
Abstract
Background
Parents of children receiving palliative care often experience significant caregiving responsibilities and unmet support needs, emphasising the importance of systematic assessments and tailored interventions.
Objectives
This study examined the feasibility of the Carer Support Needs Assessment Tool Intervention Paediatric (CSNAT-I Paediatric) within a national unit for children’s palliative care in Norway. It further explored the support needs of parents of children with severe neurological impairments, including neurometabolic conditions.
Design
A non-randomised, multi-method feasibility study.
Methods
Feasibility was examined across domains of acceptability, demand, implementation, practicality, integration, and adaptation. Cognitive interviews with parents (n=34) were conducted to examine acceptability and needs for adaptation. Overall feasibility from parents’ perspectives were measured using an electronic questionnaire (n=12), and data on parents’ support needs were extracted from the children’s medical records. Intervention providers’ perspectives on acceptability, demand, practicality, implementation and integration were explored in a focus group interview (n=6).
Results
Parents found the CSNAT-I Paediatric acceptable and all domains of the assessment tool were considered relevant, although they suggested adaptations to better capture care coordination and the child’s daytime activities. Parents’ support needs were heterogeneous and often required action from multiple parties. Intervention providers viewed the CSNAT-I Paediatric as useful for tailoring services to families but identified practical and implementation challenges in following up on identified needs.
Conclusions
The CSNAT-I Paediatric is feasible in children’s palliative care settings. Effective implementation requires interprofessional and intersectional collaboration among stakeholders to meet families’ complex support needs, and further refinement could enhance its utility.
Plain Language Summary
Testing a New Approach to Identify and Address Support Needs of Parents in Children’s Palliative Care.
Parents who care for children receiving palliative care often have many responsibilities and may not get all the support they need. It is therefore important to regularly ask parents about their support needs and to offer tailored assistance.
This study looked at whether a systematic approach for assessing and addressing parents’ support needs could be used in practice in a national children’s palliative care (CPC) unit in Norway. We focused on whether the method was acceptable to parents and providers, easy to use, and could be integrated into routine care. We also explored the types of support needs reported by parents of children with life-limiting and life-threatening conditions.
Parents were asked to give feedback on the Norwegian version of the assessment tool included in the method, complete a questionnaire about their experiences, and identify their most important support needs. The professionals who delivered the method took part in a group interview to share their experiences.
Overall, parents were happy with the method. They felt it helped identify important support needs, although some areas, such as care coordination and daytime activities for their child, could be improved. Parents’ support needs varied widely and often required input from several services. The professionals found the tool helpful for tailoring support to families but reported challenges related to time, coordination, and implementation.
In conclusion, the method, called CSNAT-Intervention Paediatric, can be used in children’s palliative care settings. To work well in practice, it needs strong collaboration between different professionals and services, and some further development may improve how well it meets families’ needs.
Introduction
An estimated 21 million children worldwide could benefit from palliative care, 1 a number that continues to grow as advances in medical care prolong survival. 2 Children’s palliative care (CPC) aims to enhance the quality of life for children with life-limiting conditions and their families by providing holistic support throughout the child’s life. 3 Parents of children receiving palliative care have considerable caregiving responsibilities and their own support needs. 4 Compared with parents of healthy children, they tend to experience greater worry and overall strain, and reduced quality of life, requiring more emotional and practical support. 5 Their support needs are diverse and multifaceted, 6 calling for comprehensive and multidisciplinary services that ensure stability and continuity in a challenging life situation. 7
By assessing and addressing parents’ support needs, parents can become better equipped to cope with the caregiving burden. 8 However, despite being recommended, 3 systematic approaches for such assessments have not yet been established within CPC in Norway. One potentially suitable approach for identifying and addressing parents’ support needs is the Carer Support Needs Assessment Tool – Intervention Paediatric (CSNAT-I Paediatric).9–11 The CSNAT-I Paediatric follows a five-stage process: (1) introduction of the intervention, (2) parents assess their own needs, (3) an assessment conversation, (4) development of a shared action plan, and (5) a shared review.
The CSNAT-I Paediatric gives caregivers the opportunity to assess, express, and prioritise their support needs, thereby providing a systematic framework for developing targeted, family-specific interventions. A central component of the intervention is the Carer Support Needs Assessment Tool Paediatric (hereafter referred to as assessment tool) that comprises 16 support domains. Half focus on the support parents need to enable care for their child (enabling support needs), while the other half addresses the support parents need for their own well-being (direct support needs). Each domain includes checkboxes allowing parents to indicate their level of need: “no need for support,” “a little more need for support,” or “quite a bit more need for support.” An additional open-text field enables parents to identify support needs not captured within the 16 domains. The purpose of the assessment tool is to inform the subsequent assessment conversation by prompting reflection and structuring discussion of parental support needs, rather than to function as a quantitative questionnaire. 12
The CSNAT-I was initially developed for use with carers of adults receiving palliative care, and its effectiveness has been validated in several countries.13–16 In 2017, the intervention was modified for use in a paediatric context 9 by revising the language to better suit parents and by adding two domains to the assessment tool, one domain on care of others in the home and another on relationship to spouse or partner, to better align with parents’ support needs. Use of the CSNAT-I Paediatric has revealed that the needs of caregivers of children with cancer differ from those of caregivers for children with non-cancer conditions, indicating that these subgroups require further attention and exploration. 17
A recent study found that the assessment tool was useful for identifying parents’ support needs and highlighted the need for further research on the feasibility of the CSNAT-I Paediatric as a whole. 11 This underscores the importance of examining feasibility when introducing an existing intervention into a new context. In this regard, feasibility studies assess whether an intervention is acceptable, appropriate, and deliverable within different organisational and cultural settings, and help identify where adaptation may be required while preserving core components. 18 More broadly, feasibility work addresses whether and how an intervention can be implemented at scale, focusing on elements such as practicality, acceptability, and implementation rather than effectiveness. 19
In Norway, the CSNAT-I Paediatric is currently used in some CPC units; however, its feasibility in a Norwegian context has not yet been evaluated.
