
Abstract
Introduction
Mental health conditions, particularly depression and anxiety, are common among individuals with life-limiting illnesses and significantly affect their quality of life. However, little is known about their burden in palliative care in rural Malawi.
Objective
This study assessed the prevalence and factors associated with depression and anxiety among adult patients enrolled in the palliative care program in Neno District, Malawi.
Methodology
A cross-sectional study was conducted across nine health facilities from January to June 2024. Using simple random sampling, 152 adult participants were selected from the Neno district palliative care database. Quantitative data was collected using the PHQ-9 and GAD-7 as screening tools for depression and anxiety. The analysis used descriptive statistics and multivariable ordered logistic regression to identify factors associated with depression and anxiety, with results reported as adjusted odds ratios and 95% confidence intervals.
Results
Of 152 eligible patients, 151 completed the study (99% response rate). The mean age was 67 years (SD = 16.3); 78% (n = 117) were female, and 66% (n = 99) were unmarried. Depression was present in 72% (95% CI: 65.0%–79.4%, n = 109) and anxiety in 70% (95% CI: 62.1%–77.0%, n = 105). Suicidal ideation was reported by 3% (n = 4) of participants. Depression and anxiety were strongly associated (depression model: aOR = 1.490, p < 0.001; anxiety model: aOR = 1.506, p < 0.001). Older age was associated with higher anxiety severity (aOR = 1.027, p = 0.016). No other sociodemographic variables were significantly associated with either outcome.
Conclusion
The study findings underscore the high burden of depression and anxiety among patients under a palliative care program in Neno District, age-trailed mental health in chronic ill patients, and integration of mental health services and palliative care programs. Future research should examine how depression and anxiety develop in older adults to tailor interventions for this population.
Background
Over the past decade, palliative care has increasingly incorporated psychological, social, and spiritual aspects of well-being, recognising that serious illness affects the whole person and family. 1 Mental health conditions, particularly anxiety and depression, are common among patients with incurable illnesses such as advanced cancer, HIV/AIDS, diabetes mellitus, and heart disease.2,3 These conditions can substantially reduce quality of life, worsen physical symptom burden, impair treatment adherence, increase caregiver strain, and contribute to poorer clinical outcomes.4,5 Unfortunately, these conditions are underdiagnosed and undertreated due to stigma, diagnostic challenges, and systemic barriers.6,7
Globally, the need for palliative care remains considerable. The World Health Organisation (WHO) estimated that 56.8 million people require palliative care annually, including 25.7 million in their final year of life, yet only 14% receive such care. 8 Access gaps are most pronounced in low- and middle-income countries (LMICs), where health systems often face workforce shortages, fragmented referral systems, and limited access to psychosocial and specialist mental health care. In such a context, psychological suffering frequently remains under-recognised and untreated. 9
Evidence from sub-Saharan Africa and other resource-limited settings indicates that depression and anxiety among palliative care patients are shaped not only by disease severity but also by broader social determinants. 10 Prior studies have identified predictors including poor social support, financial hardship, uncontrolled pain, functional decline, caregiver dependence, HIV-related stigma, and uncertainty about prognosis. 11 In comparable neighbouring settings, individuals with advanced illness who face poverty, food insecurity, and transport barriers often report greater psychological distress. 12 These findings suggest that the interplay between illness and structural deprivation strongly influences mental health outcomes in palliative care.
This is relevant in Malawi, where many households experience multidimensional poverty and where chronic illness may intensify pre-existing economic vulnerability. The relationship between poverty and mental health is well established: poverty may increase stress, social exclusion, inability to meet treatment costs, and fear of becoming a burden on family members, while depression and anxiety may further reduce functional capacity and income generation. 13
Malawi has reported substantial levels of common mental disorders in general and clinical populations, with depression ranging from 19% to 39% and anxiety affecting approximately 19.63%, with many cases remaining underdiagnosed.14–16 However, evidence specific to palliative care populations remains limited, especially in rural districts where services are decentralised, and households face persistent socioeconomic hardship. Most regional studies have focused on single disease groups, particularly oncology or HIV cohorts, limiting understanding of psychological distress within mixed-diagnosis palliative care programs that reflect real-world delivery service.
The clinical composition of palliative care populations may also influence mental health outcomes. Patients with advanced cancer may experience pain, prognostic uncertainty, and rapid functional decline, whereas those living with advanced HIV/AIDS or end-stage non-communicable diseases may face prolonged illness trajectories, stigma, recurrent admissions, or cumulative disability. Yet few studies in rural African settings have looked at factors that may be associated with depression or anxiety within integrated palliative care services.
Neno District in rural Malawi presents a particularly important setting in which to examine these questions. It is a socioeconomically disadvantaged district with a decentralised palliative care programme serving patients with diverse terminal and chronic illnesses across hospitals and health centres. This creates an opportunity to assess psychological distress at the intersection of serious illness, ageing, and poverty within routine rural service delivery.
This study, therefore, aimed to assess the prevalence of depression and anxiety among adult patients enrolled in the palliative care program in Neno District, Malawi, and to explore factors associated with these outcomes. By generating evidence from a rural mixed-diagnosis cohort, the study contributes to a limited literature base and informs integration of mental health services into palliative care in low-resource settings.
