
Abstract
Introduction
Cardiovascular (CV) disease is the leading cause of mortality in hemodialysis (HD) patients, accounting for >50% of deaths in end stage renal disease (ESRD) patients. 1 Subclinical volume overload in HD patients is directly associated with hypertension, increased arterial stiffness, and left ventricular hypertrophy (LVH). Chronic kidney disease (CKD) patients, even in their early stages, can present with overt volume overload, which may be aggravated by endotoxins and can contribute to left ventricular dysfunction in these patients. 2 An additive contribution from HD treatment may strongly enhance the severity of endotoxemia in HD patients. Onofriescu et al. showed hydration status to be associated with increased mortality risk in a HD population, independently of cardiac morphology and function. 3 There are limited cross-sectional studies on echocardiographic parameters evaluating hydration status in patients undergoing dialysis. They also found left atrial dilatation (LAD) on echocardiography to be related to overhydration (OH) status based on bioimpedance measured fluid overload (FO) in 76 HD patients. 4 Voroneanu et al. 5 on the other hand, found that HD patients with better volume control had a lower left ventricular mass (LVM). There is dearth of prospective data in HD patients correlating volume status with cardiac outcome.
Furthermore, current methods of estimating dry weight and volume status in patients on HD are mainly based on clinical assessment. 6 , 7 Bioimpedance spectroscopy (BIS) has been established as an objective method for assessing fluid status with reproducible results. 8 BIS usage has been associated with a lesser incidence of volume overload and a decrease in episodes of intradialytic hypotension.9,10 Another useful method of volume assessment in HD patients is lung ultrasonography (LUS) looking for Lung Comet Signs (LCS). 11 A simple counting of B lines on LUS provides an estimate of lung water excess, thus correlating with patient outcomes on maintenance HD. 12 The inferior vena cava (IVC) collapsibility assessment had reasonable reliability in predicting tolerance to fluid removal in critical patients. However, the practical difficulty of implementing this method in a dialysis facility has precluded its use on a wider scale. 7 A study conducted at our center among 50 maintenance hemodialysis (MHD) patients to assess the effectiveness of clinical, sonographical, and BIS methods in volume estimation in MHD patients showed both IVC assessment and LUS to be reliable, simple, and effective alternatives to BIS. 13 A study conducted in South Africa amongst 160 HD, peritoneal dialysis, and non-dialysis patients found BIS to be a sensitive and useful tool for assessing volume status in only clinically euvolemic non-dialysis patients. 14
Thus, this study was conducted to correlate the fluid status of these patients with cardiac outcome over a period of 6 months and the diagnostic utility of LUS in volume estimation, considering BIS as the gold standard.
Materials and Methods
Present study was conducted in the HD unit of Nephrology department in a tertiary care hospital from July 2021 to October 2022 after obtaining Institute Ethics Committee approval. Clinically, euvolemic patients more than 18 years old and less than 70 years and taking thrice weekly MHD for at least 6 months were enrolled. Those with implants like metallic prosthesis, history of amputation of limb, acute myocardial infarction, or acute infection within last 1 month, patients with pacemakers and active lupus nephritis, patients with interstitial lung disease, patients with pre-existing valvulopathy, and congestive heart failure (NYHA 3 and 4) were excluded.
Sample Size
The study of Di Gioia et al. 4 observed a significant correlation between FO and left atrial volume (LAV) with an r-value of 0.29. Taking this value as a reference and an alpha error of 5%, the minimum required sample size with 95% power of the study and 5% level of significance, the sample was estimated as 91.
Study Methods
Consented patients were enrolled considering inclusion and exclusion criteria. After obtaining a history, a clinical examination was done prior to the dialysis session to evaluate for intradialytic symptoms as well as to assess the hydration status of the patients. Demographic profile, comorbidities, and history including duration of illness and cause of ESRD were recorded. Clinical examination was done to assess for the presence of engorged neck veins, presence of peripheral edema, blood pressure, and auscultation for chest crepitations. Dry weight estimation was done by trial and error with the volume of ultrafiltration kept as the interdialytic weight gain. The serial assessment of post-dialysis weight at which the patient didn’t have any signs and symptoms of volume overload and volume depletion was taken as the dry weight. All the laboratory investigations were done from the same laboratory using the same method with samples drawn pre-dialysis. Baseline chest X-ray was done. Subsequently, all patients were evaluated on the same day for FO by ultrasonogram (USG) (lung comet score and inferior vena cava collapsibility index [IVCCI]) and bioimpedance analysis both during pre- and post-dialysis, during the mid-week dialysis session. Left ventricular mass index (LVMI), left atrial volume index (LAVI), and left ventricular ejection fraction (LVEF) were assessed using echocardiography prior to dialysis and measurements were recorded.