Therefore, this study aims to assess the feasibility of the CSNAT-I Paediatric for parents of children with severe neurological impairment, including neurometabolic conditions, in a Norwegian CPC context. It also aims to identify the most common support needs of these parents and how these are addressed.
Methods
Design
This study employed a multi-method approach to examine the feasibility of an intervention. We drew upon selected domains from Bowen et al.'s 20 framework for identifying feasible interventions, which provides a structured approach to assessing complex interventions across multiple dimensions of feasibility. This framework encompasses eight potential domains: acceptability, demand, implementation, practicality, integration, adaptation, expansion and limited-efficacy testing. It enables systematic examination not only of whether the intervention can be delivered as intended, but also of contextual factors that may influence its uptake and sustainability. Consistent with Bowen et al.’s guidance that the domains are not exhaustive or mandatory but should be selected according to study aims, six domains were included in this study: acceptability, demand, implementation, practicality, integration, and adaptation. Acceptability refers to the extent to which the intervention is received positively by intended recipients and those involved in its delivery. Demand relates to the actual or anticipated uptake of the intervention within the target population or setting. Implementation concerns the extent to which the intervention can be delivered as intended, including its fidelity and completeness. Practicality examines the extent to which the intervention can be delivered within real-world constraints such as time, resources, and organisational capacity. Adaptation refers to modifications made to intervention content or delivery to ensure suitability for the target context or population. Integration assesses the extent of system-level change required to embed the intervention within existing organisational structures and routines.
Setting
The study was conducted at a non-hospital-based CPC unit with a nationwide remit. The unit comprises a multidisciplinary team of professionals from health and social care services, as well as education, all experienced in providing CPC. The unit typically supports families in the “living with” phase, that is, following diagnosis and after the initial critical phase, and not in the terminal phase of life, but during the intervening weeks, months, or years between these stages. During the establishment of the CPC unit, patient organisations representing children with cancer and congenital heart disease were consulted, and it was agreed that these groups would not be included in the unit’s target population, as they already benefit from well-established care pathways and structured follow-up within specialist health services. The unit operates as a supplement to the standard health and social care system and is funded by the Norwegian Directorate of Health.
Participants and recruitment procedure
Parents of children aged 0–15 years who were part of the CPC unit’s target group were eligible to participate. Parents who did not speak Norwegian fluently were excluded. Consecutive enrolment of eligible parents referred to or seeking services from the CPC unit was conducted. All families eligible for services from the CPC unit during the recruitment period from November 2022 to June 2024 were offered the opportunity to begin the CSNAT-I Paediatric. The family’s designated care coordinator (CC) in the CPC unit provided a brief introduction to the project and requested permission, on behalf of the first author, to contact the family by telephone for more information about the study.
Delivery of the CSNAT-I Paediatric
The family’s CC within the CPC unit delivered the intervention to the parents. All CCs received formalised training in how to carry out the intervention. A written internal procedural guide was also developed, outlining how the intervention was to be implemented within the current CPC unit (Supplemental File 1). The five steps of the CSNAT-I Paediatric were delivered as follows: 1) The CC initially introduced CSNAT-I Paediatric to the parents by telephone after the referral to the CPC unit. At the same time, their local care teams were convened to gain an understanding of the family’s situation and care plans, and to inform them about the steps of the intervention. 2) The assessment tool, intended as a conversation starter, was sent by post to parents prior to the assessment conversation, allowing them time to consider their needs. 3) The first or last author conducted the assessment conversations together with the CC, who wrote the summary. When parents were a couple, they participated jointly. Divorced or single parents were given the option of an individual assessment conversation. The conversations were either face-to-face or via video. During the assessment conversation, parents were invited to describe areas where they needed additional support and were asked follow-up questions to gain a fuller understanding of their needs. The assessment conversation lasted approximately 60 minutes. Towards the end, parents were asked to rank the three support needs they considered most urgent or important. 4) The CC developed the shared action plan in collaboration with parents and relevant stakeholders to address the support needs that had been reported and prioritised. The action plan included prioritised support needs, proposed actions to address them, and an overview of the parties responsible for each action. 5) The shared review was conducted after sufficient time had been allowed for the agreed actions to be initiated and addressed. This could take place a few weeks or several months later, depending on the time required to address the prioritised support needs. The CC, the parents and potentially other involved parties participated in the meeting. During the meeting, progress on the agreed actions was discussed, including which needs had been satisfactorily addressed, which remained unaddressed, and the reasons why some actions may not have been achievable. Towards the end of the conversation, the CC and the parents agreed on the plan for follow-up, either to begin another round of CSNAT-I Paediatric or to wait and reach out when needed.
Data collection
Demographic information about the child and family was obtained from the child’s medical record.
Feasibility of CSNAT-I Paediatric from the parents’ perspective
Prior to the study, the CPC unit translated the assessment tool into Norwegian, in accordance with EORTC procedures, which follow a rigorous forward-backward translation process. 21 Interviews were conducted guided by cognitive interviewing principles 22 to validate language clarity, relevance of included domains, and sensitivity of the translated assessment tool. In addition, parents’ acceptability of the assessment conversation and potential adaptation requirements to the assessment tool were explored. Parents’ responses to being given the opportunity to identify and express their support needs were explored to assess the demand for the intervention. These interviews were integrated as an extension of the needs assessment conversation with parents. The first or last author conducted the interviews using a self-developed interview guide (Supplemental File 2); each interview lasted 5–10 minutes. The CC noted the responses in the needs assessment conversation summary and stored them in the child’s medical record with parents’ oral permission.
To examine the practicality of the intervention, the summary of the assessment conversation, the shared action plan, and the shared review summary were extracted from the child’s medical record.
To assess the overall feasibility of the intervention from the parents’ perspectives, the CC sent an electronic questionnaire to parents after the completion of the CSNAT-I Paediatric process. The questionnaire included 12 items evaluating delivery and suitability of the intervention using a five-point Likert scale. Each item also included an open comment field to allow for further elaboration.
