
Abstract


Diabetes continues to be a major public health challenge, affecting millions of individuals and disproportionately impacting underserved communities. To address this important matter, ADCES launched the DELTA LEAD initiative— Delivering Evidence Led inTerventions Across the Lifespan to improve Equity and Access to Diabetes Care. This initiative is a 5-year cooperative agreement with the Centers for Disease Control and Prevention (CDC), which aims to transform diabetes care and prevention by implementing evidence-based programs and increasing access to effective and quality care for those disproportionally impacted by diabetes.
What Is DELTA?
DELTA was driven by the necessity for a layered framework. Natalie Elleson, project director, public health practices and diabetes programing, explains, “This initiative provides an opportunity to conduct multitiered approaches to preventing, treating, and managing diabetes from youth through older adulthood using evidence-based programming.”
Currently, more than 30% of adults and about 17% of children and adolescents in the United States are living with higher weight or obesity, and diabetes rates are rising. DELTA focuses on tackling these issues early to prevent long-term health complications.
ADCES is one of 77 recipient projects supported by the Diabetes MATCH (Mobilizing Access Through Capacity Building and Health) Initiative. Through the DELTA initiative, ADCES implements 3 evidence-based strategies to address prevention of diabetes and management across the life span.
Elleson emphasizes that “prevention is key! Preventing the onset of diabetes by starting with our youth (FHWP), preventing or delaying type 2 diabetes for adults (National DPP), and preventing future complications for those with diabetes (through DSMES). These evidence-based programs all have similar goals and complement each other, so how can we think creatively to find linkages between them!”
DELTA aligns closely with ADCES’s mission and values, prioritizing equity, prevention, and evidence-based programming to deliver longterm health improvements.
Focus on Populations Most Affected by Diabetes
One of DELTA’s main goals is to address health disparities by targeting those at highest risk and enhancing access to diabetes care and prevention programs. Through collaborations with federally qualified health centers (FQHCs) in high-need counties, the initiative is making strides in reaching historically underserved populations, including Black/African American men and Spanish-speaking individuals in complex, Englishdominant health care systems. These FQHCs serve as vital partners, addressing social needs that impact health outcomes and delivering culturally relevant care to improve health for populations most affected by diabetes and related risk factors.
ADCES’s DELTA team works closely with 3 FQHC partners, located in Georgia (MedLink Georgia, Inc), Indiana (Eskenazi Health), and California (Ampla Health). These FQHCs have sites embedded in both rural and urban communities and play a critical role in engaging at-risk populations by providing tailored programs and building sustainable diabetes care models. The DELTA team supports these sites through shared resources, training, and implementing best practices to address the unique needs of their communities.
FQHC Focus on Populations Most Affected by Diabetes
The DELTA team identified the populations most affected by diabetes to target, but each FQHC served different populations in different geographic regions. To narrow down populations for each, the DELTA team facilitated discussions with each partner to determine which groups would benefit most from increased enrollment and retention in diabetes services. A funnel diagram tool was introduced to help each diabetes care team brainstorm and analyze which populations they currently serve, who is at higher risk for diabetes and its complications, and who has been historically or systematically underserved.
MedLink Georgia: Operating in a predominantly rural area, MedLink targets populations facing substantial socioeconomic barriers, such as transportation, phone, and internet access. African Americans, a group with high diabetes risk and low enrollment in diabetes programs and services, were chosen as a priority for increased outreach and program participation.
Eskenazi Health: With a robust system for assessing social determinants of health (SDOH) and strong community ties, Eskenazi identified 2 key groups for their programs. African American men, who have been difficult to engage in DSMES and diabetes prevention program, were prioritized for targeted adaptations to the DSMES curriculum to increase cultural relevance. FQHC patients speaking Spanish will be targeted for increased diabetes prevention program enrollment. The DELTA team engaged a consultant to support this process.
Ampla Health: Serving a mix of rural and urban communities in northern California, Ampla focuses on immigrant populations from Mexico and Central America. Recognizing that Hispanic/Latino individuals face significant barriers to care and are at higher risk for diabetes, Ampla is working to increase engagement with Spanish speakers and strengthen relationships within these communities. For the diabetes prevention program, Ampla launched their first Spanish-language cohort.
The funnel diagram (Figure 1), or similar tool, and collaborative brainstorming sessions used to identify populations most impacted by diabetes can serve as a practical tool for others looking to replicate this work. These are opportunities to better understand what resources partners have available and the populations they serve. The funnel diagram facilitates in-depth discussions with partners to narrow down those at highest risks to target. By targeting specific populations, DELTA aims to bridge the disparities gap in diabetes care in the United States.
