
Abstract
Background
Healthcare providers help families navigate end-of-life care decisions in the neonatal intensive care unit (NICU) and pediatric intensive care unit (PICU); however, limited studies exist regarding what values providers perceive families utilize when in these situations.
Objective
To evaluate providers’ perceptions of values that families considered when making end-of-life care decisions for their child.
Design
Develop a novel survey tool to understand providers’ perceptions of values families considered when making end-of-life care decisions for their children and distribute the survey tool to providers in a single quaternary care children’s hospital within a university hospital.
Methods
The novel survey tool was composed of survey questions based on existing literature, revised based on expert feedback, then iteratively refined through cognitive interviews. Preliminary data from this survey tool was collected from eligible participants at one study site.
Results
Feedback from nine experts and six cognitive interviews resulted in a 21-item survey. Ninety-five participants completed the survey. Participants reported that the relationship between the family and child, the child’s quality of life, and the child’s prognosis or disease course were most important to the family. Conversely, finances and prior experiences were ranked least important.
Conclusions
A novel survey tool was created to identify the core values that families were perceived to favor by healthcare providers when making end-of-life care decisions for their children, as a means to improve end-of-life care discussions at the bedside. Pilot data suggests that providers may understand the values that families utilize, though may not understand how they prioritize them. Future studies comparing family and provider responses, with mirrored surveys, are necessary to create decision support tools and to improve provider education in end-of-life care decision-making.
Introduction
End-of-life care decision-making in the neonatal intensive care unit (NICU) and pediatric intensive care unit (PICU) is complex. These decisions and surrounding discussions involve exploration into what the family considers important for their loved one, in the context of their prognosis and disease course, consideration of what would be in the perceived best interests of the child, and overarching guidance by the values of the family, with important input from the child’s healthcare team.1–4
However, the end-of-life care discussions occurring in the NICU and PICU may not adequately center the information families need to make these complex decisions. Pediatric healthcare providers have been noted to focus on possible outcomes, including the probability of morbidity and death, when facilitating end-of-life care discussions with families, and emphasize spirituality, emotions, and hope less frequently, although families often desire further communication on the latter aspects.5,6 The cause of this discrepancy is unclear, though may stem from provider discomfort with discussing unfamiliar aspects of spirituality and family values, believing their primary role is to communicate factual information only, or prognostic uncertainty—nevertheless, this primary focus on data may affect the end-of-life care decisions made.6–10
There are few recently published models for shared decision-making in pediatric palliative care, 11 but its wide-spread utilization by non-palliative pediatric providers remains seemingly limited. Pediatric palliative care providers are uniquely equipped to navigate difficult conversations and help supply families with critical information, however, pediatric providers, including pediatric clinicians, advance practice care providers, residents, fellows, nurses and social workers, often do not receive the same training,12,13 leading to a perpetuation of the disparity between the information that families hope to receive and the information communicated to them. Moreover, the need for pediatric providers to navigate difficult conversations without appropriate training can exacerbate the moral distress that providers already experience, distress that further negatively affects end-of-life care decision-making.14,15
Understanding the moral and practical values families employ when making complex decisions in the NICU and PICU will improve the effectiveness of healthcare providers navigating these discussions. End-of-life care decision-making is an emotionally vulnerable time; a provider-reported survey tool to gather perceptions of what families prioritize when making end-of-life care decisions for their children in the NICU and PICU collects critical preliminary data without causing undue harm to grieving families. Ultimately, the data collected in this study and in subsequent, larger trials would be beneficial to guide provider education. We thus aimed to create and pilot a survey tool for healthcare providers to assess considerations that families were perceived to value when making end-of-life care decisions for their child.
Methods
This is a cross-sectional survey study of provider-reported perceptions of family values and considerations when making end-of-life care decisions for their child. This study contained two components: (1) development of the research survey and (2) preliminary survey data collection at a single center. The survey tool was developed to fulfill the objective of collecting healthcare providers’ perceptions of what families value and prioritize when making end-of-life care decisions for their children. The University of California, Davis Institutional Review Board approved this study.
