
Abstract

Patients with diabetes are at significantly increased risk for genitourinary infections (GUIs), particularly women and those with hyperglycemia. The prevalence of bacterial urinary tract infections (UTIs) among patients with diabetes is estimated at 15% to 20%, with women affected at rates 2 to 4 times higher than their counterparts without diabetes.1-4 Factors associated with increased UTI risk include female sex, advanced age, longer duration of diabetes, greater glycemic variability and/or elevated A1C levels, higher body mass index, and diabetes-related complications such as nephropathy and neuropathy.1,4-6
Pathophysiology
Multiple mechanisms contribute to the increased infection risk seen in diabetes. Hyperglycemia impairs both innate and adaptive immunity, reducing neutrophil and granulocyte function and downregulating antimicrobial peptides such as psoriasin, which compromises epithelial integrity and promotes bacterial colonization by Escherichia coli.5,7 Glucosuria, a result of chronic hyperglycemia or sodium-glucose cotransporter 2 (SGLT2) inhibitor therapy, provides a nutrient-rich environment for pathogens and increases risk for both UTIs and genital mycotic infections.8-12 Additional factors that increase infection risk in people with diabetes include metabolic, neurologic, and structural abnormalities and medication-related effects (Table 1).
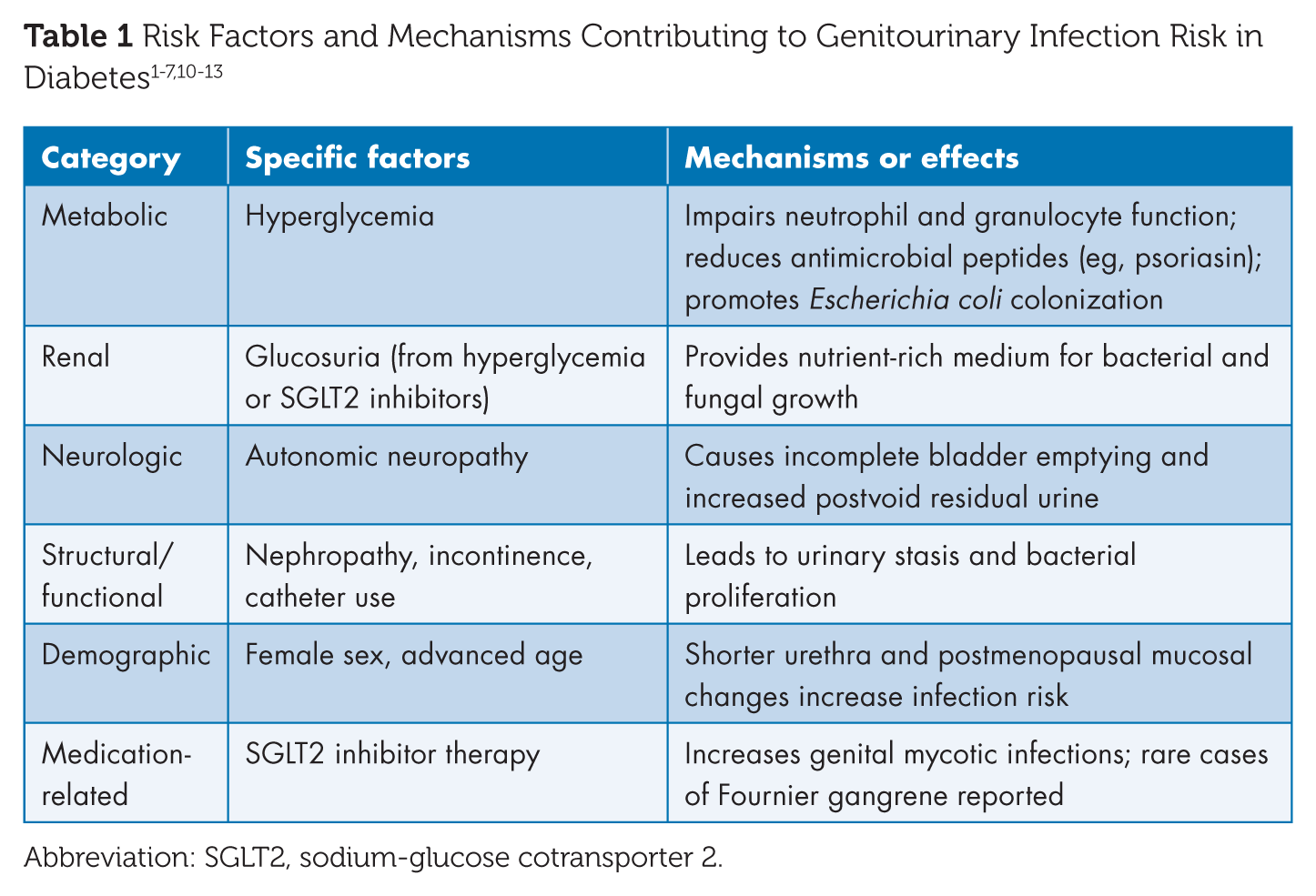
Abbreviation: SGLT2, sodium-glucose cotransporter 2.