Methods
Study design
A facility-based cross-sectional study to assess the prevalence and associated factors of depression and anxiety among patients under the palliative care program in Neno District, Malawi, was conducted. Primary data was collected using Patient Health Questionnaire-9 (PHQ-9) and Generalised Anxiety Disorder -7 (GAD-7), which have been previously used and validated in Malawi as well as similar settings, from patients enrolled in the palliative care program from nine health facilities providing the service.
Study setting
Neno District is a rural, resource-constrained setting in the southern region of Malawi characterised by high multidimensional poverty and predominantly subsistence-based livelihoods. Approximately three-quarters of households fall below the national poverty threshold, 17 creating structural vulnerabilities that intersect with chronic illness and access to care.18,19
Palliative care services in Neno District have progressively evolved from a centralised hospital-based model initiated in 2009 to a more distributed system involving both district and community-level facilities. Formal decentralisation to primary care sites occurred in 2022, where it involved devolving to seven of thirteen health centres, including Magaleta, Ligowe, Chifunga, Midzemba, Matope, Nsambi, and Dambe health centres (see Figure 1). Of the nine facilities included in this study, two are referral hospitals providing generalist palliative care services (Lisungwi Community and Neno District Hospitals), while the remaining seven are primary health centres delivering primary palliative care integrated into routine outpatient services. While core service components are standardised, minor contextual differences exist in staffing levels and access to specialist support across facilities. Patients are enrolled in the palliative care program based on clinical criteria, including terminal illnesses (advanced cancers, HIV/AIDS with complex treatment needs, end-stage NCDs, and progressive neurological conditions) or curable conditions that require complex care, including complicated TB patients. Enrollment is recommended for patients experiencing severe or persistent symptoms, recurrent hospitalisations, marked functional decline, or when disease-directed treatments offer limited benefit. Ambulatory patients receive palliative care at their nearest hospital or health centre, and others receive a home visit by staff from the referral hospital. Patients are regularly assessed across physical, psychosocial, spiritual, and socioeconomic domains. Those requiring psychosocial, spiritual, and economic support are referred to appropriate programs based on their needs, including mental health care. Shows a map of Health Facilities in Neno District.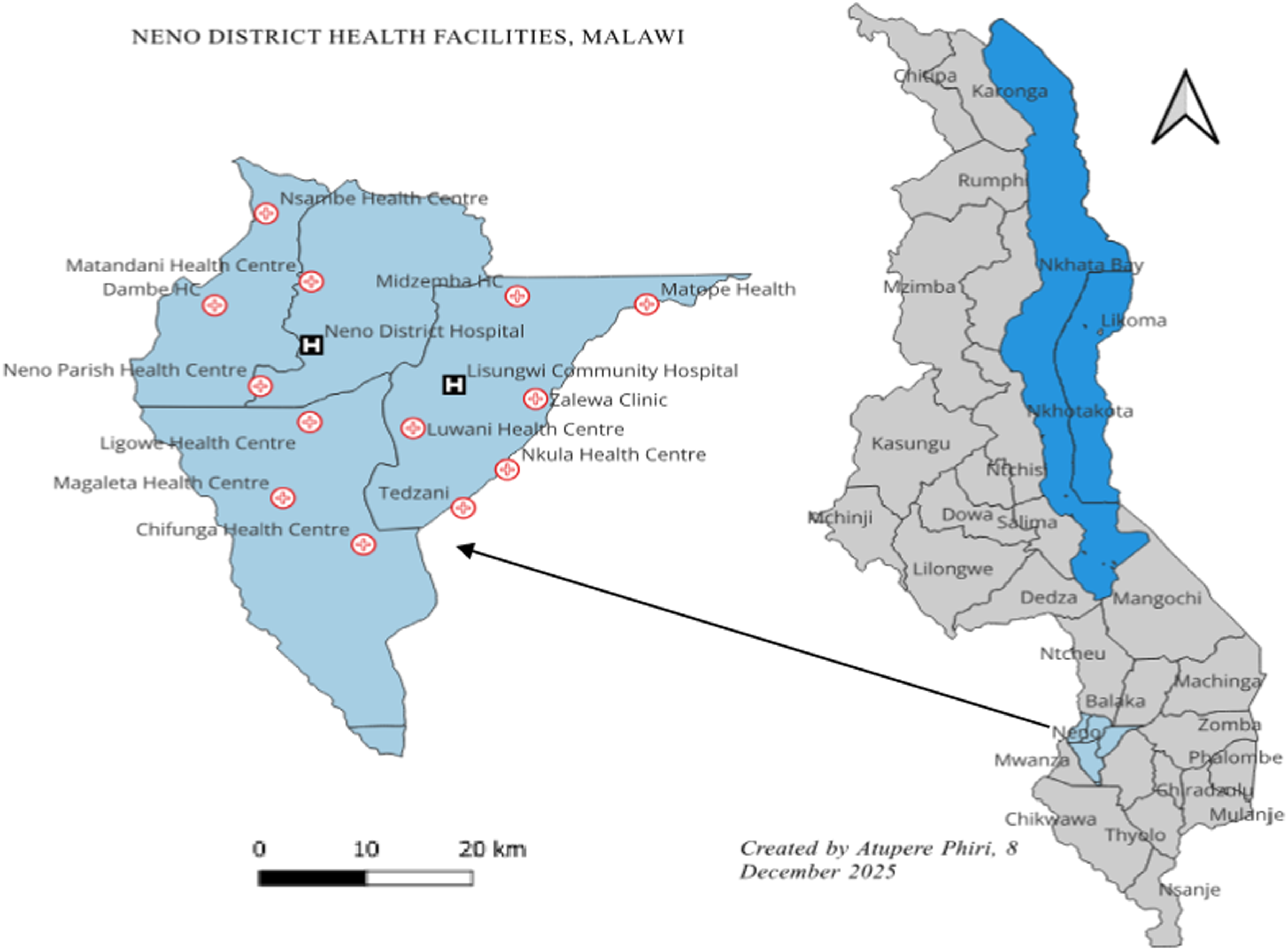
Sample size and sampling technique
The study included 152 adult participants selected from a source of 260 patients enrolled in the Neno District palliative care program between January 1 and June 31, 2024. The sample size was calculated using Cochran’s formula, assuming 95% confidence level (Z = 1.96), a 5% margin of error, and an estimated prevalence of 38% for combined mood disorders derived from prior evidence. 18 Because the source population of eligible palliative care patients was relatively small (N = 260), finite population correction was considered during sample size estimation. The corrected sample size remained comparable to the achieved sample of 152 participants. The sample size was primarily calculated to estimate the prevalence of depression and anxiety among palliative care patients. Multivariable ordered logistic regression analyses were conducted exploratorily to assess factors associated with symptom severity. To minimise model overfitting, the number of covariates included in the final models was restricted based on sample size considerations and distribution of outcome categories. Participants were randomly selected from a program registry of 260 eligible palliative care patients using a computerised process to ensure unbiased inclusion.
