
Abstract


Cardiovascular disease (CVD) is the leading cause of death in the United States, and one of the most modifiable risk factors for CVD is hypertension. A diabetes care and education specialist (DCES) commonly encounters this condition as they holistically help people with diabetes improve their cardiometabolic health. New recommendations from the 2025 hypertension guideline developed by American Heart Association (AHA) and American College of Cardiology (ACC) stress the urgent need to improve hypertension care. Perhaps most concerning are the hypertension control rates that estimate only 46.7% of people with hypertension in the United States are able to achieve a blood pressure (BP) <130/80 mm Hg. 2
Hypertension and diabetes are common overlapping comorbidities. The 2025 ACC/AHA guideline highlights the Framingham Heart Study, which found 50% of adults with diabetes were previously diagnosed with hypertension. 3 The cardiovascular risk is additive because both hypertension and diabetes independently increase the risk for adverse outcomes. Consequently, holistic care of people with diabetes requires dual management of BP and blood glucose.
The purpose of this article is to provide an overview of the important updates from the 2025 ACC/AHA hypertension guideline related to the management of people with diabetes.
Measurement and Blood Pressure Staging
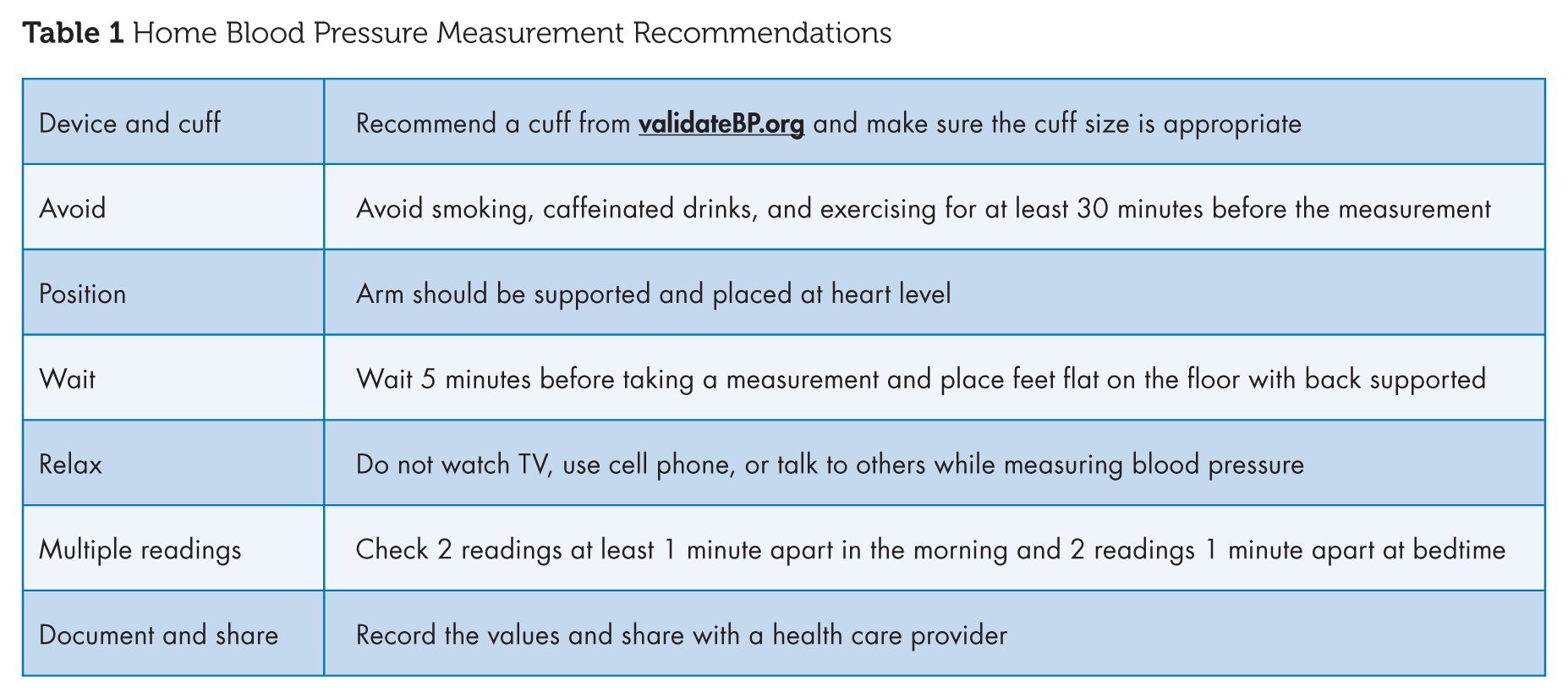
