
Abstract
Background
Silent atrial fibrillation is a common problem that often goes undetected, owing to its asymptomatic presentation. Electrocardiography is utilized to diagnose subclinical atrial fibrillation; however, it is limited by its reliance on human interpretation. To overcome this limitation, artificial intelligence has recently been integrated into the conventional electrocardiogram, facilitating earlier and more precise detection.
Objective
This review analytically discusses the current literature associated with the advantages and drawbacks of artificial intelligence in electrocardiography, providing insight into the algorithms, practical applications, and overall effectiveness as an alternative to the standard 12-lead electrocardiogram.
Results
Artificial intelligence-enhanced electrocardiography has displayed consistently promising results from its high sensitivity and specificity in detecting asymptomatic atrial fibrillation, as evidenced by its clinical validation and real-world applications. Neural network-based models detecting subtle waveform abnormalities have shown a more accurate interpretation of an electrocardiogram than a typical physician and potential integration with wearable devices to support real-time monitoring. However, significant barriers remain, including systemic algorithmic bias related to age, sex, and race, as well as certain technical limitations.
Conclusion
The use of artificial intelligence in electrocardiography demonstrates a strong potential for improving silent atrial fibrillation detection and providing timely intervention. While artificial intelligence is highly efficient for early intervention, it is currently best utilized as a clinical addition rather than a replacement for traditional care. Finally, the clinical utility of these models needs to be solidified by prospective randomized controlled trials to further establish their impact.
Keywords
Introduction
Atrial fibrillation (AF) is the most common cardiac arrhythmia and it represents a growing health burden associated with increased risks of strokes, heart failure, and mortality. 1 Strokes caused by AF are more severe; yet this risk can be mitigated by appropriate anticoagulation therapy, making early detection a clinical priority. 2 Approximately one-third of AF patients remain asymptomatic, 3 a condition termed silent atrial fibrillation (SAF) that frequently evades clinical detection until a thromboembolic event occurs. In line with existing literature, this study defines asymptomatic AF as the known AF in patients who possess no symptoms, or have a European Heart Rhythm Association score of 1, 4 while the subclinical asymptomatic episodes of paroxysmal AF that are detected incidentally by monitoring devices and confirmed using electrogram and electrocardiogram (ECG) are known as SAF.5, 6
Traditional ECG relies mainly on human interpretation, which introduces diagnostic gaps. Misplacement of limb or precordial leads, inadequate filtering, or artifact from patient movement can mimic pathological findings and lead to false results, including pseudo-infarction, bundle branch blocks, or abnormal axis deviation. 7 Doctors from different levels commonly misinterpret ECG, achieving an accuracy of 54% and improving only to 67% after training. 8 Additionally, the need for frequent monitoring and review by a cardiologist poses a drawback, with higher chances of misdiagnosis by physicians. In comparison, automated software using a 12-lead ECG is of greater specificity. 9 Interobserver variability and misdiagnosis remain persistent problems, with one study revealing that 5 out of 900 weekly ECG readings had wrong interpretations related to AF made by physicians and computer algorithms, leading to unnecessary medical treatments.10, 11 A large prospective multicenter study on stroke and transient ischemic attack survivors suggests that 72-h Holter ECG monitoring improves diagnosis of silent paroxysmal AF at a low cost; however, more than 24-h Holter monitoring is time-consuming for medical staff and uncomfortable for patients.12, 13 The current standard of care for detection has therefore proven to be inadequate for capturing paroxysmal, asymptomatic episodes of AF; catalyzing the search for a more reliable and accurate solution.
Artificial intelligence (AI) possesses the capability to modernize AF care, to transition from reactive treatment to a proactive approach, providing personalized management. 14 Asymptomatic episodes of AF can be detected by monitoring devices, such as intracardiac, implantable, or wearable devices, and are confirmed using electrogram and ECG.5, 6 Neural network-based models, namely, deep learning (DL) and Convolutional Neural Networks (CNNs), have illustrated diagnostic precision surpassing that of skilled physicians. 15
Artificial intelligence-enhanced ECG analysis offers a practical and affordable approach to early detection and personalized treatment. This review aims to critically appraise the current literature on the advantages and limitations of AI in diagnosing SAF and to assess its effectiveness as an alternative to traditional diagnostic methods. By synthesizing findings from key studies, it aims to clarify whether artificial intelligence-electrocardiogram (AI-ECG) represents a viable alternative or a complement to traditional diagnostic methods and to help identify directions for future research.