Setting
This study was conducted at a 121-bed metropolitan quaternary care children’s hospital within a university hospital. This hospital serves as a referral center for children across a 33-county region spanning 65,000 square miles and routinely receives pediatric transfers from 30 hospitals in the region. The level IV NICU has 49 beds and admits over 900 neonatal patients annually. The PICU has 24 beds (including cardiac, surgical, and extracorporeal membrane oxygenation patients) and treats over 1,600 children annually.
Eligibility criteria
Participants for both stages of this study– research survey development and survey data collection – were considered eligible to participate if they were an attending physician, fellow, resident, advanced care provider (nurse practitioner or physician assistant), nurse, or social worker working in the NICU or PICU. Additionally, eligible participants were required to have worked with a patient who required life sustaining therapy and been a party in end-of-life care discussions with the patient’s family within the past two years. As this survey was designed in English, only participants with English language preference were eligible to participate.
Research survey development
Preliminary survey development
The preliminary survey was developed de novo using existing literature5,16–19 and designed to be used to assess perceptions of family values only. Though clinical providers’ experiences notably contribute to end-of-life care decision-making, questions regarding clinician’s experiences were not included in the research survey, but rather, collected alongside demographic information. We identified five relevant domains based on the literature: (1) provider input and involvement in end-of-life care decision-making, (2) religion or cultural values, (3) prognosis, disease course, quality of life and developmental outcomes, (4) finances, and (5) the child’s role in the family. The preliminary survey contained 29-items and utilized a 4-point response scale, from “strongly agree” to “strongly disagree”.
Content expert assessment
The preliminary survey was electronically distributed to 15 content experts in the field, with nine (60%) responses received. These nine experts represented 8 distinct hospitals. Each content expert was asked to rate each survey question’s relevance to assessing family values when making decisions at the end-of-life for their children, to identify any missing or duplicative questions, and to comment on the clarity or wording of each question.
Six content experts rated each question on a 4-point scale, from “not relevant” to “highly relevant”. Responses were used to compute the item-level validity index, as described by Lynn. 20 If the item-level validity index of a question did not meet the minimum threshold, then the question was revised or removed from the survey. An additional three content experts provided feedback but did not rate the survey questions. Their feedback was taken into consideration in conjunction with item-level content validity index scores to help decide if questions should be removed, revised, or saved in the second iteration of the survey.
Cognitive interviews
After feedback from content experts was incorporated into the survey, one-on-one cognitive interviews were held with eligible participants between January 2024 and May 2024. Recruitment was completed through email outreach to role- and department-specific email listservs, and participants were instructed to email one investigator (NS) regarding their interest in participating. Participants engaged in a one-hour session that included completing the survey using the think-aloud technique, followed immediately by a semi-structed interview to assess comprehension and usability using probing techniques.21,22 Verbal consent for participation in the cognitive interview was obtained and participants received a $10 gift card for their participation.
Cognitive interviews were completed by one researcher (NS), after training completed with a study team member with known experience (JLR), via videoconference with audio recording to aid in transcript creation. The transcripts of each interview were summarized and used to code interviews thematically. After completing three interviews, three researchers (NS, CG, JLR) met to review and discuss the summaries and codes. With consensus agreement, the group added, modified, or removed questions to improve comprehension and usability of the survey tool. This process was repeated until no further areas were identified for improvement.21,22
Survey data collection
Recruitment and data collection
Potential participants were invited by email through title- and department-related listservs to complete the survey between May 2024 and November 2024. Additional recruitment was conducted through IRB-approved paper advertisements displayed in designated provider spaces in the NICU and PICU. The survey was only distributed electronically.
Every participant was required to complete a pre-screening tool, built into the survey to determine eligibility, prior to moving to the final research survey. All other components of the survey were optional. Upon completion, each participant was offered a $10 gift card.
Data analysis
Data were analyzed using descriptive statistics and two sample t-tests. Demographics and case-specific questions were analyzed using chi-square testing and descriptive statistics. Responses to the question that asked participants to rank values by what they perceived was most important to families were compared between NICU- and PICU- based participants using two sample t-tests assuming equal variances; overall mean, standard deviation, and p-values were also reported for each question. Data from questions that asked participants to indicate on a Likert scale how strongly they agreed with statements regarding family’s values and decision-making were described using median, first, and third quartiles.