Sonographic Assessment
Curvilinear 3–5 MHz probe of USG machine SonoSite was used for IVC assessment. The cross-section image of the IVC was visualized at the axis of the right atrial, hepatic vein, or IVC junction and then rotated in order to get a long-axis view of the IVC. The diameter of inspiration and expiration was measured at 2.5 cm distal to the IVC–right atrium junction. IVCC index was calculated using the formula (expiratory caval diameter − inspiratory caval diameter/expiratory caval diameter × 100%). The cut-off defining hydration status was derived from the work of Cheriex et al. Overhydration (OH) was defined by the IVCCI of less than 40%. 15
For LUS examination, same curvilinear 3−5 MHz probe of USG machine SonoSite was used, and the probe was used for scanning of anterior and lateral chest from second to fourth intercostal spaces in parasternal, mid-clavicular, anterior axillary, and mid-axillary sites. B-lines are defined as a hyperechoic, coherent US bundle with a narrow origin in the near field of the image, and recorded in each intercostal space. A total of 24 regions scanning protocol was used, and the findings were recorded in a preformed performa. The sum of B-lines produced a B-lines score. Hydration status is defined based on the literature written by Picano et al. 16 A total of 15 or more B-lines score is taken as a volume overload state.
Bioimpedance Assessment
Fresenius Body Composition Monitor BCM TM was used for the BIS technique. It measures at 50 frequencies over a range from 5 to 1000 kHz to determine the electrical resistances of the total body water and the extracellular water. The patient was allowed to rest for 10 min. The red and black electrodes were placed on the non-fistula arm and same side lower limbs. Height, weight, body mass index, blood pressure, and patient details, including anthropometric measurements, were entered. Any erroneous patients were removed, and the measurements were repeated. The values of total body water, OH in liters, extracellular water in liters, and intracellular water in liters were noted from the screen. In case of incomplete readings, the procedure was repeated. A total of two readings were taken and the average of the two readings was taken. Over hydration/extracellular water (OH/ECW) (expressed as a percentage) ≥15% will be defined as FO. 3
Echocardiographic Assessment
Cardiac evaluation using echocardiography was done prior to dialysis using echocardiography C15e probe of USG machine SonoSite. All echocardiographic data was measured according to the guidelines of the European and American Societies of Echocardiography. LVEF, LVMI, and LAVI were calculated in the parasternal long axis view using both M-mode and 2D echo imaging. LVMI was calculated using Devereux formula 0.8{1.04[([LVD + IVS + PW]3 − LVD3)]} + 0.6. The cut-off value of LVMI was more than 115 g/m2 for LVH in males and 95 g/m2 for females. LAVI is calculated accordingly: (D1 × D2 × D3) × (0.523). Left atrial dilation was considered with a LAVI ≥34 mL/m2. 4
Hemodialysis Procedure
After all the measurements by various techniques, patients were subjected to HD. All patients were dialyzed with 1.3 m2 surface area polysulphone dialyzers and dialysate temperature of 35.5°C–36.5°C. Dialysis session for 4 h was given. Constant ultrafiltration rate profiles were used. The dry weight assessed clinically by a single nephrologist was noted. Interdialytic weight gain was kept as the volume of ultrafiltration for each patient.
Follow-up
All the patients were followed up at 3 and 6 months with clinical history, laboratory examination, sonographical assessments, BIS, and echocardiography were repeated at the third and sixth months. Major CV events (ischemic heart disease including myocardial infarction, stroke, cardiac arrest, heart failure, and CV deaths) were assessed at 3 months and 6 months follow-up. Ischemic heart disease: broad spectrum of clinical manifestations from an acute coronary syndrome which includes unstable angina and acute myocardial infarction with and without ST-segment elevation accompanied with or without symptoms of angina.
17
Stroke: sudden disruption of blood supply to the brain resulting in neurological deficits in the form of hemiparesis, slurring of speech, and alteration of the sensorium, accompanied by radiological findings.