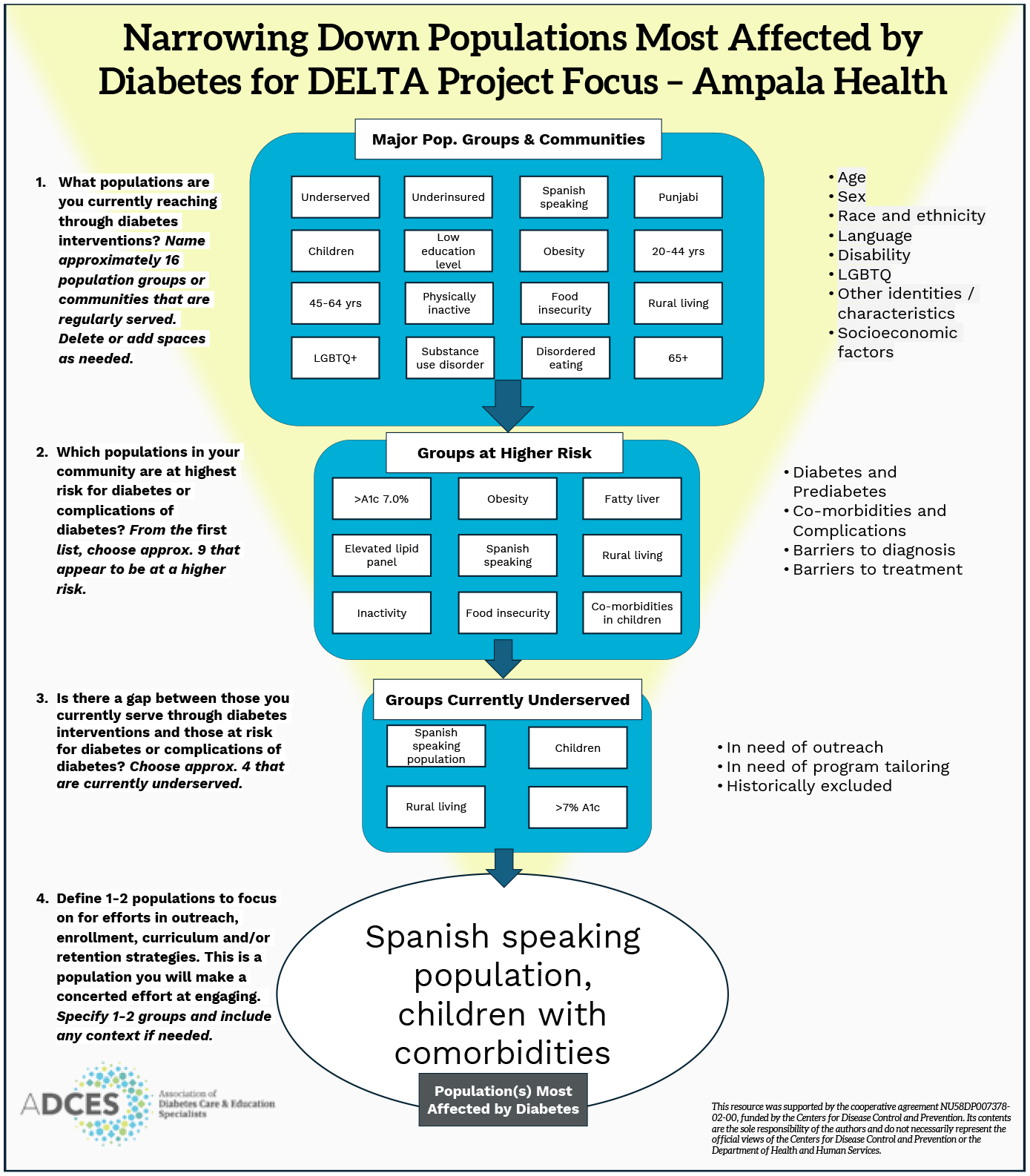
DELTA designed funnel diagram used to facilitate discussions identifying population(s) most affected by diabetes to focus on completed by Ampla Health.
Accomplishments and Impact
In its first year, DELTA established a strong foundation for long-term success and has made significant progress:
increasing the number of community sites offering DSMES
FQHC partner becoming a CDC-recognized diabetes prevention program
assessing community readiness and developing targeted marketing plans
training care teams on SDOH
exploring complementary diabetes support programs and best-fit FHWP models
establishing reimbursement and sustainability plans to support long-term viability.
The work conducted by the DELTA team and its FQHC partners aims to have far-reaching impacts, including better health outcomes for populations most affected by diabetes and the development of scalable models that can be replicated nationwide. By focusing on underserved communities and integrating culturally relevant interventions, DELTA’s approach provides a roadmap for reducing health disparities and improving diabetes care at a systemic level. DELTA’s focus on sustainability and cross-program integration offers a blueprint for creating lasting improvements in health equity.
Looking Ahead
The DELTA initiative provides more than technical assistance and support for the FQHCs it works with; it represents a transformative approach to improving health equity and access. By leveraging evidence-based strategies, increasing the sustainability and capacity of multidisciplinary care teams, and fostering collaboration among FQHCs, ADCES is improving access to diabetes care and education.
As the initiative progresses, ADCES’s DELTA team remains committed to scaling successful strategies, sharing lessons learned, and advocating for expanded access to culturally responsive programs. Through the DELTA and MATCH Initiatives, ADCES is addressing the immediate needs of individuals at risk for or living with diabetes while laying the groundwork for a healthier and more equitable future. ■
Footnotes
Funding
This resource was supported by the cooperative agreement NU58DP007378-02-00, funded by the Centers for Disease Control and Prevention. Its contents are the sole responsibility of the authors and do not necessarily represesnt the official views of the Centers for Disease Control and Prevention or the Department of Health and Human Services.