Feasibility of CSNAT-I Paediatric from the providers’ perspective
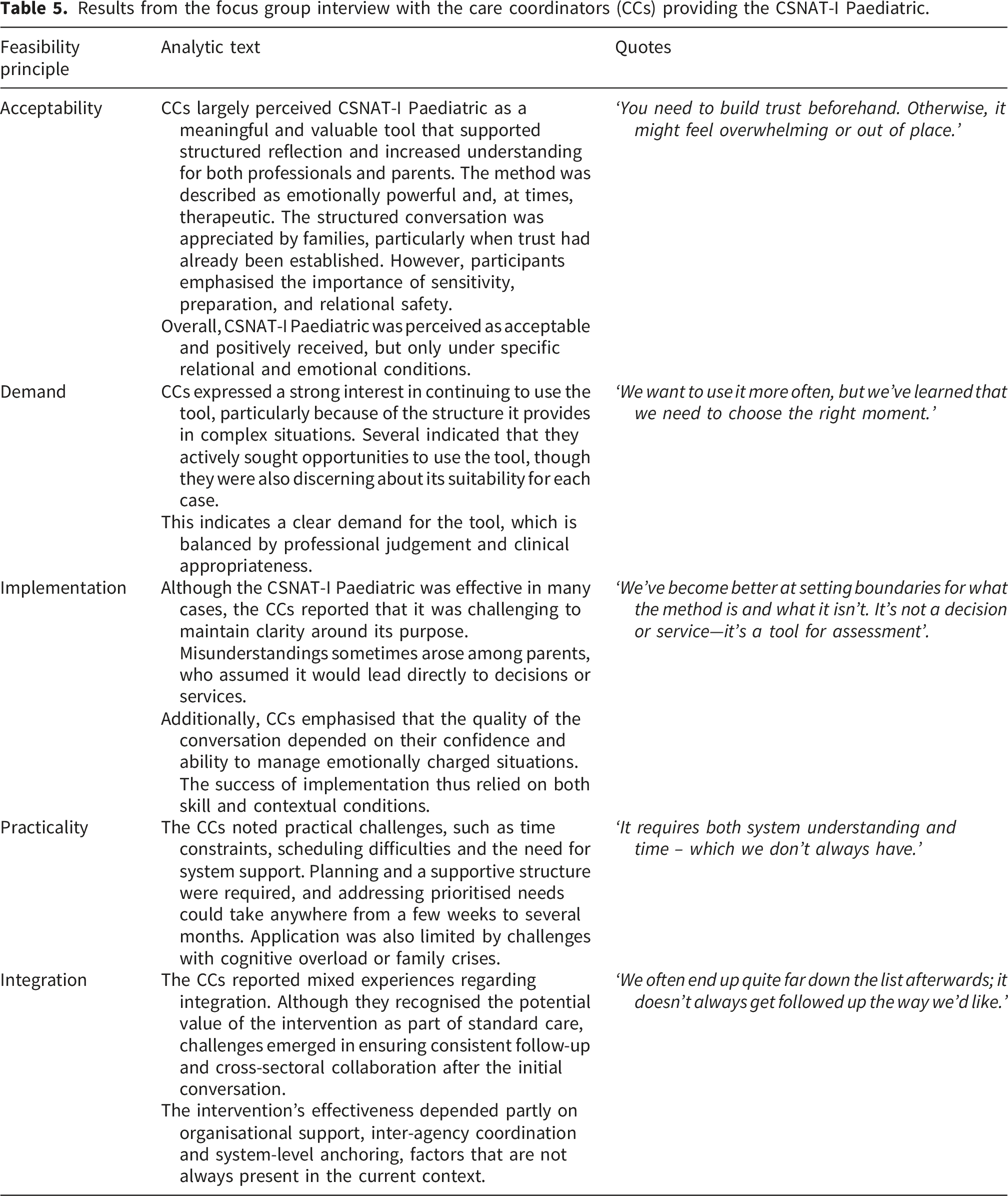
To examine feasibility domains from the providers’ perspectives, we conducted a semi-structured focus group interview with the six CCs who delivered the CSNAT-I Paediatric, using a self-developed interview guide covering the following topics: (1) overall feasibility in practice; (2) acceptability in terms of suitability and relevance; (3) demand and practicality, explored through professional experience and local collaboration; (4) implementation in relation to resource use, barriers, and potential solutions; and (5) integration with respect to sustainability and continuation. (Supplemental File 3). The first author conducted the interview, which lasted approximately 90 minutes. All of the CCs were women, from the fields of physiotherapy, clinical dietetics, psychology, nursing, special education, and medicine. The session was audio-recorded and uploaded to a secure database upon conclusion. The interview was transcribed using Whisper, an automatic transcription software developed by OpenAI (v2.0), and subsequently checked for accuracy by the first author.
Data analysis
Descriptive statistics were used to describe participants’ characteristics. The cognitive interviews were summarised by topic in the interview guide. The written summaries from the assessment conversation and the shared action plans from the CSNAT-I Paediatric process were analysed using a descriptive approach to identify parents’ prioritised support needs and the suggested actions to address them. The summary of the shared review, documented in the children’s medical records, was reviewed to provide an overview of the extent to which the reported support needs were addressed and how much time had passed between agreement on the action plan measures and the point at which they were addressed.
A deductive thematic analysis 23 was conducted to analyse the data from the focus group on providers’ experiences of intervention delivery. In the analysis, the first author familiarised herself with the data before coding it deductively into the feasibility domains of demand, acceptability, integration, implementation, and practicality. All authors discussed and reviewed the process to enrich the analysis.
Descriptive statistics were used to summarise the responses in the electronic questionnaire. As the scores were not normally distributed, results are presented as median and interquartile range (IQR). Analyses were conducted using Microsoft Excel.
Results
Demographic characteristics of parents and children 1 .