Inclusion and exclusion criteria
All adults aged 18 years and above enrolled in a palliative care program, and residing within Neno district, were eligible, while patients too ill to participate in interviews, patients with severe cognitive impairment preventing informed consent, and patients who declined participation were excluded from participating in the study.
Data collection
Data was collected between 21 August and 19 September 2024 using a structured electronic questionnaire via the CommCare platform, incorporating validated screening tools (PHQ-9 and GAD-7 assessment tools) to assess depression and anxiety symptoms among participants, for more see Supplementary Files 1 and 2. The questionnaire included the PHQ-9 and GAD-7 assessment tools. The PHQ-9 consists of 9 items scored from 0 to 3, yielding a total score of 0-27. For more information, refer to Supplementary File 1. The GAD-7 consists of 7 items scored from 0-3 with a total score range of 0-21. For more, refer to Supplementary File 2. A cut-off score of equal to or greater than 5 was used to define clinically significant depression and anxiety, respectively. The demographic information was entered once at enrolment within the application, while subsequent questionnaires focused on symptoms of depression and anxiety among the patients in the palliative care program. The GAD-7 assessment tool was validated in a secondary-level facility in Sub-Saharan Africa20,21 and used in rural Malawi, a similar setting, just as the Neno facilities, 22 while the PHQ-9 assessment tool is locally validated. 23 The PHQ-9 and GAD-7 tools have been previously validated in Malawi in primary care and community-based populations, demonstrating acceptable reliability and construct validity. While these validation studies were not conducted exclusively in palliative care populations, both instruments have been widely used in similar low-resource and chronic illness settings across sub-Saharan Africa. Given the absence of palliative care–specific validation studies in Malawi, the tools were considered appropriate for screening symptom burden in this study population. Nonetheless, interpretation of findings is made with recognition of the potential influence of advanced illness on somatic symptom reporting. Data were then collected using a CommCare application customised to the questionnaire, which included the aforementioned screening tools. These tools were translated into the local language, Chichewa.
Additionally, the screening tools captured demographic information, including patient ID, age, gender, marital status, education level, and religion. Special attention was given to question nine of the PHQ-9 assessment tool, which assessed suicidal ideation. Participants who reported any level of suicidal ideation (PHQ-9 item 9 score > 0) were immediately flagged by the electronic data collection system and referred to available mental health services within the district. Where on-site mental health specialists were unavailable, referrals were made to the nearest district-level psychiatric services, and follow-up was coordinated through the palliative care team and clinical staff to ensure patient safety. All interviews were conducted in Chichewa by research assistants who did not know the participants before the interviews. Before the interview, the study’s objectives were shared, and participants were asked to sign the consent form. Written informed consent was obtained from all participants before data collection. Interviews were conducted in a private setting to ensure confidentiality and participant comfort. All interviews lasted between 15 and 30 minutes. Participants provided a signed or thumbprint as consent.
Data analysis
Data was analysed using Stata version 18.0. Descriptive statistics were used to summarise participants’ characteristics, and results were presented as means with standard deviations for continuous variables and frequencies with percentages for categorical variables.
Depression and anxiety were analysed using ordinal outcome variables. For depression participants with scores from 0-4 were classified as having minimal or no depression, 5-9 mild depression, 10-14 moderate depression and 15+ severe/moderately severe depression. For anxiety, GAD-7 scores between 0-4 were classified as minimal anxiety, 5- 9 as mild anxiety, 10-14 as moderate anxiety and 15+ as severe anxiety. Multivariable ordered logistic regression models were used to examine associations between sociodemographic variables (age, sex, marital status, education, and religion) and clinical factors (PHQ-9 and GAD-7 scores) with depression and anxiety outcomes. Adjusted odds ratios (aORs) with 95% confidence intervals (CIs) were reported.
Model results were interpreted at a two-sided significance level of α = 0.05. No interaction terms were included in the final models, and multicollinearity was assessed before model estimation.
