
Abstract

Health equity remains a foundational element of effective public health practice. This is particularly true in diabetes prevention and management, where inequities disproportionately affect racially and ethnically minoritized communities, individuals living in underresourced areas, and populations facing systemic barriers to care. Type 2 diabetes continues to be overrepresented in communities with fewer economic opportunities, limited access to preventive services, and increased exposure to the conditions that drive chronic disease risk. As national funding agencies increasingly emphasize health equity as a core priority, the capacity of programmatic and technical assistance (TA) staff to engage confidently in equity-centered work has become essential.
The Diabetes MATCH (Mobilizing Access Through Capacity Building and Health) Initiative—jointly led by the Emory Centers for Public Health Training and Technical Assistance and the Association of Diabetes Care & Education Specialists (ADCES)—is funded through a cooperative agreement with the Centers for Disease Control and Prevention (CDC-RFA-DP-23-0021). MATCH supports recipients of the companion funding opportunity, A Strategic Approach to Advancing Health Equity for Priority Populations With or at Risk for Diabetes (CDC-RFA-DP-23-0020), by helping state health departments, community-based organizations, and partners strengthen their capacity to deliver diabetes-related interventions. As MATCH staff serve as trainers, TA providers, and capacity-building agents for recipients nationwide, the initiative recognized the need to ensure that its own team members possessed the skills, knowledge, and confidence necessary to model and support equity-informed practice.
In response, the Health Equity Team designed and implemented a comprehensive, multipronged internal training program to strengthen staff capability to operationalize health equity principles in their work. The training program was created against the backdrop of an increasingly polarized political landscape, where equity terminology and related initiatives may elicit resistance or discomfort among stakeholders. This context underscored the importance of preparing staff not only to apply equity concepts but also to navigate challenging conversations, recognize their own biases, and maintain clarity and compassion in their approach.
This article describes the development, implementation, and early outcomes of this health equity training initiative, developed to build the confidence, competence, and commitment of programmatic staff working to advance equity in diabetes prevention and management.

Methods
The training model was developed using a data-informed, iterative design process. Work began with an internal focus group involving programmatic staff representing a range of professional backgrounds, experience levels, and roles in the MATCH Initiative. The purpose of this focus group was to:
assess staff’s health equity competencies
understand their comfort level with equity-related concepts
identify common challenges encountered in their work
explore their expectations for professional development.
During the focus groups, staff were presented with the Office of Health Equity’s (OHE) Health Equity Domains, shown in Figure 1, and engaged in guided discussions about their knowledge of the domains and how they apply them in their day-to-day work. Findings revealed variation in staff’s familiarity with equity topics. Some individuals were highly experienced in facilitating equity discussions and applying equity frameworks to public health practice. Others expressed discomfort or hesitancy, often related to fears of causing harm, low confidence in their knowledge or skills, and concerns about navigating politically sensitive environments. These insights served as the foundation for designing a differentiated learning plan that acknowledged the staff’s diverse starting points.
The training program was built around 3 core principles:
Meet staff where they are by offering developmentally appropriate content that does not assume prior expertise.
Integrate structured and unstructured learning to address both technical knowledge (eg, health equity frameworks) and interpersonal skills (eg, confidence in facilitating sensitive conversations).
Promote continuous reflection and application, ensuring that staff connect learning to their daily responsibilities.