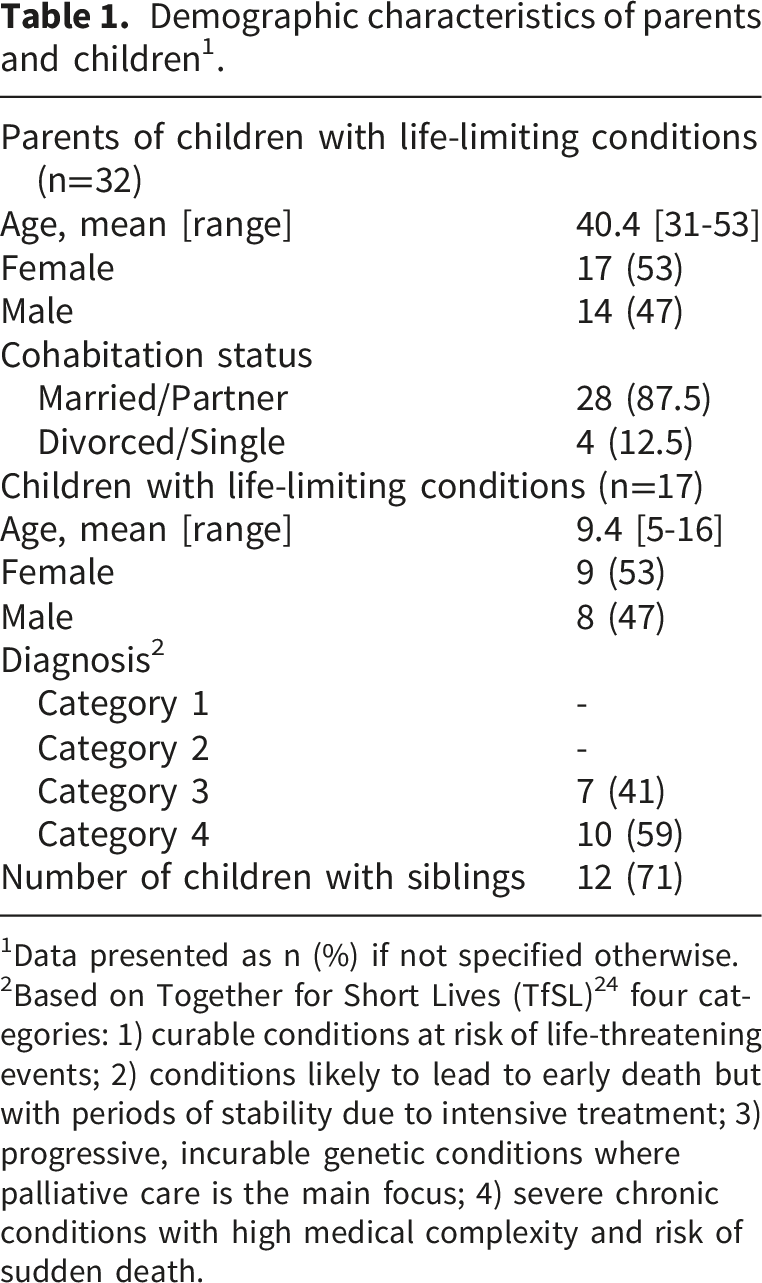
1Data presented as n (%) if not specified otherwise.
2Based on Together for Short Lives (TfSL) 24 four categories: 1) curable conditions at risk of life-threatening events; 2) conditions likely to lead to early death but with periods of stability due to intensive treatment; 3) progressive, incurable genetic conditions where palliative care is the main focus; 4) severe chronic conditions with high medical complexity and risk of sudden death.
Feasibility of CSNAT-I Paediatric from the parents’ perspective
In relation to acceptability and adaptation of CSNAT-I Paediatric based on the cognitive interviews, parents overall stated that the information in the assessment tool was concise and provided sufficient detail. They found the translated assessment tool easy to understand and use, they considered the wording to be adequately sensitive, and they found all the existing domains relevant. When asked if any topics were missing from the assessment tool, participants highlighted the need for domains addressing care coordination, navigating the support system, nutritional management, the child’s daytime activities, practical and emotional support for paid carers, and preparing for end-of-life care.
Regarding demand for such an intervention, several parents reported that it was valuable to have dedicated time and space to discuss their needs with professionals. Some noted that it felt unfamiliar to focus on their own needs, and one mother