Technological Evolution: From Convolutional Neural Networks to Multimodal Large Language Models
Artificial intelligence refers to computer automation that enables machines to analyze and respond to information, demonstrating adaptation through pattern recognition. 16 In cardiology, AI-based diagnostics facilitate precise prediction and risk stratification, potentially relieving cardiologists of the burden of manual evaluation while improving patient outcomes through personalized therapeutic strategy adaptation and dynamic risk assessment. 17
The practical value of this technology is illustrated by Kashou et al., 18 who reported a case wherein a 92-year-old woman suffered from recurrent cryptogenic strokes over several years despite a lack of history of AF or other heart conditions. While a standard 12-lead ECG showed a normal sinus rhythm, an analysis by AI-ECG revealed a forewarning risk of AF, 12 years before the first thromboembolic event. Subsequent monitoring confirmed atrial flutter with variable atrioventricular block, demonstrating that AI-ECG can identify silent pathologies during sinus rhythm that can evade traditional human interpretation. It offers critical insights into undiagnosed AF, which may contribute to earlier interventions and to help prevent recurrent strokes.
The predictive capability of AI-ECG was validated in a seminal study by Attia et al. by training a CNN on 649,931 sinus rhythm ECGs from 180,922 patients. The study demonstrated that a single AI-enabled ECG could predict incident AF with an area under the curve (AUC) of 0.87 and overall accuracy of 79.4%, improving to 0.90 and 83.3% when multiple ECGs were analyzed. 19 Both the AI-ECG and traditional CHARGE-AF (Cohorts for Aging and Research in Genomic Epidemiology-AF) score were able to independently predict who would later develop AF. Patients flagged as high risk by AI-ECG showed a 21.5% chance of AF within 2 years and more than 50% risk within 10 years. The discriminative ability measured by the C-statistic was 0.69 for both AI-ECG and CHARGE-AF, and their combination yielded 0.72. Unlike CHARGE-AF, which requires clinical data, AI-ECG needs a single ECG recording without any additional information, which can help find any risk. 20
Recent advancements have introduced multimodal large language models (LLMs) into the field, such as the ECG-LM model that transforms raw ECG signals into a high-dimensional feature space and aligns it with a textual feature space from the LLM.21, 22 Studies by Yang et al. have found that these models outperform existing solutions in cardiovascular disease detection in terms of diagnosis, rhythm, and form, allowing users to have a better insight and serving as a sophisticated preliminary interpretation assistant for medical professionals. 21 Another multimodal LLM is ECG-Chat, which accounts for subtle variations between ECG waveforms and cardiology reports. 23 The incorporation of such LLMs has allowed for the detection of intricate patterns and subtle relationships in ECG. 24 By leveraging this multi-layered architecture, cardiology is successfully shifting from a treatment-focused to a predictive and preventative care, detecting silent pathologies before their manifestations. 25
