
Abstract
Background
The subcutaneous (SC) route is used routinely in patients with advanced diseases requiring palliative care. Pre-prepared individual doses of medication stored in syringes may facilitate home administration for symptom management; however, there are limited data on the microbiological and physicochemical stability of such formulations.
Objectives
To assess the microbiological and physicochemical stability of the pre-prepared formulations stored in syringes for SC administration.
Design
Experimental study of the microbiological and physicochemical stability of pre-filled syringes during storage.
Methods
Standardised methods of medication preparation were followed for morphine, midazolam, metoclopramide, hyoscine butylbromide, levomepromazine, haloperidol, ondansetron, fentanyl, ketorolac and dexamethasone, as well as drug mixtures (morphine + midazolam and midazolam + levomepromazine). Microbiological stability of morphine, midazolam, metoclopramide, butylbromide and drug mixtures was analysed by culture on conventional media and monitoring growth over 14 days. A total of 200 syringes were analysed. Physicochemical stability was assessed using ultra-high-performance liquid chromatography with ultraviolet detection coupled to a mass spectrometer, pH measurement and visual macroscopic examination, with measurements taken at eight time points, of the formulations stored in capped polypropylene syringes in air-tight bags in the dark at room temperature (22±3°C) for 12 weeks.
Results
In the microbiological stability analysis, all cultures studied were negative. In the physicochemical stability analysis, the formulations studied retained at least 90% of the initial drug concentrations for 12 weeks, except in the case of metoclopramide (for 3 weeks) and showed no significant changes in pH or macroscopic signs of degradation.
Conclusion
Formulations aseptically prepared and stored in syringes are microbiologically and physicochemically stable for 12 weeks in the cases of almost all drugs studied, the exception being metoclopramide (which was stable up to week 3). These findings suggest that such formulations show stability characteristics consistent with suitability for SC administration of drugs in palliative home care.
Plain language summary
What is this study about? People with advanced illness who receive palliative care often need medicines given under the skin to control symptoms such as pain, anxiety, nausea, or breathlessness. Preparing these medicines in advance and storing them in syringes could make treatment at home easier for patients and caregivers. However, it is important to know whether these medicines remain safe and effective when stored this way. What did we do? We prepared several commonly used palliative care medicines, both alone and in certain combinations, following standard sterile procedures. These medicines were stored in plastic syringes, protected from light, at room temperature, for up to 12 weeks. We regularly tested the syringes to check two things: 1. whether any bacteria or other microorganisms grew in the medicines, and 2. whether the medicines kept their chemical strength, appearance, and acidity over time. What did we find? No bacteria or other microorganisms were found in any of the stored syringes. Most medicines kept at least 90% of their original strength for the full 12 weeks and showed no visible changes or signs of damage. One medicine, metoclopramide, remained stable for a shorter period of up to 3 weeks. Why is this important? These results show that most of the medicines studied can be safely prepared in advance and stored in syringes for several weeks. This approach may help simplify symptom control at home for people receiving palliative care, reducing the need for frequent preparation and supporting safer, more convenient treatment outside the hospital.
Keywords
Introduction
The subcutaneous (SC) route of administration is widely used in patients with advanced diseases requiring palliative care, especially in the home setting. It is routinely used in specialised palliative care, hospital-at-home, and primary care services. This route allows medications to be administered by continuous infusion, on-demand, or both approaches concomitantly, according to each patient’s needs. 1 SC administration is used when the oral route is compromised or to achieve good symptom control when oral treatment has not been effective.
The use of subcutaneous administration by non-professional carers can cause them anxiety due to a fear of making a mistake, of giving the patient an overdose, or of local reactions that may occur at the injection site.2,3 However, the ability of carers to manage symptoms correctly at home has also been documented4,5 with good results in terms of symptom control and high levels of satisfaction6–10 and the potential complications tend to be rare and not serious.5,8,9,11
Understanding the stability of the prepared medication could help to make it easier to administer, reduce anxiety and difficulties for carers when using the subcutaneous route, and thus contribute to improving palliative care at home.
SC medications can be administered continuously using an infusion pump or intermittently as rescue therapy to treat symptoms such as pain, dyspnoea, nausea, vomiting, agitation, delirium, and insomnia.1,5,8,11,12 Rescue or breakthrough doses are administered as needed by the patient, rather than following a fixed schedule.
In some services, caregivers are given drugs in vials, and they prepare formulations and fill syringes at home as needed. 13 In other services, including the Hospital-at-Home Service at Donostia University Hospital, formulations are prepared in advance and stored in syringes by health professionals with doses tailored for each patient.5,8,9,14 The pre-preparation of medications by health professionals may facilitate symptom management and control, as well as encourage the involvement of more caregivers who might otherwise refuse to manage symptoms at home. 15
Notably, however, the question of the microbiological and physicochemical stability of these pre-prepared formulations stored in syringes has not been fully clarified by research to date. Several authors have conducted studies on drug physicochemical stability and found that some drugs and drug mixtures remain stable for periods of several weeks, 3 months, 6 months and even up to 1 year,16–20 but these studies have involved various concentrations of drugs stored under different conditions. 18 Furthermore, the study objectives have not focused on home-based palliative care and drug preparation methods have differed from those we usually use.21,22 In some cases, unlike in our service, the formulations were prepared under strict sterile conditions,22–25 or frozen and subsequently thawed, 21 while in others, they were based on drug concentrations or mixtures not used in our routine practice,21,22,24,26,27 or they were stored in bags or large vials rather than in syringes.21,22,28 Overall, the heterogeneous nature of studies reported reflects the reality that different centres currently adopt notably different approaches, and a current lack of guidelines or even consensus on preparation and storage of medications for home care. On the other hand, most previous studies have focused on physicochemical stability,16–18,21,22,29 without addressing microbiological stability or potential microbiological contamination of the formulations and have not cultured samples.
Given all this, the objective of this study was to assess the physicochemical and microbiological stability of pre-prepared formulations stored in syringes for SC administration and used for controlling symptoms.
Material and methods
Sample preparation
In this study, the drug formulations were prepared using a standardised procedure and stored in syringes by hospital-at-home nurses in the service’s medication preparation room at Donostia University Hospital, following the usual procedure detailed in Appendix 1.
Drugs analysed. Composition, concentration and formulation preparation.