stated, “We haven’t been asked before what we actually need.” Parents described the intervention as a form of support they have not previously received and indicated that they would recommend CSNAT-I Paediatric to other parents.
The summaries from the assessment conversations and subsequent action plans showed that parents’ prioritised support needs varied widely, with multiple stakeholders responsible for initiating and following up on actions to address them. These included the CC in the CPC unit providing CSNAT-I Paediatric, municipal care coordinators or other local service providers and various professionals within specialist healthcare, including members of the specialist CPC teams. The frequency of the domains in which parents prioritised their top three support needs in the assessment conversation based on the domains of the assessment tool is shown in Figure 1. Frequency of parents’ (n=32) top three prioritised support needs.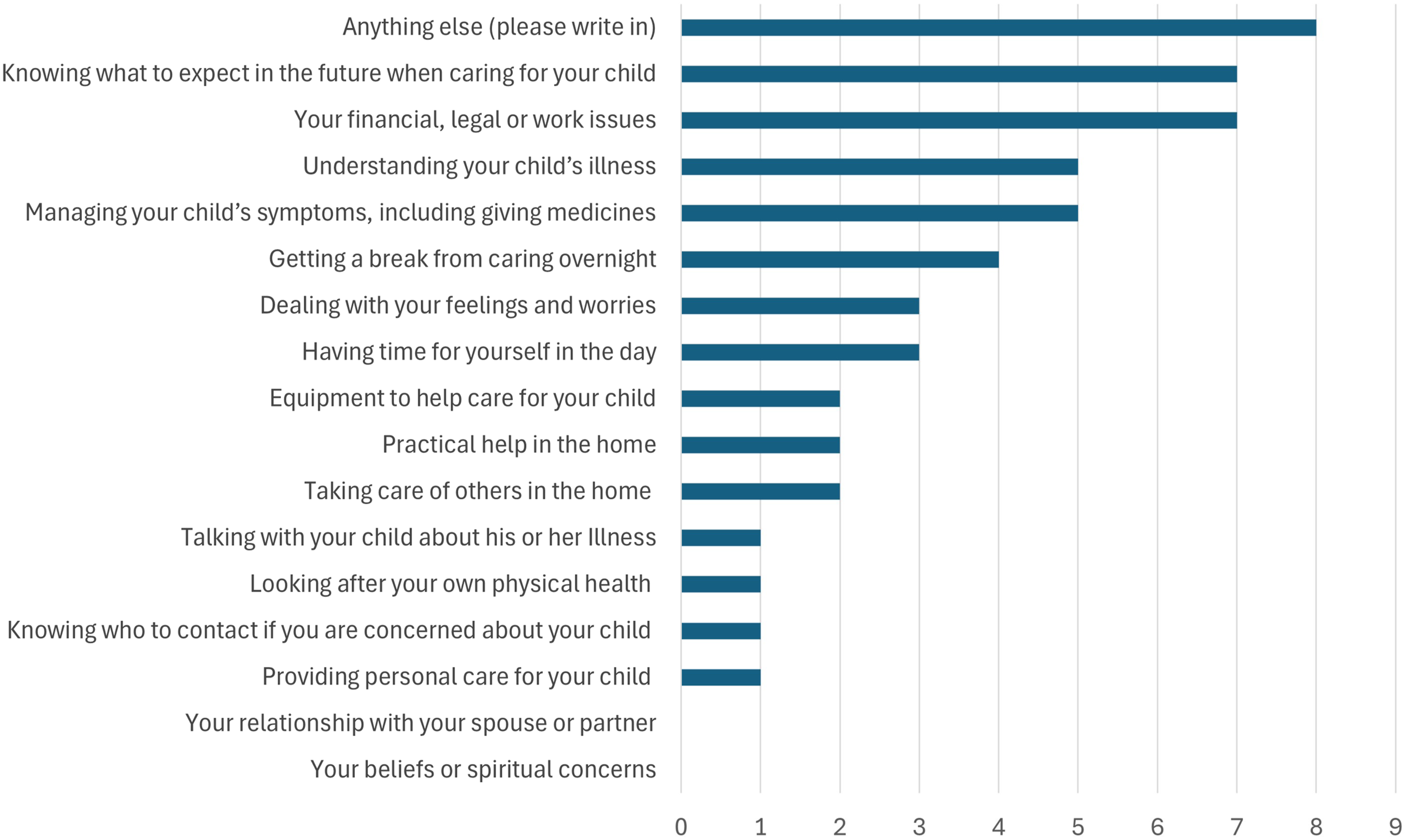
Reported prioritised support needs and corresponding actions that enable parents to care for their children.
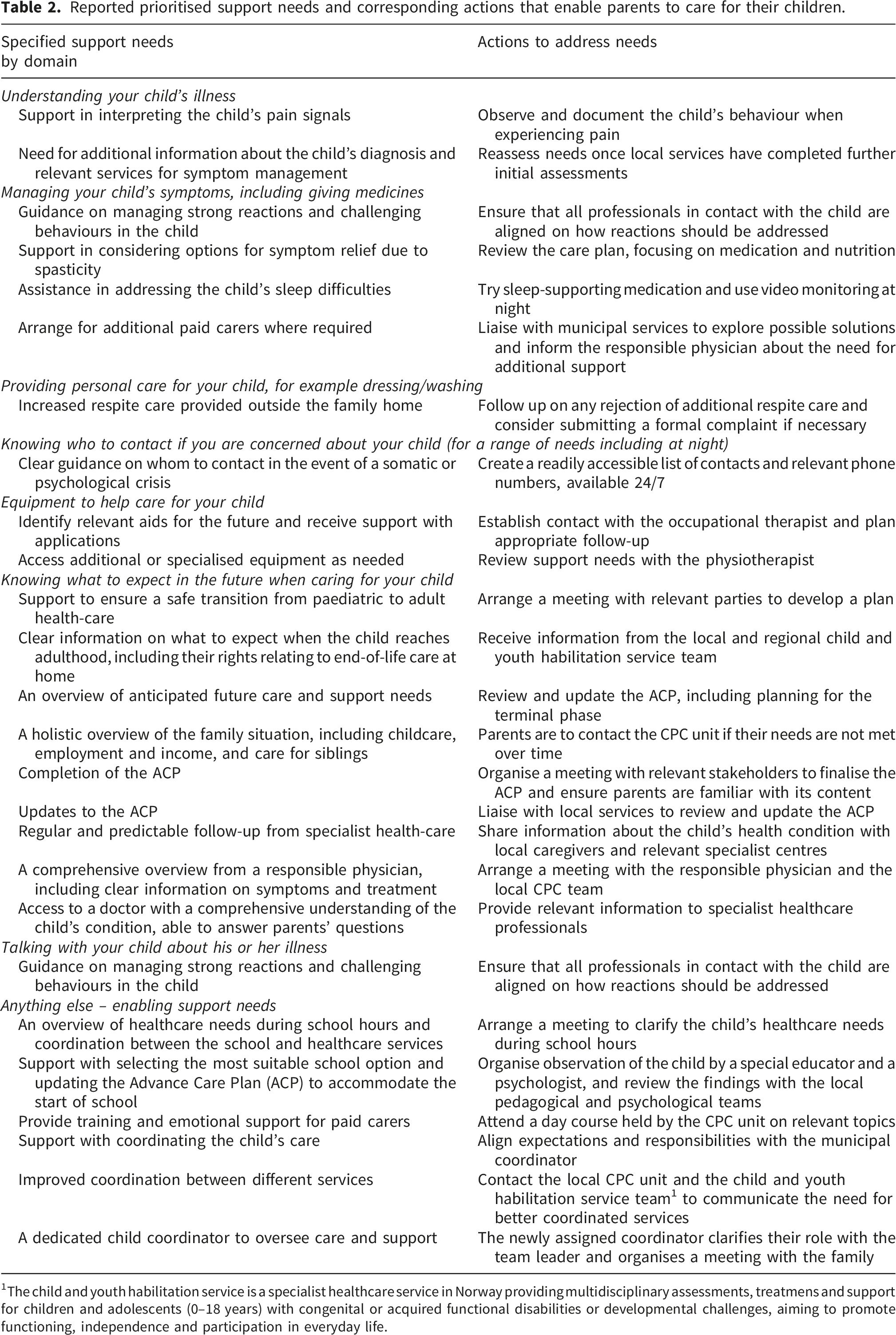
1The child and youth habilitation service is a specialist healthcare service in Norway providing multidisciplinary assessments, treatmens and support for children and adolescents (0–18 years) with congenital or acquired functional disabilities or developmental challenges, aiming to promote functioning, independence and participation in everyday life.