The efficacy of AI-guided screening has been further determined by a prospective, non-randomized intervention trial where 1,003 individuals at risk of stroke without a prior AF diagnosis underwent AI-assisted screening, and were associated with higher rates of AF detection. Patients were monitored for 30 days using a continuous ambulatory heart rhythm monitor and classified into high-risk and low-risk stroke groups, which led to the detection of AF in 48 out of 633 high-risk patients and 6 out of 370 low-risk patients. 26
Technically, the field distinguishes between machine learning (ML) and its more complex subset, DL. Traditional ML consists of supervised, unsupervised, and reinforcement learning, relying on iterative pattern detection based on human-defined rules.16, 27 However, ML is constrained by these human definitions, leading to potential misdiagnosis when differentiating the fine ECG variations. 28 In contrast, DL uses hierarchical layers to derive features from data, allowing end-to-end learning without manually engineered features.29, 30 A survey conducted from 2017 to 2023 proves a superior performance of DL used in ECG arrhythmia detection, surpassing traditional ML approaches. 31 Recent comparative studies show that while DL models like InceptionTime were found to achieve similar accuracy to ML algorithms like XGBoost; they offer lower cost, greater stability, and improved interpretability, making them highly valuable for real-world healthcare applications. 32
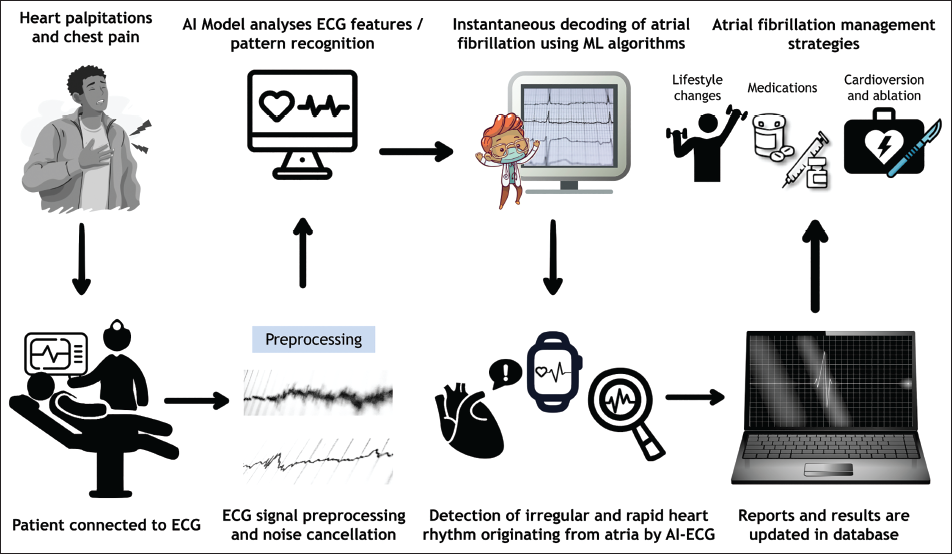
The extraction of key features from ECG is primarily achieved through CNNs. These networks utilize various layers, like the convolutional, activation, pooling, and fully connected layers, to amplify essential features of the ECG waveform while eliminating irrelevant noise.33-35 This allows for the precise analysis of the P, QRS complex, T, and U waves representing atrial depolarization, ventricular depolarization, and repolarization, respectively, which serve as an input. 36 In fact, a recently proposed DENS-ECG model now combines the CNN with long short-term memory (LSTM) to detect the onset, peak, and offset of the different waveforms. 37 A number of studies have shown that CNNs are particularly effective at identifying local patterns, such as ST-segment changes and QRS complex morphology; for instance, studies by Makimoto et al. observed that CNNs focused strongly on the ST-T elevation in an ECG of myocardial infarction (MI) cases, whereas in non-MI cases, it concentrate primarily on the area from the QRS complexes to the ST-T segment.37, 38 Figure 1 illustrates the stepwise process of AF detection using AI-ECG.
