion of prolonged hospital stays among sPC patients may reflect both clinical complexity and system-level factors, including limited availability of appropriate discharge settings (e.g., hospice or community care), resulting in patients remaining in hospital until death. These factors may contribute to longer LOS and higher cumulative costs independent of the timing of sPC involvement. Although propensity score weighting was employed, the set of observed covariates was limited.
Fifth, as a consequence of the above, no causal claims are possible.
Finally, our dataset lacked complete discharge and survival status data, restricting our ability to follow patient trajectories post-discharge. A prospective, longitudinal design encompassing multiple care settings would be more suitable for fully capturing the cost dynamics of palliative care.
Conclusion
Our study highlights the complex relationship between sPC, hospital resource use, and costs in a university hospital in Switzerland. While sPC was associated with lower daily hospital costs—primarily related to diagnostic procedures, medication, and physician services—longer LOS may offset these differences when considering total hospital costs. Timely sPC referral was associated with shorter hospital stays and lower overall costs, suggesting potential efficiency gains when sPC needs are identified early. However, nearly half of patients only received sPC after 3 days, limiting benefits.
Investments in sPC and alternative care models may improve care quality while contributing to more efficient use of healthcare resources. University hospitals may therefore play an important role in integrating sPC into end-of-life care pathways.
Future research should examine cost trajectories across care settings, including hospice and home care, to better understand the broader economic implications of sPC. In particular, future studies should account for patient trajectories and system-level constraints, such as discharge capacity, when interpreting LOS and cost outcomes. A comprehensive economic perspective that captures costs across different care settings during the final phase of life may help inform strategies for effective and patient-centered care for individuals with advanced serious illness.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524261452273 – Supplemental material for Cost impact of in-patient specialist palliative care: A retrospective economic study of administrative end-of-life hospital costs across 7 years in Switzerland
Supplemental material, sj-docx-1-pcr-10.1177_26323524261452273 for Cost impact of in-patient specialist palliative care: A retrospective economic study of administrative end-of-life hospital costs across 7 years in Switzerland by Monika Hagemann, Matthias Schwenkglenks, Odile Stalder, Steffen Eychmüller and Maud Maessen in Palliative Care and Social Practice
Footnotes
Appendix A
Adjusted potential mean of hospital costs per day comparing usual care and sPC patients (incl. ICU) excluding long-term patients with a length of stay >28 days using a propensity score model.

| Results | Usual Care patients excl. long-term patients | sPC patients excl. long-term patient | ATE | PMD | |
|---|---|---|---|---|---|
| Potential outcome mean (95% CI) | Potential outcome mean (95% CI) | Mean ratio (95% CI) | p-Value* | Mean difference (95% CI) | |
| Adjusted average costs per hospital day | 6615 (6369–6880) | 3597 (3302–3541) | 0.55 (0.50–0.54) | <0.001 | −3017 (−3374 to −2990) |
| Catering | 28 (27–29) | 43 (40–47) | 1.54 (1.44–1.69) | <0.001 | 15 (12 to 19) |
| Laboratory | 386 (359–416) | 119 (89–188) | 0.32 (0.23–0.48) | <0.001 | −267 (−312 to −191) |
| Material | 876 (786–967) | 378 (281–281) | 0.79 (0.34–0.34) | 0.39 | −499 (−557 to −520) |
| Patient management | 67 (65–69) | 28 (25–32) | 0.42 (0.37–0.48) | <0.001 | −39 (−43 to −35) |
| Pharmacy | 800 (728–886) | 240 (158–368) | 0.31 (0.20–0.47) | <0.001 | −561 (−681 to −414) |
| Rooms | 347 (316–384) | 190 (171–220) | 0.55 (0.47–0.66) | <0.001 | −157 (−199 to −114) |
| Staff | 4020 (3910–4136) | 2600 (2405–2546) | 0.65 (0.60–0.64) | <0.001 | −1420 (−1639 to −1424) |
| Nursing | 1298 (1252–1345) | 1429 (1330–1445) | 1.11 (1.02–1.13) | 0.017 | 131 (28 to 169) |
| Physician | 2634 (2540–2741) | 1061 (929–1108) | 0.41 (0.35–0.42) | <0.001 | −1573 (−1730 to −1487) |
| Social counseling | 41 (39–42) | 42 (38–45) | 1.03 (0.93–1.12) | 0.55 | 1 (−3 to 5) |
| Therapist | 48 (46–50) | 67 (60–69) | 1.43 (1.26–1.47) | <0.001 | 20 (12 to 22) |
ATE: average treatment effect; PMD: potential mean difference; sPC: specialist palliative care.
p-Values were derived from bias-corrected point estimates using bootstrap standard errors and a normal approximation. Tests were two-sided. Not corrected for multiple testing.
Acknowledgements
We thank the anonymous reviewers, patients for sharing their data, and Dr. Kristin Marie Bivens for scientific editing.
Ethical considerations
Ethical approval for this study was obtained from the Ethics Committee of the Canton of Bern (BASEC-ID: 2021-00253) and conducted in accordance with the Swiss Human Research Act (HRA). Due to the retrospective nature of the study and the use of routinely collected data, the requirement for informed consent was waived by the ethics committee.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Our work was supported by the Swiss National Science Foundation (10531G_212822). The grant provider had no influence on designing the study; collecting, analyzing, and interpreting data; writing the report; and deciding to submit the article for publication.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Due to institutional policies and strategic restrictions by the university hospital’s finance department, raw cost data cannot be shared. Other data can be shared on request.
AI use disclosure
This manuscript benefited from the use of OpenAI’s GPT-5 for language refinement. The AI tool was used only to improve readability and efficiency; all interpretations, data analyses, and conclusions are the sole responsibility of the authors. The authors have verified the accuracy and integrity of all AI-assisted content.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.