Results
Research survey development
Content expert assessment
The preliminary survey contained 29 questions, 14 of which were removed or altered given an item-level content validity index of less than 0.8320. Of these 14 questions, 6 were removed and 8 were amended. Suggestions regarding the clarity of questions were incorporated. All but one free response question was removed. The resulting instrument had 22 questions, with one additional optional free response. Twenty of these questions utilized a 5-point scale from “strongly disagree” to “strongly agree”, one question was a binary “yes” or “no” question, and one asked participants to rank values in order from most to least important in the family’s end-of-life care decision-making processes.
Cognitive interviews
Six interviews were conducted over videoconference between April and May of 2024. The 20-question survey was revised within two rounds, after which there were no other issues identified by the participants. Participants reported concerns with the response scale, with question clarity, and with missing items. All questions were amended to fit the 5-point scale previously described; five questions were edited to impart clarity, two questions were added, and two questions were combined into one for a final survey with 21 questions and one free response.
Final survey
The final research survey included 20 Likert scale-based questions, one ranking question, and one free response question (Figure 1, Supplementary File 1). Every participant was invited to complete a screening tool to assess eligibility, and if eligible, were allowed to move to the final research survey. The final research survey had each participant consider their most recent experience when taking part in end-of-life care decision-making with families for their children, and answer each question based on that experience. At the end of the survey, we queried participants’ demographics, position and experience, specifics pertinent to the case participant’s envisioned while responding to the survey, their personal level of agreement with decisions made by the family, and their personal experience of burnout to contextualize the responses received. Flow diagram of the development of the survey tool.
Survey data collection
Survey results
Among the 483 healthcare providers invited to complete the survey, 95 participants completed a portion of the survey with missingness ranging from 3 - 82% of survey questions; 73 (76.8%) completed the entire survey with no missingness and were included in the final analysis. We had a 19.7% response rate, with 15.1% completing the research survey and 14.3% completing the entire survey.