Clinical Validation and Real-world Application
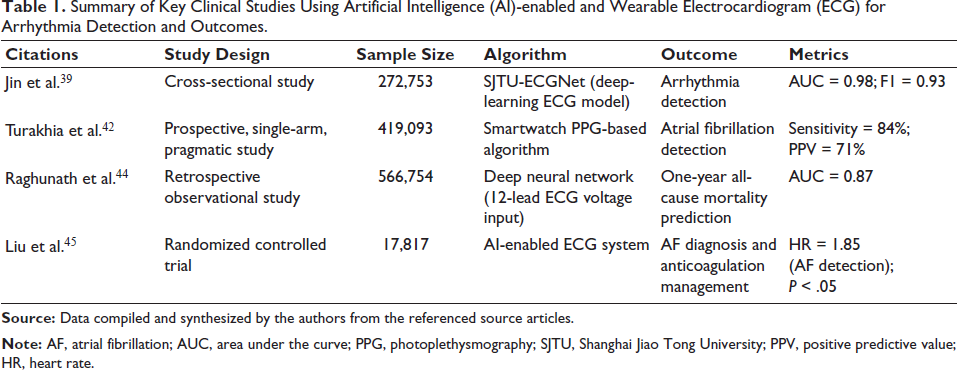
The clinical validation of DL models has portrayed diagnostic precision that frequently matches or exceeds that of clinicians. Jin et al. introduced Shanghai Jiao Tong University (SJTU)-ECGNet, a DL model designed to identify six common arrhythmias, including AF. It was trained on 352,725 12-lead ECGs from 272,753 patients, achieving a remarkable accuracy of 93.74% and an F1 score of 83.51%. 39 Similarly, Hannun et al. developed a 34-layer deep neural network (DNN) from a single-lead ECG, which was trained on 91,232 ECGs from 53,549 patients. It achieved an F1 score of 0.837, significantly surpassing the average cardiologist’s F1 score of 0.780, and was also found to have higher sensitivity across all 12 rhythm types. 40 Further evidence of AI’s scalability is found in the work of Ribeiro et al., whose end-to-end DNN model was trained on over 2 million 12-lead ECGs. This model achieved a specificity greater than 99%, outperforming not only medical students and residents, but also experienced cardiologists, while demonstrating a superior ability to process signal noise. 41
The transition of these algorithms into consumer-based technology was most evident in the Apple Heart Study. 42 This prospective, single-arm, pragmatic study utilized the Apple Watch irregular rhythm notification (IRN) to detect AF in a large-scale population. While the IRN demonstrated a low rate of false positives and high accuracy for identifying previously asymptomatic AF, its sensitivity for detecting specific individual AF episodes was notably lower. These findings suggest that while the wearable devices are highly effective for broad population screening, further improvements in sensitivity and in wear time are needed to move these devices from screening tools to disease management instruments. 43
Beyond simple diagnosis, AI-ECG also serves as a strong risk marker for mortality prediction. Raghunath et al. utilized a DNN model trained on 1.77 million 12-lead ECGs to predict 1-year all-cause mortality with high precision, attaining an AUC of 0.83. In a blinded comparison, the AI categorized patients as high- or low-risk, outperforming cardiologists, whose accuracy in predicting survival based on the same ECGs was estimated at just 55%-68%. 44 This study signifies the importance of AI in capturing subtle physiological patterns linked to survival risk that remain invisible to the human eye, shifting its role from a diagnostic alternative to a revolutionary tool for long-term risk stratification.
AI-ECG also plays an essential role in narrowing the diagnostic gap between specialists. This was demonstrated by Liu et al. in a randomized trial, where noncardiologists equipped with AI-ECG alerts (intervention group) achieved higher rates of AF diagnosis and oral anticoagulant prescriptions than those without (control group) in Taiwan, China. This suggests that AI-enabled ECGs can reduce the disparity in AF quality care between cardiologists and non-cardiologists; however, several limitations were found in this study including the limited sample size, lack of comparison with commercial software, the failure of clinicians to act on the AI alerts, and the high persistent misdiagnosis rates—55.1% in the intervention group compared to 68.6% in the control group. 45 These findings highlight that while AI can standardize care, organizational barriers and a lack of follow-through remain as the main hurdles.
