
Abstract
Background
Individuals with multimorbidity often have complex health and social care needs and experience frequent transitions across various settings and providers, including home, community services, primary care, and hospitals. These transitions represent pivotal moments within their care trajectories, where the risk of care fragmentation is significantly increased. Although these transitions play an important role in shaping patient experiences and outcomes, the factors associated with them remain insufficiently documented.
Objective
This study aimed to identify individual and environmental factors associated with either positive or negative experiences of care transition among individuals with complex needs.
Design
Using a prospective correlational design, participants were recruited from emergency departments at three sites in two Canadian provinces. Eligible individuals had ≥3 ED visits in the past year, screened positive on the COmplex NEeds Case-finding Tool–6 (CONECT-6), and had complex needs confirmed by an INTERMED Self-Assessment (IMSA) score of 19 or higher. Baseline data included sociodemographic, clinical, and psychosocial variables; environmental variables were derived from geocoded postal codes. At six months, participants completed a 12-item scale on care transitions adapted from the Patient Experience of Integrated Care Scale (PEICS). Multivariable linear regression identified factors associated with transition experiences.
Results
Of 292 participants recruited, 167 completed the follow-up. Biopsychosocial complexity, self-management capacity, and recruitment site were significantly associated with transition experiences. Higher complexity was associated with less favorable experiences, while stronger self-management was linked to more positive transitions.
Conclusion
Care transition experiences are associated with biopsychosocial complexity and self-management abilities, with site-level differences point to organizational and systemic influences. Further research is needed to examine how organizational and system-level factors shape transition experiences for individuals with complex needs.
Introduction
The interaction of chronic physical and mental health conditions with factors such as socioeconomic status, cultural background, and environmental context may create complex health and social care needs (hereafter complex needs).1–4 Individuals with complex needs require services across various sectors,5,6 resulting in frequent care transitions between home, community, primary care, and hospital settings. 7 Care transitions are defined as the transfer of responsibility between providers across different settings and sectors, 8 and are critical for care continuity and patient safety. Transitions are events where patients must repeat their health histories, build trust with new providers, and make important decisions about their care. These high-risk moments are particularly prone to gaps or disruptions in care, especially when new diagnoses, treatments, or changes in physical, mental, or social health occur.7,9 Poorly managed transitions can cause emotional and physical distress, delays in timely care, increased morbidity, provider frustration, and avoidable costs due to repeated testing, emergency visits, and hospital readmissions. 10
A mixed-methods study showed that multimorbidity exacerbates the challenges associated with care transitions after hospital discharge, particularly in terms of communication and information sharing among providers, caregivers, and patients. 11 Consistent with these findings, a retrospective cohort study demonstrated that multimorbidity is associated with an increased risk of hospital readmissions among older people receiving post-acute care. 12 Beyond the burden of chronic disease, evidence indicates that self-management ability plays an important role in the success of care transitions.13,14 For example, a systematic review of medication continuity interventions highlighted the importance of self-management activities and coordination tasks as key components of effective care transitions for older people. 15
Psychosocial conditions also appear to significantly influence care transition experiences. A scoping review focusing on patients with cognitive impairment following emergency care found that social isolation and economic deprivation further complicate care transitions. 16 Similarly, a narrative review identified several social vulnerability factors, such as limited access to healthcare, unstable housing, and transportation challenges, as important barriers to smooth transitions of care. 17 Environmental factors may further shape these experiences. A retrospective correlational study demonstrated that disadvantaged neighborhood status is associated with reduced early follow--up and a lower intensity of post discharge care coordination-.
These studies assessed specific dimensions of complexity independently, rather than concomitantly. Moreover, previous research and existing frameworks have tended to focus narrowly on particular types of transitions, primarily those related to hospital discharge or hospital-to-home care. As a result, they often overlooked the broader range of transitions that individuals with intersecting vulnerabilities must navigate across multiple sectors. In addition, much of the available evidence came from geriatric and frailty literature, which concentrated on age-related decline and functional loss.16,18–20 Consequently, there remains limited understanding of how individuals with complex needs across diverse age groups experience multiple care transitions. This study seeks to identify individual and environmental factors associated with the experiences of care transition among individuals with complex needs.
Methods
Study design
This study used a prospective correlational design 21 conducted over a six-month period.
