
Abstract

Continuous glucose monitoring (CGM) has transformed diabetes self-management by providing real-time glucose data, trend information, and actionable feedback. Beyond glycemic benefits, growing evidence demonstrates meaningful impacts in diabetes-specific psychosocial outcomes across type 1 and type 2 diabetes populations. These outcomes are particularly relevant to diabetes care and education specialists (DCESs), registered dietitians, and all other multidisciplinary diabetes care teams who support patients navigating both the benefits and challenges of diabetes technology.
Psychosocial Benefits of CGM
Recent literature consistently demonstrates that CGM is associated with reductions in diabetes distress, increased confidence in managing hypoglycemia, and decreased fear of hypoglycemia. These benefits are most pronounced in individuals with impaired hypoglycemia awareness, higher baseline A1C, or greater perceived diabetes distress at initiation.1-7 Diabetes distress refers to the emotional and behavioral burdens specifically related to living with and managing diabetes. It encompasses worries about daily regimen demands (eg, glucose monitoring, insulin dosing, dietary decisions), frustration with glycemic variability, fear of acute and long-term complications, perceived lack of social support, and concerns about access to or quality of medical care. 3
In youth and families, early CGM initiation is associated with low diabetes-related distress, increased technology acceptance, and improved confidence in diabetes management without evidence of adverse psychological effects.6,7 Adolescents and parents frequently report reductions in diabetes distress; however, emerging data suggest that adults may not experience the same magnitude of benefit, highlighting important age-related differences in psychosocial response. 7
Quality-of-life improvements associated with CGM appear to be primarily diabetes-specific rather than reflective of general health status. CGM satisfaction is strongly linked to reduced diabetes distress, increased perceived control, and improved well-being, even when general health quality-of-life measures remain unchanged.2,4,6
Emerging Psychosocial Risks and Unintended Consequences
Despite the benefits, the rapid expansion of diabetes technology introduces potential psychosocial risks that warrant careful attention. Device-related emotional burden, anxiety related to food choices, data overload, and concerns regarding disordered eating behaviors have been increasingly described.3,5,8-10 Psychiatric comorbidities, including disordered eating behaviors, are common and often underrecognized in people with diabetes and are associated with poorer glycemic and psychosocial outcomes. 9
Frequent exposure to real-time glucose values, trend arrows, alarms, and color-coded ranges may increase vigilance toward glucose fluctuations and contribute to emotional distress in some users. Precision monitoring frameworks describe how continuous feedback, although intended to enhance safety and engagement, may intensify anxiety, frustration, or self-criticism in response to expected physiologic glucose variability.8,10 Some individuals report distress when glucose values deviate from target ranges despite adherence to recommended self-management behaviors. Qualitative research suggests that CGM data may also influence eating behaviors beyond intended self-management goals. Some individuals describe modifying food choices, portion sizes, or meal timing primarily to avoid glucose excursions rather than in response to hunger cues, nutritional adequacy, or individualized nutrition guidance.8,11 In this context, food choices may become driven by glucose trends rather than flexibility or balance, potentially increasing nutritional risk and psychological burden in susceptible individuals.
Although no evidence establishes a causal relationship between CGM and eating disorders, overlap exists between CGM-related behaviors, such as hypervigilance, glucose avoidance, and self-judgment, and known risk factors for disordered eating. These patterns may be more likely to emerge in specific subgroups, including individuals with elevated anxiety, perfectionism, or prior disordered eating behaviors, and may remain undetected in studies focused primarily on glycemic outcomes.5,8-10,12
Clinical Vignette
A 38-year-old woman with type 1 diabetes treated with a basal-bolus insulin regime initiates real-time CGM to improve glycemic awareness. Within weeks, her time in range improves, and hypoglycemia is reduced. However, during follow-up with the DCES, she reports increasing anxiety around meals. She describes avoiding carbohydrate-containing foods, skipping meals, and feeling significantly distressed when postprandial glucose values exceed her target range despite following nutrition recommendations.
Review of CGM data shows expected postprandial excursions that are resolved within 2 hours. Further discussion reveals that the patient checks CGM values frequently and interprets transient elevations as personal failure. Formal assessment using the validated 17-item Diabetes Distress Scale identified elevated diabetes distress, particularly in the domains of emotional burden and regimen-related distress. Formal assessment using the validated 16-item Diabetes Eating Problem Survey–Revised did not reveal concerns for an eating disorder.
Despite targeted diabetes self-management education and support (DSMES), including normalization of physiologic glucose variability, emphasis on meal composition rather than single foods, and collaboration with a registered dietitian to support flexible nutrition strategies, the patient continued to report intrusive thoughts about glucose values and persistent food-related anxiety. She notes that although she appreciates the time she spends with the multidisciplinary care team, she spends more time with her glucose values than the team and struggles to disengage from the CGM device.
