
Abstract
Longitudinal extensive transverse myelitis is defined as a spinal cord lesion that extends over three or more spinal segments. Varicella zoster virus is an exclusively human neurotropic virus that reactivates following the weaning of cell-mediated immunity as age advances, resulting in herpes zoster. We report the case of a 61-year lady presenting with dorsal cord longitudinally extending transverse myelitis following herpes zoster infection that resolved with immunomodulation and antivirals.
Introduction
Herpes zoster is caused by the reactivation of latent virus in the sensory ganglia with subsequent spread along the nerves. The neurological complications associated with herpes zoster include post-herpetic neuralgia, stroke, vasculitis, encephalitis, and myelitis. The re-emergence of herpes infection after the covid pandemic has been remarkable. Among the neurological complications, myelitis has been reported in 0.3%. 1 We report the case of a woman who developed transverse myelitis 2 months post herpes infection to highlight the prolonged latent period between dermatological and neurological presentations.
Case
This 61-year-old, right-handed lady without comorbidities developed a left D4 Herpes zoster 2 months prior to the presentation. She was managed with antiviral valacyclovir 1 g three times a day for seven days. She presented now with asymmetric sensory symptoms with numbness and decreased temperature sensation over the right thigh for 10 days prior to the presentation. The sensory loss progressed to involve the left thigh and ascended up to involve the anterior abdomen till D4 distribution over the next three days. Simultaneously she developed heaviness of the right lower limb and weakness with bladder involvement with difficulty in initiating micturition and urinary urgency.
On examination, she had healed herpes lesions in the left D4 dermatome. Her cranial nerves including fundus examination were normal. She had asymmetric spasticity (right > left) of lower limbs with exaggerated knee and ankle jerks and ill-sustained ankle clonus. Abdominal reflex was absent in all quadrants and plantar reflex was extensor on the right side. Sensory examination revealed dissociated and suspended sensory loss from the D4-L3 dermatome. The loss was partial in D4-D8 and total from D8-L3. There was no evidence of the autonomic system or cerebellum affection.
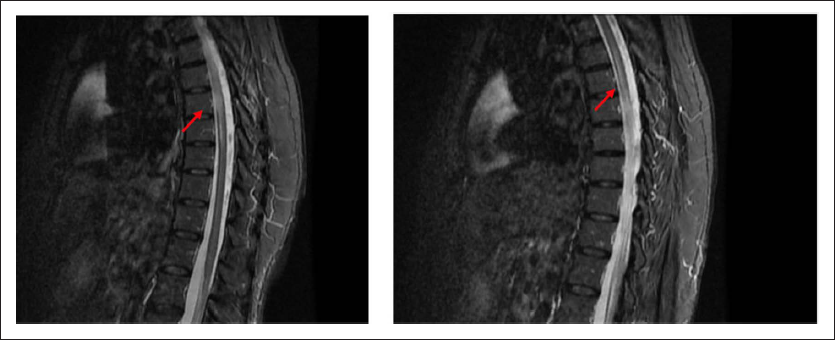
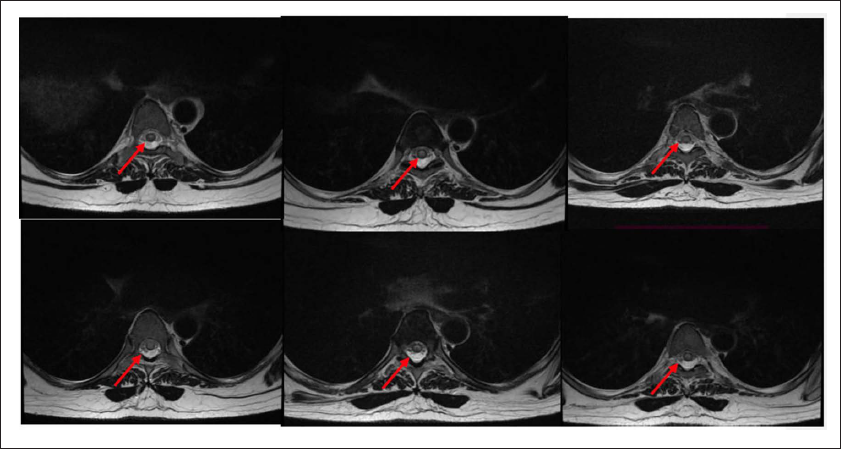
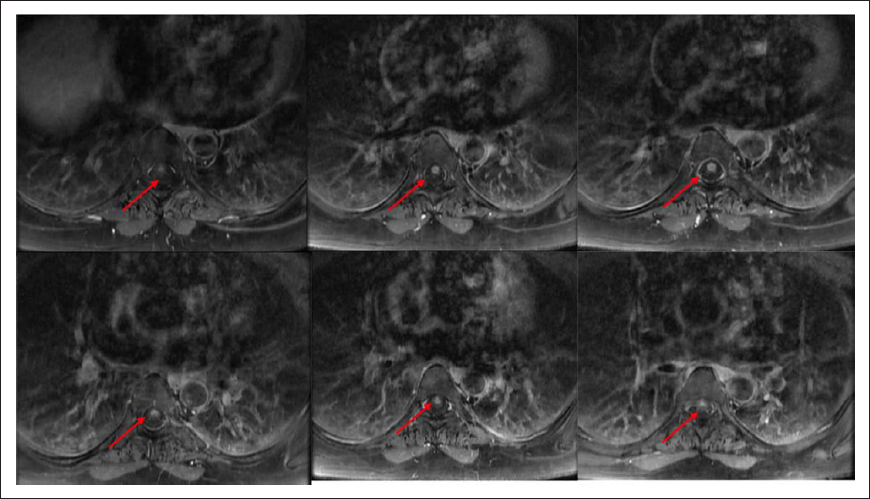
Her routine blood investigations including blood count, renal function, liver function, erythrocyte sedimentation rate, C-reactive protein, and thyroid function were normal. Serum ACE was normal. MRI Dorsal spine showed T2 hyperintensity affecting the central cord from the D4-D8 region with intense post-contrast enhancement (Figures 1–3). There was no diffusion restriction in the affected region. Her MRI brain was normal.