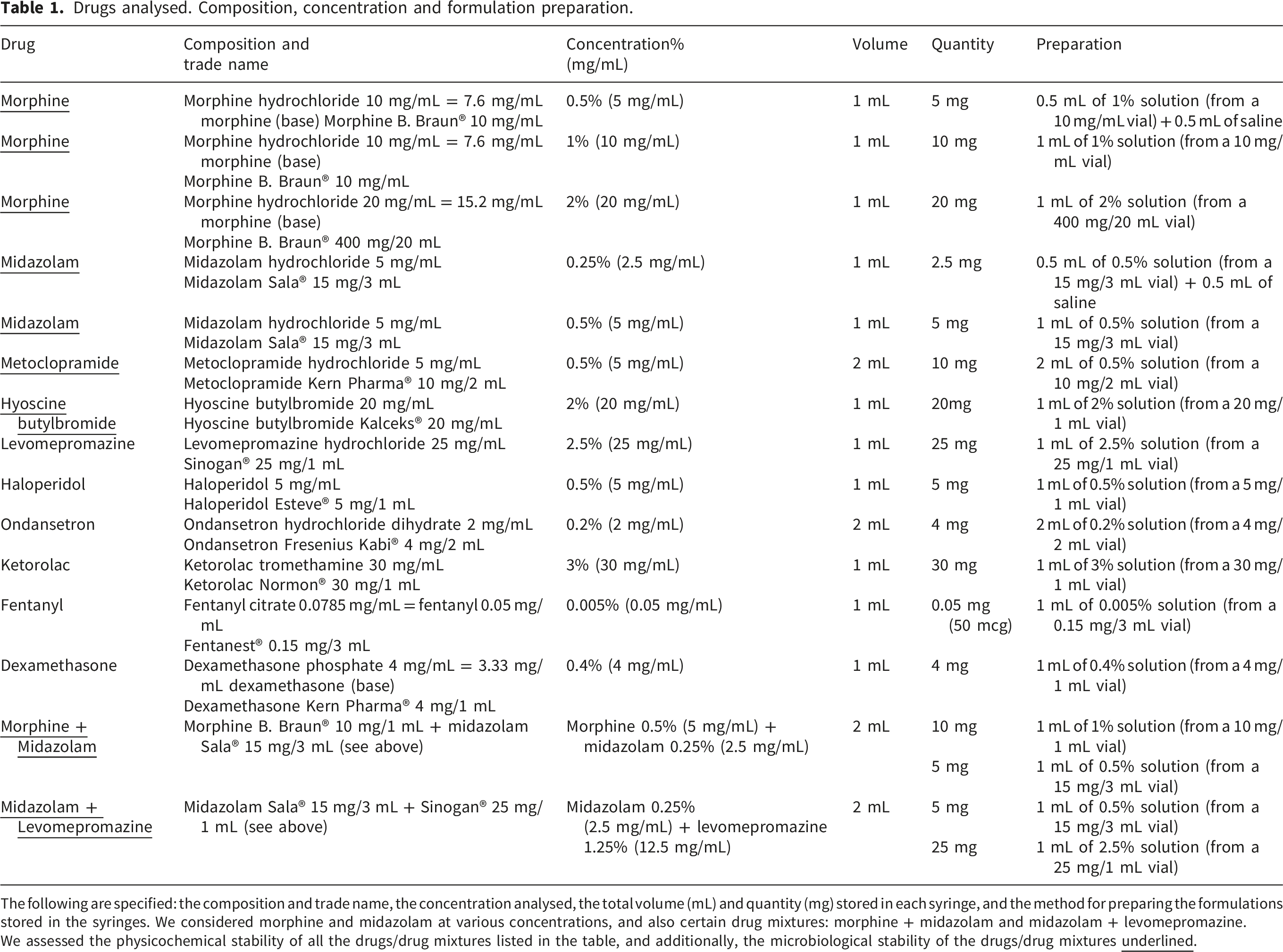
The following are specified: the composition and trade name, the concentration analysed, the total volume (mL) and quantity (mg) stored in each syringe, and the method for preparing the formulations stored in the syringes. We considered morphine and midazolam at various concentrations, and also certain drug mixtures: morphine + midazolam and midazolam + levomepromazine.
We assessed the physicochemical stability of all the drugs/drug mixtures listed in the table, and additionally, the microbiological stability of the drugs/drug mixtures
All formulations were stored in a closed cabinet protected from light in an office environment (not a laboratory), where temperature and humidity conditions are not controlled and reflect normal environmental conditions. The variations in temperature and humidity that have been recorded are the result of daily fluctuations in temperature and humidity and of changes over the course of the study months, with the aim of ensuring that storage conditions were as similar as possible to those in a domestic setting.
Material used for sample preparation (Figure 1): - 2 mL and 10 mL Omnifix® Luer Solo (Braun) syringes. Materials used for sample preparation: (a) Preparation material (b) Material on sterile drape (c) Distribution of samples into 2 ml syringes after performing the desired dilution (d) Final result with labelled syringes, capped and in labelled airtight bags ready for storage.

Syringe barrel and plunger are made of polypropylene. The plunger stopper with double sealing ring is made of polyisoprene. Manufactured according to ISO 7886-1. Not manufactured with Polyvinylchloride (PVC), Bisphenol A (BPA), Diethylhexylphthalate (DEHP) and Latex. - Combi-Stopper® caps (Braun).
Made of Polyethylene. - Unidix® three-way stopcock - Excellent Medical Technology Group® sterile drape - Deltalab® zip-lock bags
Design
Experimental study of the microbiological and physicochemical stability of pre-filled syringes during storage.
Analysis of microbiological stability
Formulations assessed in the microbiological stability analysis. Number of samples and composition.

In this analysis, a smaller range of formulations was studied than in the physicochemical stability analysis. Specifically, we focused on the formulations used most often in our area, and by considering various concentrations and dilutions, with and without saline.
Twenty samples were prepared each day for 10 days by four different hospital-at-home nurses. The twenty daily samples represented different types of medication, ensuring that all nurses worked with all the medicines under study, in order to avoid any potential individual bias in the handling of the samples. The recommendations of the Spanish Society of Infectious Diseases and Clinical Microbiology (SEIMC) were followed for the processing and analysis of samples. 30
After preparation, samples were immediately transported at room temperature. On receipt at the laboratory, direct inoculation was performed, transferring the formulations to be studied directly onto the culture medium.
The culture media used were thioglycolate broth, for the growth of aerobic and anaerobic bacteria, and casein-soybean broth (TSB), for aerobic bacteria and fungi. These types of culture were incubated at 30–35°C and 20–25°C, respectively, for 14 days (in both cases).