18
Cardiac arrest: the sudden cessation of cardiac activity so that the victim becomes unresponsive, with no normal breathing and no signs of circulation.
19
New onset heart failure: acutely worsened heart function without known underlying heart disease.
20
CV deaths: deaths that result from an acute myocardial infarction, sudden cardiac death, death due to heart failure, death due to stroke, death due to CV procedures, death due to CV hemorrhage, and death due to other CV causes.
21
Outcome: the occurrence of any of the major adverse CV outcomes and change in echocardiographic parameters in patients was correlated with volume overload determined by the methods described above.
Statistical Analysis
The data entry was done in the Microsoft EXCEL spreadsheet and the final analysis was done with the use of Statistical Package for Social Sciences (SPSS) software, IBM manufacturer, Chicago, USA, Version 25.0. The normality of the data was tested by Kolmogorov–Smirnov test. In our study, we found the normal distribution of data, and parametric tests were used. All the demographic data, presented in the form of categorical variables were done in the form of numbers and percentages. On the other hand, the quantitative data were presented as the means ± standard deviation. The association of the variables which were qualitative in nature was analyzed using the chi-square test. A parametric test was done using a paired t-test. A repeated measure analysis of variance (ANOVA) with Bonferroni analysis was used to measure differences of continuous variables across the time period of follow-up. FO by bioimpedance was taken as the gold standard and repeated measures ANOVA was used to analyze the association between FO and demographic variables, sonographic variables, and echocardiographic parameters at baseline, 3 months, and 6 months’ follow-up. All the above variables were expressed as means ± SD. The association of LVH, LAD, low EF, and the presence of