The 2025 ACC/AHA guideline recommends patients monitor their out-of-office BP to detect white coat and masked hypertension. Ambulatory blood pressure monitoring (ABPM) and home blood pressure monitoring (HBPM) are the methods proposed by the 2025 ACC/AHA guideline for checking BP at home. An ABPM is worn by the patient for 24 hours and automatically checks BP at select intervals, including morning and nighttime readings. ABPM has traditionally been considered the gold standard for measuring BP outside of the clinic setting but is not often readily available, and studies have failed to demonstrate a consistent benefit over HBPM. As shown in Table 1, HBPM requires individuals to check their blood pressure at select times over 7 days to determine an average BP. It is important that validated devices are utilized to ensure readings are accurate. A list of validated devices can be found at validatebp.org. 2
Home Blood Pressure Measurement Recommendations
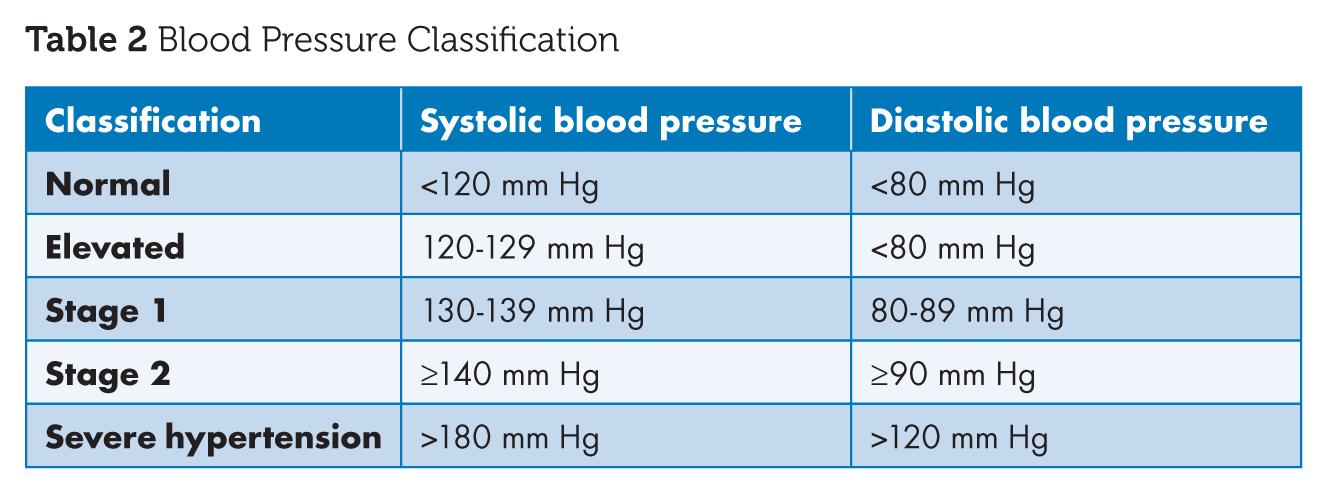
Office-based measurements remain the most common method for evaluating BP. Automated oscillometric devices with validated algorithms continue to be preferred over auscultatory methods in the 2025 ACC/AHA guideline. Importantly, at least two readings on separate occasions are needed for appropriate evaluation of blood pressure. The classification of high BP based on office readings is listed in Table 2. Despite the emphasis on automated office devices, errors in patient preparation and technique can still result in inaccurate measurements in practice. 2 Given the importance and complexity of measuring BP, the DCES is well positioned to aid in proper assessment and monitoring practices to ensure optimal patient outcomes.