The cultures were examined daily up to day 14, applying the following criteria:30–32 • If turbidity was observed in the culture medium, a subculture was performed in solid media (chocolate, blood, Schaedler and Sabouraud agar) for 72 hours. Any bacteria and/or fungi that grew in these subcultures were identified to species level using matrix-assisted laser desorption/ionisation time-of-flight mass spectrometry (MALDI-TOF-MS). In such cases, the samples would not be considered sterile and would be reported as positive. • If no turbidity was observed in the culture medium, samples were considered sterile and reported as negative. • Materials: o Thioglycolate Broth (Biomérieux S.A., Ref: 42074, 9ml tubes) o Tryptone Soya Broth (ThermoFisher Diagnostics S.L.U, Ref: TV5002E, 10ml tubes) o Incubator: Heraeus B6420
The microbiological stability study was conducted throughout February 2024.
Analysis of physicochemical stability
The physicochemical stability of the samples was analysed at the CIC BiomaGUNE research centre in Donostia-San Sebastian.
All samples for physicochemical stability testing were prepared simultaneously at the start of the study, T0, in accordance with the methods used for sample preparation and storage described in Appendix 1. All formulations were stored in a closed cupboard, protected from light, in an office environment (not a laboratory), where temperature and humidity conditions are not controlled and reflect normal environmental conditions. By using these storage conditions, we have sought to replicate home storage conditions as closely as possible. Stability was evaluated by comparing the sample concentration to the control and the relative concentrations calculated in comparison with day 0 (T0).
Formulations were assessed sequentially using ultra-high-performance liquid chromatography (UPLC) with ultraviolet and mass spectrometry detection to provide appropriate data for quantitative and qualitative analysis. For each type of drug, in some cases considering different concentrations and drug mixtures (Table 1), serial studies were performed at baseline (T0) (the day on which all the formulations were prepared and stored in syringes), and subsequently, at weeks 1, 2, 3, 4, 6, 8 and 12 (T1, T2, T3, T4, T5, T6 and T7, respectively). At each time point, six independent replicates of each formulation were prepared to assess the reproducibility between samples.
Calibration curves were prepared independently at each sampling time point to ensure the reliability and stability of the quantitative response throughout the study.
In addition, for each of the samples at each time point, the pH was measured, and the sample was visually examined to check for turbidity, colour changes and the formation of precipitates.
The samples were considered to be physicochemically stable when they retained at least 90% of the initial drug concentration.19,21,23,25,33 In this study, we also wanted to measure whether the formulations were stable enough to retain 95% of the initial drug concentration. • Chemicals and reactants
Solvents and additives for chromatography: acetonitrile, water, and formic acid (Fisher Optima Grade, Thermo Fisher Scientific Inc., Waltham, MA, USA).
Standards: supplied by Donostia University Hospital’s Pharmacy Department (Table 1).
Chromatography column: 1.7 μm particle Acquity UPLC BEH C18 (2.1 mm x 50 mm; Waters, Milford, MA, USA). • Equipment for UPLC with ultraviolet and mass spectrometry detection
All chromatographic separations were performed using an Acquity Premier UPLC system (Waters). This system is equipped with a UV diode array detector lamp and coupled to a LCT Premier XE mass spectrometer, featuring an electrospray source and a high-resolution time-of-flight analyser. The acquisition and processing of chromatographic data were performed using the MassLynx 4.1 software (Waters). • Analysis of the pH
The pH was measured using an Oakton pH 510 Series pH meter equipped with an XS Sensor electrode (Oakton Instruments, IL, USA), which was calibrated prior to the measurements using reference buffers (at pH 2, 7, and 10). The pH values of each formulation and at each time point were measured using the six replicates available for each time point. • Temperature and humidity monitoring
The temperature and relative humidity in the sample storage room were measured with a calibrated Testo 175 H1 meter (Titisee-Neustadt, Germany). • Visual examination
Visual macroscopic examination of samples was conducted at each time point to check for the formation of precipitates, colour changes or turbidity.
The physicochemical stability study was conducted from 9 April to 2 July 2024.
Statistical analyses
For contamination assessment, the sample size calculation was performed using the GRANMO sample size calculator version 8.0. 34 Contamination of less than 1% of samples was considered acceptable. Under similar situations, up to 16% of samples have been found to be contaminated. 35 Using GRANMO, it was estimated that 50 samples would be sufficient to detect statistically significant differences with a power of 80% and a significance level of 5% in a one-tailed test. Accordingly, we analysed 50 samples in each group, yielding a total of 200 samples.
For the physicochemical stability analysis, sample size was calculated using GRANMO. It was estimated that six samples of each formulation at each time point were required to be able to detect a difference in concentration of 5% or more, 28 assuming a standard deviation of 3%, and considering a power of 80%, significance level of 5% in a two-tailed test, and a loss to follow-up of 0%. We assessed whether the mean concentration was significantly lower than 90% or 95% of the initial value, for each formulation and at each time point (T0, T1…T7). Statistical analyses were performed using one-tailed Student’s t-test or the Wilcoxon signed-rank test, depending on the normality of the data. An alpha level of 5% was considered statistically significant. All analyses were conducted using R statistical open-source software, version 4.4.3. 36
Results
Microbiological stability
No microbiological growth was observed from any of the 200 samples analysed, indicating microbiological stability.
Physicochemical stability
Physicochemical stability results for formulations analysed without drug mixtures applying a concentration cut-off of >90% and >95%. Values represent mean drug concentration (% relative to T0) at each time point with standard deviations. Cells with bold text indicate statistically significant changes from the predefined stability limits.