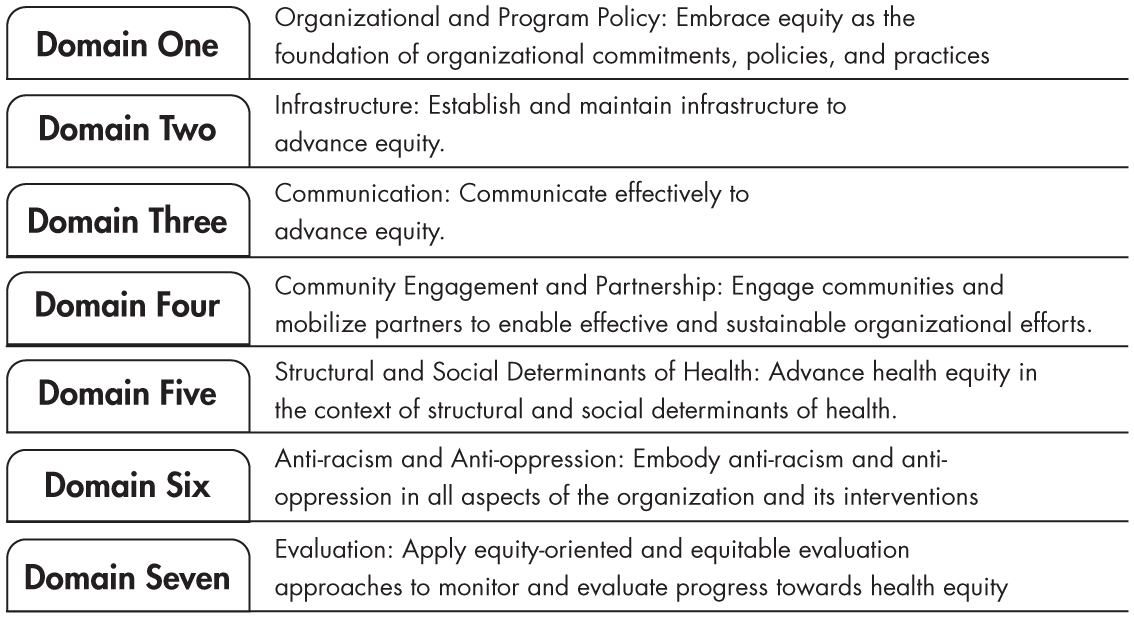
Office of Health Equity’s Health Equity Domains
Training sessions are held monthly and facilitated by the internal Health Equity Team with contributions from external experts specializing in messaging, bias, structural determinants of health, human behavior, and reflective practice. Each session followed a consistent structure:
Foundational content: definitions, frameworks, and practical tools.
Facilitated breakout discussions: small-group dialogue designed to allow staff to process material in a supportive environment.
Application scenarios: realistic TA challenges requiring staff to apply health equity principles.
Reflective assignments: short, structured prompts encouraging ongoing self-assessment and integration into daily work.
Session topics included health equity messaging, unconscious and implicit bias, culturally responsive engagement, navigating politicized environments, trauma-informed communication, and strategies for identifying opportunities to embed equity into program planning, development, and implementation. The initial sessions were grounded in a set of core health equity imperatives, shown in Figure 2, which served as a foundational framework for the training series. During these sessions, the imperatives were first introduced and situated within relevant organizational and programmatic contexts. Staff then engaged in facilitated breakout discussions using role-specific scenarios that reflected real-world challenges. These discussions provided participants with structured opportunities to practice applying the imperatives to their daily work, including program planning, implementation, and decision-making.

Health equity core imperatives.
Progress was monitored through postsession surveys and informal feedback. The Health Equity Team used this data to continuously refine the curriculum, adjust facilitation approaches, and add targeted content where additional support was needed.
Results
Evaluation findings indicate that the internal health equity training initiative has improved staff confidence, awareness, and readiness to embed equity principles into their TA delivery and other projects. Early sessions revealed initial hesitation driven by both personal discomfort with sensitive topics and uncertainty about how equity fits into varying programmatic roles. However, comfort levels have increased over time as staff built shared language, trust, and familiarity.
More than 90% of evaluation respondents reported that the trainings helped them better integrate health equity into their work or increased their ability to recognize patterns, behaviors, or biases within themselves. Participants also described feeling more equipped to identify entry points for advancing health equity in conversations with recipients, even when equity was not explicitly requested or when partners expressed reluctance to engage in equity discourse.
Qualitative feedback illuminated several key themes:
Increased confidence: Staff reported feeling more secure in their ability to explain health equity, address misconceptions, and engage in conversations previously perceived as challenging or risky.
Greater self-awareness: Reflective exercises prompted participants to identify personal biases, communication habits, and assumptions that influence their approach to TA.
Enhanced practical skills: Staff gained concrete tools, such as messaging frameworks and question prompts.
Stronger team cohesion: The shared learning environment fostered a collective sense of purpose and mutual support, making equity-related conversations feel safer and more productive.
Additionally, staff reported that the training program helped bridge the gap between theoretical understanding and real-world application. This was particularly important given the broad portfolio of MATCH recipients, whose geographic, political, cultural, and organizational contexts vary widely.
Conclusion
Health equity is not a checklist item but an ongoing practice rooted in continuous learning, reflection, and skill-building. For programmatic and TA staff who play a critical role in shaping how funded entities and community partners interpret and apply equity principles, ongoing professional development is essential. The training initiative described in this article demonstrates that a thoughtfully designed, multipronged approach (detailed in Table 1) can effectively strengthen staff capacity to advance equity in diabetes prevention and management settings.