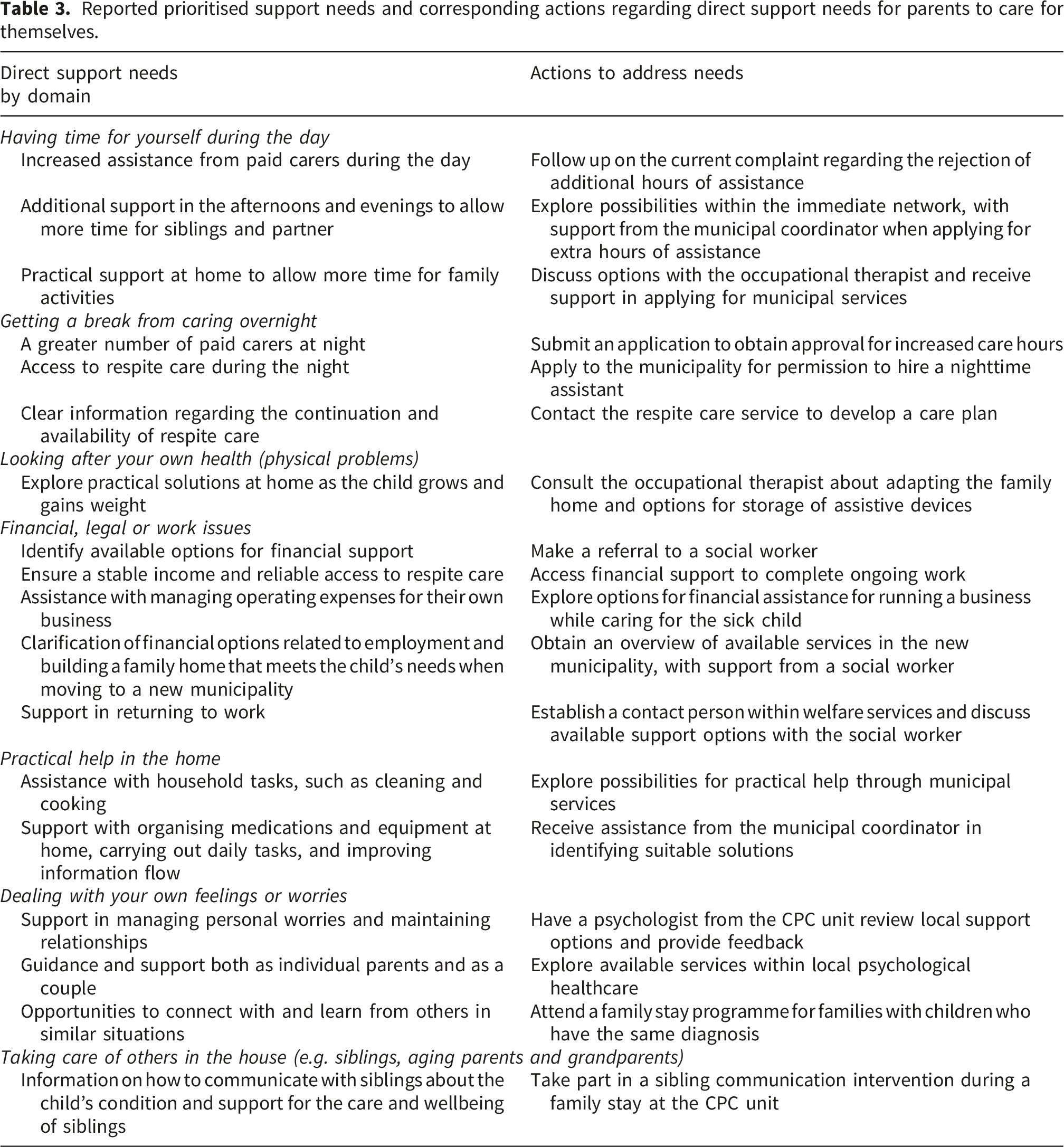
Reported prioritised support needs and corresponding actions regarding direct support needs for parents to care for themselves.
From the child’s medical record, we found that the time between the agreed action plan and the shared review varied from a few weeks to several months, corresponding to the overall duration of the CSNAT-I Paediatric process. At the point of the shared review, most support needs had been addressed, while some were still in progress or remained unresolved.
Parent (n = 12) electronic evaluation of the CSNAT-I Paediatric.