Demographic information for respondents and case-specific information.
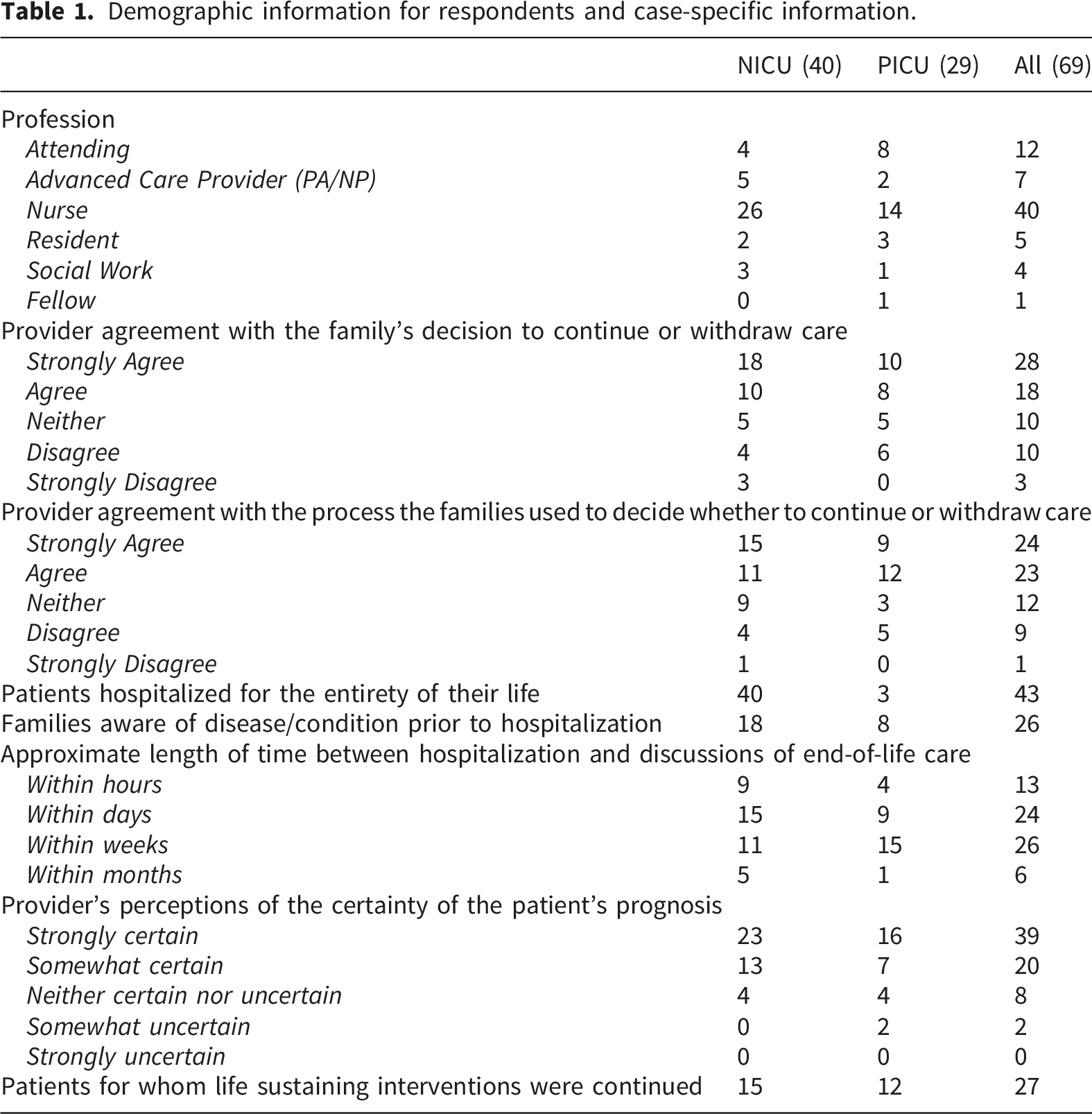
Most respondents agreed with the decision the family made (67%) and the process by which they made the decision (68%). The cases respondents considered differed in terms of parents’ knowledge of the condition prior to hospitalization and length of stay, though the majority reported that the prognosis was certain at the time decision-making occurred (Table 1). Fifty-two (75.4%) respondents reported experiencing some level of moral distress in caring for their patient, with 9 (13%) reporting that they experienced “significant” moral distress.
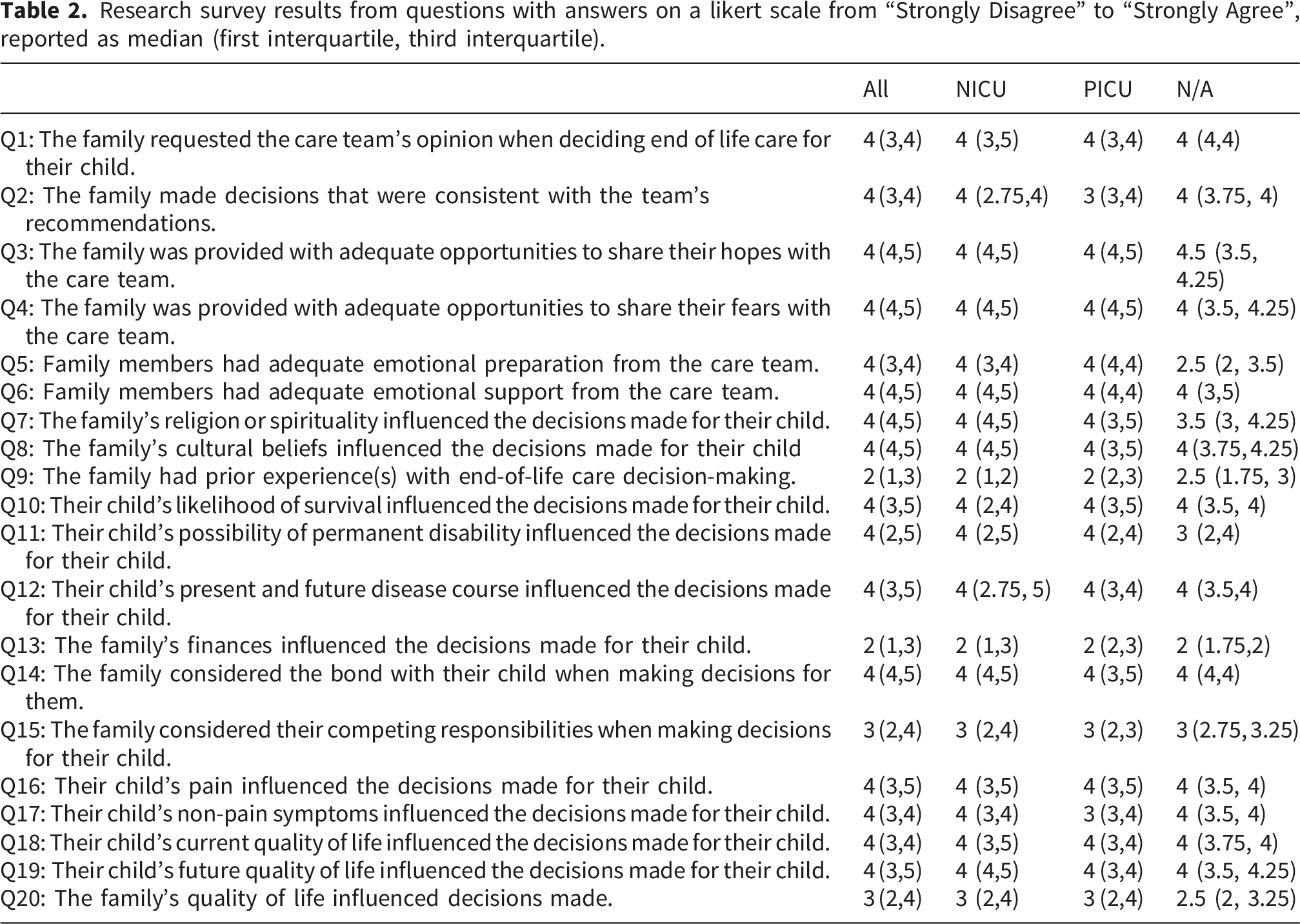
Research survey results from questions with answers on a likert scale from “Strongly Disagree” to “Strongly Agree”, reported as median (first interquartile, third interquartile).
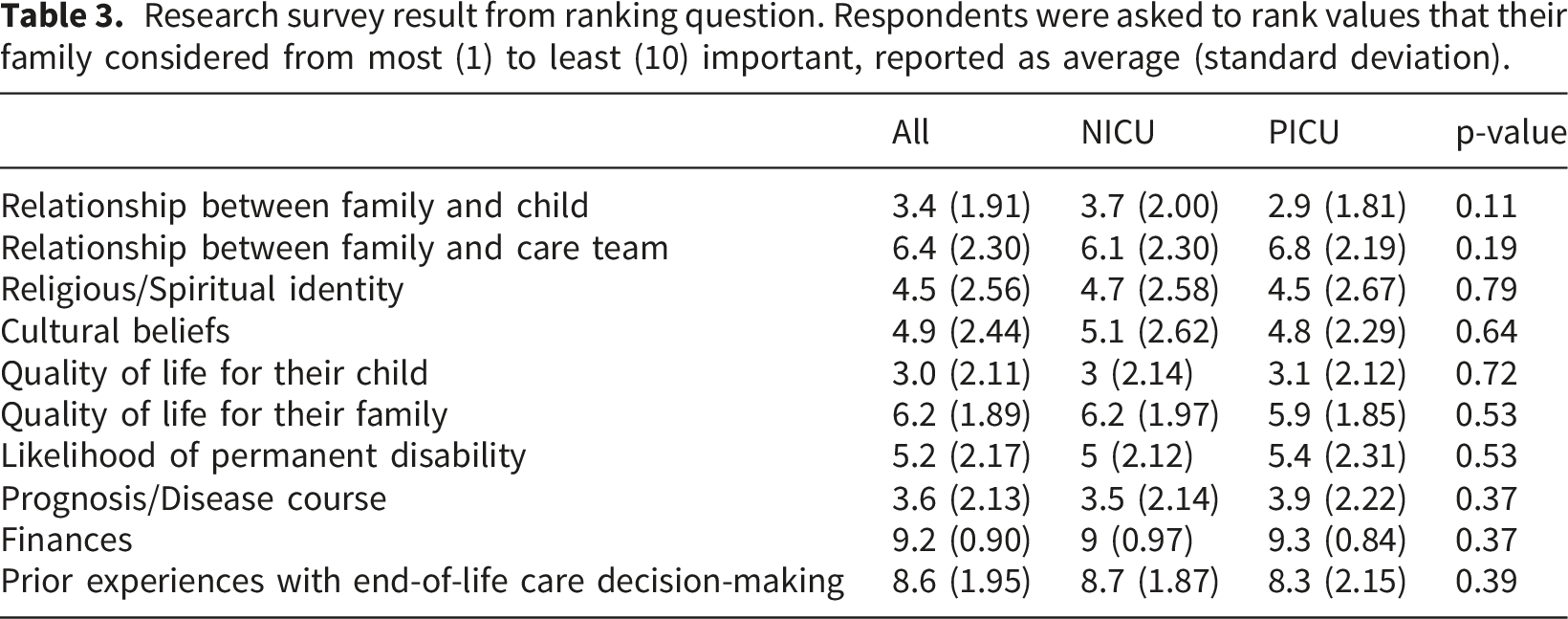
Research survey result from ranking question. Respondents were asked to rank values that their family considered from most (1) to least (10) important, reported as average (standard deviation).