Study sites
Three study sites were purposefully selected
22
across two Canadian provinces to capture a diversity of care transition contexts. Although they were located in urban centers, each served adjacent semi-urban and rural populations
23
: • Site A, a community hospital in the province of Quebec, was part of a healthcare organization serving approximately 440,000 individuals in a dense urban area marked by high newcomer rates, cultural diversity, and socioeconomic deprivation. A small subset of participants (n = 8) was recruited from a nearby hospital affiliated with a different administrative organization. • Site B, also in the province of Quebec, was the main hospital within a health organization serving over 500,000 individuals across a vast 13,000 km2 territory that includes urban, semi-urban, and rural areas. • Site C located in New Brunswick, included two hospitals offering complementary services: a tertiary care hospital serving around 170,000 individuals and a community hospital serving about 10,000. Both facilities also covered surrounding semi-urban and rural regions.
EDs served as entry points for patients’ care transitions. Each site included hospital settings along with community-based, primary care, and private sector services, reflecting the diversity of transitions across geographic contexts. To protect the anonymity of the participating institutions and the geographic recruitment areas, the sources of these data has not been cited.
Recruitment procedure
Identifying patients with complex needs is inherently challenging, as these needs are not defined by a single diagnosis. However, frequent use of health and social services—particularly repeated ED visits—has been recognized as a reliable proxy for identifying this population. 24 From June 2022 to March 2024, trained research assistants were present in EDs in each site several days per week at different times between 7:00 am and 12:00 am.
Sampling of patients with complex needs
Using the EDs information system, patients who had visited the ED three or more times within the previous 12 months were identified. These individuals were initially screened using the COmplex NEeds Case-finding Tool – 6 (CONECT-6). 25 This is a 6-question validated tool with a sensitivity of 90% and a specificity of 66% when using a threshold of two or more positive answers. 25 Individuals who screened positive were then invited to complete the INTERMED Self-Assessment (IMSA), 26 a validated self-report version of the INTERMED questionnaire to assess biopsychosocial complexity needs. The IMSA has demonstrated valid psychometric properties.27–31 A score of 19 or higher on the IMSA confirms the presence of complex needs and was used to determine eligibility for study participation. 32 The study excluded individuals living in long-term- care facilities to focus on ambulatory care transitions, as well as those with cognitive impairment that prevented them from completing the questionnaire independently.
Variables
At the outset, participants completed a series of validated questionnaires assessing a broad range of sociodemographic, clinical, and psychosocial variables. Selection of variables was informed by the literature and research team’s expertise, and all instruments demonstrated good psychometric properties and were available in both English and French. Trained research assistants administered the questionnaires either in person during the waiting time for the participants’ ED visit or by telephone within two weeks of the visit, ensuring flexibility and maximizing response rates: • Sociodemographic characteristics – Age, language, marital status, education, occupation, and income were assessed using items from the Canadian Community Health Survey (CCHS).
33
Sex and gender were assessed using Statistics Canada census questions,
34
while ethnicity, Indigenous identity, and disability were measured using the Tri-Agency Equity and Diversity Questionnaire.
35
• Clinical variables – In addition to the biopsychosocial complexity, substance use was assessed using the 9-item Alcohol, Smoking and Substance Involvement Screening Test (ASSIST),
36
and multimorbidity was evaluated using the 21-item Disease Burden Morbidity Assessment (DBMA).37,38 • Psychosocial variables – Housing satisfaction was assessed with a single item from a validated source,
39
and food security was measured using the U.S. Household Food Security Survey 6-item Short Form.
40
Social support was evaluated using the 8-item Medical Outcomes Study Social Support Survey,
41
health literacy using the 3-item Brief Health Literacy Screening (BHLS) questionnaire,42,43 and self-management using the 12-item Partners in Health Scale (PIH).44,45 • Environmental variables – Environmental variables were mapped across available data sources, also based on the literature and research team’s expertise. They were derived from geospatial data linked to participants’ six-digit postal codes. These included indicators of neighborhood deprivation,46,47 gentrification,
48
marginalization,
49
and accessibility to health facilities50,51 obtained from national databases, including Statistics Canada and Quebec Institute of Statistics.
Six months after enrollment, participants completed a follow-up telephone questionnaire assessing their experience of care transitions (the dependent variable) over the preceding six months. This timeframe was chosen because individuals with complex needs are likely to undergo several transitions over this interval, yet it remains short enough to help limit attrition.52,53 Experience of care transitions was measured using the validated 12-item Patient Experience of Integrated Care Scale (PEICS). 54 The scale was adapted to specifically assess care transitions using a continuous score from 0 to 48, with higher scores indicating a more positive experience. The adaptation consisted solely of rewording all items to explicitly refer to care transitions. One non-applicable item was removed. This process was carried out collaboratively by the research team, including patient partners. To support consistent interpretation, a standardized definition of care transitions was provided prior to questionnaire administration.
