
Abstract
This study aimed to determine the proportion of diphtheria patients who develop post-diphtheritic polyneuropathy (DP) later on and also to study the clinical features and outcomes of children with post-DP. This prospective observational study was conducted at the Department of Pediatrics, King George’s Medical University, Lucknow, Uttar Pradesh, India. Children under 14 hospitalized with clinically diagnosed diphtheria and post-DP were recruited (n = 81). Detailed clinical examination with appropriate investigations was conducted, including throat swabs for staining and culture for Corynebacterium diphtheria, nerve conduction studies, electrocardiography, and echocardiography. The data were analyzed using Statistical Package for Social Sciences (SPSS) version 16.0. Seventy-four cases of diphtheria and seven cases of post-DP were enrolled, 56.8% were male, and the most prevalent age group afflicted was two to five years. Fifty-three children (65.4%) were partially immunized for diphtheria. Neck swelling, voice change, difficulty breathing, noisy breathing, respiratory involvement, and stridor were significantly more common in the unimmunized group. Voice change, heart rate irregularity, and hypotension were substantially more common in patients who developed clinical neuropathy than those who did not. Early administration of antibiotics in children with diphtheria before hospital admission was found to be significant in those children who did not develop clinical polyneuropathy, 38.5% of diphtheria survivors had abnormal nerve conduction study at six weeks of illness. Neck swelling and change in voice were significantly more common in patients with abnormal nerve conduction velocity (NCV) than in normal nerve conduction studies, 87.5% of children who had taken antibiotics before hospital admission had no clinical neuropathy, and NCV was also normal. Clinical neuropathy developed in just 20% of diphtheria patients with impaired NCV. Any child diagnosed with diphtheria should be followed for three to six months in anticipation of neurological complications. DP carries a good prognosis; hence, timely diagnosis and differentiation from other neuropathies is a prerequisite for rational management.
Introduction
Diphtheria is a life-threatening, communicable disease caused by Corynebacterium diphtheriae (C. diphtheriae). C. diphtheriae is a Gram-positive bacillus, non-spore-forming, non-motile, and is transmitted via aerosol pathways. Toxigenic strains of C. diphtheriae release a toxin that leads to formation of a pseudo membrane in the pharynx—pharyngeal diphtheria. In addition, the toxin also results in systemic toxicity, myocarditis, and polyneuropathy. The clinical course of diphtheria depends on the severity of symptoms, extent of membrane and also the amount of toxin absorbed by Schwann cells. Toxin inhibits the synthesis of myelin and leads to various neurological symptoms. Neurological complications have been observed in 15%–27% of cases of diphtheria. Hadfield et al., 1 found that these complications occur more in cases with severe respiratory disease (75%) in comparison to mild respiratory diphtheria (20%).
Due to poor vaccination coverage, diphtheria is common in India. Among 20,000 cases of diphtheria reported by WHO during 2007–2011, 17,926 (89.6%) cases were from India alone. Most persons with diphtheria in India are either partially immunized or unimmunized. Diphtheritic polyneuropathy (DP) is recognized as one of the most severe complications of diphtheria.
Post-diphtheritic neuropathy is defined as signs and symptoms suggestive of various cranial nerve involvement and/or limb neuropathy within six weeks of compatible clinical illness suggestive of diphtheria. The incidence of DP is directly proportional to the severity of intoxication.
Diphtheriae toxin, secreted by toxigenic strains of C. diphtheriae, is a single polypeptide of M 58,342. Toxigenic strains of C. diphtheriae carry the tox structural gene found in lysogenic corynebacteriophages b tox1, g tox1, and q tox1. Strains which are highly toxic have two or three tox1 genes inserted into the genome. Gene expression is regulated by the bacterial host and is iron-dependent. Low concentrations of iron inhibit the gene regulator, resulting in increased toxin production. Toxin is excreted from the bacterial cell and undergoes cleavage to form two chains, A and B, which are held together by an interchain disulfide bond between cysteine residues at positions 186 and 201. With an increase in toxin concentrations, the toxic effects extend beyond the local area due to distribution of the toxin by the circulation. Diphtheriae toxin does not have a specific target organ, but myocardium and peripheral nerves are most affected.