adverse CV events was assessed using the Cochran’s Q test with the presence of FO by IVC, LUS, and BIS at baseline, 3 months, and 6 months’ follow-up. All the above variables were expressed as percentages. Sensitivity, specificity, positive predictive value, and negative predictive value were calculated for the ultrasound B-line using logistic regression analysis to predict OH after taking bioimpedance-measured OH/ECW as the gold standard. A correlation diagram was done to see the association of LVMI and LAVI as outcome variables, and OH/ECW and LUS score as predictor variables. For statistical significance, a p-value of less than .05 was considered statistically significant.
Results
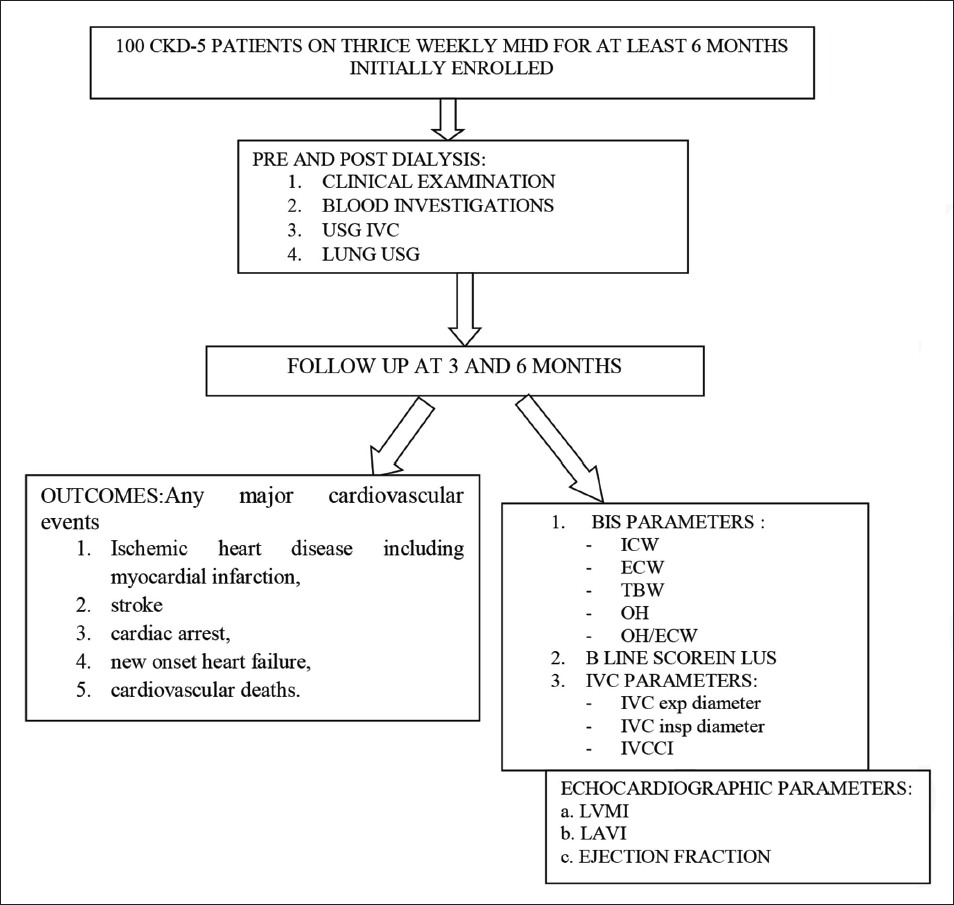
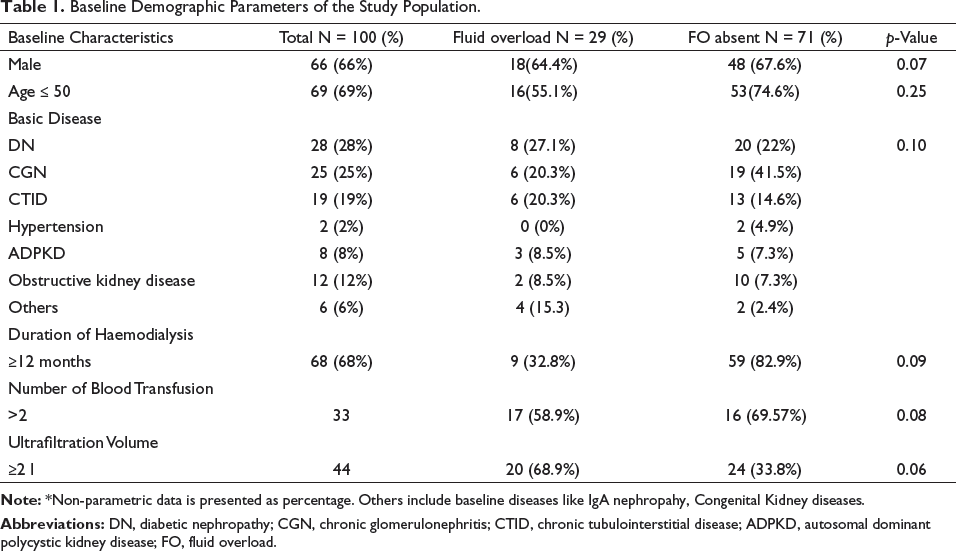
A total of 100 MHD patients were enrolled over 6 months as shown in the flow chart (Figure 1). The mean age of the study participants was 43.7 ± 12.1 years, and 66% of the study participants were men. The most common primary disease was chronic glomerulonephritis (28%), followed by diabetes mellitus (25%). At baseline, none of the demographic parameters were significantly associated with FO determined by BIS (Table 1).
Baseline Demographic Parameters of the Study Population.
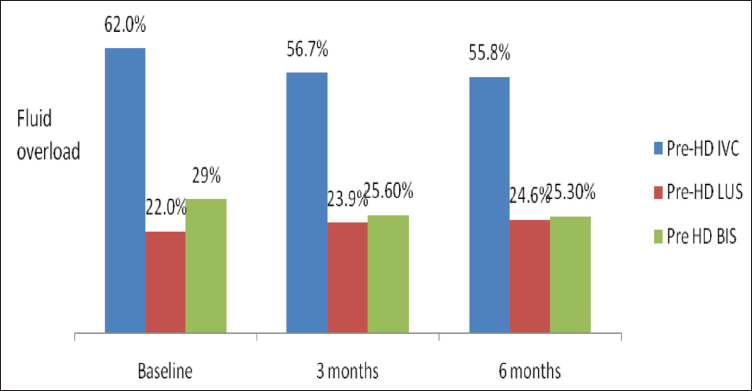
When assessed clinically in FO state, the number of patients developing lower limb edema was significantly less at 6 months’ follow-up as compared to 3 months (p-value .01). Jugular venous pressure, hypertension, and crepitations on chest auscultation were not associated with FO determined by BIS. None of the laboratory parameters were associated with FO. For both LUS and BIS, the incidence of FO for LUS among the patients decreased statistically significantly from baseline observations (p-value .02 and p-value < .001, respectively), 3 months (p-value .01 and p-value < .001, respectively) and 6 months follow-up (p-value .004 and p-value < .001, respectively) (Figure 2).