Statistical analysis
Descriptive statistics (frequency, percentages, mean, standard deviation – SD) were used to summarize all study variables. Categorical variables were reported as frequencies and percentages, while continuous variables were described using means and standard deviations or medians and interquartile ranges, depending on the distribution of the data. To compare baseline characteristics between participants who continued the 6-month follow up and those who did not, categorical variables were compared using chi-square tests or Fisher’s exact tests. Continuous variables were compared using Student's t-test for normally distributed data or Mann-Whitney’s test to those that were irregularly distributed. To explore associations between the care transitions experience score (dependent variable) and each potential correlates, Spearman’s rank correlation coefficients were calculated. This non-parametric method was chosen due to the presence of non-normally distributed variables and the inclusion of categorical and ordinal data among these potential correlates.
Given the multi-site nature of the study, a linear mixed-effects model with a random intercept for site was initially employed to assess inter-site variability. Since site-level variance in care transition scores was only 2.3%—below the 5% threshold where multilevel modeling offers added value— 55 subsequent analyses were conducted using standard linear regression without random effects. Variables with a p-value < 0.10 in the bivariate Spearman correlation analyses were entered into the multivariable model. Multilevel categorical variables (anxiety and housing satisfaction) were dichotomized based on clinical relevance before being incorporated into the regression model.
In the final multivariable linear regression model, age and sex were included a priori, while the remaining variables were entered using a forward selection approach. Only variables with a p-value < 0.05 were retained in the final model. Multicollinearity was assessed using variance inflation factors, and residual analyses were performed to verify that assumptions of linear regression were met. All statistical analyses were conducted using IBM SPSS Statistics, version 28. At a 5% significance level, a sample size of 117 provided 80% power to detect a medium effect size (R2=0.15) 56 with up to 10 predictors in the final model (G*Power 3.1.9.4). 57
Results
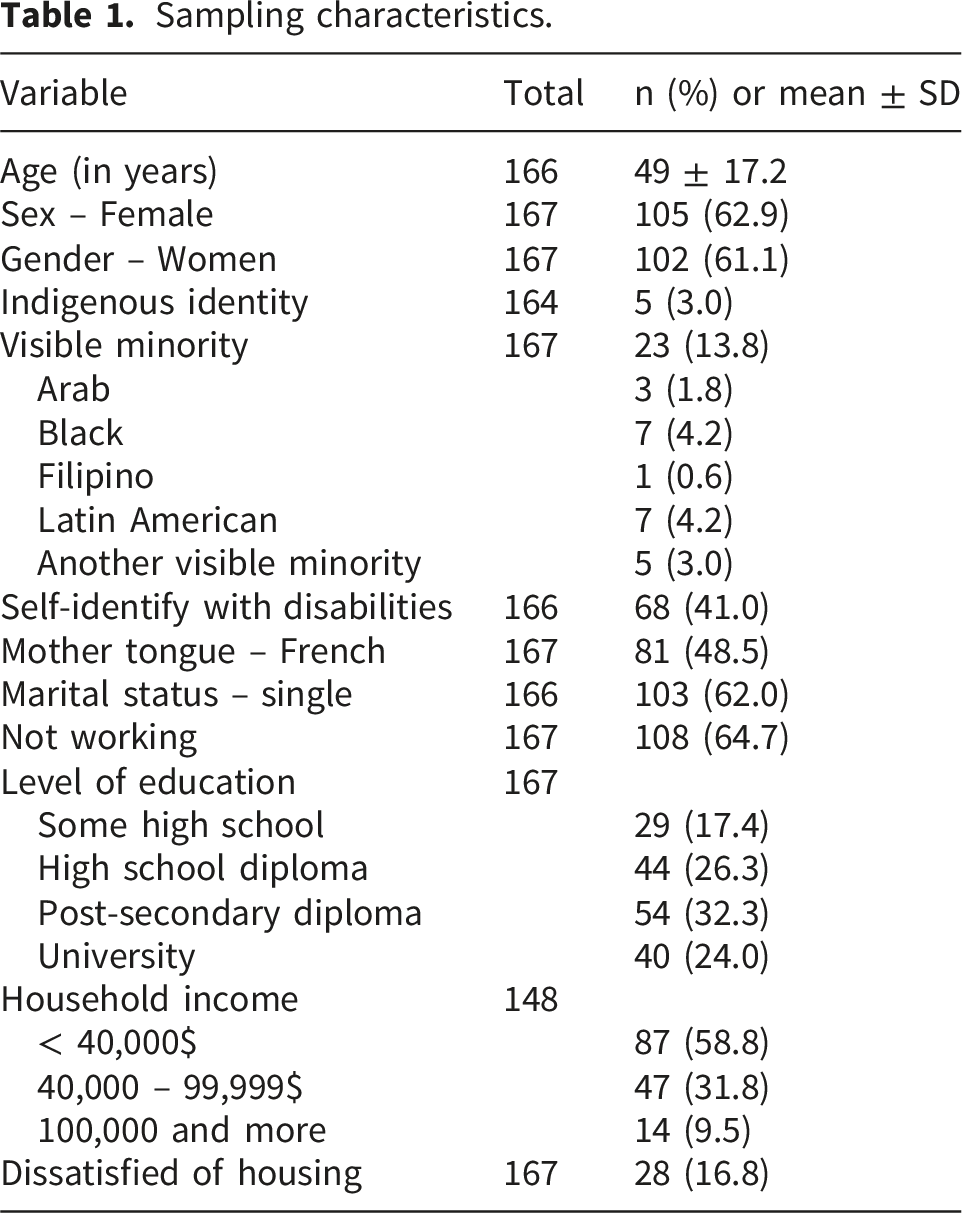
Sampling characteristics.
