
Abstract

Chronic kidney disease (CKD) is a progressive disease that can cause numerous complications, including electrolyte imbalances, anemia, and bone and mineral disorders. 1 It may eventually progress to end-stage kidney disease (ESKD) requiring dialysis and kidney transplant. Diabetes is a risk factor for CKD, which develops in 20% to 40% of individuals with diabetes. 1 Additionally, the presence of CKD increases the risk of cardiovascular disease.
The American Diabetes Association (ADA) recommends metformin as first-line therapy for all patients with type 2 diabetes mellitus (T2D), including those with CKD. 1 Metformin should be continued as long as it is tolerated and not contraindicated. A sodium-glucose cotransporter-2 (SGLT-2) inhibitor with evidence of reducing CKD progression is also recommended in individuals with T2D and established renal disease if estimated glomerular filtration rate (eGFR) is adequate. The purpose of this article is to review the evidence supporting the use of SGLT-2 inhibitors to preserve kidney function in people with diabetes (for SGLT-2 inhibitors renal dosing recommendations, see Table 1).
Renal Dosing Recommendations for SGLT-2 Inhibitors in People With Diabetes a
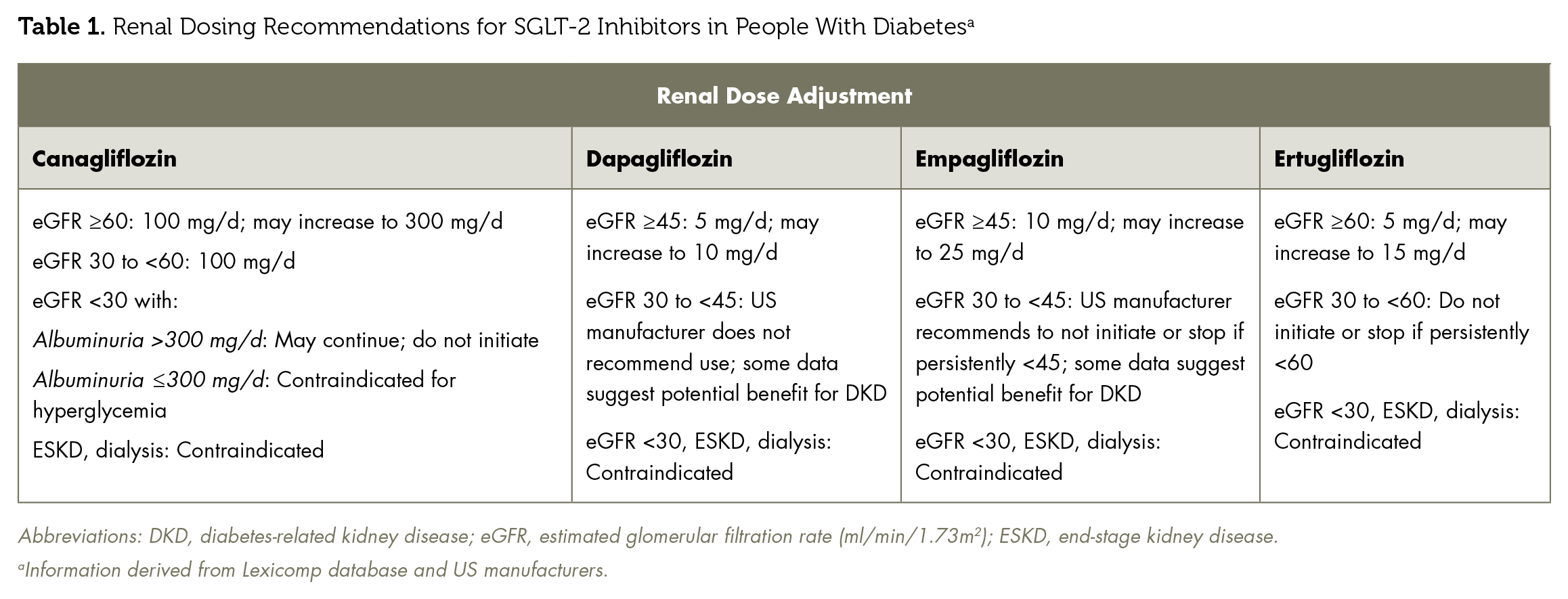
Abbreviations: DKD, diabetes-related kidney disease; eGFR, estimated glomerular filtration rate (ml/min/1.73m2); ESKD, end-stage kidney disease.