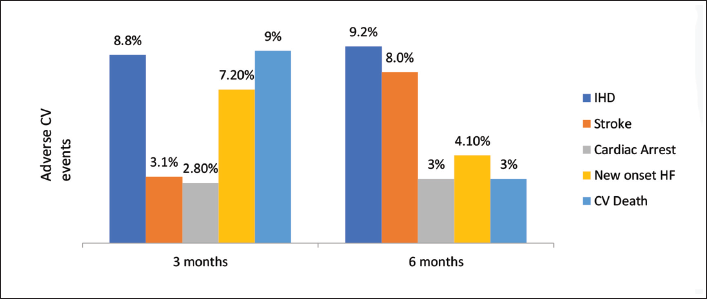
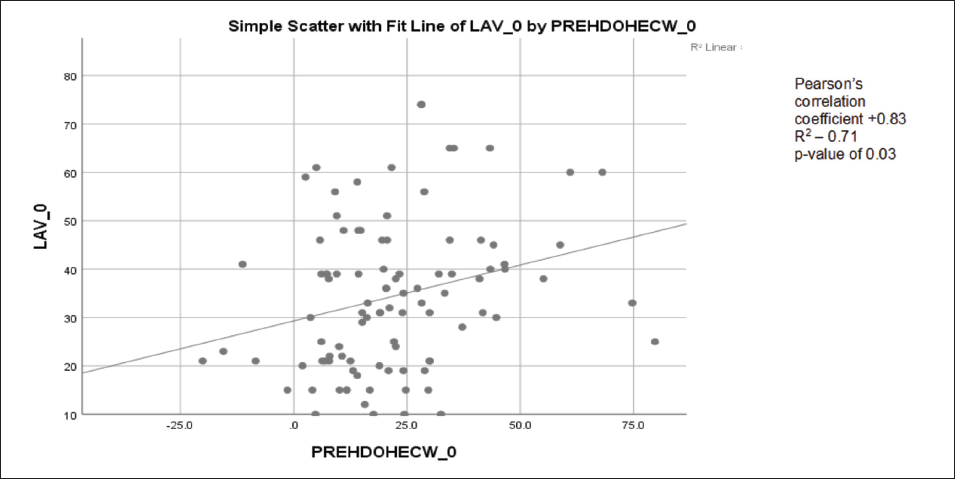
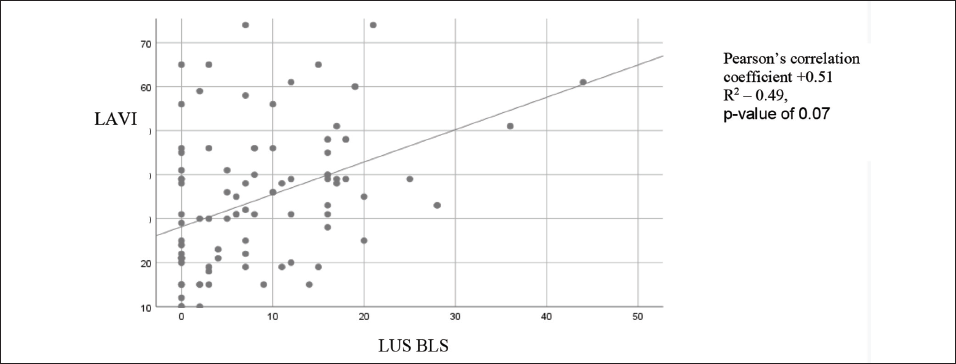
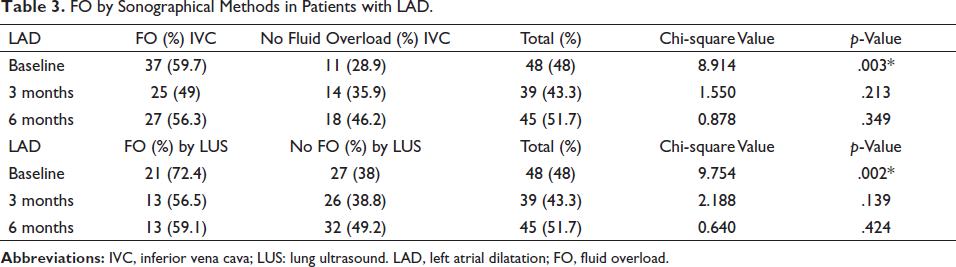
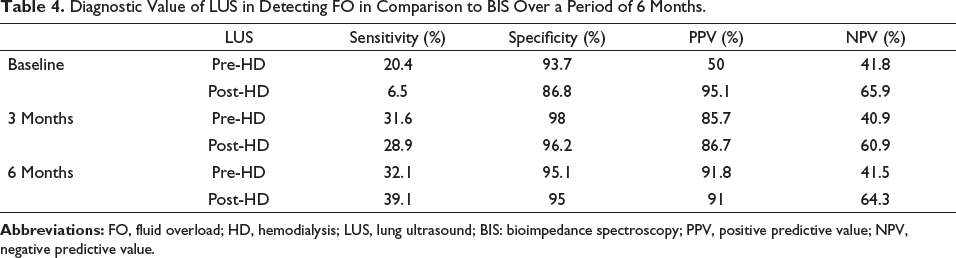
The distribution of major adverse CV events at 3 and 6 months’ follow-up is depicted in Figure 3. Both LAVI and LVMI at 6 months’ follow-up were significantly higher than that at baseline (p-value .001 and p-value .026, respectively) and at 3 months’ follow-up (p-value .048 and p-value .039, respectively) (Table 2). A significantly higher incidence of FO by IVC assessment was found among those with LAD at baseline (p-value −.003). However, these differences were not significant at 3 and 6 months. Similarly, significantly higher incidence of FO by LUS was present among those with LAD at baseline (p-value −.002). There was also a significantly higher incidence of FO by BIS HD among those with LAD at 6 months (p-value .007) (Table 3). FO by all three methods were not associated with LVH, EF, and adverse CV outcomes. There was a significantly higher incidence of FO by BIS among those with LVH, at baseline (p-value .001). FO determined by BIS didn’t