Correlations with the experience of care transitions (PEICS score).
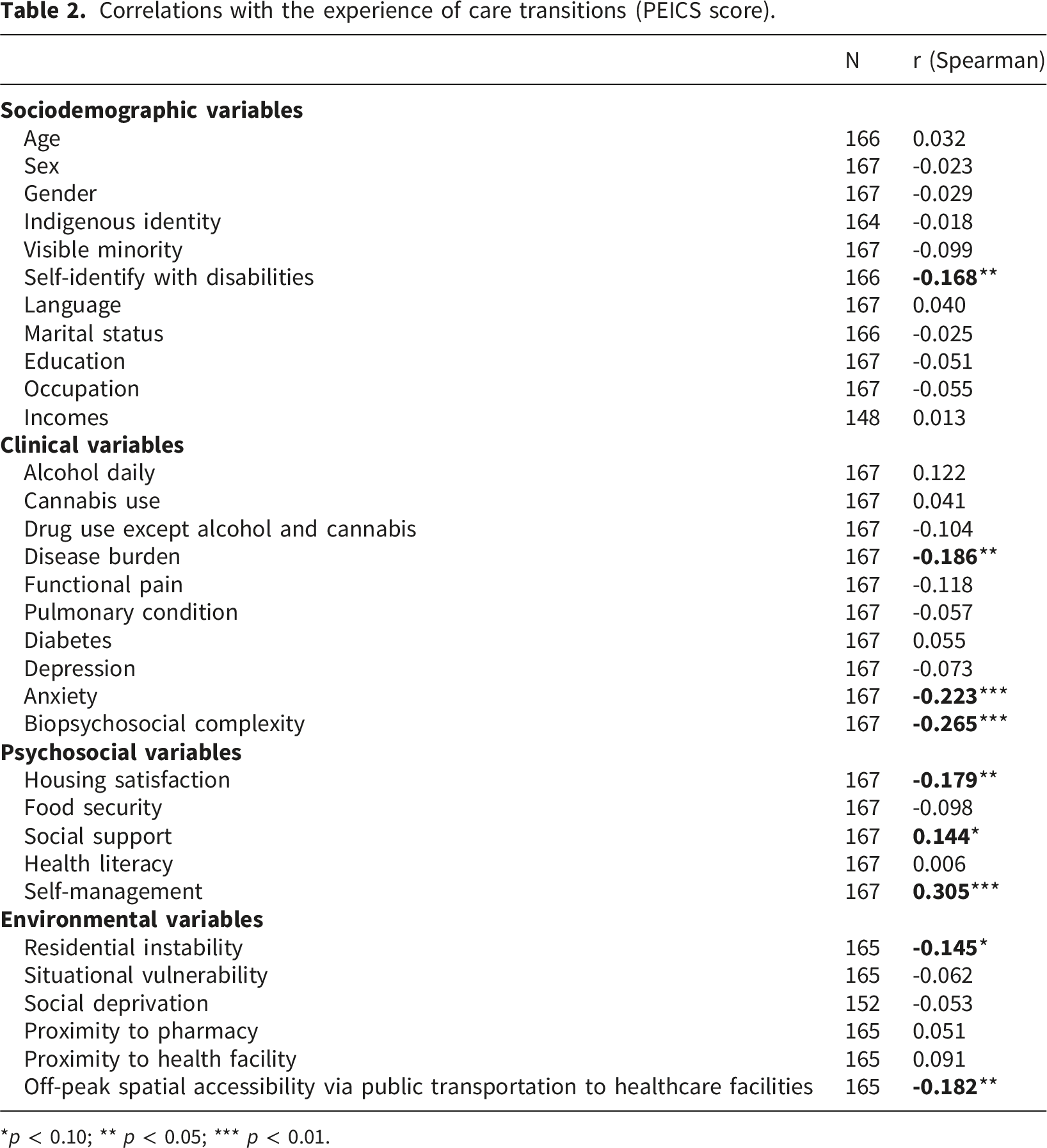
*p < 0.10; ** p < 0.05; *** p < 0.01.