Information derived from Lexicomp database and US manufacturers.
Pathophysiology and SGLT-2 Inhibitor Mechanism
The development of diabetes-related kidney disease involves multiple changes, including glomerulopathy, progressive albuminuria, and tubulointerstitial damage. 2 Excessive levels of plasma glucose and amino acids in people with diabetes has been linked to kidney inflammation and fibrosis. Increased proximal tubular reabsorption of glucose by SGLT-2 decreases distal delivery of sodium chloride to the macula densa. The resulting decrease in tubuloglomerular feedback and impact on afferent and efferent arteriole diameter is a proposed mechanism for elevated intraglomerular pressure and glomerular hyperfiltration. Thus, the renal protection exerted by SGLT-2 inhibitors may be explained by mechanisms independent of glucose control. 3
Randomized controlled trials have provided important evidence on the benefits of SGLT-2 inhibitors on renal outcomes on top of the standard of care (blood glucose management, renin-angiotensin system blockade, smoking cessation, and blood pressure control). The renal protective effects of SGLT-2 inhibitors were first observed in large clinical trials evaluating cardiovascular safety of canagliflozin (CANVAS Program), empagliflozin (EMPA-REG OUTCOME), and dapagliflozin (DECLARE-TIMI 58).4-6 These trials demonstrated that SGLT-2 inhibitors reduce albuminuria progression, prevent eGFR decline, and decrease the incidence of renal replacement therapy. However, renal outcomes were secondary endpoints, and a majority of patients were at low risk for renal disease with an average eGFR >60 mL/min/1.73m2 and urine albumin-to-creatinine ratio (UACR) <30 mg/g. Recent trials have studied renal endpoints as the primary outcome in patients with higher risk for renal disease.
Empagliflozin
The EMPA-REG OUTCOME trial examined 7020 patients with T2D and evaluated the primary composite outcome of death from cardiovascular causes, nonfatal myocardial infarction, or nonfatal stroke. The primary outcome occurred in 10.5% of patients in the empagliflozin group versus 12.1% in the placebo group (hazard ratio [HR], 0.86; 95% CI, 0.74-0.99). 6 A secondary analysis of the EMPA-REG OUTCOME trial found empagliflozin to have better results for the post hoc composite renal outcome of doubling of serum creatinine (SCr), the initiation of renal replacement therapy, or renal death (HR, 0.54; 95% CI, 0.40-0.75). 7 Incident or worsening nephropathy occurred in 12.7% of the empagliflozin group and in 18.8% of the placebo group, a significant relative risk reduction of 39% (HR, 0.61; 95% CI, 0.53-0.70). This trial did not evaluate individuals with an eGFR <30 mL/min/1.73m2. The ongoing EMPA-KIDNEY trial aims to address the renal effects of empagliflozin on patients with overt diabetes-related kidney disease and is estimated to be completed in 2022.
Dapagliflozin
The DECLARE trial was designed to investigate the impact of dapagliflozin on major adverse cardiovascular events and renal function as a secondary outcome in 17 160 patients. In addition to showing positive cardiovascular outcomes, there was a statistically significant renal benefit, defined as a composite of ≥40% decrease in eGFR to <60 ml/min/1.73 m2, new ESKD, or death from renal or cardiovascular causes. A renal event was seen in 4.3% of the dapagliflozin group compared to 5.6% of patients on placebo (HR, 0.76; 95% CI, 0.67-0.87). A limitation in terms of determining renal impact of dapagliflozin in this study includes an exclusion criterion of creatinine clearance <60 mL/min. The DAPA-CKD trial enrolled patients with CKD irrespective of T2D and was stopped early at the recommendation of an independent data monitoring committee due to renal benefit. 8 The complete results from that study have yet to be published.