After shared decision-making, the care team and patient agree to pause CGM use and return to intermittent glucose monitoring while continuing DSMES and addressing underlying diabetes distress. The patient reports reduced anxiety around eating and improved quality of life following this change. Plans are made to reassess CGM readiness in the future as her confidence and distress improve.
Role of DCESs and Registered Dietitians
DCESs and registered dietitians play a critical role in contextualizing CGM data and mitigating psychosocial risk. Nutrition counseling should emphasize that postprandial glucose responses reflect overall meal composition rather than isolated foods. Carbohydrate-containing foods do not need to be universally avoided, and steadier glucose excursions may be seen when carbohydrates are paired with protein, fiber, and fat. CGM trends should be interpreted within the complexity of mixed meals, portion sizes, interaction and timing of diabetes medications, physical activity, and individual variability rather than as a judgment of food quality or personal success.13,14 When CGM use is associated with significant distress, anxiety, or maladaptive behaviors, a temporary pause or modification of CGM use, guided by clinical judgment and shared decision-making, may be appropriate while psychosocial supports are addressed. At this juncture, DCESs should recognize clinical thresholds that warrant timely communication and collaboration with primary care and behavioral health colleagues, particularly when CGM-related distress intersects with worsening glycemic levels, disordered eating behaviors, mood symptoms, or impaired self-management.
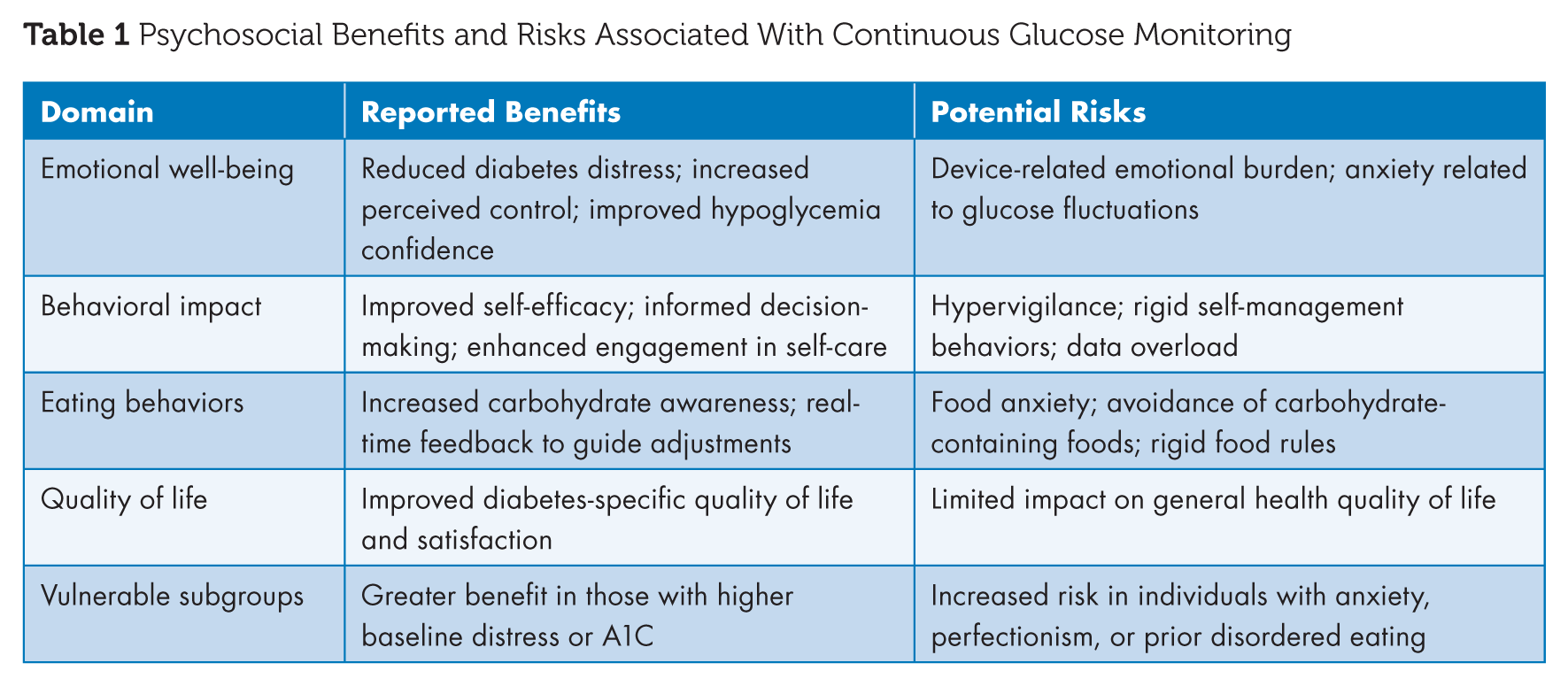
Routine assessment of diabetes distress and eating disorders also provides an opportunity to identify when interdisciplinary collaboration with primary care and behavioral health is needed to support both metabolic and psychological safety.2,9 DSMES, particularly when individualized and behaviorally informed, can be effective in reducing diabetes distress and improving both psychosocial and glycemic outcomes.2,9,15 Technology-enabled DSMES, including telehealth and virtual platforms, can further enhance access and ongoing support. See Table 1.