The results revealed significant correlations between care transition experiences and several independent variables. Negative correlations were observed with disability, disease burden, anxiety, biopsychosocial complexity (IMSA score), housing satisfaction, residential instability, and off-peak spatial accessibility via public transportation to healthcare facilities. Positive correlations were found with social support and self-management. The spatial accessibility variable displayed a highly skewed distribution. Diagnostic checks further indicated that the inclusion of this variable violated key regression assumptions (particularly regarding linearity and residuals). Consequently, this variable was excluded from further multivariable analysis.
Linear regression model.
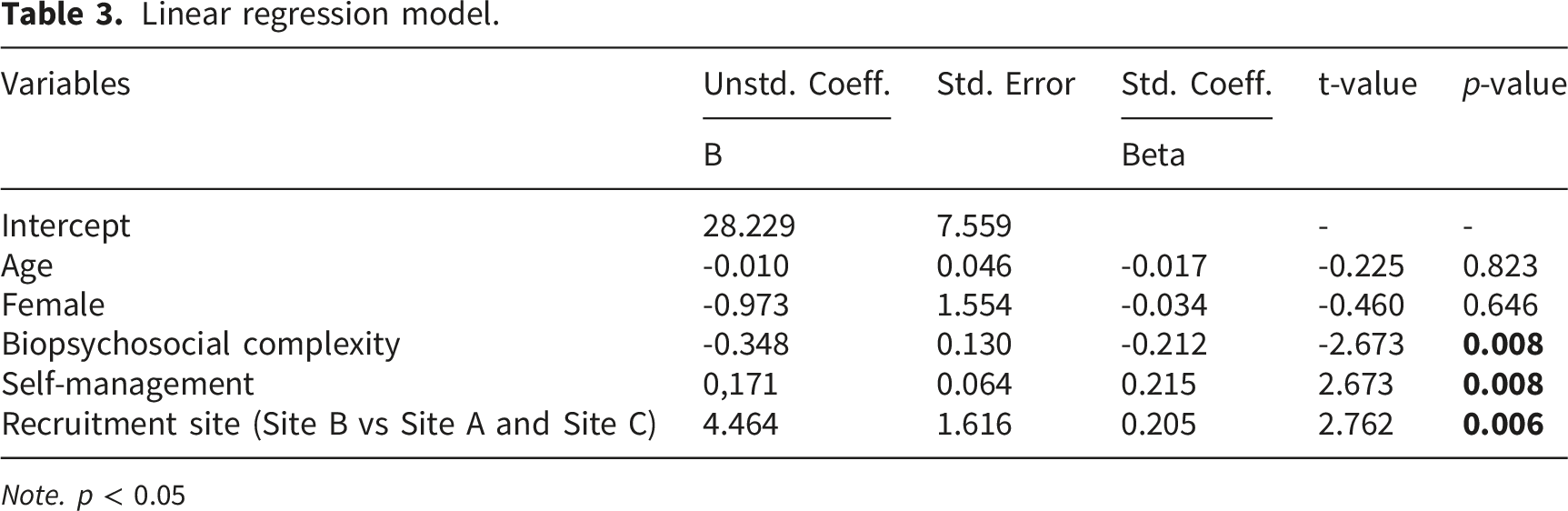
Note. p < 0.05
Higher biopsychosocial complexity was associated with poorer experiences of care transitions, whereas stronger self-management skills were associated with better experiences. Participants from Site B also reported significantly better care transition experiences. The final model explained 16.6% of the variance in care transition experiences.
Discussion
This prospective study investigated how individual and environmental factors influence patient-reported experiences of care transitions among people with complex needs. Over six months, greater biopsychosocial complexity was associated with less favourable transition experiences, whereas stronger self-management capacity was linked with more positive experiences. Additionally, participants from one site reported better experiences of care transitions. These results suggest that transitions may be driven more by overall complexity profiles than by single clinical or psychosocial variables. This shifts the focus from isolated determinants to the interplay between biopsychosocial dimensions, which has received limited attention so far.