Diphtheritic toxin invades Schwann cells and it inhibits the synthesis of myelin proteolipid and basic protein. Transport down the axon of newly synthesized protein with eventual destruction of the myelin sheath accounts for the delay in neuropathic symptoms (mean eight weeks) after initial infection. The period between the appearance of first symptom of diphtheria and the development of DP is termed latency, which varies from 10 days to three months. The first indication of neuropathy is paralysis of the soft palate and posterior pharyngeal wall. Bulbar dysfunction typically develops during the first two weeks. Oculomotor and ciliary paralyses seen after three weeks are common and distinctive features of DP. Peripheral neuritis develops later, from 10 days to three months after the onset of oropharyngeal disease. In some patients, there may be a secondary worsening of the bulbar symptoms along with the occurrence of peripheral neuropathy.
DP is a potentially reversible condition, and surviving patients often report few to no neurologic symptoms. DP is generally considered a demyelinating neuropathy with proximal to distal spread of weakness and prominent sensory features. In patients with DP, motor symptoms improve within two to four months. 2
Literature on post-DP in children with diphtheria is scarce. There are only a few studies in which cases of diphtheria were prospectively followed up to discover diphtheria’s neurological complications. None of the studies studied the association of DP with other clinical features. So, this prospective observational study was planned to determine the proportion of diphtheria patients who develop post-DP later on and also to study the clinical features and outcomes of children with post-DP. A nerve conduction velocity (NCV) test was also performed in all patients of diphtheria between four to six weeks of illness to determine whether NCV abnormalities are present in children who do not develop clinical neuropathy.
Materials and Methods
This prospective observational study was conducted at the Department of Pediatrics in collaboration with the Department of Neurology, King George’s Medical University (KGMU), Lucknow, Uttar Pradesh, India, from April 2019 to March 2020. After written informed consent, children under 14 who were hospitalized with clinically diagnosed diphtheria and post-DP were recruited (n = 81). They were followed up for three months for any neurological weakness or complications. Detailed clinical examination with appropriate investigations, including throat swabs for staining and culture for Corynebacterium diphtheria, nerve conduction studies, electrocardiography, and echocardiography, was conducted, and results were tabulated and analyzed. Ethical clearance was obtained from the institutional ethical committee vide letter 97th ECM II B-Thesis/P76.
Statistical Analysis
The data was entered in an MS EXCEL spreadsheet, and analysis was done using Statistical Package for Social Sciences (SPSS) version 16.0. Categorical variables were presented in number and percentage, and continuous variables were presented as mean ± SD and median. Quantitative variables were compared using a parametric Unpaired t-test in two groups. Qualitative variables were compared using the appropriate Chi-Square test/Fisher’s exact test. A p value of <.05 was considered statistically significant.
Results
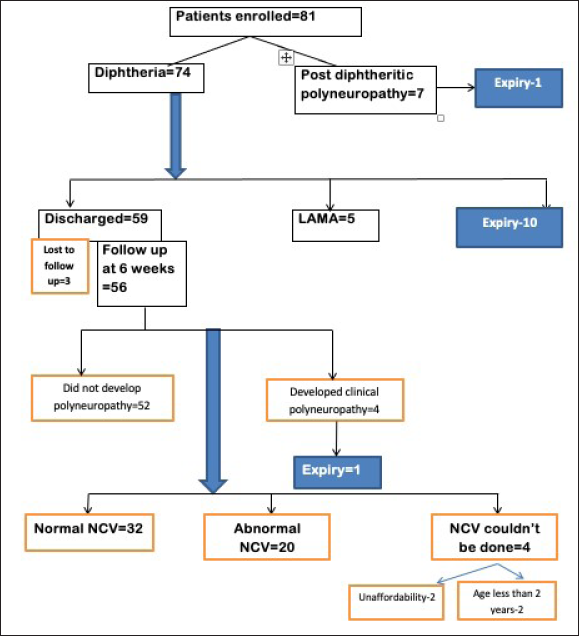
During the study period, 81 patients were enrolled, with males (56.8%) outnumbering females (43.2%) by a ratio of 1.3:1, the majority of patients (54.3%) being in the age group of two to five years and belonging to the upper lower class (53%). There were 74 diphtheria patients and seven people hospitalized with post DP. Out of 74 diphtheria patients, 56 could be followed up on up to six weeks after illness onset, three were lost to follow-up, and 10 died during hospitalization. NCV was performed in 52 cases after 6(±1) weeks of symptom onset. In the course of the study, four patients developed post-DP, one of whom died. NCV was performed in 52 cases. It was normal in 32 cases, and abnormal in 20 (Figure 1). Among the enrolled patients, 53 (65.4%) were partially immunized for diphtheria.