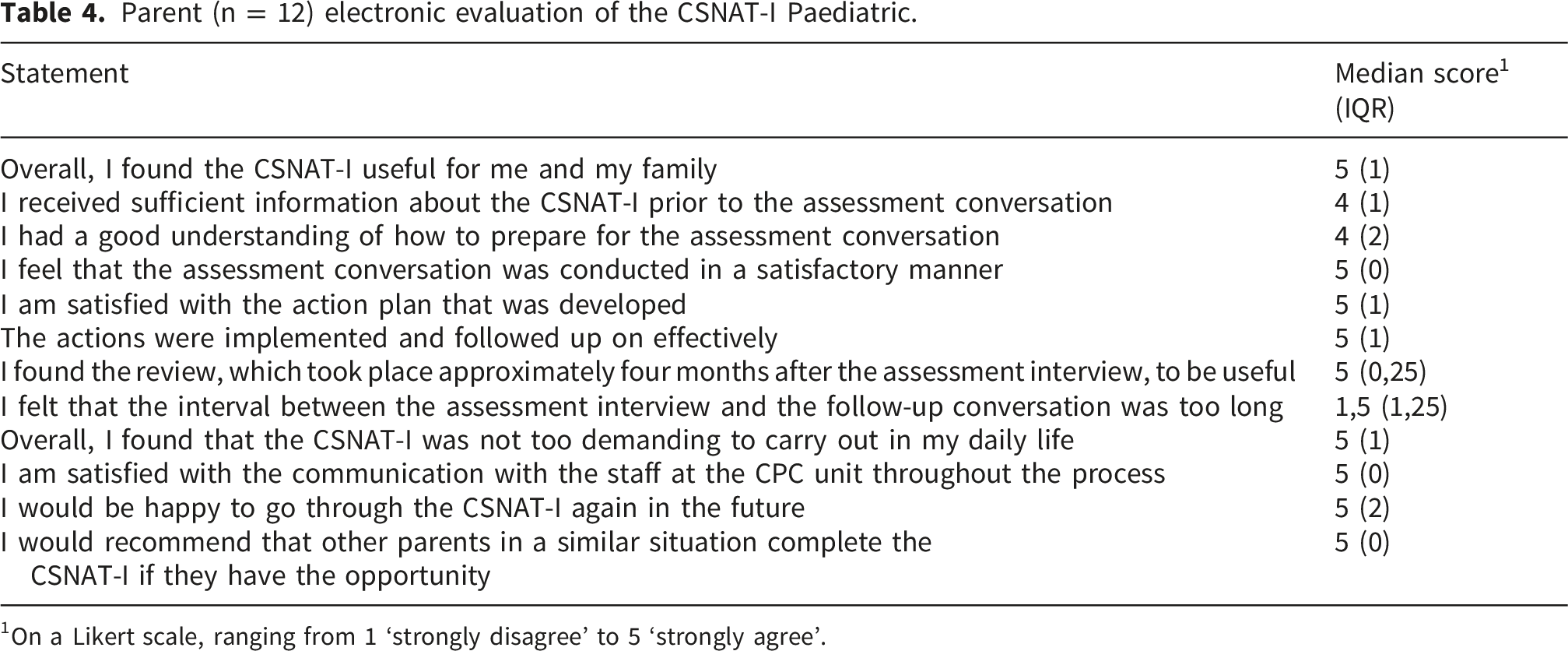
1On a Likert scale, ranging from 1 ‘strongly disagree’ to 5 ‘strongly agree’.
Feasibility of CSNAT-I Paediatric from the providers’ perspectives
Results from the focus group interview with the care coordinators (CCs) providing the CSNAT-I Paediatric.
Discussion
This study examined the feasibility of the CSNAT-I Paediatric as a structured approach to assessing and addressing parents’ support needs within CPC in Norway and is the first to focus exclusively on parents of children with severe neurological impairment, including neurometabolic conditions. The findings suggest that the intervention is well accepted by both parents and providers, is suitable for implementation in the current context, and our findings indicate clear demand for a structured approach to systematically assessing and addressing parental support needs in CPC. Nevertheless, our study identified challenges relating to the integration and practicality of the CSNAT-I Paediatric that should be considered in future implementation. These challenges were largely driven by the diversity of parents’ support needs and the involvement of multiple stakeholders. As a result, completing all five steps of the intervention was time-consuming, and maintaining consistent follow-up and cross-sectoral collaboration to adequately address parents’ reported support needs was challenging.
Parents reported that they found the assessment tool embedded within the intervention easy to understand and appropriately concise. All domains of the assessment tool were considered relevant, suggesting that the current structure largely reflects parents’ support needs in CPC. However, several needs were identified as missing: care coordination and support system navigation, training and emotional support for paid carers, daytime activities for their child, nutritional management and end-of-life care. While some of these needs may be covered by existing domains, others may be considered for inclusion in the assessment tool. A United Kingdom study examining the same assessment tool also noted the absence of a domain addressing educational needs, 11 aligning with our findings regarding limited support for children’s daytime activities. These results reinforce Fisher et al.’s recommendation to introduce a specific domain capturing support for daytime activities, including educational needs. In addition, parents emphasised the need for support with care coordination. As care coordination was frequently described in the open-text field of the assessment tool, this suggests that parents did not perceive the existing domains as adequately capturing this area. Given that care coordination is a well-documented unmet support need among parents of children receiving palliative care,6,25–27 we propose refining the assessment tool to also include a dedicated domain on care coordination support. Such adaptations would help ensure that the assessment tool more fully captures parental needs not addressed by the current domains.
Parental evaluations overall indicated that the intervention was generally acceptable, suitable and well-received, consistent with the findings of a previous Australian feasibility study of the CSNAT-I Paediatric, which found that parents valued the systematic approach for facilitating conversations about their needs, priorities, and potential solutions. 10 In the parental evaluations, parents reported high satisfaction with the CSNAT-I Paediatric and the involvement and communication with competent professionals. This suggests that the intervention is a valuable component of care, as it provides protected time to reflect on and articulate needs. This process may offer support, validation and insight, which directly contribute to parents’ well-being, thereby benefiting the child. 28
Parents’ support needs identified in this study varied considerably across the domains of the assessment tool. Although not prioritised among the top three support needs, those related to relationships with a spouse or partner and to beliefs or spiritual concerns were discussed in several assessment conversations, showing that all the domains are relevant for this group of parents. This finding is consistent with previous research demonstrating the diversity of needs within this population.6,27,29 CPC is generally more complex than adult palliative care because children often have rare, long-term and fluctuating conditions, which create a wide range of evolving family needs. 30 These needs often span many years and require coordinated input from multiple sectors and levels of care, including specialist healthcare, community services, social care and education. The breadth, duration and cross-sector involvement create a level of complexity that typically exceeds that seen in adult palliative care.30,31 Therefore, assessment of parental support needs in CPC requires a broad range of relevant domains to adequately capture the needs of all family members and support a holistic, family-centred approach.
From the providers’ perspective, CCs reported that the CSNAT-I Paediatric provided structure to their work and facilitated prioritising parents’ support needs, reflecting clear demand for such an intervention. They emphasised that CPC expertise among providers of the intervention is essential for exploring parental needs in depth and determining which professionals are best placed to address them. The CCs also emphasised the importance of establishing a safe and trusting relationship between providers and parents, and of carefully considering when and to whom to introduce the CSNAT-I Paediatric. Previous studies have identified both CPC expertise and relational safety as key factors in delivering high-quality CPC,32–34 underscoring our findings.