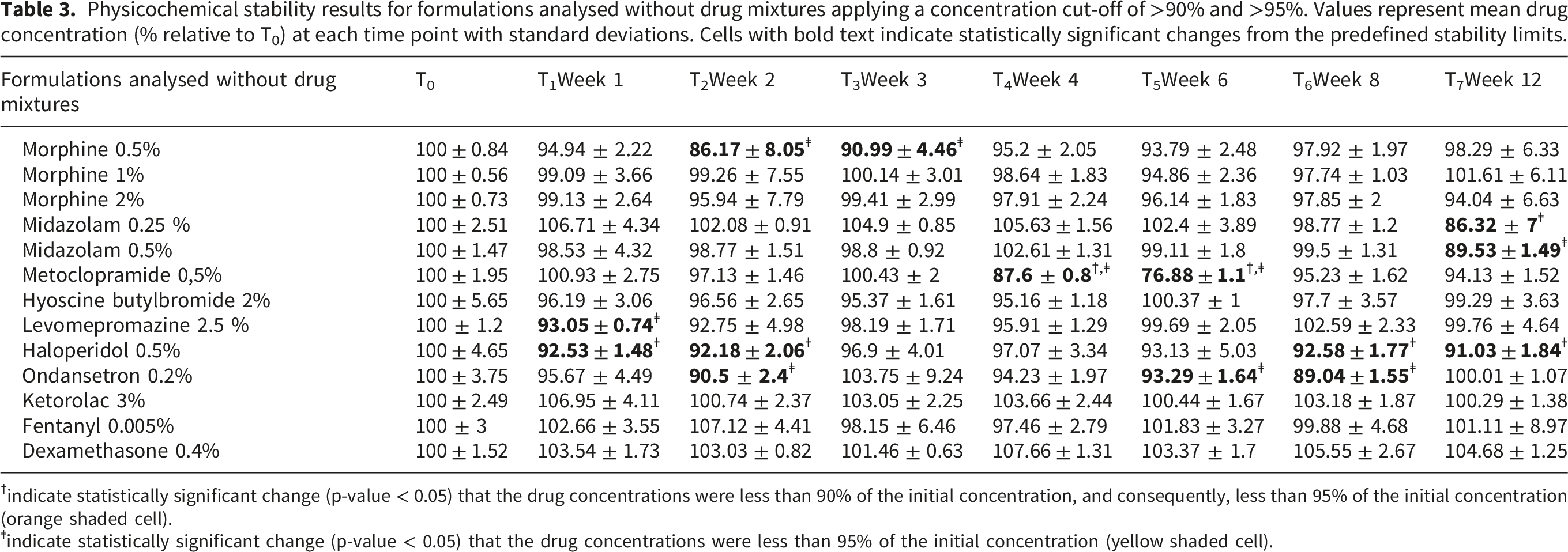
†indicate statistically significant change (p-value < 0.05) that the drug concentrations were less than 90% of the initial concentration, and consequently, less than 95% of the initial concentration (orange shaded cell).
ǂindicate statistically significant change (p-value < 0.05) that the drug concentrations were less than 95% of the initial concentration (yellow shaded cell).
Physicochemical stability results for formulations analysed with drug mixtures applying a concentration cut-off of >90% and >95%. Values represent mean drug concentration (% relative to T0) at each time point with standard deviations. For each row, results correspond to the
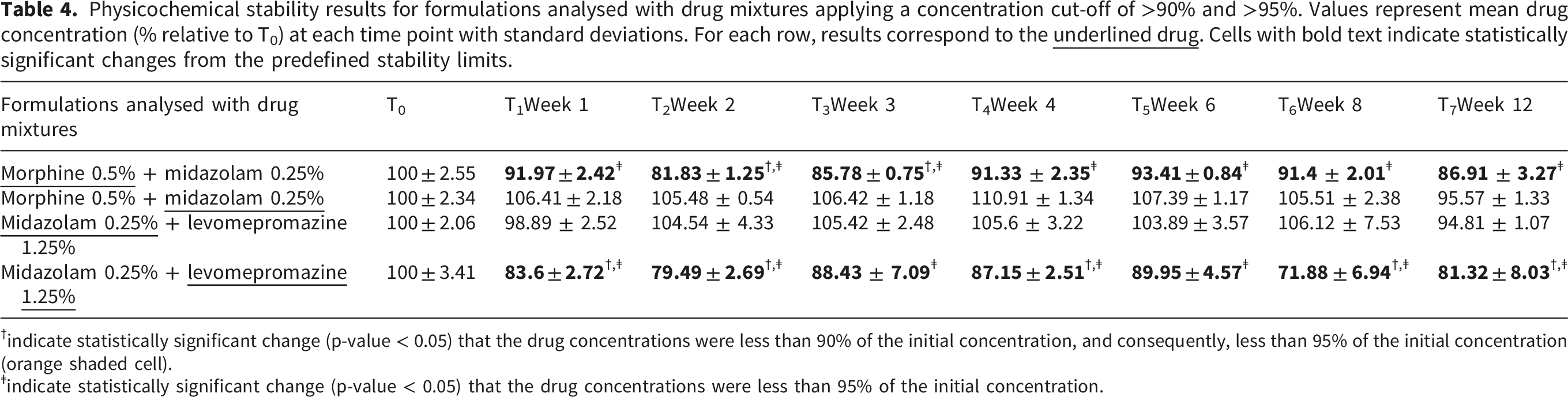
†indicate statistically significant change (p-value < 0.05) that the drug concentrations were less than 90% of the initial concentration, and consequently, less than 95% of the initial concentration (orange shaded cell).
ǂindicate statistically significant change (p-value < 0.05) that the drug concentrations were less than 95% of the initial concentration.
The analytical method showed excellent linearity over the studied concentration range, with correlation coefficients (R2) consistently exceeding 0.996 (see regression curves in Apendix 2).