Discussion
We sought to understand healthcare provider’s perceptions of family values and priorities during end-of-life care decision-making for their children in the NICU and PICU, and we developed a novel survey tool towards that purpose. Our pilot revealed that this survey can be completed with low missing values.
The survey was intended as a first step towards understanding the priorities families have when making end-of-life care decisions for their children to improve and inform end-of-life care discussions at the bedside. While our study focused solely on the perspectives of healthcare providers, true understanding of family values, how they contribute to end-of-life decision-making, and the differences between healthcare providers’ and families’ perceptions and families’ values requires surveying both families and members of the care team. The scope of this study was to develop a survey tool to assess provider perceptions and additionally intended to serve as a starting point for developing similar survey tools that would be appropriate to ascertain families’ perspectives.
Study participants in the NICU and PICU identified that families value current and future quality of life for their child, religious and cultural factors, pain and non-pain symptoms, the relationship between the family and child, competing responsibilities of the family, likelihood of permanent disability or death, and prognosis and disease course, which is consistent with what has been reported in the literature by parents.5,16,19,23–25 When respondents were asked to rank perceived values from most to least important, they reported prognosis and disease course, quality of life, and relationship between the family and child to be most important; however, bereaved parents of children who died in the PICU have previously reported quality of life, likelihood of clinical improvement, likelihood of death, and perceived pain to be the most salient factors for end-of-life care decision-making for their children. 19 Additionally, respondents perceived past experiences of or previous involvement in end-of-life care decision-making to be of less value for families making similar decisions for their children; however, in a prospective study of 14 parents of children in the PICU, past experiences with end-of-life heavily influenced parents’ decision-making, noting that parent’s often compared their child’s situation with that of loved ones who have previously passed away. 23 Respondents viewed finances to not play a significant role in end-of-life care decision-making—consistent with prior research 19 —though whether finances play a significant role in decision-making is difficult to assess, as finances may not be routinely brought up in family meetings. The discrepancies elicited by our survey item requires further investigation—if reproduced in larger studies and the difference corroborated with a mirrored, family-focused survey tool, it highlights a gap between true family values and provider perceptions of the same, and indicate a need for education interventions so that providers are better equipped to delve into what values families prioritize most when discussing end-of-life care for their children.
Our survey did not discern a difference between responses from respondents in the NICU and PICU, although there is emerging evidence that end-of-life care decision-making differs between units.26–29 At our hospital, neonates requiring advanced cardiac support, including extracorporeal membrane oxygenation, are transferred to the PICU where our cardiac intensive care subunit is located, contributing to our inability to discern a difference.
Most respondents (75.4%) from the NICU and PICU reported that they experienced some level of moral distress in caring for their pediatric patient. End-of-life care decision-making in pediatrics is emotionally fraught, with clinical providers often experiencing moral distress rooted in value differences.15,30,31 The experience of moral distress, especially when value conflicts exist, can often be exhibited as rude or dismissive behaviors that risk the parent-provider relationship. 32 Although differences in values will persist, providers’ acknowledgement of specific family values in end-of-life care decision-making may allow for better coping and reduced moral distress in the NICU and PICU. 30
There are several limitations to this study. This study asked participants to consider the most recent patient where they were involved in the end-of-life care discussions with their family. Given the limited number of patients that required end-of-life care discussions in the NICU and PICU at our hospital during our study period, multiple providers may have envisioned the same case, possibly skewing results. This may be mitigated in larger trials, but unavoidable in this study. Additionally, we had a low response rate, likely secondary to our methods of outreach—our survey was primarily distributed through email listservs, and secondarily through paper flyers in teamwork spaces, methods that can easily be overlooked in high-stakes clinical settings. Targeted emails to potential participants, rather than emails distributed through listservs, and in-person recruitment efforts may increase response rate. While this survey was developed and pilot tested at a single site, larger studies in a variety of children’s hospital settings (including free-standing, university-affiliated, and community children’s hospitals) should be completed to confirm our study findings.