Results
Study population characteristics
Demographic characteristics of the study population.
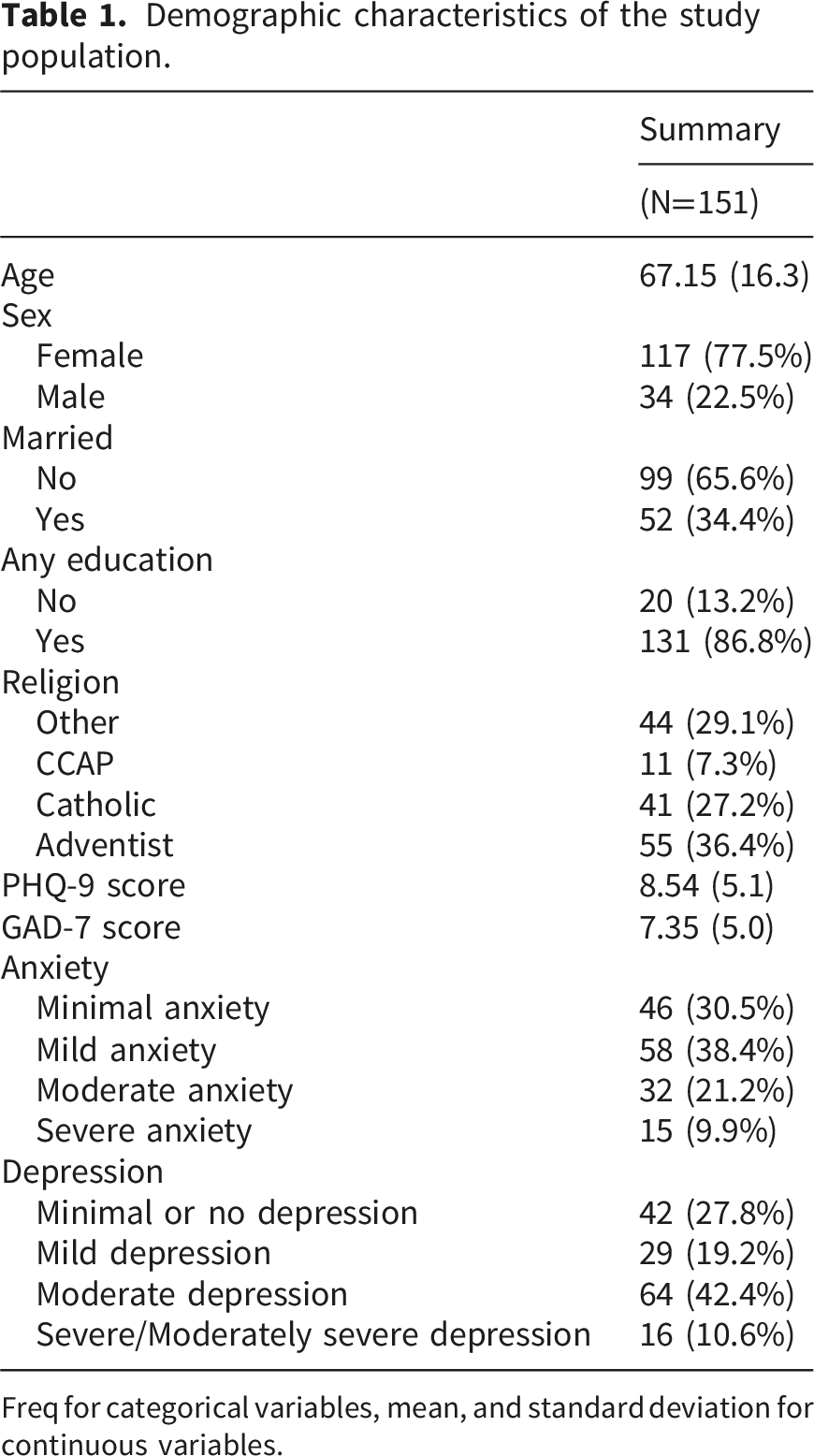
Freq for categorical variables, mean, and standard deviation for continuous variables.
Over 72% (95% CI: 65.0%–79.4%, n = 109) of participants had depression, with 19% screening for mild, 42% for moderate, 9% moderately severe, and 1% severe. About 70% (95% CI: 62.1%–77.0%, n = 105) of patients had anxiety, which ranged from mild to severe anxiety (38% mild, 21% moderate, and 10% severe forms). More details are displayed in Table 1 above. Among the 151 participants, 4 (3%) reported suicidal ideation (PHQ-9 item 9 score > 0). All participants were immediately referred to trained mental health personnel for further assessment and follow-up according to the study’s established referral protocol.