Multipronged Health Equity Training Approach
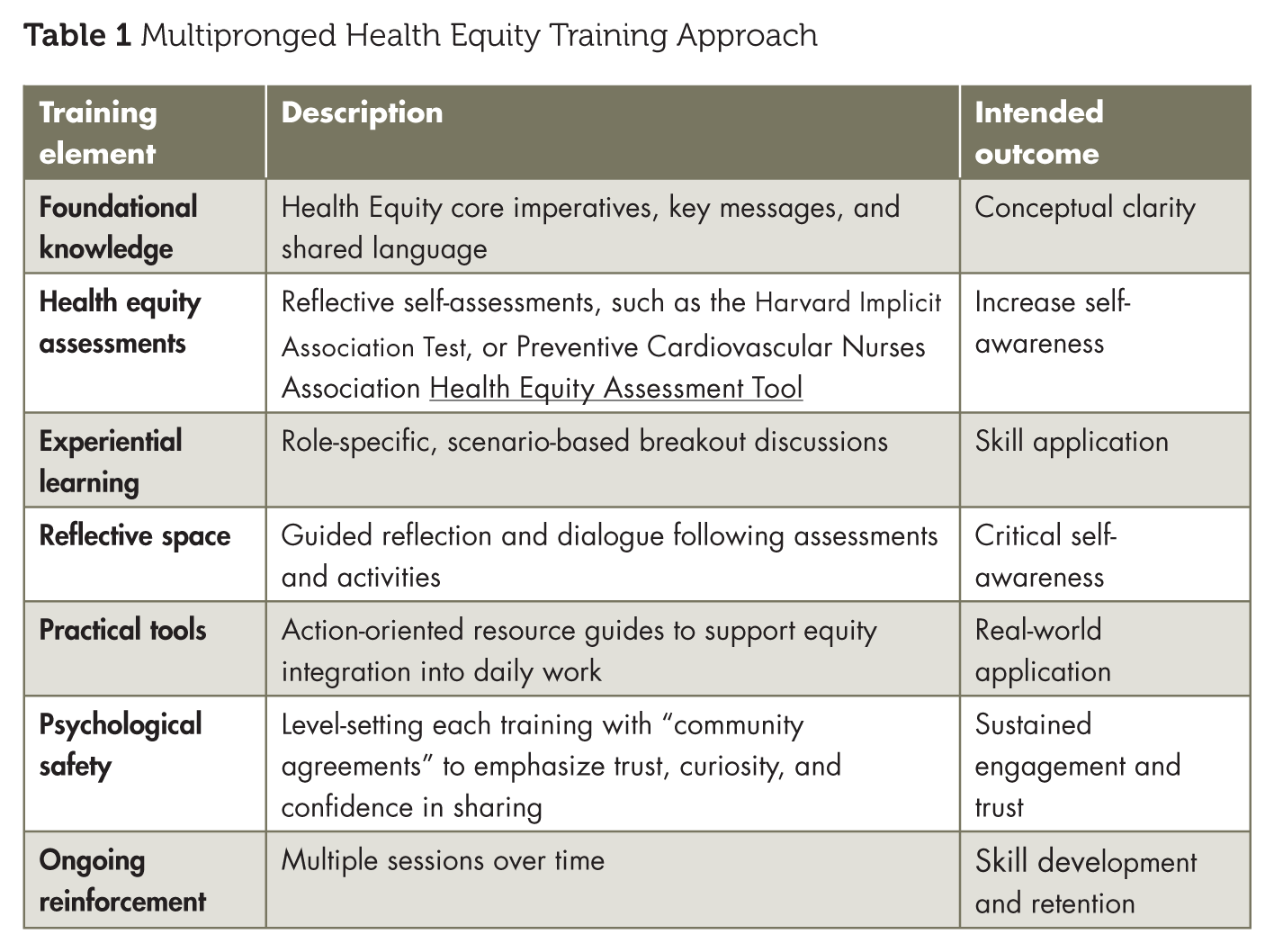
Early results demonstrate that staff benefit from a training structure that balances foundational knowledge with experiential learning, provides dedicated space for reflection and practicing how to incorporates practical tools for real-world application. The model also underscores the value of creating psychologically safe learning environments where questions, uncertainty, and vulnerability are parts of the growth process. As health equity continues to evolve in public health and society at large, sustained investment in workforce development will remain critical to ensuring that equity goals translate into meaningful, measurable action.
This initiative offers a replicable model for public health organizations seeking to strengthen internal health equity competencies. As MATCH continues its work with diabetes prevention and management partners nationwide, the internal training program ensures that staff are equipped to lead with clarity, compassion, and confidence in an increasingly complex and politically charged environment. Long-term success in advancing health equity depends not only on strong external programming but also on the readiness and resilience of the workforce that supports it. ■