Previous research has predominantly considered comorbidities as predictors of readmissions. For instance, a mixed-method cross-sectional study involving 1,066 general medicine patients revealed that 41% identified comorbidities as contributing to their readmission. 58 Likewise, a cohort study in 21 tertiary hospitals of different westerns countries found that half of patients with chronic conditions were readmitted due to comorbidities. 59 Although both studies accounted solely for comorbidity, the authors strongly advocated for a more holistic approach during the post-discharge phase of care.
In addition to medical factors, several studies have identified the influence of psychosocial and sociodemographic determinants on hospital-to-home transitions. A longitudinal study involving 3,021 older adults over 15 years revealed that, beyond age, sex, multimorbidity, and functional capacity, educational attainment was a significant predictor of both the number and type of care transitions. 60 Similarly, a prospective cohort study of 202 participants found that those facing at least two social determinants of health barriers, or with a history of homelessness or substance use disorder, were more likely to experience preventable readmissions. 61
Our results challenge the assumption that comorbidities or psychosocial factors alone determine transition experiences, emphasizing the need to consider biopsychosocial complexity through the integration of psychosocial factors with clinical characteristics for a more holistic perspective. Although self-identification with disabilities, disease burden, anxiety, and housing satisfaction were initially identified as relevant factors in bivariate analyses (Table 2), these associations did not persist in multivariable regression, where only biopsychosocial complexity remained in the final model. This indicated that the combined influence of clinical and psychosocial factors—rather than either aspect in isolation —is more closely linked to patients’ experiences during transitions.
Our findings are consistent with previous research demonstrating the connection between self-management abilities and patients’ experiences during care transitions. For example, findings from a cross-sectional study indicated that, although most readmitted patients felt sufficiently prepared at discharge, more than half faced practical barriers to self-management, such as limited social support and challenges in following post-discharge instructions (e.g., diet, medication, transportation). 58 These results highlighted self-management as a key explanatory factor influencing readmissions. To improve safety for patients with limited self-management capacity, the authors emphasized the importance of considering the patient’s living environment and support system, extending beyond the discharge process itself. Despite increasing recognition of the role of self-management, structured initiatives to develop these skills remain inadequate at discharge. 58 Our findings further underscore the necessity of supporting self-management, not only at discharge, but also across various types of transitions within the continuum of care.
As individual-level factors accounted for only 16.6% of the variance, this modest explanatory power highlights the need to explore additional determinants at other levels of care. Several studies highlighted the importance of considering not only individual-level characteristics but also organizational and systemic factors in understanding care transitions.62–64 In this study, participants from one site reported more positive transition experiences, suggesting that organizational practices, coordination models or local care pathways may influence patients’ experiences independently of individual characteristics. These dynamics will be further examined in a subsequent qualitative study.
Regarding environmental factors influencing care transitions, the associated variables had to be excluded for statistical reasons. Consequently, our study does not allow conclusions to be drawn on their potential effects. Further research will be required to adequately address this issue, particularly given that existing literature indicates that environmental factors may play a significant role in shaping care transitions. A retrospective correlational study examined the relationships between early provider follow-up, the intensity of post-discharge care coordination, neighborhood disadvantage, and 30-day readmission rates among older adults with heart failure. 65 The authors reported that individuals living in the most disadvantaged neighborhoods, women, and racialized individuals were more likely to receive lower levels of transitional care, including less early provider follow-up and coordination. 65 In addition, several qualitative studies have highlighted that transportation barriers and limited access to healthcare facilities can negatively influence care transitions.17,66
Strengths and contributions of the study
This study has several strengths, including its prospective design, with a six-month interval between the measurement of independent and dependent variables which enhances the temporal validity of the findings. Although an extended follow-up might have offered further insights, the risk of participant attrition was considerable within this vulnerable cohort. Conducting the study across five ED of varying sizes from three sites in two Canadian provinces enhances the generalisability of the results.
This study contributes to a broader understanding of care transitions for individuals with complex needs. Notably, it differs in scope by examining all transitions these individuals experience, rather than restricting focus to a single event such as hospital discharge. Moreover, while earlier studies typically concentrated on older adults or on specific medical conditions, our research placed complexity itself at the forefront. In doing so, it advances the conceptualization of care transitions beyond disease-specific models and foregrounds the experiential perspective of patients.
Limitations
This study has certain limitations. The sample size reflects the challenges of recruiting individuals with complex needs—a population difficult to identify and generally hard to reach.67,68 The 167 participants represent 11% of 1,487 patients approached over 21 months in the EDs, underscoring the effort required. The calculated power was 93.8%, indicating that the statistical power was adequate.