Blood Pressure Classification
Updates to Assessing Risk in People With Hypertension
The 2025 hypertension guideline adopted the Predicting Risk of Cardiovascular Disease Events (PREVENT) calculator as the primary tool for risk assessment. The are 3 PREVENT calculators developed by AHA: (1) PREVENT CVD, (2) PREVENT ASCVD (atherosclerotic cardiovascular disease), and (3) PREVENT HF (heart failure). Specifically, the PREVENT CVD calculator is recommended to estimate a patient’s risk of CVD, including heart attack, stroke, and HF. The AHA developed the PREVENT calculator using patient-level data between 1992 and 2017 from 25 data sets involving over 3 million people. Khan et al 4 authored the AHA document and also reported the PREVENT calculator model was externally validated with an additional 21 data sets, meaning that collectively, the PREVENT calculator was tested in over 6 million individuals. 2 Importantly, the PREVENT CVD calculator replaces the ASCVD risk estimator plus calculator based on pooled cohort equations (PCE) previously recommended in the 2017 ACC/AHA guideline. 5
Several key differences exist between the ASCVD risk estimator plus and the PREVENT calculator. The PREVENT CVD calculator includes short-term (10-year) and long-term (30-year) estimates for total CVD, including HF and ASCVD, whereas the ASCVD risk calculator estimates the 10-year and lifetime risks for ASCVD (stroke, myocardial infarction, or death from either). Whereas the ASCVD risk plus calculator included race, the PREVENT calculator eliminated this factor and instead included an option to enter the patient’s zip code to capture the risk from social determinants of health. Removing race from the risk calculator allowed for the elimination of race as a biological predictor of CVD rather than the social construct that it is. The PREVENT calculator also includes the option to input a patient’s estimated glomerular filtration rate (eGFR), hemoglobin A1C, and urine albumin creatinine ratio. Finally, the PREVENT calculator can estimate the risk of CVD for patients as young as 30 years, which is 10 years younger than the ASCVD risk calculator. Understanding the variables and outcomes associated with risk assessment tools is essential for clinicians to develop treatment plans and to educate patients on their estimated risk. 4
Risk-Based Decision-Making
For individuals with stage 1 hypertension without comorbidities, a PREVENT CVD estimate should be calculated. Pharmacological treatment is recommended at a threshold of 7.5%. If the PREVENT CVD score is <7.5%, a trial of nonpharmacological therapy should occur for 3 to 6 months. Importantly, this is a lower threshold than the previously recommended 10% ASCVD risk using the PCE. People with clinical CVD, chronic kidney disease (CKD), diabetes, or a PREVENT 10-year risk >7.5% should initiate pharmacological treatment immediately at stage 1 hypertension. 2
Nonpharmacologic Therapy
Once an adult is diagnosed with hypertension, it can lead to microvascular damage, which reinforces the importance of prevention achieved through nonpharmacologic therapies, especially in adults with elevated BP. Nonpharmacologic interventions are largely consistent with the previous 2017 ACC/AHA guideline, and they remain a foundational aspect of BP management. 5 However, lifestyle changes are not only beneficial for adults without hypertension. These interventions can delay worsening of hypertension and reduce pill burden. The four main approaches to lifestyle interventions are nutrition changes, specifically, following a DASH (dietary approaches to stop hypertension) eating pattern, reducing alcohol intake, increasing physical activity, and reducing stress. Alongside the 4 main approaches to lifestyle interventions, weight loss is recommended. All adults who meet criteria for overweight or obesity are recommended to lose at least 5% of their body weight. Improvement in any 1 lifestyle factor listed has the ability to decrease BP and should be discussed as part of the hypertension treatment plan. 2
Several new lifestyle recommendations are noteworthy in the 2025 ACC/AHA guideline. Potassium-based salt substitutes (eg, potassium chloride, KCl) are an evidence-based strategy that lowers sodium consumption while experiencing the benefits of potassium. Importantly, this strategy is not recommended in people with CKD due to the risk of hyperkalemia. Stress management through transcendental meditation, yoga, and breathing exercises have also shown beneficial effects on BP reduction. Lastly, stronger guidance for avoiding any amount of alcohol is optimal for reducing BP. These recommendations are several highlights for nonpharmacological management, but readers are encouraged to review the full ACC/AHA guidelines section on nonpharmacological management interventions. 2
Pharmacotherapy Management