The results indicated that all the formulations analysed remain stable for 12 weeks, retaining >90% of the initial concentration (see Figure 2). Measurements of metoclopramide found concentrations below 90% of the initial value at weeks 4 and 6 of the study, but over 90% in the samples analysed at weeks 8 and 12. Concentrations in each formulation without drug mixtures during the 12-week study period. At each sampling point, mean drug concentrations relative to T0 and their corresponding error bars, representing the standard errors, are shown. The red shaded areas indicate the ±10% and ±5% physicochemical stability limits relative to T0. Dashed horizontal lines mark these boundaries.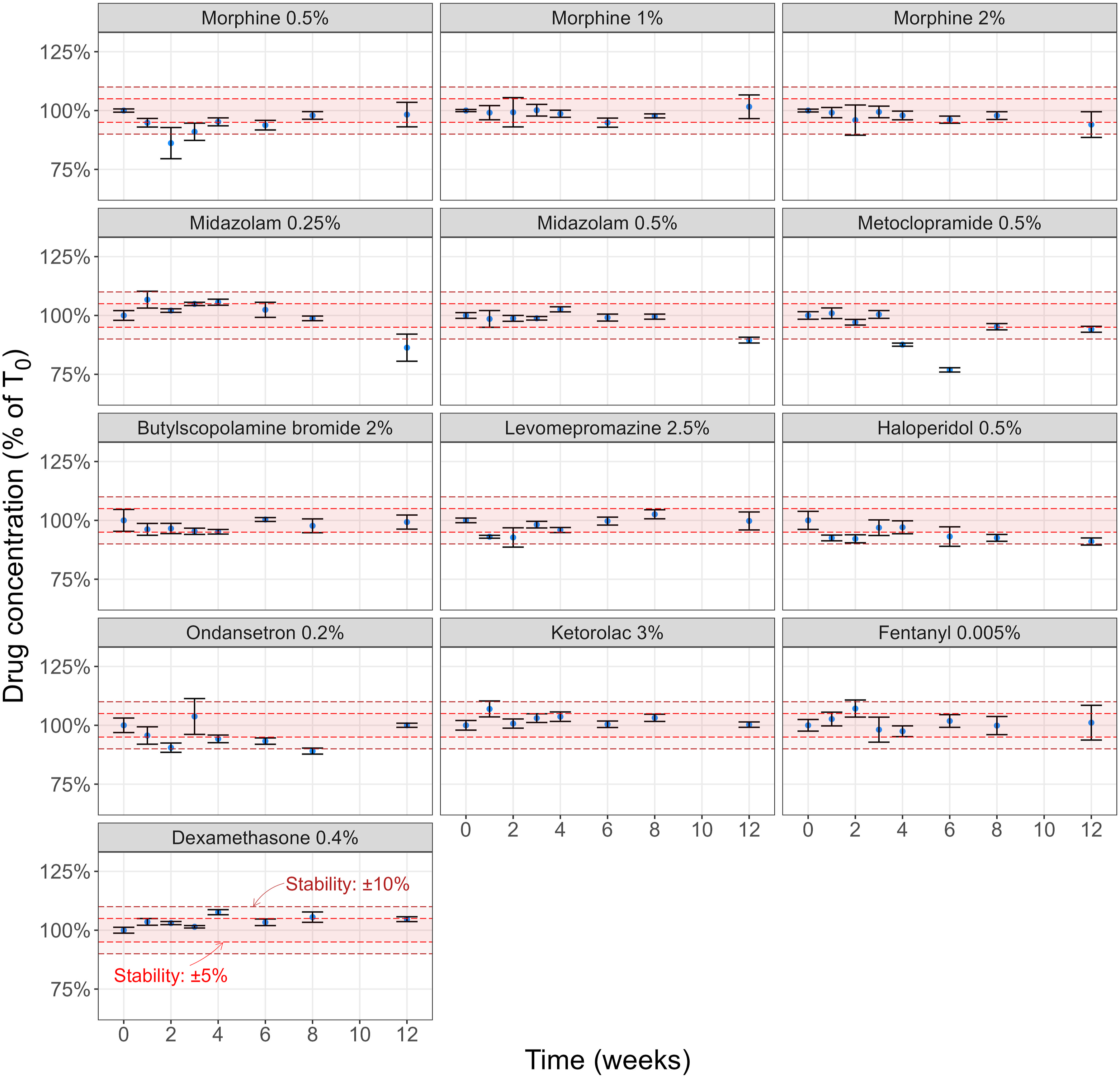
The drug mixtures were found to be more unstable, with concentrations falling below 90% of the initial values from the first week in the case of midazolam + levomepromazine and from the second week in the case of morphine + midazolam (see Figure 3). Concentrations in each drug mixture during the 12-week study period. At each sampling point, mean drug concentrations relative to T0 and their corresponding error bars, representing the standard errors, are shown. The red shaded areas indicate the ±10% and ±5% physicochemical stability limits relative to T0. Dashed horizontal lines mark these boundaries.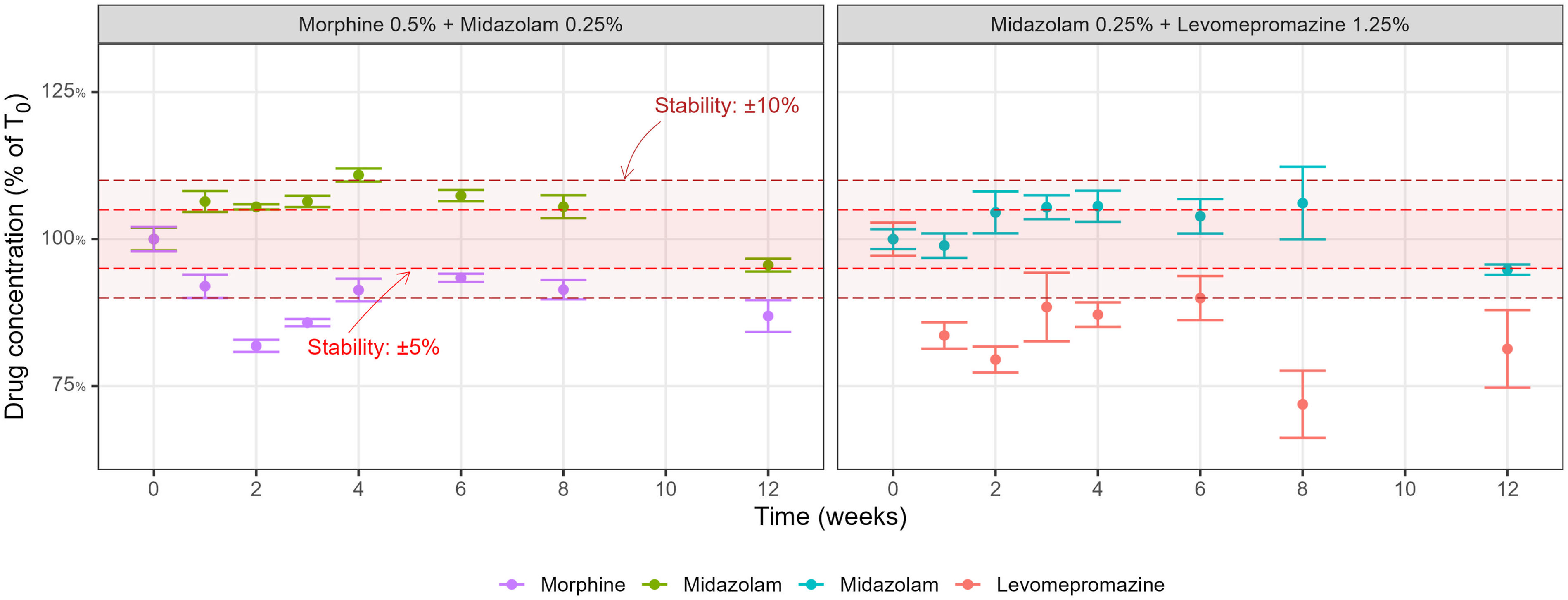
Most of the formulations analysed showed stability over the 12-week study period, retaining >95% of the initial drug concentration (morphine 1%, morphine 2%, hyoscine butylbromide, ketorolac, fentanyl and dexamethasone). For some formulations, drug concentrations fell to less than 95% of the initial value at some points, but returned to values indicative of stability later in the study (morphine 0.5%, metoclopramide, levomepromazine, haloperidol, ondansetron). Midazolam showed stability (retaining 95% of the T0 concentration) up to week 8.