find any significant association with EF and adverse CV outcomes. LUS was found to be highly specific in diagnosing FO in comparison to BIS with 3 months and 6 months specificity of 98% and 95.1%, respectively. Comparatively, it was found to be less sensitive in detecting FO as compared to BIS (Table 4). LAVI showed a positive linear correlation with OH/ECW at baseline (p-value .04, correlation coefficient: 0.83, and R2 of 0.71) (Figure 4a). For LUS, LAVI showed a weak correlation at baseline with B-line score at baseline (p-value .08, correlation coefficient: 0.51, and R2 of 0.49) (Figure 4b).
Association of Echocardiography Parameters with FO.
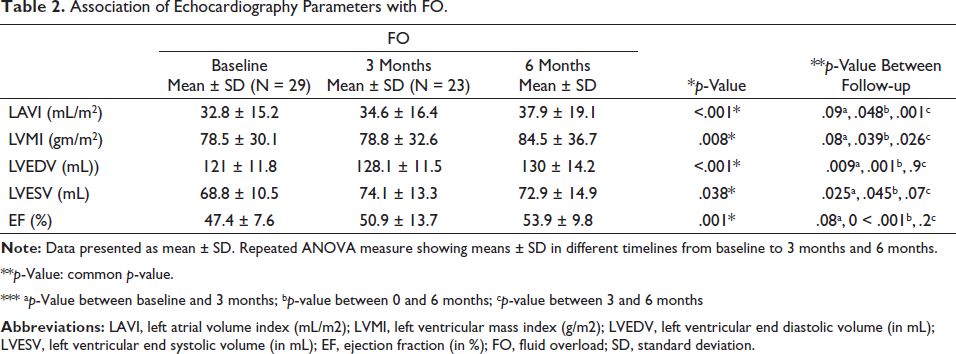
**p-Value: common p-value.
*** ap-Value between baseline and 3 months; bp-value between 0 and 6 months; cp-value between 3 and 6 months
FO by Sonographical Methods in Patients with LAD.
Diagnostic Value of LUS in Detecting FO in Comparison to BIS Over a Period of 6 Months.
Discussion
To the best of our knowledge, this is the first study done in Asian patients correlating fluid status with cardiac outcomes in HD patients in MHD patients on a prospective basis.