Adults with stage 1 hypertension should start with a single antihypertensive agent. Most adults with stage 2 hypertension or blood pressures ≥20/10 mm Hg above goal should begin drug therapy with 2 antihypertensive medications rather than monotherapy. Dual therapy achieves faster BP reduction and improves the likelihood of reaching BP goals. To reduce barriers to optimal medication administration, the ACC/AHA guidelines strongly favor the use of single-pill combination (SPC) therapy whenever possible. Importantly, there are many generic SPC available, which offers an affordable treatment for many. Treatment with SPC therapy also reduces pill burden and increases the ability of the patient to take medications as prescribed while maximizing therapeutic benefit compared to prescribing the same agents as separate medications. 2 The emphasis on SPC is an important change with many available treatment options. The DCES is a valuable resource in helping patients and providers identify SPCs to reduce costs and simplify medication administration.
Initial drug therapy, including for those with diabetes, continues to include angiotensin-converting enzyme inhibitors (ACE-Is), angiotensin II receptor blockers (ARBs), long-acting dihydropyridine calcium channel blockers, and thiazide-type diuretics. The preference for these medication classes is based on their tolerability, BP lowering, and cardiovascular benefit. Other antihypertensive treatment options should only be considered after the initial treatment choices are exhausted, including beta blockers, unless there is a compelling indication necessitating a specific treatment (eg, heart failure with reduced ejection fraction and beta blocker treatment). 2
Most adults diagnosed with hypertension, especially those with diabetes, are encouraged to reach a BP goal of ≤130/80 mm Hg, and medication should be initiated if their BP is above 130/80 mm Hg. Additionally, more stringent systolic BP (SBP) goals have been linked to a decrease in the incidence of CVD and total mortality; thus, the 2025 ACC/AHA guideline encourages a more intensive BP goal of <120/80 mm Hg. Adults with hypertension and diabetes who develop CKD are indicated for ACE-Is or ARBs. The guideline defines CKD by an eGFR <60 mL/min/1.73 m2 or the presence of albuminuria ≥30 mg/g. In patients with CKD, ACE-Is and ARBs lower the amount of urine protein levels, increase time to the development of end-stage kidney disease, and reduce cardiovascular events. 2
The ACC/AHA guideline also provides updates on the diagnosis and treatment recommendations for patients with resistant hypertension. Resistant hypertension is defined as a person undergoing treatment with 3 or more hypertensive agents, including a diuretic, who continues to have elevated BP that is above goal or those who are on 4 or more antihypertensive medications with BP at goal. Before patients can be identified as having resistant hypertension, clinicians must first rule out pseudoresistance. Common causes of pseudoresistant hypertension include inaccurate BP measurements, white coat hypertension, medication interactions, and inadequate medication administration. 2 It is important to assess for adequate medication-taking behaviors before treating resistant hypertension. Individuals with resistant hypertension have a 50% increased risk of developing secondary hypertension, CVD, or end-stage kidney disease. 6 Once a resistant hypertension diagnosis is established, a long-acting thiazide diuretic (chlorthalidone or indapamide) should replace hydrochlorothiazide. Evaluation for secondary causes of hypertension, including primary aldosteronism, should also occur. 2 Mineralocorticoid receptor antagonists (MRAs) are the drug class of choice for the treatment of resistant hypertension based on the PATHWAY-2 trial, which showed spironolactone was more efficacious than bisoprolol (beta blocker) and doxazosin (alpha-1 blocker). Referral to a hypertension specialist may be considered, especially when MRAs are not tolerated. 7
Antihypertensive Effects of Diabetes Agents
There are several medications for diabetes that demonstrate beneficial effects on BP. One class of agents includes the glucagon-like peptide-1 (GLP-1) + glucose-dependent insulinotropic polypeptide receptor agonists (RAs), which often are also approved for obesity. While weight loss is the main driver of lowering BP with GLP-1 RAs, it is not likely the sole mechanism. The BP lowering effects reported with GLP-1 RAs in clinical trials are variable, especially in people with and without diabetes. In a systematic review by Kennedy et al, 8 the SBP and diastolic blood pressure (DBP) lowering of GLP-1 RAs was approximately 5 mm Hg and 2 mm Hg, respectively. Because the weight loss effects are generally less in people with diabetes, the BP lowering effects are also attenuated. Importantly, weight loss is gradual with these agents, and maximal BP reduction may not occur for several months once patients reach their optimal dose. Careful monitoring of BP should occur for patients on antihypertensives to assess the need for deprescribing.