In contrast, in the drug mixtures (morphine + midazolam and midazolam + levomepromazine), drug concentrations did not stay above the 95% cut-off after the first week.
Appendix 2 provides the complete report of the physicochemical stability analysis, including all six measurements for each formulation at each time point, calibration curves and graphs of all the data.
pH values of the formulations during the study period.
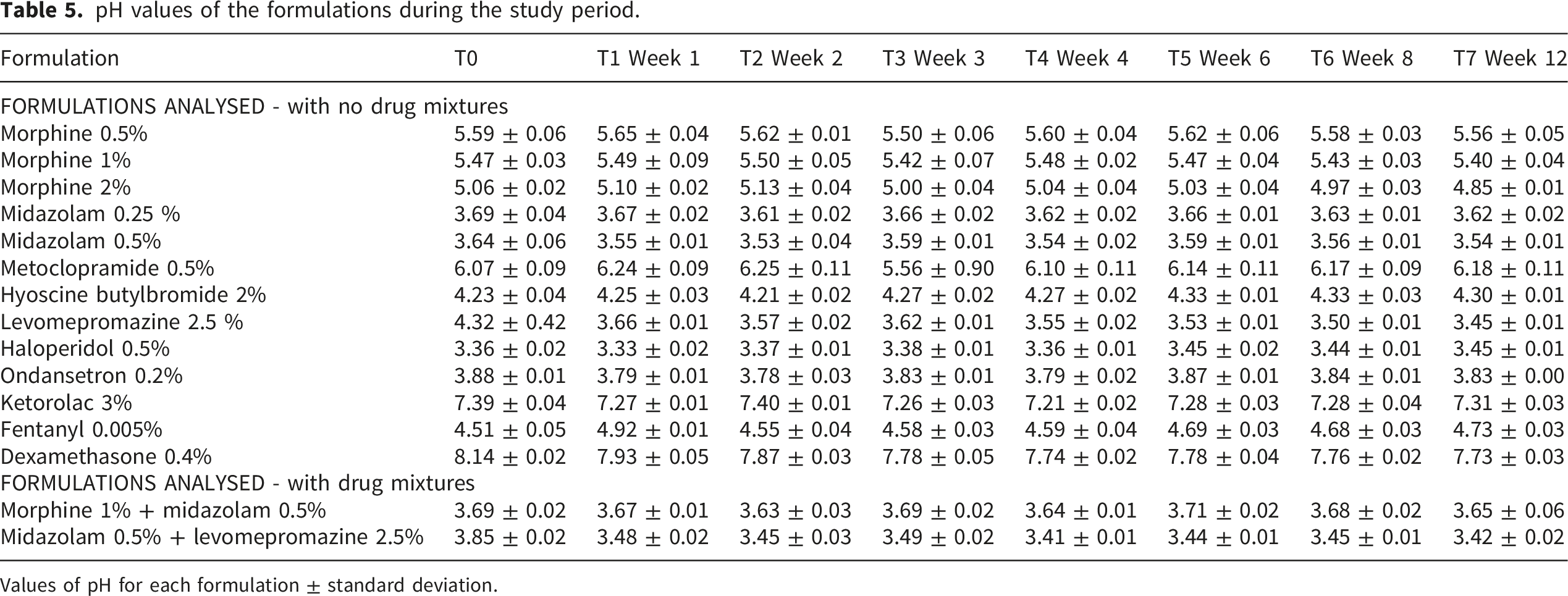
Values of pH for each formulation ± standard deviation.
The pH of all the formulations remained stable over the study period, varying by less than one unit. Temperature and humidity in the storage room during the study period.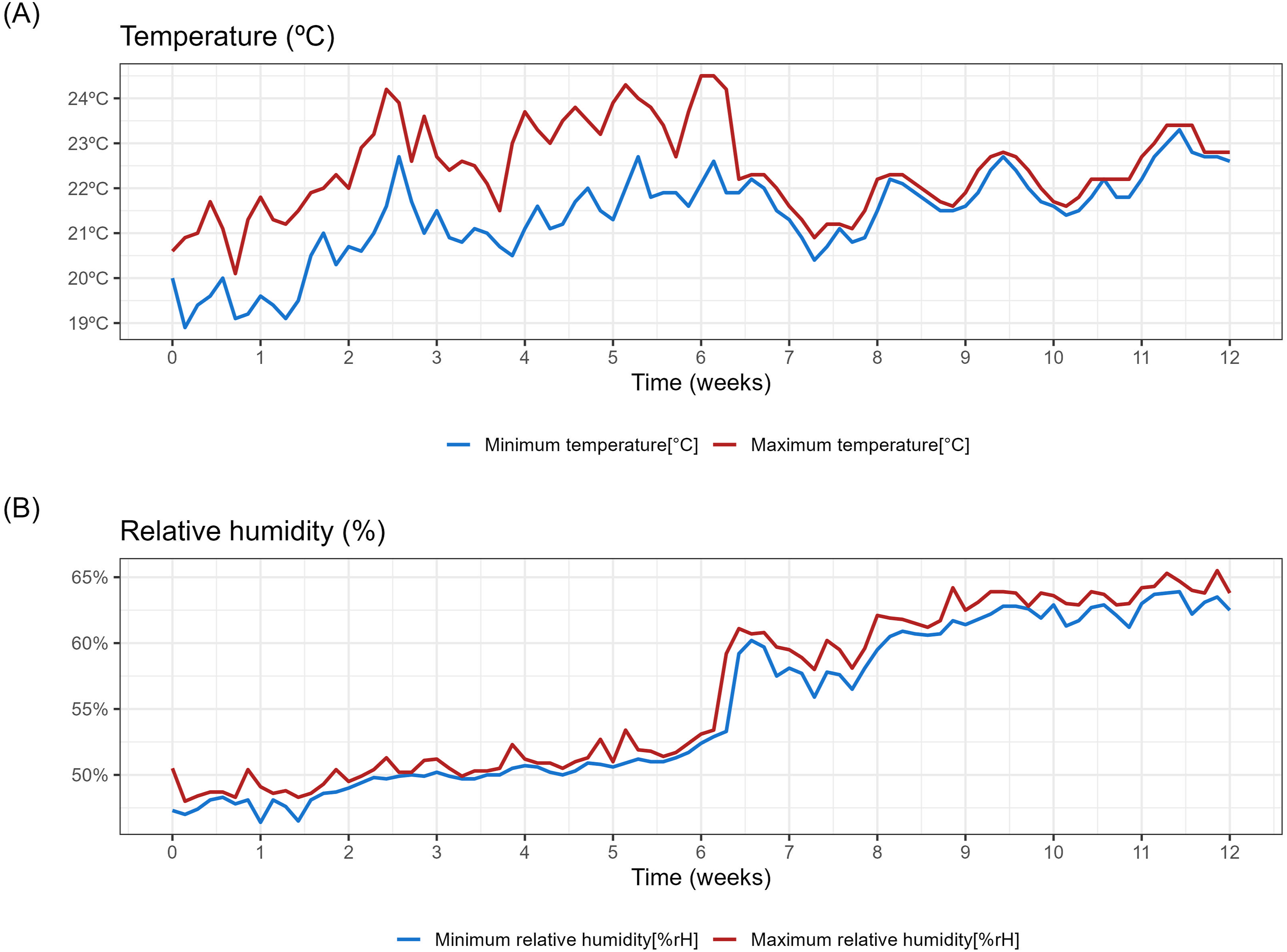
During the study, the temperature remained stable between 19.9°C and 24.2°C. The relative humidity ranged from 46.4% to 65.9%. (Figure 4). The temperature and humidity log data have been included in Appendix 3.