Clinical Manifestations
Patients with diabetes experience more frequent and severe UTIs, including complicated infections such as emphysematous pyelonephritis, emphysematous cystitis, renal papillary necrosis, and perinephric abscess.2,3,13 Fungal infections, especially Candida species, are also common. Genital mycotic infections, such as vulvovaginitis and balanitis, are particularly increased among patients taking SGLT2 inhibitors.8-17
SGLT2 Inhibitors and GUI Risk
SGLT2 inhibitors are associated with a 3- to 5-fold increased risk of genital mycotic infections, which are generally mild and manageable. The association with UTIs, however, is less consistent across studies.11,12,15-19 Although rare, severe complications such as Fournier’s gangrene have prompted FDA warnings and warrant clinician vigilance and patient education.11,15,19
Given these risks, diabetes care and education specialists (DCESs) play an essential role in supporting safe and effective SGLT2 inhibitor use. DCESs reinforce practical self-care behaviors, such as maintaining daily genital hygiene, staying well hydrated, and recognizing early signs of infection, and ensure patients understand when to contact their care team. They also help contextualize mild genitourinary symptoms within the broader benefits of SGLT2 therapy, addressing concerns that might otherwise lead to discontinuation. Through individualized education and close communication with prescribers, DCESs help patients balance infection risk with the significant glycemic and cardiorenal advantages of these agents.
Implications for the Diabetes Care Team
Effective prevention and management of GUIs in diabetes require proactive, team-based strategies. DCESs and other diabetes team members play a key role in assessing risk, providing education, and coordinating care. Prevention and management of GUIs require a proactive, multidisciplinary approach centered on education, risk assessment, and timely intervention. Key strategies for diabetes care teams are outlined in Table 2.
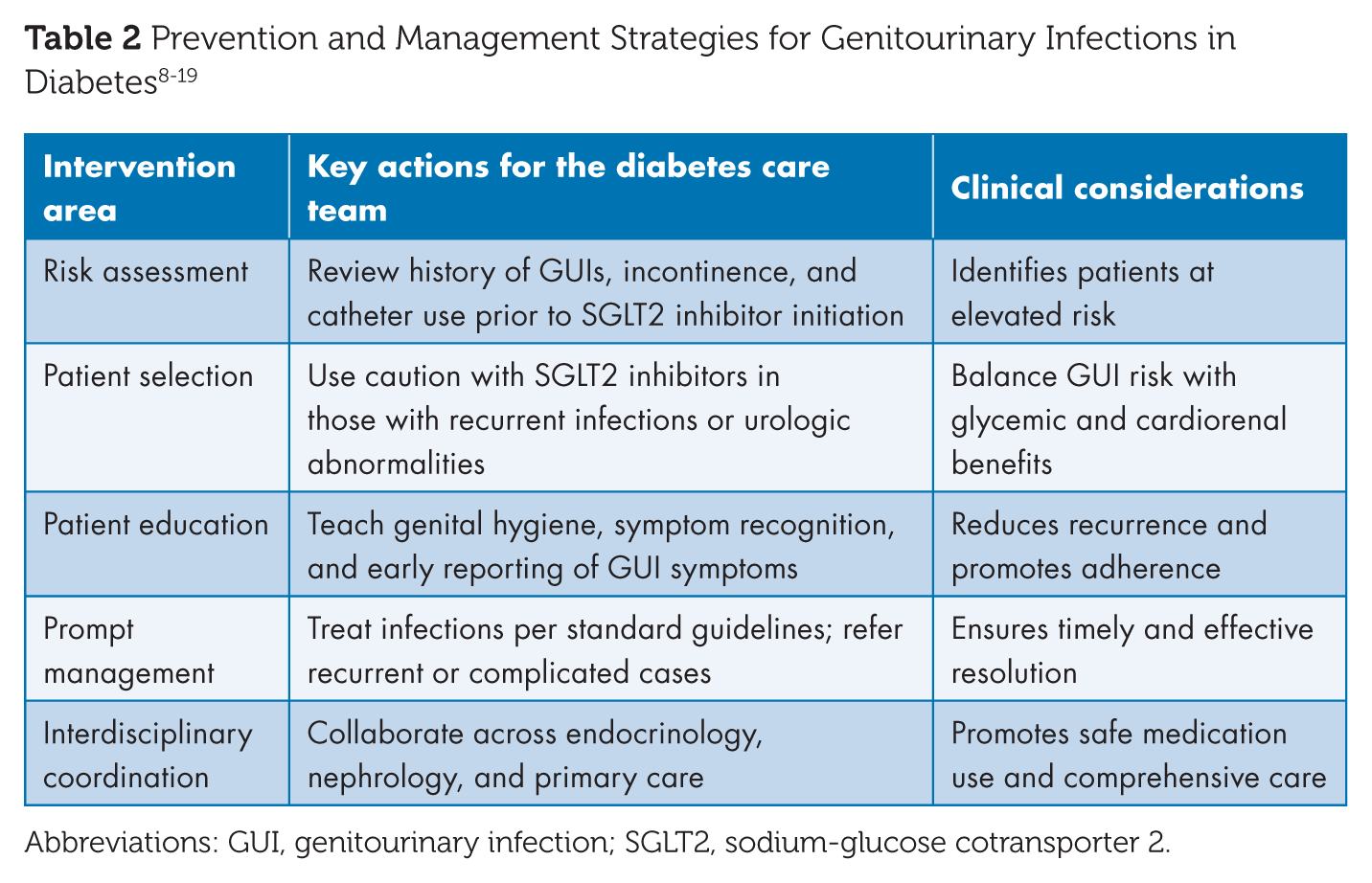