Study Flow Chart.
The majority of the patients in the current research had fever (90.5%) and difficulty swallowing (82.4%). Diphtheritic membrane was found mostly in pharynx (93.2%) and in tonsillar areas (90.5%). Eight patients died during treatment owing to myocarditis, and two died due to breathing difficulties since they arrived late and died before tracheostomy could be performed. The following were the mean durations of symptoms before hospitalization; fever 5.20 ± 3.27, neck swelling 2.03 ± 2.57, difficulties with swallowing 3.57 ± 3.60, and difficulty breathing 1.43 ± 2.03.
All 74 diphtheria patients who participated in the study received IV fluids, IV antibiotics, and antidiphtheritic serum. The mean time between the onset of symptoms and the antidiphtheritic serum was 6.66 ± 3.19 days, and the mean hospital stay was 11.19 ± 8.01 days. Before forthcoming to our side, 24 of the 74 diphtheria patients had received therapy in the form of IV and oral antibiotics, and three of them had received 10,000, 30,000 and 40,000 IU of antidiphtheritic serum, respectively. None of the patients had thrombocytopenia or abnormal liver function test.
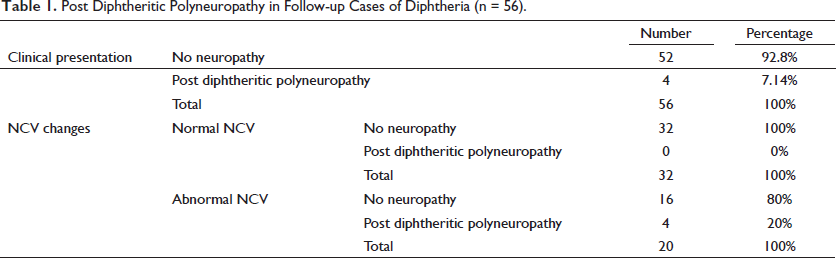
Fifty-six patients (75.6%) were followed up on for three months, and polyneuropathy was identified in 4 (7.14%). Patients with normal NCV findings did not develop polyneuropathy, whereas four patients (7.14%) with abnormal NCV findings did. However, polyneuropathy did not develop in 16 patients (80%) with abnormal NCV (Table 1).
Post Diphtheritic Polyneuropathy in Follow-up Cases of Diphtheria (n = 56).
Seven patients reported for the first time with post-DP and four were followed up on. Almost all patients with post-diabetic polyneuropathy had a change in voice, difficulty swallowing, and nasal regurgitation of feeds. Palatal palsy, 9th and 10th cranial nerve palsy were seen in all individuals with post DP. Polyneuropathy occurred in the study’s subjects who had received previous antibiotic therapy and ADS vials. When five patients were hospitalized for the first time, they were given ADS at a dosage of 100,000 IU. The latent time between the onset of diphtheria symptoms and neurological problems ranges from 7 to 42 days, with a mean length of 251.7 days. Nine patients were discharged from the hospital in the recovery phase, and no neurological deficit was discovered during the follow-up period. Polyneuropathy patients had an 18% mortality rate.
A comparison of the demographic profile and clinical presentation of diphtheritic individuals (n = 56) who developed clinical neuropathy (n = 4) versus those who did not develop clinical neuropathy (n = 52).
Four children who acquired clinical neuropathy were also unimmunized, and the result was shown to be statistically significant. Among all features, voice change was significantly more common in patients who developed clinical polyneuropathy. Children who received antibiotics and antidiphtheritic serum prior to hospital admission did not develop. There was no significant difference in the duration of days between children who had clinical neuropathy and those who did not develop clinical neuropathy.