Canagliflozin
The CANVAS Program combined data from 2 trials involving a total of 10 142 participants with T2D and high cardiovascular risk. The primary outcome (composite of nonfatal myocardial infarction, nonfatal stroke, or cardiovascular death) was lower with canagliflozin than with placebo (HR, 0.86; 95% CI, 0.75-0.97). The results also showed a possible renal benefit of canagliflozin with respect to the progression of albuminuria (HR, 0.73; 95% CI, 0.67-0.79) and the composite of a sustained 40% eGFR reduction, need for renal replacement therapy, or renal death (HR, 0.60; 95% CI, 0.47-0.77).
CREDENCE was a double-blind randomized trial powered to evaluate the effects of canagliflozin on the primary composite outcome of ESKD (dialysis, transplantation, or a sustained eGFR of <15 ml/min/1.73m2), doubling of SCr, or death from renal or cardiovascular causes. 9 The trial included 4401 patients with diabetes, albuminuria, and an eGFR between 30 and 90 mL/min/1.73 m2. The trial was stopped early on the recommendation of the data and safety monitoring committee. The canagliflozin group had a 30% relative risk reduction compared to placebo (HR, 0.70; 95% CI, 0.59-0.82). Additionally, as seen in previous trials, the canagliflozin group showed lower risk of cardiovascular death, myocardial infarction, or stroke (HR, 0.80; 95% CI, 0.67-0.95) and hospitalization for heart failure (HR, 0.61; 95% CI, 0.47-0.80). Based on these results, canagliflozin was granted an FDA-approved indication for risk reduction of ESKD, doubling of SCr, cardiovascular death, and hospitalization for heart failure in adults with T2D and diabetes-related nephropathy with urinary albumin excretion >300 mg/d.
Ertugliflozin
The VERTIS CV trial evaluated the cardiovascular safety of ertugliflozin in 8246 patients with T2D and established atherosclerotic cardiovascular disease. 10 The renal composite outcome was a secondary endpoint that consisted of renal death, dialysis, renal transplant, or doubling of SCr. There was no statistically significant renal benefit of ertugliflozin compared with placebo, although there was a trend toward beneficial effect (ertugliflozin 3.2% vs placebo 3.9%, P = .08). The complete results from that study have yet to be published.
SGLT-2 Inhibitors Meta-Analyses
The renal benefits of SGLT-2 inhibitors appear to be a class effect. In a meta-analysis evaluating the renal effects of SGLT-2 inhibitors, there was a 38% reduction in the primary composite outcome of new-onset macroalbuminuria, doubling of SCr, and 40% decline in eGFR, ESKD, or renal death (HR, 0.62; 95% CI, 0.58-0.67), which remained significant with the exclusion of macroalbuminuria (HR, 0.55; 95% CI, 0.48-0.64). 11 There was a similar renal benefit in patients on SGLT-2 inhibitors regardless of baseline atherosclerotic cardiovascular disease. 12 In addition, the renoprotective effect was present across all eGFR levels but was greatest in those with preserved renal function at baseline. There was a 33% reduction in patients with an eGFR <60 mL/min/1.73m2, 44% reduction in patients with an eGFR between 60 and 90 mL/min/1.73m2, and 56% reduction in patients with an eGFR >90 mL/min/1.73m2.
Conclusion
CKD in individuals with diabetes is a major problem of public health. The first-line treatment for patients with T2D and CKD should remain metformin for individuals with sufficient renal function. In addition, there is now evidence to support the use of SGLT-2 inhibitors and GLP-1 receptor agonists for their cardiovascular and renal benefits. In terms of renal outcomes, GLP-1 receptor agonists primarily reduce the risk of macroalbuminuria, whereas SGLT2 inhibitors have a more marked effect on progression of kidney disease. ■