Psychosocial Benefits and Risks Associated With Continuous Glucose Monitoring
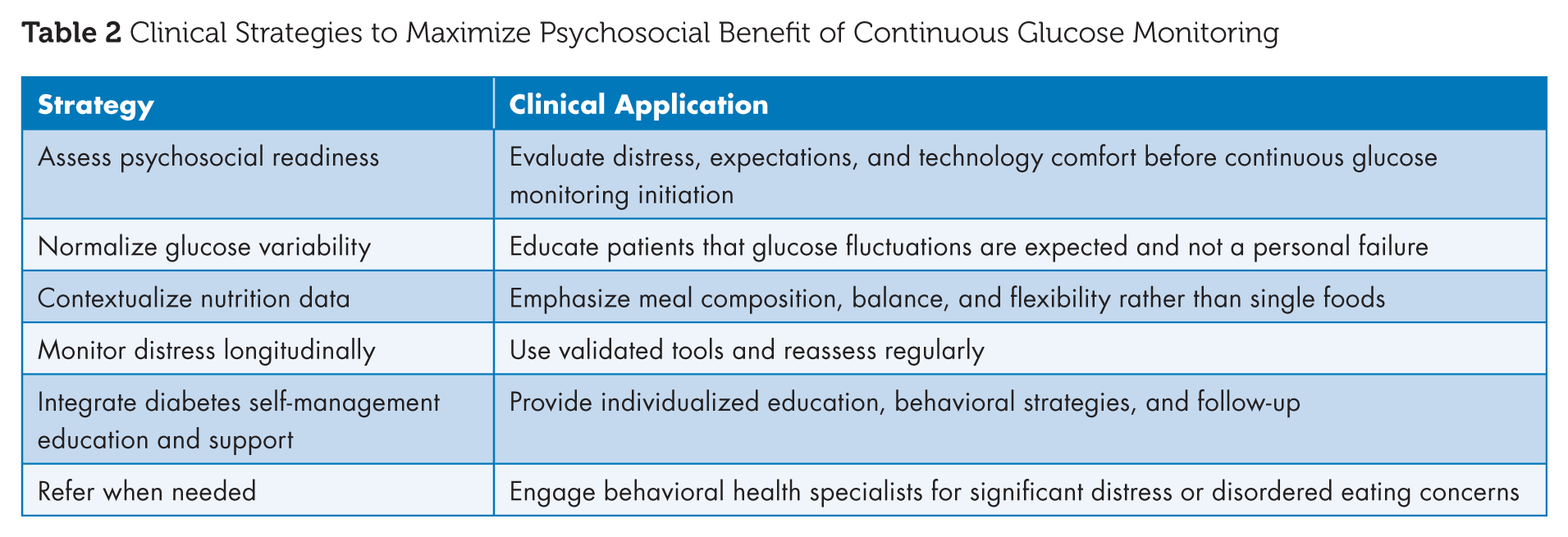
Precision monitoring approaches that combine CGM data with behavioral and mental health metrics may enable just-in-time adaptive interventions, targeting support to those most at risk for psychosocial complications. 8 Care teams should systematically assess technology readiness, equity in access, and patient-reported outcomes to ensure that technological advancement translates into improvements in both glycemic outcomes and well-being.3,5 See Table 2.
Clinical Strategies to Maximize Psychosocial Benefit of Continuous Glucose Monitoring
Conclusion
CGM offers substantial psychosocial benefits for many individuals with diabetes, including reduced distress, enhanced confidence, and improved engagement in self-management. However, emerging evidence and clinical experience highlight the potential for unintended psychosocial and eating-related consequences in some users. Systematic screening for diabetes distress and disordered eating using validated tools should accompany CGM initiation and follow-up to identify individuals at increased psychosocial risk. Recognizing individual variability in response to continuous glucose data and integrating DSMES, nutrition expertise, and behavioral health support are essential to ensuring that CGM adoption translates into improved well-being alongside improved glycemic outcomes. Integrating CGM data with psychosocial metrics further underscores the importance of coordinated communication among DCESs, primary care clinicians, and behavioral health professionals to ensure that emerging risks are addressed early and holistically. ■
Footnotes
Author Contributions
Angie Clinton served as the primary and senior author, led manuscript conceptualization, and authored sections addressing emerging evidence, dietary considerations, and gaps in the literature. Brian Burroughs contributed subject-matter expertise and authored sections synthesizing the existing evidence base and describing the benefits of continuous glucose monitoring. All authors critically reviewed, edited, and approved of the final manuscript.
Declaration of Conflicting Interests
None.
Funding
None.
Guarantor Statement
Angie Clinton serves as the guarantor of this work and takes responsibility for the integrity of the content, including the accuracy of the data and analysis presented.