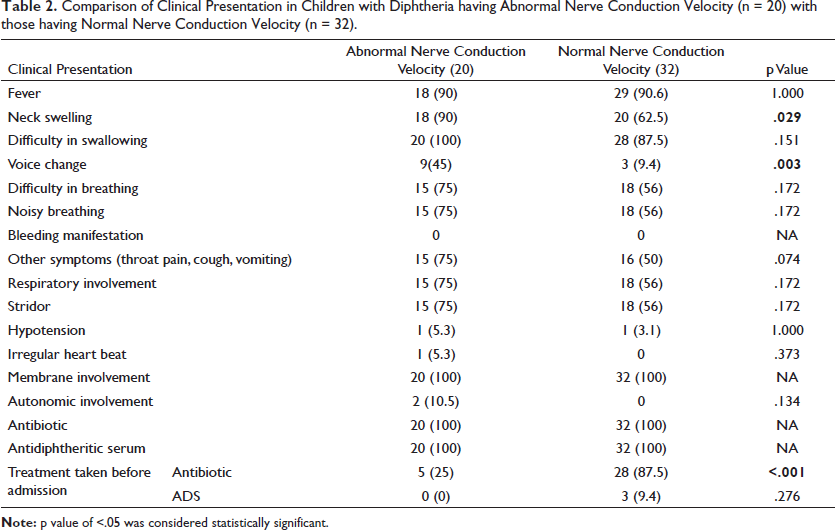
Table 2 shows that individuals with impaired NCV had considerably higher neck swelling and vocal changes. Children who had received antibiotics before admission did not have clinical neuropathy, and NCV was likewise normal. Children who had ADS before admission, on the other hand, showed no correlation.
Comparison of Clinical Presentation in Children with Diphtheria having Abnormal Nerve Conduction Velocity (n = 20) with those having Normal Nerve Conduction Velocity (n = 32).
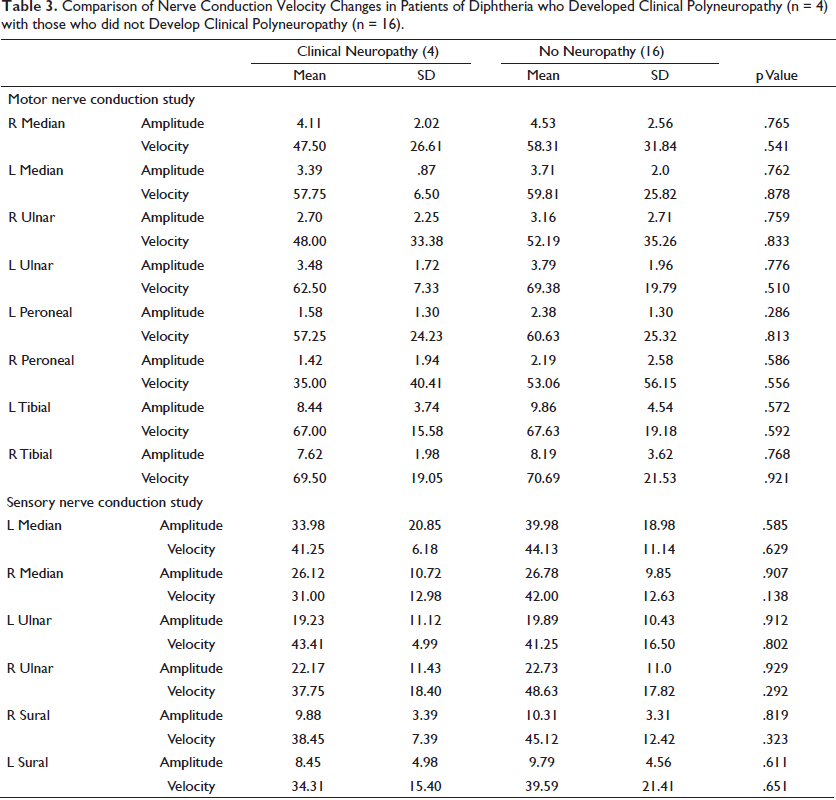
There was no significant difference in aberrant NCV alterations between children who had clinical neuropathy and those who did not develop clinical neuropathy (Table 3).
Comparison of Nerve Conduction Velocity Changes in Patients of Diphtheria who Developed Clinical Polyneuropathy (n = 4) with those who did not Develop Clinical Polyneuropathy (n = 16).