Figure 2 above displays the prevalence of depressive symptoms among patients under a palliative care program, revealing notable psychological distress within this vulnerable group. Specifically, 54% (n = 81) reported little interest or pleasure in activities, while 73% (n = 111) felt down, depressed, or hopeless. Sleep disturbances were also significant, with approximately 66% (n = 99) having trouble falling or staying asleep. Fatigue was prevalent among 71% (n = 108) of patients, and 73% (n = 106) reported feeling bad about themselves. Suicidal thoughts were present in about 3% (n = 4) of respondents. Prevalence of depressive symptoms.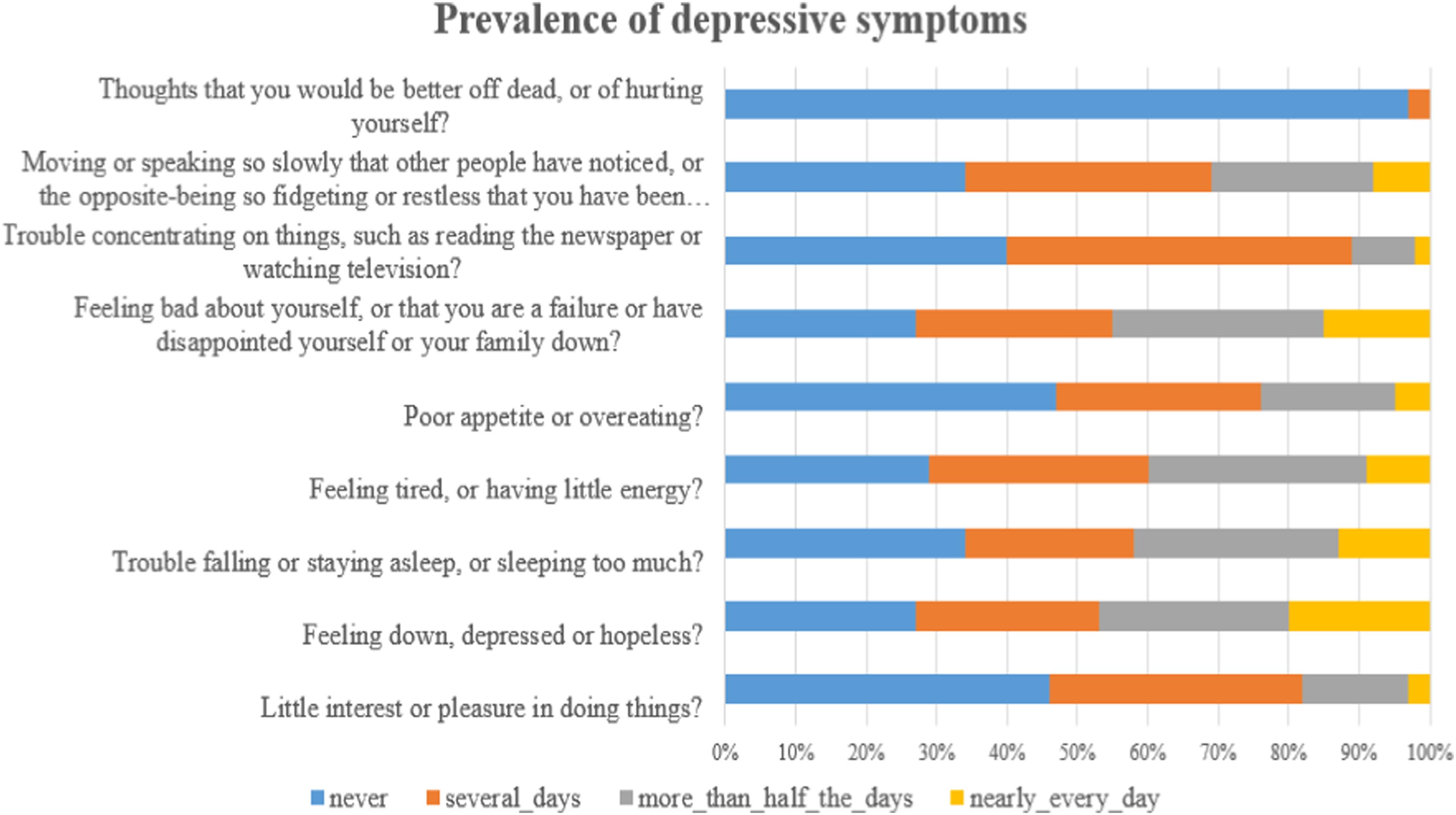