The sodium glucose transport-2 inhibitors (SGLT2is) have several indications beyond diabetes management, including HF and CKD, and SGLT2is are also associated with improvements in BP. A systematic review by Baker et al, 9 found that the use of SGLT2is in people with type 2 diabetes reduced SBP and DBP by approximately 4 mm Hg and 1.6 mm Hg, respectively. Initial BP lowering effects of SGLT2is are predominantly due to natriuresis, with other mechanisms likely contributing to sustained reductions in BP over time. Because people with hypertension and diabetes often have a high medication burden, clinicians should prioritize agents with the dual purpose of lowering BP and improving glycemic control.
Evidence Supporting Changes in Treatment Goals
The 2017 ACC/AHA guideline lowered the blood pressure goal for most individuals, including those with diabetes, to <130/80 mm Hg; however, the 2025 ACC/AHA guidelines now recommend to further aim for a SBP <120 mm Hg in patients who are at a high cardiovascular risk, including those with diabetes.2,5 Importantly, this recommendation referred to individuals already at or below the 130/80 mm Hg and tolerating antihypertensive treatment. Further intensifying blood pressure goals to <120/80 mm Hg in these populations has consistently shown to reduce major cardiovascular outcomes with only a mild increase in adverse effects in clinical trials (Table 3).
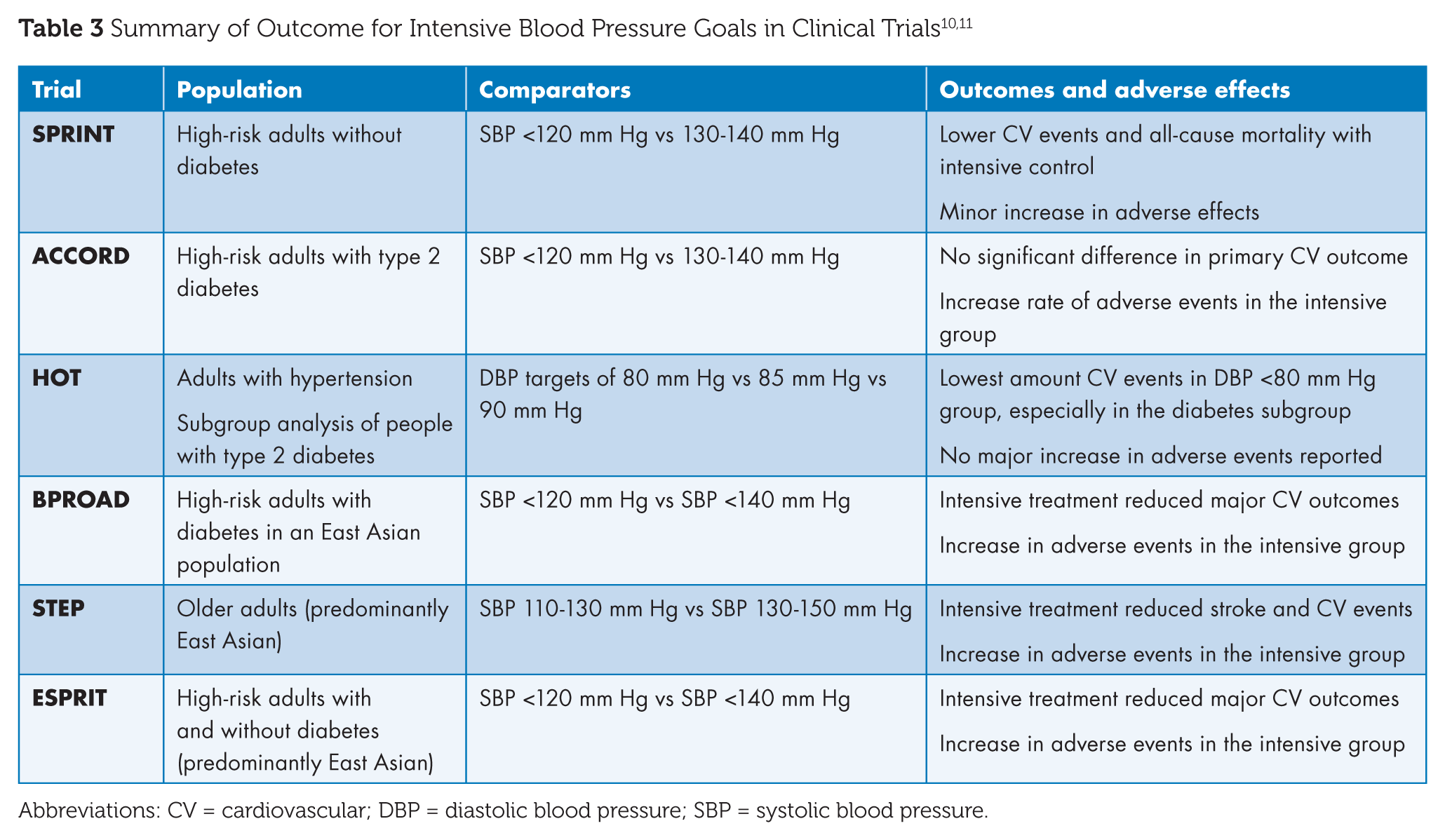
Abbreviations: CV = cardiovascular; DBP = diastolic blood pressure; SBP = systolic blood pressure.