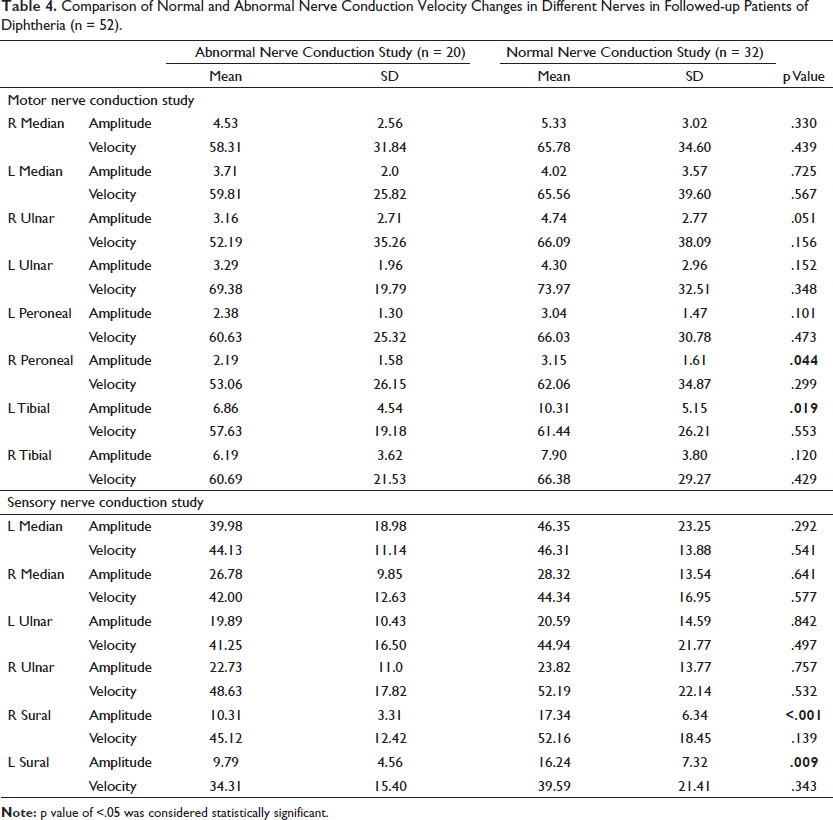
From the study of NCV, amplitude of motor part of right peroneal & left tibial nerve, amplitude of motor part of right & left sural nerve were found to be statistically significant (Table 4).
Comparison of Normal and Abnormal Nerve Conduction Velocity Changes in Different Nerves in Followed-up Patients of Diphtheria (n = 52).
Discussion
Post-diphtheritic neuropathy is defined as signs and symptoms of limb neuropathy, palatal weakness and/or cranial nerve involvement within six weeks of clinical illness suggestive of diphtheria. The incidence of DP is directly proportional to the severity of the disease. DP is reversible, and survival patients report minimal to no neurologic symptoms. Only a few studies have been done regarding the prevalence of post-DP in children with diphtheria. Our primary aim was to find the proportion of children with diphtheria developing post-DP during illness.
In the current prospective observational study, 81 patients were included. Their demographic information, socio-economic background, gender and age distribution, diphtheria immunization status, clinical symptoms, NCV study, and results were thoroughly examined. During the six-week follow-up, almost all patients were investigated by performing an NCV study. Most patients were monitored for any remaining neurological impairment for three months. The study’s clinical and demographic characteristics revealed that boys were more impacted than girls, and most patients were between two and five years old and immunized. Several other studies3,4 found that boys outnumbered girls. Socio-economic status is one of the most critical social determinants of health and illness. The modified Kuppuswamy scale 5 was used to categorize families of enrolled patients. In our study, most patients (97.4%) belonged to the lowest socio-economic class. Other studies have found that most affected children come from lower socio-economic backgrounds.6,7 Children of low socio-economic class are more vulnerable to infectious diseases such as diphtheria due to their rural upbringing, poor sanitation, lack of education, and lack of immunization awareness.
Clinical profile has been the focus of attention in our study which aims to determine the factors which led to post-DP. In our study, fever, and difficulty in swallowing were the two most common symptoms followed by neck swelling. Kole et al. investigated the epidemiological profile and clinical aspects of diphtheria patients, finding that fever was present in 56% of the cases. 6 In Meera and Rajarao’s 8 investigation in Hyderabad, all patients with clinical diphtheria came with fever, sore throat, and a pseudo membrane. At the time of admission, 33% of patients had neck swelling and 9% had stridor.