MRI T2 STIR Sagittal Section Showing Central Hyperintensity Extending from D4-D8 (Arrows).
Axial T2 Showing Central Cord Hyperintensity Extending from D4-D8 (Arrow).
Axial T1 Post Contrast Showing Intense Enhancement of Central Cord Extending from D4-D8 (Arrow).
CSF was acellular with normal protein and sugar. CSF Varizella zoster DNA PCR was negative. IGG index was elevated (0.76; Normal < 0.45). IGG Varicella zoster antibody was positive in CSF (449.5). Workup for connective tissue markers including ANA, C-ANCA, P-ANCA, and compliment assay was negative. Anti-NMO and anti-MOG antibody was negative in serum. CSF did not show oligoclonal bands and the IGG index was elevated (0.76).
Considering the possibility of post-infectious longitudinally extending transverse myelitis, she was initiated on 5 days of intravenous steroids (methylprednisolone 1 g/day) followed by oral steroids. She recovered completely over the next three weeks and was asymptomatic in the last follow-up, six months post-discharge.
Discussion
Varicella zoster virus (VZV) causes chickenpox in younger children. As a neurotrophic virus, it resides in the dormant dorsal root ganglia and is reactivated at a later date, resulting in herpes zoster. With age, the cell-mediated immunity wanes off and the virus gets reactivated causing herpes zoster causing widespread inflammatory damage to the neuraxis involved. 2 From the fourth to the eighth decade of life, the incidence of herpes zoster increases from 3.4 to 11 cases per 1000, indicating the role of acquired immunity in its prevention. 3
The virus replicates in the dorsal root ganglia and spreads along sensory nerve roots through axonal transport, initiating a cascade of inflammatory changes. 4 Multiple mechanisms have been postulated to cause myelitis in herpes infection. This includes direct invasion as well as vascular and allergic mechanisms.5–7 Myelitis level and the dermatomal level of herpes are concordant in most of the cases, probably supporting the hypothesis of direct spread. The development of myelitis usually shows a latent period of one-two weeks.8,9
The presence of viral particles in the CSF during the acute phase, as proven by varicella zoster DNA PCR or IG G detection, could contribute to the diagnosis. 10 There have been cases reported in the literature where PCR for VZV DNA and antibody, viral isolation, and viral culture can all be negative. 11 For example, in our case, where the above findings are absent and with a history of zoster infection, imaging studies may come in handy where MRI findings include a diffuse increase in the T2 weighted signal intensity throughout the affected segments. 12
Our patient had a typical herpes rash, which was followed by an odd long latent period of 2 months. The imaging findings of intense post-contrast enhancement, usually seen in infective myelitis, were perplexing. However, the negative PCR results for VZV DNA and positive IGG results prompted us to consider post-infectious demyelination and clinical response to corticosteroids to prove the same.
Conclusion
Varicella zoster can be spread centrifugally to cause myelitis which manifests at the same spinal level as dermatomal affection. Whether myelitis is secondary to infection or para infectious is controversial. The detection of VZV DNA or IgG index in CSF can be used as a surrogate marker, and prompt initiation of immunomodulation can lead to clinical resolution.
Footnotes
Author Contribution
Conceptualization, design, writing—original draft preparation: MC, KVV; design, writing—reviewing and editing, supervision: RTP, RCP; writing— reviewing and editing: KVV
All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent has been obtained from the mother of the subject and the same has a corresponding author. We have uploaded a copy of the same on the website along with the submitted material.