Despite these limitations, the results of our novel survey reveal interesting preliminary results, that, if corroborated by future studies in larger sample sizes with a mirrored, family-focused survey, may serve to guide clinical trainee and provider education in end-of-life care decision-making. The preliminary data collected shows that while providers may demonstrate understanding of the core values that families prioritize when making end-of-life care decisions, there may be differences in what providers believe is most important to families when compared to published literature. By constructing support tools and education for providers to elicit values that families prioritize, and how they prioritize them, we encourage end-of-life care discussions that support the needs of the family, positively influence the patient’s and families’ experience during their hospitalization,24,33–35 as well as serve to mitigate moral distress as experienced by providers. 30
Supplemental material
Supplemental material - Healthcare provider’s perceptions of family values when making end-of-life care decisions for their children: Developing and implementing a survey tool
Supplemental material for Healthcare provider’s perceptions of family values when making end-of-life care decisions for their children: Developing and implementing a survey tool by Nithya Sivakumar, Stephanie Kukora, Cherie Ginwalla, Satyan Lakshminrusimha, and Jennifer Rosenthal in Palliative Care and Social Practice.
Footnotes
Acknowledgements
We would like to acknowledge the contributions of Dr. Jeanne Krick, Dr. Katherine Guttmann, Dr. Amy C. Trowbridge, Dr. Naomi Laventhal, Dr. Erin Rholl, Dr. Uchenna E. Anani, Dr. Marlyse Haward, Dr. Elliott Weiss, and R. Dawn Hood-Patterson, all of whom shared their valuable insight and served as expert reviewers for this study.
Ethical considerations
This study (IRB # 2122059-1) was deemed exempt from formal IRB review by The University of California, Davis Institutional Review Board.
Consent to participate
Participation from our expert reviewers, cognitive interviewees, and survey respondents were voluntary, and verbal consent was obtained for recording of cognitive interviews. A letter of information (consistent with HRP-502, as required by The University of California, Davis Institutional Review Board) was provided for participants to review prior to their participation in this study, which included the purpose of the study, the involvement of research, procedures to be performed, that participation is voluntary, the risks and benefits of participating, as well as the name and contact information of the investigator. Per The University of California, Davis Institutional Review Board, no further written consent form was necessary for this study.
Consent for publication
Participants were made aware that the results of these research procedures may be published, and that data collected may be used in future studies, prior to their participation. By participating in this study, participants consented for their de-identified data to be used for publication.
Author contributions
This was a highly collaborative undertaking, and every author contributed significantly from conception to publication.
Nithya Sivakumar, MD, MBE, contributed through study conception, funding acquisition, method development, survey development and iterative revisions, survey administration, data analysis, as well as writing the original draft and editing it further.
Stephanie Kukora, MD contributed through study supervision, study conception, survey development and iterative revisions, data analysis, and reviewing and editing manuscript drafts.
Cherie Ginwalla, MD, contributed through study supervision, study conception, survey development and iterative revisions, data analysis, and reviewing and editing manuscript drafts.
Satyan Lakshminrusimha, MD, contributed through study supervision, study conception, funding acquisition, and reviewing and editing manuscript drafts.
Jennifer Rosenthal, MD, MAS contributed to the study through study supervision, study conception, method development, survey development and iterative revisions, survey administration, data analysis, and reviewing and editing manuscript drafts.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the National Center for Advancing Translational Sciences, National Institutes of Health, through grant number UL1 TR001860 and linked award TL1 TR001861. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The final version of the survey utilized is available as a supplemental file in this article; demographic and supplemental questions, as well as preliminary data collected, is available by contacting the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.