In our study, children with clinical polyneuropathy had a change in voice more frequently. Voice alteration as a symptom was similarly statistically significant in children with clinical polyneuropathy, with an odds ratio of 0.12 (p = .001). All patients with clinical polyneuropathy had a fever, neck swelling, difficulties with swallowing, difficulty breathing, and stridor, albeit the correlation was not statistically significant.
In comparison to earlier research (15%–27%), the proportion of children acquiring neuropathy in the current study was found to be low (7.4%). Pathogen, immunization status, and therapy may all be factors in this disparity. All diphtheria patients in our research got antidiphtheritic serum and antibiotics quickly after admission, which may have resulted in a less severe toxin impact on nerves. The majority of youngsters in our research were only partly immunized. Many studies have found that disease severity is lower in immunized children compared to non-immunized children. In research done by Nabaneeta et al (2019), two-thirds of the children were not immunized, 9 but in the current study, 65.4% were partially immunized and 8.6% were totally immunized.
All of the children with post-diabetic polyneuropathy (n = 11) had a change in voice, difficulty swallowing, nasal regurgitation of feeds, and palatal palsy. All patients had cranial nerve palsy (9th and 10th CN). Neck muscular weakness was evident in 72.7% of patients, followed by limb weakness, 36.3% of patients had respiratory muscle weakness. Deep tendon reflexes were reduced in 63.6% of patients, while tone was reduced in 54.5%; 18.2% of patients had autonomic involvement. The nerves included in research done by Piradov et al. (2001) were the 9th and 10th CN (32 patients), 7th CN (28 patients), 3rd, 4th and 6th CN (27 patients), and 11th CN (27 patients). 10 The remaining patients had quadriplegia and one-third had quadriparesis. Kanwal et al. (2012) discovered that 52% of patients with DP exhibited palatal palsy and 94% experienced limb paralysis. In 85.4% of patients, respiratory muscles were affected. 4
In our study, NCV was done in 52 patients of diphtheria after six weeks of presentation. Out of these, 32 patients had normal NCV studies and 20 showed abnormal NCV studies. In abnormal NCV patients, only four had features of clinical neuropathy. Neck swelling and change in voice were significantly more common in patients with abnormal NCV. Children who had taken antibiotics prior to admission had no clinical neuropathy and NCV was also normal. Change in voice and autonomic involvement was significantly more common in patients who developed clinical polyneuropathy. This indicates that NCV can be abnormal in diphtheritic patients even in absence of clinical neuropathy.
Work up
Laboratory Parameters
In research done by Dash et al. (2019), 22.3% of diphtheria patients had abnormal renal function tests, and 25.3% had thrombocytopenia. 9 In our investigation, however, regular test results in diphtheria patients were within the normal range.
Nerve Conduction Study
In our study, NCV was done in 52 patients of diphtheria. 20 of them had abnormal NCV study and 32 showed normal NCV. Out of 20 abnormal NCV studies, four patients also developed clinical polyneuropathy. We could not find any study in which NCV was done in diphtheritic children without polyneuropathy for comparison. Kanwal et al. (2012) 4 measured NCV in 12 children with post-DP, three of whom had decreased amplitude and five of whom had decreased conduction velocity.
Treatment
In our study, all patients were initially kept on iv fluids with a duration of 2.43 ± 1.52 days. All patients were treated with antibiotics and antidiphtheritic serum. Out of enrolled diphtheria cases, 49.5% of patients required oxygen support with a mean duration of 1.88 ± 2.74 days; 13.5% of patients required ventilatory support with a mean duration of 2.34 ± 4.34 days. Tracheostomy was done in 13.5% patients and mean duration was 2.39 ± 7.40 days. Patients having autonomic dysfunction in the form of irregular heart rates were treated with levocarnitine. Duration of hospital stay was 11.19 ± 8.01 days. Four patients had received ADS in a dose of 100,000 IU when admitted for the first time as a case of diphtheria while one of the patients with post-DP received 100,000 IU of ADS as membrane was present at the time of presentation. Exavier et al. (2018) conducted a study on 26 patients. All children received penicillin, metronidazole, and dexamethasone. Sixteen of the patients (61.5%) received DAT at doses ranging from 16,000 to 80,000 units with a mean dose of 56 000 units (SD 6,22,000). Among patients who survived, 10 of 13 (77%) received DAT, while 6 of 13 (45%) who did not survive received this treatment (p = .23).