The macroscopic examination of samples did not detect changes in turbidity or colour, or the formation of precipitates during the entire study period.
Discussion
For routine clinical practice in home-based palliative care, it is important to know the stability of pre-prepared drug formulations stored in syringes for subsequent SC administration. To our knowledge, no previous studies have investigated the stability of medications kept in syringes under routine clinical practice conditions. We assessed the microbiological and physicochemical stability of drug formulations prepared and stored in syringes using doses commonly administered, following a specific preparation and storage protocol, which may be useful to many professionals. The protocol we studied is easily reproducible, polypropylene syringes are widely used, and the medicines we propose cover a wide range of drugs useful in palliative care. These stability data may prove valuable for improving palliative home care provided by both specific palliative care services and primary care teams.
Various factors explain the design of our standardised protocol for medication preparation. We use single-dose syringes in order that each syringe is only manipulated once. They are stored with a cap and in an airtight bag seeking to minimise degradation and reduce the risk of evaporation or liquid leakage. 16 Medications have been stored in a dark place and at room temperature, because light exposure may cause certain drugs to degrade faster and lower temperatures may trigger faster precipitation of some chemicals.17,18,37 Although a range of different medications are used subcutaneously, 38 we used the same protocol for formulation preparation and storage in all cases. On the other hand, various dilutions were analysed for morphine and midazolam to cover a wide range of concentrations used in daily practice.
In this study, drug stability was analysed up to 12 weeks. Compared to the duration of care, this is a relatively long period for many patients requiring SC treatments, but data for this length of time may be useful for more stable patients.
Microbiological stability
A selection of the medications has been analysed at different concentrations and in various forms of preparation and we did not find any contaminated samples among the 200 samples analysed. This finding suggests that both the procedure and the drug preparation practices we propose are appropriate, and that the prepared formulations remain microbiologically sterile. There are no standard guidelines or recommendations on the microbiological monitoring of this type of activity. In this context, it seems a good idea to implement a local surveillance programme with regular monitoring to ensure the correct functioning of the procedure.
Physicochemical stability
In the physicochemical stability analysis, all formulations retained >90% of the initial drug concentrations up to week 12, except for metoclopramide (only up to week 3). When requiring >95% of the expected initial values, we observed stability except in the cases of morphine 0.5% (2 weeks), midazolam 0.25 and 0.5% (8 weeks), metoclopramide (3 weeks), levomepromazine (1 week), haloperidol (1 week) and ondansetron (2 weeks).
Among our findings, several drugs showed non-monotonic fluctuations despite using six samples per formulation per time point. At the >95% cutoff, morphine 0.5% was statistically less than 95% at T2 and T3 while later measurements were more than 95%, deviating from typical degradation. Similarly, levomepromazine and haloperidol dipped at T1, and ondansetron at T2, respectively, with concentrations >95% in subsequent measurements.
A dexamethasone concentration reached 108% of expected. This could theoretically result from evaporation, which would concentrate the drug and potentially mask underlying degradation. However, if evaporation had occurred, similar trends would be expected in other formulations and at later time points, which was not observed. Although dexamethasone exceeded 100% at almost all time points, this exceedance was not statistically significant, as it did not surpass the upper 90% or 95% confidence intervals. We therefore attribute this to analytical variability rather than evaporation.
In addition, the results of metoclopramide warrant discussion. Concentrations appeared lower at 4 and 6 weeks, but above 90% and 95% of initial values at 8 and 12 weeks. However, given that different syringes were used at each time point, the low variability observed between the concentrations at these time points (SD 0.8 and SD 1.1), and the fact that this pattern was not observed at other time points or with other medicines, this pattern likely reflects analytical inaccuracy (e.g., calibration error). Previous studies report metoclopramide stability –defined as maintenance of more than 90% of the initial concentration– lasting less than 3 weeks,27,39 while in others, very similar to ours, stability was observed for up to 60 days. 40 Overall, these findings require further investigation to clarify the patterns observed.
On the other hand, we observed greater instability in the drug mixtures (morphine + midazolam and midazolam + levomepromazine), at both >90% and >95% cutoffs, as expected from previous research indicating that mixing medications shortens the stability of some drugs.16,33,41,42 In clinical practice, we use drug mixtures in patients who have previously received both components, usually patients with advanced or unstable conditions or in end-of-life care, who are visited frequently, providing opportunities to replenish medication supplies.