The economic advantage of these systems is further supported by cost-effective analyses. Models detecting AF in ischemic stroke patients enable early diagnosis and secondary prevention, 46 while mobile health-based AF screening for high-risk individuals (CHA₂DS₂-VASc ≥4) prevents a marked number of strokes and deaths, with a favorable cost per prevented stroke for 10 years. 47 Furthermore, a randomized trial has tested AI-enabled ECG alert systems and showed improvement in 90-day all-cause mortality with no notable increase in healthcare costs, which suggests cost-effective benefits. 48 Continuous mobile ECG monitoring in post-stroke patients also increases AF detection, which in turn aids in recurrent stroke prevention, proving to be cost-effective. 49
Finally, technical advancements continue to push the boundaries of detection with ML models achieving an accuracy of more than 95%, as evidenced by several studies.50-52 Models such as the Graph Hybrid-Multi-scale-CNN presented by Zhang et al. for binary AF classification have reported a mean accuracy of 0.9984, precision of 0.9989, and F1 of 0.9954. 50 Similarly, CNN-LSTM-based model and CNN-BiLSTM model have demonstrated near perfect identification rates for paroxysmal AF, reaching an accuracy of 97.99% for CNN-LSTM and 99.79% for CNNs-BiLSTM. A summary of key studies evaluating AI-enabled and wearable ECG technologies for the detection of AF is presented in Table 1.51, 52
Summary of Key Clinical Studies Using Artificial Intelligence (AI)-enabled and Wearable Electrocardiogram (ECG) for Arrhythmia Detection and Outcomes.
Challenges and Limitations
While AI-ECG has shown remarkable progress, it is not without its challenges. AI-based ECG algorithms organize and manage large datasets, but encounter challenges in developing generalized, interpretable, and user-focused solutions. 53 A primary concern is algorithmic bias, which is a systemic deviation in algorithm output, performance, or impact related to a norm or standard. 54 Such biases often arise when the AI-ECG models prioritize diagnostic accuracy over demographic inclusivity, placing underrepresented groups (age, sex, or race) at a disadvantage in receiving an accurate clinical diagnosis. Empirical evidence highlights a sex bias, with men frequently attaining a higher score in automated arrhythmia detectors when compared with women.54, 55 Similarly, racial disparities persist; while epidemiological data place Black Americans at a higher risk for cardiovascular conditions, including AF, systemic bias in model training fails to account for their unique physiological risk factors.56, 57
Adding to these challenges are the limitations in technological hardware. Many wearable devices utilize photoplethysmography (PPG) technology, which detects changes in heart rate and blood flow using photodetectors and light-emitting diodes that absorb green light with a high absorption spectrum. However, they limit light penetration by melanin in dark-skinned individuals, leading to inaccurate readings. This creates a “technological bias” where its systematic process of excluding the black population could result in inaccurate and undetected AF in the Black population, further widening healthcare inequities.58-60 This systemic bias often results from overrepresentation of a majority class, leading to model bias, incomplete data for the minority groups, causing model variance, and outcome noise due to the undesirable impact of unobserved variables. 61 Patient selection bias can also influence the generalizability of the model, as the features presented in the ECG usually differ between races. 62
Beyond demographic bias, the standardization and integrity of data prove to be a major hurdle. AI-ECG interpretation is often limited by inconsistent storage formats, incomplete data, noise, and ambiguity, which collectively reduce diagnostic accuracy. 61 When algorithms are trained on nonrepresentative datasets, they are prone to produce false positives and negatives, failing to perform consistently across different groups. 63 While DL approaches have demonstrated a 93% capacity to differentiate high-quality signals from noise, they still misqualify approximately 5% of clean AF segments as “noisy”. 64 Correspondingly, ArNet2, which is a DL model that worked across various groups, has also shown differences in terms of accuracy, underscoring the ongoing challenge of creating a universal diagnostic tool. 65
Health information exchange (HIE), which shares patient data to improve the efficiency and effectiveness of healthcare, is giving rise to privacy concerns affecting patients’ candor in their therapeutic patient-provider relationship. Although public education and engagement could build trust and change perspectives on HIE, it is still not well understood and overestimated by the healthcare community. 66