Ideally, separate regression models for women and men would have been developed, but the sample size constraints required combining both sexes to ensure sufficient statistical power. Importantly, sex was not a significant variable in the final model. Beyond these analytical considerations, reliance on self-reported data for the six-month PEICS outcome may have introduced recall bias. In addition, using ED utilization as a proxy for complexity may have underrepresented well-supported individuals with complex needs, whose care transition experiences likely differ from those captured in this study. Consistent with this limitation, retaining participants facing greater social disadvantage proved challenging, potentially introducing selection bias. Consequently, generalizability to more socially disadvantaged populations should be made with caution.
At a broader level, organizational and systemic factors are also likely to influence care transition experiences. However, these variables were not available for inclusion in the current model. This limitation will be addressed in a subsequent qualitative phase involving patients, healthcare professionals, and managers. Finally, environmental variables—particularly the spatial accessibility measure—could not be fully assessed because their highly skewed distributions did not meet key statistical assumptions. Nevertheless, environmental factors may meaningfully influence care experiences, underscoring the need for further research to better address this dimension.
Practical implications and recommendations
The findings underscore the necessity for care transition planning that goes beyond standard clinical discharge protocols, addressing both biopsychosocial vulnerabilities and self-management abilities. Supporting individuals with biopsychosocial complexity needs requires coordinated strategies, such as proactively developed individualized care plans and case management69,70 tailored to patients needs, to help them navigate fragmented care pathways. While these coordination mechanisms are essential, they must be complemented by components that strengthen patient capacity, including self-management support. Healthcare systems should therefore integrate biopsychosocial assessments into transition planning to more effectively identify patients at risk of negative experiences and to prevent disruptions in - care transitions. Policymakers and healthcare leaders should recognize care transitions as intersectoral processes and invest in comprehensive strategies that reflect the lived experiences of patients moving across multiple providers and services.
Future research directions
This study identifies several promising directions for future research. The prospective design of this study suggests a possible causal relationship between biopsychosocial complexity, self-management and care transitions experiences. However, additional studies are necessary to confirm the causality. Research should also focus on pinpointing the organizational factors that may contribute to more favourable transitions. More broadly, there is a need to examine influences on care transition experiences that extend beyond the individual, encompassing organisational and systemic aspects. Lastly, the role of environmental variables warrants further investigation to better understand their potential influence on care transition experiences.
Conclusion
Care transitions represent pivotal moments in the patient journey, particularly for individuals with complex needs. In this prospective study, greater biopsychosocial complexity was associated with less favourable transition experiences, whereas stronger self-management abilities corresponded to more positive outcomes over six months. The results underscore the value of a holistic approach to care transitions, one that considers biopsychosocial complexity, as well as the patient’s full care trajectory, rather than limiting focus to particular events such as hospital discharge. Strengthening care transitions for patients with complex needs requires integrated strategies that combine biopsychosocial assessment with structured support for self-management and navigation. At the policy and system levels, these findings align with ongoing efforts in integrated and transitional care programs to better coordinate services across sectors. Public policies should be explicitly oriented toward strengthening integration across organisational, professional, and clinical levels. Future work should examine how organizational and system-level factors influence patients’ experiences of care transitions.
Supplemental material
Supplemental material - Factors associated with care transition experiences among individuals with complex needs: A prospective study
Supplemental material for Factors associated with care transition experiences among individuals with complex needs: A prospective study by Catherine Hudon, Emilie Angrignon-Girouard, Shelley Doucet, Marie-France Dubois, Nathalie Carrier, Olivier Dumont-Samson, Charlotte Schwarz, Mireille Lambert, Grégory Moullec, Benoît Thierry, Yohann Moanahere Chiu, Alison Luke, Marlène Karam, Kris Aubrey-Bassler, Maud-Christine Chouinard, Marie-Dominique Poirier, Betty Maloney in Journal of Multimorbidity and Comorbidity.
Footnotes
Acknowledgments
The authors would like to thank the participating healthcare organizations for their collaboration and support throughout the project. For confidentiality reasons, the names of these institutions are not disclosed.
Ethical considerations
This study was conducted in accordance with the Declaration of Helsinki and received ethical approval from the Research Ethics Board of CIUSSS de l’Estrie-CHUS (#MP-31-2022-4501) on January 7th, 2022.
Consent to participate
All participants provided written informed consent before enrolment.
Consent for publication
The study did not use any personal information, images, or data that could identify any individual.