Regarding the analysis of pH, values remained stable, varying by less than one unit. Large changes in pH may accelerate drug degradation and compromise its stability. 43
Limitations
We acknowledge several limitations in this study. First, our analyses included microbiological stability, UPLC-UV-MS chromatography, macroscopic inspection, and pH measurements; however, the most exhaustive stability studies also incorporate osmolarity, particulate, and viscosity assessments.
Second, although the same analytical instrument and the same protocol for the preparation of samples and calibration standards were used throughout the study, the measurements were performed in different analytical batches and new calibration curves were generated for each time point. This may introduce additional variability in the results, which should be taken into account.
Third, our protocol was not compared with alternative protocols or different types of syringes and containers. The study only included medicines routinely used in our department, and although analyses were carried out in an independent laboratory, the selection of formulations and time points was based on our local clinical practice and experience. Although we did not find similar protocols in the literature for comparison, all these factors may introduce confirmation bias and limit the generalizability.
Fourth, the prepared formulations were stored in syringes at room temperature, not refrigerated. Therefore, our data cannot be compared with results based on other types of storage. Such information would be useful, as cold storage, if associated with better stability, could be easily recommended for home settings.
Fifth, the exclusion of some of the formulations from the Microbiological stability section might be regarded as a limitation of this part of the study. Some studied drugs have reported bacteriostatic or antimicrobial properties44,45; though other authors found no such effect.46–48 Demonstrating antimicrobial activity was not our aim; however, this may mean some negative cultures were false negatives.
Sixth, modifying drug packaging can introduce interactions with polymers (e.g., adhesion to polypropylene surfaces or leaching of syringe components). Comprehensive stability studies also assess container closure integrity, extractables and leachables. 49 While previous research suggests that medicines studied here do not undergo significant deterioration in polypropylene syringes,29,50–54 we did not perform these analyses. Future research should address this before clinical implementation.
Finally, our sample size calculation assumed a standard deviation of 3% based on preliminary data. However, greater variability was observed for some formulations (e.g. morphine T2, levomepromazine at T7, ondansetron at T3, fentanyl at T7), with standard deviations exceeding 8% at certain time points. Consequently, the precision for these specific cases is reduced, and results should be interpreted with caution. Future stability studies should consider using pilot data to inform more conservative variance estimates or increasing the number of replicates to account for formulation-specific variability.
Despite these limitations, we assessed physicochemical and microbiological data for a wide range of formulations (10 medicines, some at multiple concentrations, as well as combinations). We believe that this provides a useful foundation for understanding the stability of medications prepared by professionals in an area where evidence remains notably scarce. This study proposes a protocol for the preparation and storage of medications for subsequent SC administration that any in-hospital or out-of-hospital service could implement. It would be especially useful for hospital-at-home and palliative care at home services, given that they commonly administer medications subcutaneously. It can contribute making palliative care at home more accessible and safer.
Conclusion
The formulations studied (containing morphine, midazolam, hyoscine butylbromide, metoclopramide, haloperidol, levomepromazine, ondansetron, fentanyl, dexamethasone, and ketorolac) when prepared aseptically and stored in polypropylene syringes at room temperature, protected from light exposure, showed stability characteristics consistent with suitability for SC administration in palliative home care.
According to our study, formulations remain microbiologically and physicochemically stable for up to 12 weeks in almost all cases (the exception being metoclopramide, which showed stability for 3 weeks).
The proposed preparation and storage method is simple and could be easily implemented in in-hospital and out-of-hospital settings. The evidence of the stability of medication for up to 12 weeks provided by this study may be useful for all health professionals involved in SC administration of medications, particularly those working in hospital-at-home and palliative care settings.
Supplemental material
Supplemental material - Medication for subcutaneous administration: Microbiological and physicochemical stability of drug formulations prepared in advance and stored in syringes
Supplemental material for Medication for subcutaneous administration: Microbiological and physicochemical stability of drug formulations prepared in advance and stored in syringes by Iñigo Suberbiola, Ana Casado, Idoia de la Caba, Javier Calvo, Lore Zumeta-Olaskoaga, Maddi Aramburu, Nerea Moreno in Palliative Care and Social Practice
Supplemental material
Supplemental material - Medication for subcutaneous administration: Microbiological and physicochemical stability of drug formulations prepared in advance and stored in syringes
Supplemental material for Medication for subcutaneous administration: Microbiological and physicochemical stability of drug formulations prepared in advance and stored in syringes by Iñigo Suberbiola, Ana Casado, Idoia de la Caba, Javier Calvo, Lore Zumeta-Olaskoaga, Maddi Aramburu, Nerea Moreno in Palliative Care and Social Practice
Supplemental material
Supplemental material - Medication for subcutaneous administration: Microbiological and physicochemical stability of drug formulations prepared in advance and stored in syringes
Supplemental material for Medication for subcutaneous administration: Microbiological and physicochemical stability of drug formulations prepared in advance and stored in syringes by Iñigo Suberbiola, Ana Casado, Idoia de la Caba, Javier Calvo, Lore Zumeta-Olaskoaga, Maddi Aramburu, Nerea Moreno in Palliative Care and Social Practice
Footnotes
Acknowledgements
We acknowledge the help of Ideas Need Communicating Language Services in improving the use of English in the manuscript. The authors would like to thank Idoia Miner and Maite Murua from the Hospital-at-Home Service at Donostia University Hospital for their support in conducting the study and preparing the samples; Eukene Ansuategi, Donostia Hospital archivist, for helping with the literature search; and Maria Teresa Iglesias, for guiding the initial study design. We also wish to thank other staff at Donostia University Hospital: Diego Vicente and Marta Gómez from the Microbiology Department for help with the microbiological stability analysis; Belén Irastorza and Iris González from the Pharmacy Department for reviewing the manuscript; and Koro Andueza from the Pharmacy Department for overall support of the project. We gratefully acknowledge the invaluable support received from the Biogipuzkoa Research Institute in initiating and coordinating the entire project, with special mention of the assistance provided by Maider Mateo. Finally, the support and assistance provided by Rebeka Rodríguez, a nurse at the Lesaka health centre, in designing and organising the research has been invaluable.
Ethical considerations
This study did not include human participants or any identifiable personal data. It was approved by the Research Ethics Committee of Donostialdea IHO with approval number 08/2023.
Author contributions
All authors contributed to the conception and design of the study.
All authors reviewed the manuscript and approved the final version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received funding from the Government of the Basque Country through bottom-up, [grant number 24BU212], funding exclusively to cover the costs of conducting the study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analysed during this study are included in this article and its supplementary information files. They are available from the corresponding author upon request.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.