Outcome
Outcome of patients has been described in terms of discharge, LAMA, mortality. Out of 74 enrolled patients of diphtheria, five patients went LAMA, 10 patients expired. Four patients developed clinical neuropathy. Neurological outcome was based on remaining 59 patients who were discharged and followed till three months. However, three patients were lost to follow-up as they could not be contacted telephonically or they did not visit OPD. Mean duration of hospital stay was 11.19 ± 8.01 days. Mortality was due to myocarditis and shock in 80% patients, 20% died due to respiratory compromise.
Among 11 patients of post-DP, nine patients (81.8%) were discharged from the hospital. Mortality in polyneuropathy patients was 18% due to hypotension and autonomic involvement. In our study, children with palatal palsy recovered within three to five weeks while children with limb weakness recovered within four to six weeks. Jayashree et al. (2006) 11 studied the predictors of outcome in patients with diphtheria in which out of 48 patients, 21 survived and 27 died (56.3%). Immediate cause of death was myocarditis (85%), airway compromise (11.1%). In Kole et al. (2010) study, 4 complications observed were myocarditis (68%), neuropathy (15%) and respiratory compromise (7%). Death occurred in 2.5% of patients. In a study conducted by Dash et al. (2019) 66% survived, 23% died and 11% opted for discontinuity of care owing to unfavorable prognoses. Complications seen were airway compromise (61.7%) followed by myocarditis (35.4%). 10 In Prasad et al. (2018) study palatal palsy was present in 18 children (64%). 12 Bulbar symptoms in the form of nasal twang, regurgitation, and dysphagia were observed in all children. Nine children had symmetric limb weakness. Ascending paralysis was seen in seven cases (25%), whereas descending in two cases (7%). Most of the patients had hyporeflexia or areflexia (88.9%) and hypotonia. Sensory symptoms like paresthesia, hypoesthesia, and hyperesthesia were present in all cases (100%). Duration of recovery was one to five weeks in case of bulbar palsy. In a study of post-DP conducted by Kanwal et al. (2012), 4 52% had palatal palsy and limb muscle weakness was present in 94%. Involvement of respiratory muscles was observed in 85.4% and 60.4% were mechanically ventilated. Post-diphtheritic myocarditis occurred in 41.7% of children; 25% had a cardiogenic shock and 10.4% showed rhythm disturbances. Median duration of hospital stay was 18 days and 20.8% of patients stayed for more than one month. Out of 48 patients, 85.4% of children were discharged and 14.6% died. In Manikyamba et al. (2015) study, 13 isolated palatal palsy was seen in seven children (53%) and six children (46.1%) developed quadriparesis. One child expired & recovery was complete in 12 children.
Conclusion
In light of the recent recurrence of diphtheria in some regions of India, pediatricians/neuro-physicians should have a high index of suspicion for DP. Any child diagnosed with probable diphtheria should be monitored for neurological complications for three to six months. As observed in our case series, DP has a favorable prognosis; thus, earlier identification and distinction from other neuropathies is essential for appropriate therapy and contact tracing.
The continued occurrence of diphtheria highlights the importance of public health measures such as: (a) strengthening routine immunization and mandatory booster vaccination at school entry and Td booster at 10-year intervals after that. (b) vaccinating susceptible contacts and providing prophylactic antibiotics to contacts. (c) Ensuring ADS availability for timely administration and therefore avoiding issues. (d) The AFP surveillance system may be used to detect DP and hence regions of diphtheria recurrence, as well as to boost immunization programs in such pockets.
Limitations of the Study
Most of the youngsters that came to us were referred from other facilities. Details of therapy received before admission were frequently unavailable. Due to technological concerns, NCV could not be performed on little infants. Visual indications of diphtheria could not be remarked on since they appear late, and the mean length of hospital stay in the current research was only 11.19 days. During the hospital stay, no child was found to have ocular paralysis. The study was done at a tertiary care center, which may have resulted in selection bias because patients admitted were unwell and had previously received therapy.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Ethical clearance was obtained from the institutional ethical committee vide letter 97th ECM II B-Thesis/P76.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Nil.