Authors contributions
CH conceptualized and designed the study; ODS, CS, EAG, ML and BT collected and curated the data; NC conducted the data analysis; EAG created the figures and tables; CH and EAG drafted the manuscript; every authors critically revised the manuscript for intellectual content; CH supervised the project and secured funding. All authors reviewed and approved the final manuscript and are accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Canadian Institutes of Health Research (CIHR). The funder had no role in the study design, data collection, analysis, interpretation, or decision to submit the manuscript. Additionally, the lead author holds the Canada Research Chair in Implementing Integrated Care for People with Complex Needs.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available upon reasonable request.
AI Assistance Declaration
Microsoft Copilot was used to assist with text editing during the preparation of this manuscript. All content generated or modified with AI assistance was reviewed and approved by the authors, who take full responsibility for its accuracy and integrity.
Supplemental material
Supplemental material for this article is available online.
Appendix
Recruitment flowchart.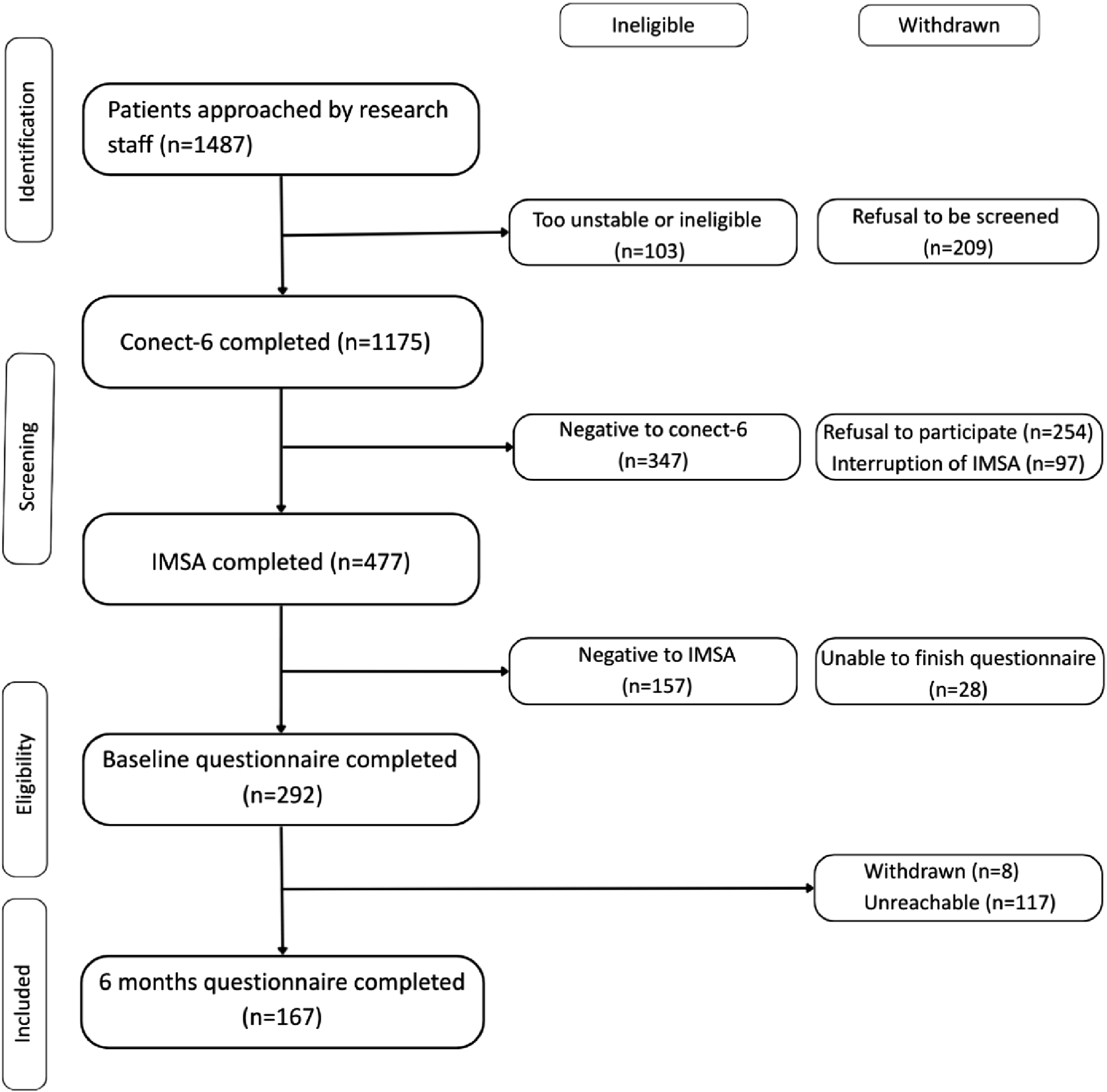
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.