A recent meta-analysis by Guo et al 10 summarized the safety and efficacy outcomes of more intensive BP goals (SBP <120 mm Hg and <130 mm Hg) from ACCORD BP, SPRINT, ESPRIT, BPROAD, STEP, and CRHCP. The analysis demonstrated that intensive SBP goals produced a relative risk reduction in major cardiovascular events by approximately 24% compared to standard targets and an absolute risk reduction of 1.73% (NNT 58). Although adverse events had an absolute increase of 1.82% (NNH 55), the most common adverse events were acute kidney injury and reduction in kidney function. 10 Together, these findings reinforce guideline recommendations for a BP goal <130/80 mm Hg and an SBP goal <120 mm Hg in select high-risk patients who tolerate treatment.
Conclusion
The 2025 ACC/AHA guidelines provide important updates while maintaining many recommendations from the 2017 ACC/AHA guidelines. Perhaps the biggest changes for clinicians to adopt are related to the new PREVENT CVD calculator and the targeting of a lower SBP goal (<120 mm Hg) when possible. Intensive BP targets were previously debated, but the addition of several recent randomized controlled trials has solidified the concept that lower SBP is better as long as it can be safely attained. Importantly, the 2026 American Diabetes Association Standards of Care adopted similar language regarding SBP goals and received an endorsement from the American College of Cardiology. 12 Together, clinical practice recommendations are harmonizing their recommendations for more intensive treatment of patients with hypertension, especially in people with diabetes. ■
Footnotes
Author Contributions
Declaration of Conflicting Interests
None.
Funding
No funding was given for this article.
Guarantor Statement
The corresponding author takes full responsibility for the accuracy of the information and integrity of the article.