Another challenge in the application of AI in the health care system is the “black box” problem characterized by the opacity and lack of interpretability. 67 This inadequate transparency is caused by the inability to trace or provide reasoning behind the outputs impedes trust and accountability. 68 It poses a test of the critical thinking and decision-making ability of healthcare professionals as AI gives recommendations with no supporting information, leading to over-reliance without critical assessment or underutilization, wherein there is a decrease and hesitance with the use of DL tools. 69 Chan 70 argued that black boxes undermine physicians’ care to patients, as they take away their ability to comprehend, and it provides limited insight into how predictions are made from the ECG input data. 71
The integration of AI-based ECG analysis into existing clinical workflows and electronic health records (EHRs) encounters multiple obstacles due to the technical and organizational barriers, such as scattered data assets, inconsistency in data formats, and the proprietary status of many ECG devices and hospital systems.72-74 Furthermore, there are also data privacy and security concerns associated with processing personal ECG data on large scales, as ECG signals are considered biometric identifiers and attributors, which make anonymization extremely complex. Current frameworks reveal a difficult trade-off: anonymization methods are becoming critical to protect privacy, yet minimizing clinical utility. 75 The centralization of sensitive health data in cloud environments further adds to the risk of technical failure, like cyberattacks and data theft, resulting in an increase in risks, loss of control, and network threats of data exposure. 76
To address these risks, international regulatory bodies have established stringent requirements for AI/ML-based software as a medical device. The US Food and Drug Administration necessitates that AI-integrated devices undergo rigorous real-world screening followed by a postmarketing surveillance. 77 Similarly, an AI Act, proposed by the European Commission, mentions that healthcare AI systems, including AI-ECG, are considered high-risk and require strict compliance with transparency, risk management, and data governance standards. 78 Ethically, when AI tools provide predictions without clear medical interventions, the technology may shift from a diagnostic benefit to a psychological and emotional burden for the patient. 79
Ultimately, while primary decision-making remains the responsibility of the clinical professionals, the escalating complexity of AI tools undermines traditional systems of accountability. The absence of clear legal and ethical guidelines creates significant uncertainty regarding liability, specifically whether it resides with the software developers, healthcare facilities, or individual providers.61, 80
Future Directions
Future AI models in cardiology should be designed in a way that is fair and inclusive, ensuring that data curation and algorithmic design are optimized for real-world clinical application. A significant disadvantage of current models is the exclusion of specific individuals due to sparse data, resulting in biased and unfair results. To address this issue, strategies such as data augmentation are being utilized to add diversity to the data, thereby improving the generalizability of AI-ECG tools across the population. 81
The application of transparent reporting standards is essential for building clinician trust and ensuring the reproducibility of AI-ECG performance. They are a set of frameworks that mandate comprehensive documentation regarding data collection protocols, and describing the model’s code, training settings, datasets, features, and predictions. Such transparency is the cornerstone of fairness-aware interpretable modeling (FAIM), an approach that optimizes model fairness without compromising diagnostic precision. As tested by Liu et al., FAIM utilizes a variety of models relying on different features to prioritize selection based on sensitive features like race or sex, giving precedence to pick the fair and most accurate model. FAIM also uses AI to explain the changes and choices to clinicians, facilitating informed decision-making among clinicians and developers. 82
For the acceptance and integration of medical AI into clinical practice, explainable AI (XAI) is considered vital because it offers insights into how predictions and outcomes are made through global and local explanations.83, 84 By offering clarity and identifying trends, XAI serves as a direct solution to the “black box” problem that otherwise impedes clinician trust and accountability. 84 To achieve adequate interpretations, XAI approaches known as ante hoc, beginning with an understandable model, and post hoc, posttraining black box model, are applied. Local Interpretable Model-agonistic Explanations and Gradient-weighted Class Activation Mapping (Grad-CAM), which approximate the behavior of a complex model, are some of the examples of post hoc XAI techniques that make black box AI more interpretable. 85
In ECG analysis, these methods, along with saliency maps, emphasize key diagnostic features within the ECG waveform. While saliency maps and Grad-CAM are used by CNN to infer its class labels, producing a map of weights,86-88 another technique called SHAP (Shapley Additive Explanations) calculates an additive importance score for each prediction by showing both the weight and direction of the impact of a feature on the potential outcome. 89 For instance, in a study by She et al., 90 it was demonstrated how SHAP could quantify the contribution of clinical markers, like maximum P wave duration and augmented vector right/first precordial lead (V1), to AF risk prediction, thus contributing to the decision-making process. Despite its benefits, multiple studies have found that a comprehensive approach integrating multiple XAI methods is still necessary, as ECG heatmap explanations themselves remain inadequate. 86