The duration of the CSNAT-I Paediatric process varied from a few weeks to several months, reflecting differences in parents’ prioritised support needs and the actions required to address them. Some needs could be addressed promptly, depending on the content of the action plan, whereas others required longer timeframes, particularly when multiple stakeholders were involved. The feasibility and timing of the intervention were influenced by the nature of the prioritised needs, the stakeholders involved, and the expected time required for implementation. Consistent with previous research, communication and collaboration across sectors remain challenging within CPC,34–37 highlighting the need for improved coordination between specialist and community-based services.
In light of these findings, the CSNAT-I Paediatric may provide a valuable starting point for joint efforts to address parents’ support needs. Such processes require careful planning and adequate time, as mapping needs without subsequent action could be ethically problematic. Successful integration therefore depends on having enough time and effective coordination and collaboration across sectors. Future research should focus on optimising communication and streamlining the process of assessing and addressing parents’ support needs, ensuring that structured interventions such as the CSNAT-I Paediatric lead to meaningful action and improved support for families.
Strengths and limitations
A strength of this study is that it sheds light on the support needs of parents of children with severe neurological impairment, including neurometabolic conditions, which are often underrepresented in research compared to cancer. This addresses a knowledge gap identified in previous research on the intervention. 17 In our study, participation was nearly equal between fathers (47%) and mothers (53%), reflecting a relatively high level of father participation compared with other studies. 38 It is important to assess the support needs of all parental caregivers to ensure a comprehensive understanding of needs within CPC, as fathers may have support needs that differ from those of mothers within CPC.38,39 Involving both parents in assessment conversations appears particularly important, as this fosters mutual understanding and helps to ensure that the intervention responds equitably to all caregivers’ needs.
This study was limited to parents who were native or long-term Norwegian speakers, which may have resulted in the perspectives and support needs of parents from other cultural and linguistic backgrounds being overlooked. However, this was necessary to ensure that the wording of the assessment tool could be adequately evaluated for sensitivity, clarity, and relevance by individuals with strong proficiency in Norwegian.
With a consecutive enrolment design, the study sample included parents of children aged 5–16 years, with no representation of parents of children aged 0–5 years. This limits the generalisability of the findings to families of younger children and highlights the need for future studies to examine the applicability of the intervention in this age group.
We used self-developed interview guides that were not pilot tested prior to the study. The two qualitative components of the study employed different interview formats with distinct purposes, which partly informed this decision. The cognitive interviews with parents were brief think-aloud sessions focusing on their recent experiences with the assessment tool and assessment conversation, where flexibility and participant-driven reflection were prioritised over a highly structured interview flow. In contrast, the focus group interviews with intervention providers were not time-limited and were designed to allow participants to raise perspectives beyond those explicitly covered in the interview guide, thereby reducing the risk that the lack of pilot testing would constrain data richness.
This study was designed to examine selected domains of feasibility, including acceptability, demand, adaption, practicality, implementation and integration. It was not designed to assess efficacy; therefore, no hypothesis testing, sample size calculation, or power analysis was undertaken. The small sample sizes limit generalisability and prevent statistical inference beyond the study sample.
Conclusion
By using multiple methods to assess intervention feasibility, this study suggests that the CSNAT-I Paediatric is both acceptable and feasible within a Norwegian CPC context. However, successful implementation require sufficient time, consistent follow-up, and cross-sectoral coordination to ensure that parents’ support needs are adequately addressed. Practical and structural challenges remain, particularly regarding integration across services and follow-up of identified needs. The complex and long-term needs of parents of children with severe neurological and neurometabolic conditions highlight the importance of systematically assessing and addressing parental support needs within CPC.
These findings support the implementation of the CSNAT-I Paediatric in new contexts and contribute to the ongoing development of structured, family-centred approaches in CPC.
Supplemental material
Supplemental material - Tailoring support for parents of children in palliative care: Feasibility of the carer support needs assessment tool intervention paediatric in a Norwegian context
Supplemental material for Tailoring support for parents of children in palliative care: Feasibility of the carer support needs assessment tool intervention paediatric in a Norwegian context by Gro Trae, Anette Winger, Marianne Nordstrøm in Palliative Care and Social Practice
Supplemental material
Supplemental material - Tailoring support for parents of children in palliative care: Feasibility of the carer support needs assessment tool intervention paediatric in a Norwegian context
Supplemental material for Tailoring support for parents of children in palliative care: Feasibility of the carer support needs assessment tool intervention paediatric in a Norwegian context by Gro Trae, Anette Winger, Marianne Nordstrøm in Palliative Care and Social Practice
Supplemental material
Supplemental material - Tailoring support for parents of children in palliative care: Feasibility of the carer support needs assessment tool intervention paediatric in a Norwegian context
Supplemental material for Tailoring support for parents of children in palliative care: Feasibility of the carer support needs assessment tool intervention paediatric in a Norwegian context by Gro Trae, Anette Winger, Marianne Nordstrøm in Palliative Care and Social Practice
Footnotes
Acknowledgements
We sincerely thank all the parents and professionals who participated in our study. We also thank the User Panel and Advisory Board of Leve NÅ — Paediatric Palliative Care Unit for their valuable insights and discussions on the research topic.
Ethical considerations
The study was submitted for assessment to the Regional Committees for Medical and Health Research Ethics (REK). Following review, REK concluded that the project did not fall within the scope of formal ethical approval requirements. Data protection was ensured in accordance with the General Data Protection Regulation. The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki.
Consent to participate
Sikt, the Norwegian Agency for Shared Services in Education and Research, has confirmed that the study complies with the Personal Data Act (Reference number 203705). In accordance with Sikt guidelines, all parents provided oral or written consent before participation, where at least one of the child’s parents provided written consent to allow for access to the child’s medical record.
Authors contributions
MN and AW jointly planned the study. GT and MN conducted the assessment conversations with parents. GT conducted and analysed the focus group interview with care coordinators and performed descriptive analyses. GT drafted the manuscript, prepared it for submission and responded to reviewers’ comments, with support from MN and AW. MN and AW provided intellectual input on earlier drafts and critically revised and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Norwegian Directorate of Health funded the study, funding number 10258. The authors were free to choose the research topic, and all views expressed are their own.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are not publicly available due to privacy and confidentiality restrictions. Access to these data can be requested from the corresponding author, subject to reasonable justification and approval.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.