Abbreviations: GUI, genitourinary infection; SGLT2, sodium-glucose cotransporter 2.
Special Considerations in Women
Urinary incontinence is common among postpartum and postmenopausal women with diabetes and increases risk for recurrent UTIs and skin infections. Glucosuria in the context of incontinence can lead to severe skin infections, including necrotizing fasciitis. Addressing incontinence prior to SGLT2 inhibitor initiation and reinforcing hygiene and skin care strategies can reduce these risks.2,3,19
Conclusion
GUIs represent a common and clinically meaningful complication of diabetes, driven by the combined effects of hyperglycemia-related immune dysfunction, glucosuria, and diabetes-associated neurologic and structural abnormalities.1-6,13 The expanding use of SGLT2 inhibitors further underscores the need for careful risk assessment because these agents provide substantial glycemic, cardiovascular, and renal benefits while increasing susceptibility to genital mycotic infections and, rarely, severe infectious complications.8-12,15,19 Effective management therefore extends beyond treatment of active infection and requires proactive, preventive strategies embedded within routine diabetes care. DCESs and other members of the diabetes care team are uniquely positioned to translate pathophysiologic risk into practical self-care behaviors, support informed and sustained medication use, and facilitate early recognition and intervention for genitourinary symptoms.14-16 By integrating patient-centered education, anticipatory guidance, and interdisciplinary collaboration into diabetes management, care teams can reduce infection-related morbidity, promote therapeutic persistence, and optimize outcomes for people living with diabetes.15,16 ■
Footnotes
Author Contributions
Brian Burroughs conceptualized, wrote, and edited the entirety of the article.
Declaration of Conflicting Interests
None.
Funding
None.
Guarantor Statement
Brian Burroughs serves as the guarantor of this work and takes responsibility for the integrity of the content, including the accuracy of the data and analysis presented.