Figure 3 displays the prevalence of anxiety among patients under the palliative care program. Notably, 75 % (n = 112) reported feeling nervous, anxious, or on edge, and more than 70% (n = 105) experienced worrying too much about different things. Additionally, 76% (n = 115) said they were not able to stop or control worrying, and 70% (n = 106) experienced being so restless that it was hard to sit still. Prevalence of anxiety symptoms.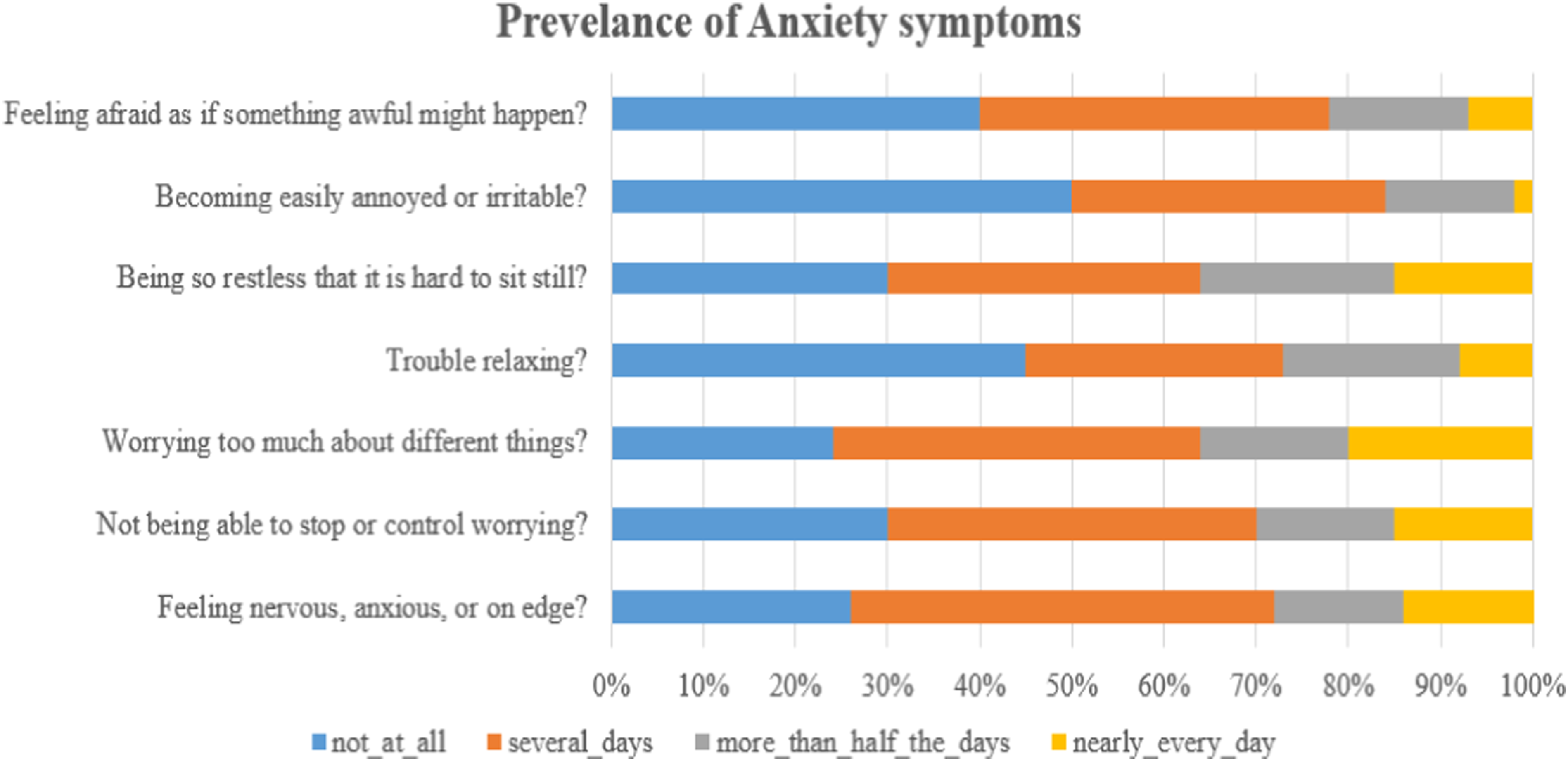
Factors associated with depression and anxiety
Depression model.
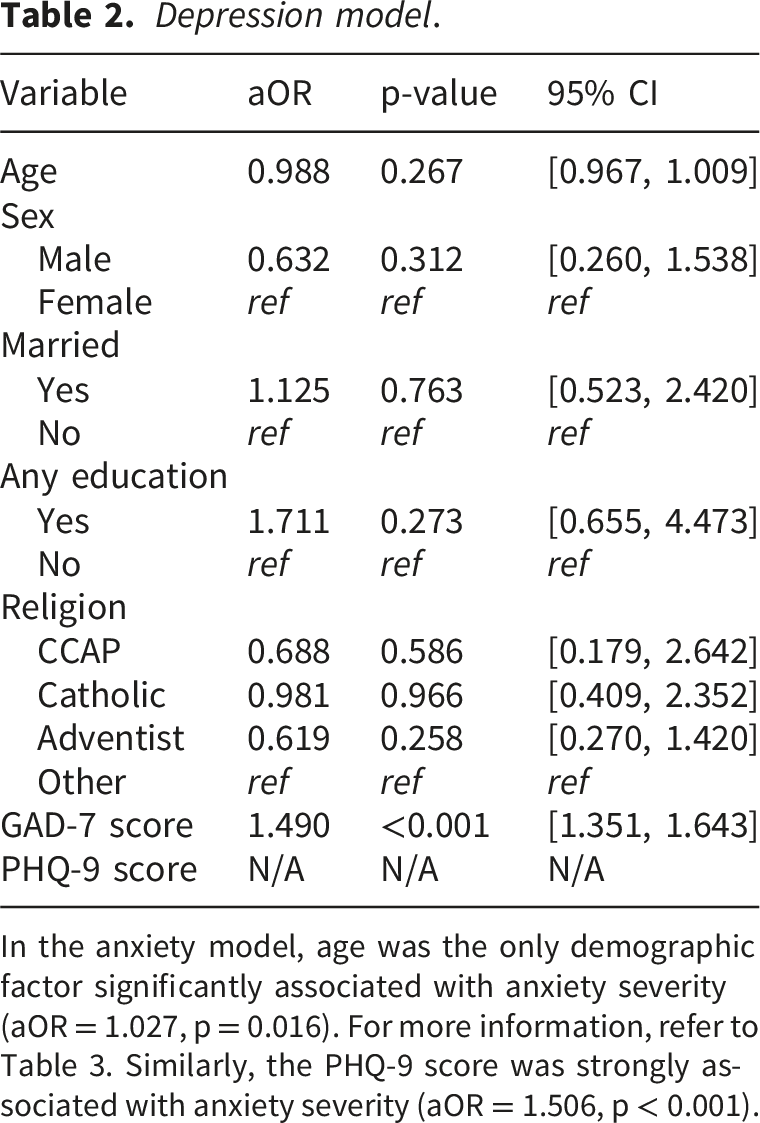
In the anxiety model, age was the only demographic factor significantly associated with anxiety severity (aOR = 1.027, p = 0.016). For more information, refer to Table 3. Similarly, the PHQ-9 score was strongly associated with anxiety severity (aOR = 1.506, p < 0.001).