FO by IVC was significantly associated with left atrial enlargement on echocardiography at baseline. Contrary to our findings, Wu et al. 22 found that patients with low IVCCI not only had a significantly greater left atrium diameter but also a higher left ventricular end-diastolic diameter, left ventricular end-systolic diameter, and LVMI than those with higher IVCCI. However, IVC ultrasound may be limited by factors that affect IVC diameter or collapsibility, such as respiration, right heart function, and intra-abdominal or intrathoracic pressure changes. Muller et al. 23 found that high variations in IVC diameter are associated with fluid responsiveness, but low variations do not exclude fluid responsiveness emphasizing that the results should be interpreted carefully. There was a significantly higher incidence of FO by LUS among those with LAD, at baseline in our study. Zoccali et al. 24 found HD patients with congestion on LUS had a 4.2-fold higher risk of death and a 3.2-fold higher risk of cardiac events even after adjusting for other risk factors. They concluded that the degree of lung congestion was a better predictor for mortality, CV events, and hospitalization than the assessment done by the NYHA score. However, echocardiography was not done in the above study. In a recent randomized control trial, among 71 clinically euvolemic HD patients, it was found that patients who had a LUS-guided fluid removal had a significant lower LAVI, but didn’t have any association with LVMI, a finding similar to our study. 25 Contrary to our study, Donadio et al. 26 also didn’t find any significant association between B-line score and left atrial dilation on echocardiography. There was a significantly higher incidence of FO by BIS among those with LVH (determined by LVMI) at baseline and with LAD (determined by LAVI), at 6 months. Hur et al. 27 in a randomized control trial also found both OH determined by BIS to be significantly associated with LVH and LAD at baseline. In the absence of an association with any CV events, including mortality, FO determined by BIS was associated with both LAD and LVH, both of which are well-established markers of future CV events. None of the methods for fluid estimation correlated with any of the major adverse CV outcomes, which might be due to the fact that echocardiographic parameters are early indicators of CV morbidity and mortality.
Out of the clinical parameters, only pedal edema was associated with FO determined by BIS both at baseline and at 6 months follow-up. In a cross-sectional study among asymptomatic HD patients, it was found that pedal edema correlated with CV risk factors such as age and BMI but did not reflect volume status in HD patients. 28 LUS in diagnosing FO with respect to BIS had a specificity of 98% and 95.1% at 3 months and 6 months, respectively. The high specificity of LUS means that it can be an effective tool to exclude FO. However, the low sensitivity means its use as a reliable tool in detecting FO is low. A study conducted at our center among 50 MHD patients to assess the effectiveness of clinical, sonographical, and BIS methods in volume estimation in MHD patients showed both IVC assessment and LUS to be a reliable, simple, and effective alternative to BIS. 15
Hardly any studies are there comparing sonographical and BIS methods in correlating with cardiac outcomes on a prospective basis. Most of the previous studies were cross-sectional and retrospective in nature. In our study, the echocardiographic assessment was done at each follow up so that a simultaneous trend of volume status and cardiac structure in HD patients could be assessed. There were limitations in our study. The cohort was small as it was a single hospital-based study. Non-CKD patients were not included as controls. Also, BIS was not done in healthy persons, and validation of BIS as a volume estimation tool was not available in the local population. Although sonographic and echocardiographic assessment was done by nephrologists under the guidance of cardiologists and radiologists, there might be interpersonal variation with respect to standardization.
Conclusion
In MHD patients, LAD was a better predictor for the development of CV events than the more established LVH; hence, routine echocardiographic screening should be implemented rather than on an indication basis. Subsequently, appropriate diagnostic, as well as therapeutic interventions, might be undertaken to decrease CV events and reduce mortality in HD patients. Furthermore, routine LUS can be considered a reliable tool to exclude FO in these patients. Though this study showed an association between FO and echocardiographic parameters and larger follow-up studies are further needed to establish this association.
Footnotes
Acknowledgment
We would like to thank the patients for their cooperation in conducting this study and our institution for providing the necessary infrastructure for the study
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Committee Approval
All procedures performed and planned in studies involving human participation were in accordance with the standards of the institutional and /or national research committee at which the studies were conducted. (Approved by IEC of PGMER, Dr RML Hospital vide letter no:-2/2010/PGIMER/RMLH dated 30.7.2013) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Informed consent was obtained from all individual participant.