
Abstract
Aneurysm of the extracranial carotid artery is a rare disease, mycotic pseudoaneurysms being even less common. They are a life-threatening complication of systemic infection and atherosclerosis. Immunocompromised people, including patients with HIV, uncontrolled diabetes melltus, those on immunosuppressants like high-dose steroids, and chemotherapy, are at a higher risk for development of mycotic pseudoaneurysms. Due to the high risk of potential complications like rupture and thromboembolic events, mycotic aneurysms always require surgical management. Early detection followed by restoration of blood flow is critical to minimize a fatal outcome. Here we report the case of a 52-year-old man with a past history of hypertension and dyslipidemia who presented with a pulsatile painful neck swelling. On evaluation, the patient was diagnosed to have Salmonella typhi bacteremia, HIV infection, and a mycotic aneurysm of the left common carotid artery.
Introduction
Mycotic aneurysm, a term described by Osler in 1885, denotes a false aneurysm on a vessel associated with an infection. The common pathogens in Western countries are Staphylococcus aureus (28%), Salmonella spp (15%), and Pseudomonas aeruginosa (10%), while most Asian countries have constantly reported Salmonella as the most common pathogen. 1
The most common site of a mycotic aneurysm is the femoral artery (38%), followed by the abdominal aorta (31%). Carotid artery aneurysms account for only 5% of cases. 2
Aneurysms of the extracranial carotid artery are rare; mycotic aneurysms are even less frequent. Though rare, aneurysms of the carotid artery can have fatal outcome, thereby making surgical correction necessary to prevent possible rupture, embolization, or death. Primary resection of the aneurysm with autologous vein interposition, in association with prolonged antibiotic therapy, is the preferred mode of treatment. 3
Here we describe a case of mycotic aneurysm of the common carotid artery due to Salmonella typhi bacteremia in a 52-year-old, treatment naïve HIV patient.
Case Report
A 52-year-old man with a past medical history of hypertension and dyslipidemia presented to our hospital with fever and a painful left-sided neck mass of 2 weeks duration. He had developed a feeling of generalized tiredness, and high-grade fever with chills and night sweats from the last 14 days before admission along with a rapid increase in the size of the neck mass over the last 7 days. He had developed low-grade fever and intermittent diarrhea for the past 1 month, for which he was prescribed multiple oral antibiotics without proper evaluation. He denied history of neck trauma or intravenous drug abuse. On physical examination, he was febrile, diaphoretic, poorly nourished, with a temperature of 38.1 °C, increased pulse rate of 116 bpm, and blood pressure of 110/70 mmHg. He had a 6×5 cm tender, inflamed pulsatile mass on the left side of neck with a systolic bruit on auscultation. There was no focal neurological deficit and the rest of the examination was unremarkable except for the presence of oral candidiasis and hepatosplenomegaly.
Routine investigation showed neutrophilic leukocytosis with normocytic normochromic anemia. His erythrocyte sedimentation rate and C-reactive protein were well above normal limits. An ultrasound scan of the neck was done, which revealed a focal outpouching from the wall of the left common carotid artery. A doppler study of the neck vessels showed normal color flow in the CCA, as well as in the saccular outpouching with no filling defects or echogenic material.
He was admitted to the intensive care unit and treated with intravenous fluids and empirical broad spectrum antibiotics in view of suspected infection.
CT angiogram revealed a multilobulated aneurysm in the left common carotid artery. The blood cultures drawn from the patient grew Salmonella typhi, sensitive to ceftriaxone, chloramphenicol, and ciprofloxacin. A transthoracic echocardiogram showed no evidence of infective endocarditis. WIDAL O titer was 1:640. USG abdomen showed mild hepatosplenomegaly. His Retro ELISA test was positive for HIV-1 and CD4 count was 60/cm.
The history of persistent fever and a rapid increase in the size of the aneurysm, in an immunocompromised patient with Salmonella typhi bacteremia led to the diagnosis of a mycotic pseudoaneurysm of the left common carotid artery. An emergency vascular surgery consultation was sought, and a need for immediate surgery was advised. Despite persuasion, the patient and bystanders were unwilling for surgical intervention. He was continued on intravenous antibiotics. The patient developed rupture of the aneurysm and expired 2 weeks after admission.

Left common carotid artery bifurcation appears normal with normal appearing internal carotid artery and external carotid artery. The right common carotid artery appears normal.
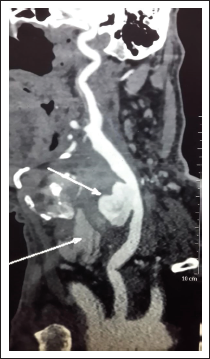
The aneurysmal sac shows normal contrast opacification with no filling defects. The remaining portion of the CCA appears normal in calibre. No significant luminal narrowing/irregularity noted. No thrombosis/contrast extravasation/adjacent hematoma noted.
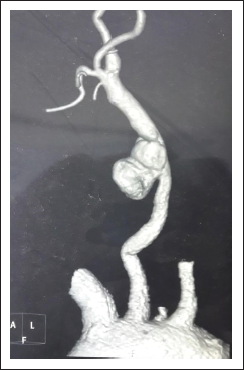
VRT Image—The Arch of Aorta with the Brachiocephalic Trunk, the Left Common Carotid Artery and Left Subclavian Artery Arising Normally.