Discussion
Anxiety model.
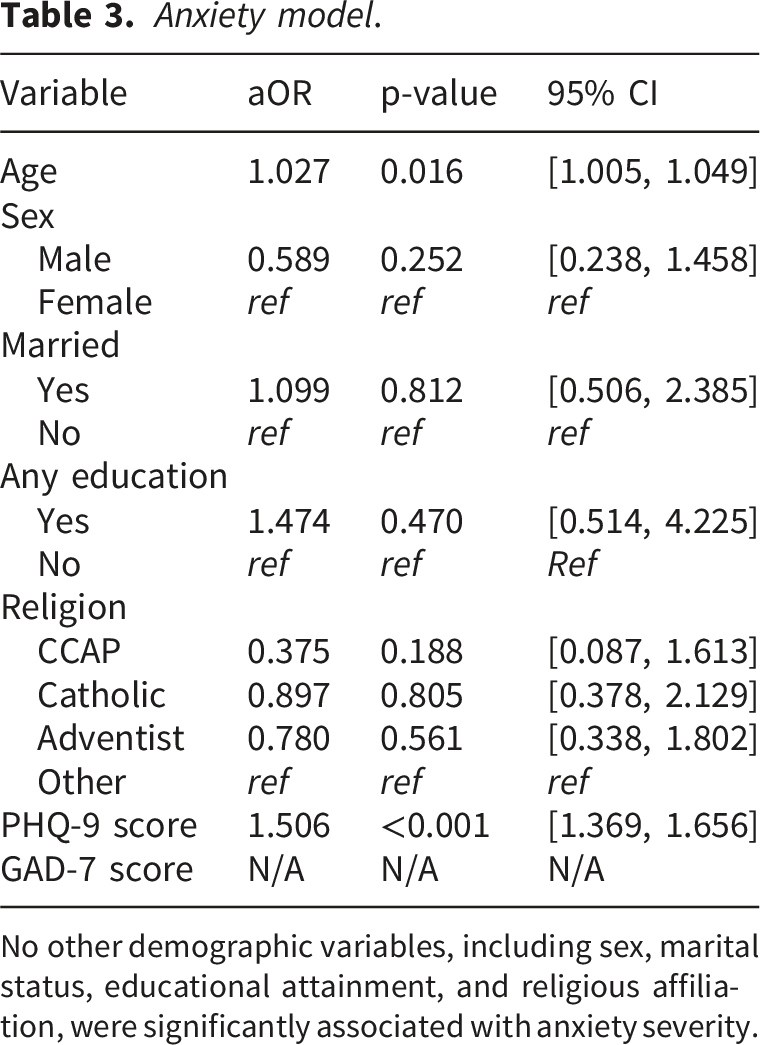
No other demographic variables, including sex, marital status, educational attainment, and religious affiliation, were significantly associated with anxiety severity.
The strong association between depressive and anxiety symptoms reflects the high degree of psychological comorbidity commonly observed in palliative care populations. In patients with advanced illness, these conditions often coexist as part of a broader syndrome of emotional distress driven by physical symptom burden, uncertainty about prognosis, and social and economic hardship. 5 In low-resource settings, these experiences may be intensified by poverty, limited access to care, and weak psychosocial support systems.12,13 For frontline health workers in resource-constrained settings, this overlap highlights the need for integrated approaches to psychological assessment and management rather than treating depression and anxiety as isolated clinical entities.
These findings support the integration of routine mental health screening within palliative care services, particularly in rural settings where specialist mental health services remain limited. Task-shifting approaches involving trained lay counsellors, community health workers, and primary care providers may strengthen early identification, psychosocial support, and referral for severe mental health conditions.24,25 Such approaches are particularly relevant in rural Malawi, where decentralised health systems often rely on non-specialist providers to deliver comprehensive chronic care services.
Older age was significantly associated with anxiety severity in this study. This association likely reflects the interaction between ageing, chronic illness, and structural vulnerability within rural communities. In districts such as Neno, where many households depend on subsistence livelihoods, older adults with advanced illness may experience heightened anxiety related to functional decline, dependency on caregivers, food insecurity, and financial instability.12,19 Social isolation and weakening family support systems may further exacerbate psychological distress among older patients, particularly where younger family members migrate for economic opportunities. These findings align with broader evidence demonstrating the influence of social determinants, including poverty, inequality, and limited social support, on mental health outcomes.11,13
The identification of suicidal ideation among 3% of participants, although relatively low, further underscores the importance of integrating mental health screening into palliative care services. Psychological distress among patients with life-limiting illness is associated with reduced quality of life, increased suffering, and greater caregiver burden.1,18 In rural and resource-constrained settings, strengthening referral pathways and integrating basic psychosocial support into decentralised palliative care services may improve early identification and management of severe psychological distress.
