
Abstract
We present the case of a patient with chest pain whose history suggested vasospastic angina. Despite the absence of ischemic electrocardiographic changes, the patient underwent coronary angiography, which showed no atherosclerotic lesions but a diffuse stenosis of the right coronary artery that was resolved promptly by intracoronary nitrate injection, therefore confirming spasm. Angiography also showed a straight vessel in the posterior atrioventricular sulcus, which was recognized as an intercoronary communication that connected the right coronary artery with the left circumflex artery and enabled bidirectional flow. The intercoronary communication likely served to partially protect the right coronary artery-dependent myocardium from ischemia during spasm. This case highlights the significance of a detailed history in constructing an investigation plan in order to make the correct diagnosis. By precluding concurrent ischemic electrocardiographic changes, the intercoronary communication made the diagnosis more challenging.
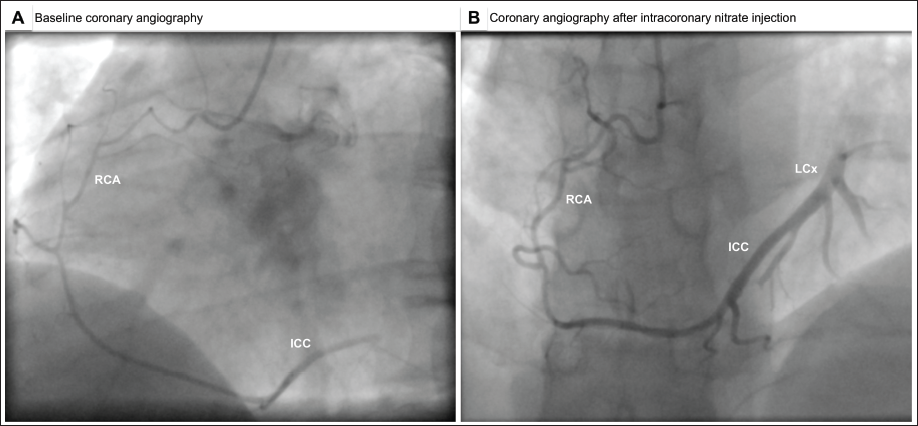
A 31-year-old man was admitted in the early morning hours to the emergency department after experiencing unprovoked, substernal, pressure-like chest pain and left arm numbness recognized as angina. He denied having acid reflux or dysphagia, which often present with symptoms similar to angina. He had neither a viral respiratory nor gastrointestinal infection prodrome that could have raised the suspicion of peri- and/or myocarditis. Furthermore, on admission, he was afebrile, with nothing remarkable on physical examination. He was a heavy smoker and had a paternal history of sudden cardiac death due to coronary heart disease and a maternal history of coronary artery disease (CAD) at the age of 33 years. He denied any alcohol or illicit drug use and reported having experienced two previous similar, but less intense, episodes of chest pain during the past month, also during the early morning hours. His pain was promptly relieved by sublingual nitroglycerin. The electrocardiogram (ECG) taken while the patient was experiencing angina revealed no evidence of ischemia. Neither did subsequent ECGs recorded after the resolution of chest pain show any evolutionary changes consistent with myocardial ischemia. Echocardiography was also unremarkable. Serum levels of troponin remained within normal limits. Because of a strong family history of CAD and a smoking habit, our patient was considered to be at high risk for acute coronary syndrome. Also, our patient presented with spontaneous, nitrate-responsive rest angina early in the morning, therefore raising suspicion of vasospastic angina. Accordingly, we refrained from subjecting our patient to any noninvasive functional tests and performed invasive coronary angiography instead. Angiography revealed no atherosclerotic CAD of the left coronary artery system but a diffuse stenosis of the right coronary artery (RCA) (Figure 1A and Video 1 in the supplemental file). The patient did not complain of chest pain during RCA angiography, nor did the ECG show ischemic changes. The stenosis was resolved promptly by intracoronary nitrate injection, confirming spasm. If the spastic stenosis had been caused by the catheter, it would have been discrete, concentric, and located at the tip of the catheter. However, the stenosis started at least 10 mm distal to the tip of the catheter in the proximal segment and extended into most of the mid-segment of the RCA, favoring a nontraumatic, spontaneous origin, therefore, further strengthening the suspicion of vasospastic angina. Angiography of the RCA also showed retrograde opacification of the distal part of a dominant left circumflex (LCx) artery (Figure 1B; Videos 2 and 3 in the supplemental file) through a large, straight connecting vessel. Retrograde opacification of the distal RCA from the distal LCx artery through the same connecting vessel was also shown (Video 4 in the supplemental file). The patient was discharged home on a calcium channel blocker and remained asymptomatic at a 6-month follow-up.
Conventional Angiography Images. (A) Left Anterior Oblique View Displaying Diffuse Spasm of the Right Coronary Artery (RCA) and Retrograde Faint Opacification of the Distal Left Circumflex (LCx) Artery via the Intercoronary Communication (ICC) That is Formed by a Large-sized, Single, Straight Vessel Coursing in the Posterior Atrioventricular Sulcus. (B) Anteroposterior Cranial View Displaying Resolution of RCA Spasm and Retrograde Full Opacification of the Distal LCx Artery via the ICC.
Intercoronary communication is a rare congenital anomaly comprising a large-sized (≥1 mm), single vessel with a rectilinear trajectory and histologic appearance typical of an epicardial coronary artery that courses either in the posterior atrioventricular sulcus connecting the RCA with the LCx artery, as in this patient, or in the distal interventricular sulcus connecting the left anterior descending artery with the posterior descending artery. 1 Depending on the presence of bidirectional or unidirectional flow, ICC may protect the myocardium from ischemia or lead to myocardial ischemia secondary to a coronary steal phenomenon, respectively.2, 3 Our patient’s history was highly suspicious of vasospastic angina, and the ICC, which enabled bidirectional blood flow, likely served to partially protect the RCA-dependent myocardium from ischemia during spasm. This case highlights the significance of a detailed history in constructing an investigation plan in order to make the correct diagnosis. By precluding concurrent ischemic ECG changes, the ICC made the diagnosis more challenging.
Data Availability
The data underlying this article are available in the article and in its online supplementary material.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The author is accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee(s) and with the Helsinki Declaration (as revised in 2013).
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
The author confirms that witnessed verbal consent for the submission and publication of this case report, including images and associated text, has been obtained from the patient. The information provided in the article has been sufficiently anonymized to ensure that the patient cannot be recognized by themselves or others.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.