The clinical acceptance and trust of clinicians in XAI varies, as observed by Rosenbacke et al., 91 showing that out of 10 analyzed studies, five reported that XAI increased trust, two observed that it both increased and decreased trust levels, two noted that no effects of XAI were shown, and one did not reach any conclusion. Despite this variance, XAI helps bridge the gap of complexity generally faced in AI by improving the confidence among patients and doctors, as well as meeting regulatory transparency requirements. 92 For instance, the application of Grad-CAM in Holter ECG monitoring has demonstrated practical value by highlighting specific signal features such as irregular QRS complexes and the absence of P-waves, which distinguish AF from normal sinus rhythm, thereby providing the needed transparency for clinical interpretability.93, 94
Beyond interpretability, the future of AI-ECG integration necessitates a commitment to continuous equity audits, which must be conducted during and after the development of AI models to ensure fair performance across diverse patient groups. However, researchers warn that individuals should not rely on it due to its limitations. Instead, it is important to test the model’s work by giving a specific task and getting input from individuals who used the model, such as doctors. 95 Furthermore, to transition from a diagnostic aid to a gold-standard clinical tool, there is a need for a prospective randomized controlled trial to provide strong evidence that using AI-ECG in SAF reduces hospitalization, lowers cardiovascular mortality, and improves outcomes. 96
Future AI models should apply the concept of a multimodal AI to AI-ECG, creating a holistic profile, using echo, cardiac magnetic resonance imaging, genomics, EHR, and wearable devices. 97 There should also be a focus on edge computing, which is a tool utilized in managing bottlenecks in technology, as it enhances latency, decreases transmission of data, minimizes the strain on cloud computing, and improves privacy and security. 98
Ultimately, the evolution of AI-ECG must be governed by ethical guidelines that emphasize the importance of collaboration between humans and AI. AI should not only be able to provide us with fair and accurate outcomes but also with support for right and fair decisions in healthcare practice or settings. 93
Conclusion
Artificial intelligence-electrocardiogram models represent a major turning point in cardiovascular care, transforming the approach to SAF detection from a reactive model to a proactive one. These tools detect silent pathologies during sinus rhythm, years before a clinical thromboembolic event occurs. They are highly efficient, particularly for preventive therapy trials, aiming to treat individuals early before symptoms, marking a shift from traditional care, which, by contrast, starts after the cardiac condition is detected.
For widespread clinical acceptance, and to meet high-risk transparency and regulatory requirements, issues such as “black box” problem, systemic algorithmic bias need to be addressed. Furthermore, techniques such as Grad-CAM and SHAP need to be integrated to provide the reasoning behind AI outputs, thereby building clinician trust and ensuring accountability.
Ultimately, for a more specified and clear result, it would be best to consider AI-ECG as an addition rather than a replacement. While it does have promising potential, its clinical utility must be solidified through prospective randomized trials that could ultimately reduce SAF-related casualties, thereby proving AI-ECG to be a revolutionary component of 21st-century cardiovascular care.
Footnotes
Authors Contribution
HAR: Conceptualization, writing—original draft, writing—review and editing, supervision. IM: Writing—original draft, writing—review and editing. MEBL: Writing—original draft, writing—review and editing. HJM: Writing—original draft, writing—review and editing. DH: Writing—original draft, writing—review and editing. ATMKE: Writing—original draft, writing—review and editing. SH: Writing—original draft. RA: Writing—original draft.
All authors read and approved the submitted version.
Data Availability Statement
Data sharing is not applicable to this article as no new primary datasets were generated or analyzed during the current research. All data and findings presented in this review are available within the cited literature, and their respective references are listed in the bibliography.
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest regarding the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
As this study is a literature review and did not involve the direct recruitment of human participants or the use of animal subjects, formal ethical approval and informed consent were not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.