Limitations
Some limitations should be considered when interpreting these findings. First, the cross-sectional design limits causal inference between sociodemographic characteristics and mental health outcomes. Consequently, the temporal relationship between disease progression and psychological distress could not be established, warranting future longitudinal investigations. Second, although the PHQ-9 and GAD-7 are validated screening instruments, some items, such as fatigue, sleep disturbance, and reduced appetite, overlap with symptoms commonly associated with advanced chronic illness, potentially leading to overestimation of depression and anxiety prevalence among palliative care patients.
Third, although simple random sampling reduced selection bias by providing equal selection probability to all eligible participants, diagnosis-specific stratification was not performed. Therefore, variation in diagnosis categories within the sampled population may not fully reflect the broader program population. Fourth, despite the use of translated and locally validated tools, cultural interpretation and expression of psychological symptoms may have influenced participant responses. Finally, the study was conducted within a single rural district characterised by substantial socioeconomic and health system constraints, which may limit generalisability to urban or better-resourced settings within Malawi and similar contexts.
Despite these limitations, the study provides important evidence on the substantial burden of depression and anxiety among patients receiving palliative care in rural Malawi. It contributes to the limited literature on integrated mental health and palliative care in low-resource settings.
Conclusion
This study demonstrates a high burden of depressive and anxiety symptoms among patients receiving palliative care in rural Malawi, highlighting the substantial psychological distress experienced by individuals living with life-limiting illness. The strong association between depression and anxiety suggests significant psychological comorbidity, reinforcing the need for integrated approaches to mental health assessment and management within palliative care services. Older age was significantly associated with higher anxiety severity, underscoring the influence of structural vulnerabilities such as poverty, functional decline, dependency, and limited social support in rural settings.
The findings support the integration of routine mental health screening, psychosocial support, and strengthened referral pathways within decentralised palliative care programs. In resource-constrained settings where specialist mental health services remain limited, task-shifting approaches involving primary care providers, lay counsellors, and community health workers may strengthen early identification and management of psychological distress. Integrating mental health into palliative care is essential to improving person-centred care, quality of life, and overall well-being among patients with advanced illness in low-resource settings.
Supplemental material
Supplemental material - Prevalence and determinants of depression and anxiety among patients enrolled in palliative care: The Case of a palliative care program in Neno District, Malawi
Supplemental material for Prevalence and determinants of depression and anxiety among patients enrolled in palliative care: The Case of a palliative care program in Neno District, Malawi by Atupere S. Phiri, Kondwani Mpinga, Moses Banda Aron, Owen Mwale, Cecilia Needham, Judith Kanyema
Supplemental material
Supplemental material - Prevalence and determinants of depression and anxiety among patients enrolled in palliative care: The Case of a palliative care program in Neno District, Malawi
Supplemental material for Prevalence and determinants of depression and anxiety among patients enrolled in palliative care: The Case of a palliative care program in Neno District, Malawi by Atupere S. Phiri, Kondwani Mpinga, Moses Banda Aron, Owen Mwale, Cecilia Needham, Judith Kanyema
Footnotes
Acknowledgement
Special thanks to Malawi’s Ministry of Health and PIH colleagues: Dr. Enock Ndarama (the district health service director), Dr. Albert Chafunya, Dr. Christopher Banda, and Horacio Lucious (the Neno district palliative care coordinator) for their support during the fieldwork. And to all the study participants for their dedication. Thanks to the Neno District Health Office and PIH/APZU leadership for their support, the Palliative Care Team, the health centre in-charges, the research assistant, San N. Banda, and Stamper Chifenthe.
Ethical considerations
The study received ethical approval from the National Health Science Research Committee-Malawi, protocol # 24/02/4363: Assessing the Prevalence and factors associated with Depression and Anxiety in Palliative Care: The Case of Palliative Care Program in Neno District, dated 21st March 2024, and the Neno District Health Office, letter dated December 15, 2023, to conduct the study in the Neno District. Furthermore, the ethical principles in the Declaration of Helsinki were followed. 26 Participants were informed about the study aims and procedures through trained research assistants who read the information sheet aloud. The participants were given a unique identifier to protect their identity, and the study team conducted themselves with good clinical practice training.
Consent to participate
Participants provided consent by signing or thumbprinting the consent form, and witnesses were also asked to sign. The witnesses were present only during the consent signing process and were asked to move away during interviews to maximise participant privacy and confidentiality.
Author contributions
AP led the conceptualisation, methodology development, investigation, formal analysis, project administration, supervision, visualisation, and drafting of the original manuscript, as well as review and editing. KM contributed to methodology, investigation, formal analysis, software use, validation, visualisation, project administration, and manuscript review and editing. MAB contributed to methodology, formal analysis, supervision, validation, and manuscript review and editing. OSM contributed to formal analysis, project administration, and supervision. CDN contributed to manuscript review and editing. JSK, BDK, and PCK contributed to project administration and supervision, with BDK also contributing to manuscript review and editing. RM contributed to methodology, formal analysis, supervision, and manuscript review and editing. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was made possible with support from Atlas Corps under the Community Impact Fund ($1000), as part of the leadership project fund and human resource (research assistance) support from the IC3D project under capacity building. The funding sources were not involved in or interfered with the study design, data collection, analysis, or report writing.
Declaration of conflicting interests
The authors declare no potential conflicts of interest regarding the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the conclusions of this article are provided as additional files. Documents required to replicate this study are available from the corresponding author upon reasonable request.
Paper context
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.