Discussion
Mycotic aneurysms are defined as a localized, irreversible dilatation of an artery caused by destruction of the vessel wall by infection. A primary mycotic aneurysm develops following infection of a previously healthy arterial wall, while a secondary mycotic aneurysm refers to the secondary infection of a pre-existing aneurysm. 4
The term “mycotic” was described by Willaim Osler in 1885 in his Gulstonian lectures, where he described multiple aortic aneurysms in a patient with infective endocarditis. The name refers to their gross appearance, resembling that of a fleshy fungus and not to their etiology, as bacterial pathogens are considered to be responsible for the majority of infected aneurysms. He has explained their pathogenesis to be the destruction of the arterial wall by embolization of infected material arising in the heart. 5
Several mechanisms have been proposed for the pathogenesis of infection of an arterial wall including:
There has been a paradigm shift in the etiology of mycotic aneurysms from untreated infective endocarditis, tuberculosis, and syphilis being the most common cause in the preantibiotic era, to arterial trauma including angiographic procedures, intravenous drug abuse, and dental extractions in the modern era.4, 7
Blood cultures are positive in 50% to 85% of the cases. The common pathogens reported in Western countries are S. aureus (28%), Salmonella spp (15%), and P. aeruginosa (10%), while most Asian countries have reported Salmonella as the most common pathogen for mycotic aneurysms.1, 6
Endovascular involvement though, a rare complication of Salmonella bacteremia, can result in significant morbidity and mortality. Nontyphoidal Salmonella gastroenteritis is known to cause bacteremia in up to 8% of patients, with immunodeficiency as the major risk factor. Endovascular complications are seen to develop in 10% to 25% of patients older than 50 years of age with Salmonella bacteremia.4, 8, 9
Old age, atherosclerosis, diabetes mellitus, hypertension, peripheral occlusive vascular disease, and previous ischemic stroke include the major risk factors predisposing to endovascular complications in salmonellosis. Persistent bacteremia in a patient with underlying atherosclerotic disease increases the risk for endovascular infection.4, 10
The presence of risk factors like AIDS, hypertension, and dyslipidemia points to a possible underlying atherosclerotic disease in our patient that must have facilitated endovascular infection from Salmonella bacteremia and subsequent development of the mycotic aneurysm.
The pathogenesis of endovascular involvement in salmonellosis has been explained to include 3 steps. The bacterium uses fimbriae for attachment to intestinal epithelial cell membranes, following which they are phagocytosed by lymphoid tissue, followed by dissemination via the hematogenous or lymphatic route. The mechanism of the final step, which includes the progression from bacteremia to endovascular infection, remains vague. 4
The femoral artery is the most commonly involved site of a mycotic aneurysm (38%), followed by abdominal aorta (31), superior mesenteric (8%), brachial (7%), and iliac (6%) arteries. The carotids are involved in only 5% of mycotic aneurysms.6, 11, 12
Mycotic aneurysms of the carotid artery are infrequent with only a few cases reported in the literature. Timely diagnosis followed by prompt surgical management influences the outcome of the patient. A high index of suspicion is necessary for the diagnosis of carotid mycotic aneurysms given its varied and nonspecific presentation.
Carotid mycotic aneurysms present as a rapidly enlarging pulsatile neck mass associated with pain, tenderness, hoarseness of voice, dysphagia, and systemic features of infection, including high-grade fever and chills. Signs of infective aneurysm of the carotid artery include recurrent, undiagnosed oropharyngeal bleeding, slow or incomplete resolution of an appropriately treated neck infection, a neck mass expanding over hours, hemoglobin lower than clinically expected, purplish or brown discoloration of the skin or mucosa in the region, presence of bruit or thrill, 10th or 12th cranial nerve palsy, and Horner’s syndrome.2, 3, 13, 14
Differential diagnosis of a neck mass includes cervical lymphadenitis, carotid body tumor, peritonsillar abscess, or internal carotid artery kinking.2, 3, 14, 15
These can be differentiated and the diagnosis confirmed with a duplex ultrasound or arteriography. Computed tomography angiogram remains the gold standard and magnetic resonance imaging/magnetic resonance angi-ography is also useful. 3
Surgical treatment should be the mainstay of treatment, as, without surgery, there is a high risk of rupture, hemorrhage, and thromboembolic complications (septic emboli to the brain) with obvious neurologic sequelae, and mortality rates reaching 70% to 90%.3, 16
Conclusion
Mycotic aneurysm involving the extracranial carotid artery is an extremely rare, life-threatening complication of Salmonella typhi bacteremia. Patients at high risk of developing mycotic aneurysms include the elderly with underlying diabetes mellitus, hypertension, atherosclerosis, and immunosuppression. A high level of clinical suspicion is required for the timely diagnosis and though rare, a mycotic carotid aneurysm must be considered as a differential diagnosis while evaluating tumors of the neck in these patients. Surgical treatment with prolonged antibiotic cover remains the mainstay of treatment. Despite its high mortality, early surgery and reconstitution of blood flow is associated with a good outcome with minimal neurological sequelae.
Footnotes
Author Contribution
Conceptualization, design, writing-original draft preparation: SPN; design, writing-reviewing and editing, supervision: AR; writing-reviewing and editing: AG; writing-reviewing and editing: KVS; design, writing-original draft preparation: SS. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.