
Abstract
This article explores a variety of chemosensory strategies – pungent foods, ammonia salts, and essential oils – as potentially useful interventions for clinical states of dissociative shutdown (including functional/dissociative seizures); re-experiencing symptoms of posttraumatic stress disorder; and other states involving changes in arousal and a loss of balance in the neural pathways or networks crucial for the processing and integration of somatic, or body-based, sensations, as a result of stress-system dysregulation or trauma-related experiences. All of these states are common in clinical practice. Patients find them distressing as they interfere with normal daily function, quality of life, and capacity to manage the daily challenges of life. Based on the current literature we, the authors, provide an update pertaining to the current knowledge base about the neurobiology that underlies the therapeutic effects and clinical utility of these chemosensory substances. Whilst the use of chemosensory substances goes back into antiquity, our understanding of underlying neurobiological mechanisms is just beginning to emerge.
Keywords
In January 2026, following the publication of ‘Pickle Juice – and Other Pungent Foods – as a Grounding Strategy for Managing Episodes of Dissociative Shutdown’ (O’Sullivan et al., 2026), we the authors received a multitude of interesting emails. The comments and questions from our readers stimulated and challenged our thinking, and led us into new avenues of research. In addition, during the time that we were working on this material, Stanley Lyndon published an expanded and updated version of the predictive-coding model of FND (Edwards et al., 2012; Lyndon, 2026). Against this background we extend our previous discussion and, in responding to some of the comments and questions posed by our readers, hope to sharpen our understanding of pungent foods and their clinical uses.
To recap briefly, our article was about the use of pickle juice and pungent foods as a grounding strategy to disrupt dissociative shutdown states by helping patients maintain their connections with the body, self, close others, and the environment (O’Sullivan et al., 2026). In the article we also presented a hypothesis and neurobiological model – the homeostatic sensory-reset hypothesis – as to the mechanism by which pungent foods work. Pungent foods activate special sensory receptors in the mouth, oesophagus, and stomach – called transient receptor potential (TRP) channels. Signals from TRP channels enter the central nervous system via peripheral nerves and go up the neuraxis within the body’s somatosensory ascending pathways (interoceptive part) (see Figure 1 in O’Sullivan et al., 2026). As they go up, the signals are processed in a hierarchical manner in integrating centres located first in the dorsal horn of the spinal cord, then in the lower brainstem, midbrain, and hypothalamus, and finally in the insular cortex and limbic system. These integrating centres control behavioural and autonomic responses and ensure homeostasis is maintained. Thus, at each level of integration, the sensory information from TRP channel activation can modulate neural function at that level of the hierarchy, with the consequence that a coordinated response is put together in a top-down manner. In brief, TRP channels can feed into multiple neural circuits within the central nervous system, thereby resetting the central circuitry that maintains homeostasis. On this hypothesis, the somatosensory input from pungent foods feeds into the brain’s interoceptive/homeostatic system, activates it, and resets the system and associated neural networks in a way that supports, once again, the individual’s subjective sense of connection to the body, the emotional self, and to the environment.
The comments, thoughts and questions from the readers of our article, cover a broad range of issues and we discuss them one by one. The term chemosensation – which we have used in the abstract – refers to neural processes that enable us to detect chemical stimuli. It includes odours (smell), pheromones, tastants (taste), and irritants/pungent chemicals (somatosensory). Irritant and pungent chemical detectors include TRP channels located on free nerve ending in the skin, in moist surfaces of the eyes, nose, mouth, throat, gastrointestinal system, and in other parts of the body (Lundström et al., 2011). Some but not all of these processes are discussed in the current article. Appendix A defines key terms used throughout the article.
Comments by readers on application of pungent foods and other tastes and odours in their own clinical work
In response to our article, Bruce Bean, whose work we had built upon (Murray, 2016; The People’s Pharmacy, 2017), wrote, ‘By the way, one way of increasing the “jolt” from TRP channel activation would be to add a bit of concentrated ginger juice (which you can buy on Amazon) to pickle juice. I think you could probably come up with a mixture that was powerful but still palatable’ (Email communication, 13 January 2026). Along the same lines Lee Crothers, a Melbourne occupational therapist and psychotherapist, reported ‘I have a client who chose to use ginger shots and wasabi to “come back to themselves.” It helped reduce self-harm as this was often used to bring them back to their body’ (LinkedIn communication, 18 January 2026).
Many clinician readers, including occupational therapists (OTs), physiotherapists, and neuropsychiatrists, wrote us to say that they were already using a range of pungent foods – chilli, apple cider vinegar, mint, ginger, têtes brûlées candies (France), pepper, umeboshi plums (Japan), and lemon in water – as part of their clinical practice.
Lucia Tesolin, a neurologist working in Peru, wrote that in that cultural context ‘we have many culturally congruent, accessible and well-accepted TRP-activating options. Foods such as ají, lime and rocoto, kión (ginger) (core ingredients of Peruvian cuisine), and even Inca Kola carbonated drink, the national counterpart to Coca-Cola, are easily available in any local street market. I already use some of these pungent stimuli routinely with patients experiencing dissociative symptoms, precisely because they are familiar, inexpensive, and immediately accessible in daily life’ (Email communication, 20 January 2026). Subsequently, Lucia also mentioned that ‘one particularly relevant and culturally embedded option [is] muña leaves [Andean mint], which are widely used by the local population as infusions accompanying meals, often replacing plain water. They provide a strong, familiar aromatic stimulus that is very well accepted by patients and recognized as an arousing stimulus’. Lucia also shared that she was coordinating a project that included group cognitive-behavioural therapy/aromatherapy sessions for patients with functional/dissociative seizures. ‘During these sessions, patients [are] exposed to different odors and tastes . . . in order to explore the individual bodily responses to these sensory inputs while patients were in a state free of symptoms, and to help them learn how to intentionally use such stimuli when dissociative symptoms arise’ (Email communication, 20 January 2026). Lucia’s comment raises a question as to the neurobiology of aromatherapy: is the mechanism by which pleasant odours engage neural mechanisms the same or different to the mechanism engaged by pungent foods. We answer this question in the latter part of this article.
Two experienced occupational therapists working with functional neurological disorder (FND) described their own use of pungent tastes – such as mint-flavoured mouthwash and lemon juice – during the warning-symptoms phase of functional/dissociative seizures. One of them, Mary Mathews (Brisbane) also reported that in her group intervention for functional/dissociative seizures, a number of patients were now utilising pickle juice at the earliest sign of an imminent functional/dissociative seizure, with positive response (LinkedIn communications, 28 January and 25 February 2026).
Kate Gill, president and founder of FND Australia Support Services, noted that the homeostatic sensory-reset hypothesis aligns with the commonly used FND metaphor distinguishing between hardware and software dysfunction, framing the intervention as analogous to restarting a computer program rather than repairing structural pathology (Teaching session, 2 February 2026).
The neurologist Jeff Waugh of the University of Texas Southwestern told us about the use of a TRP-activating food for functional neurological symptoms not included under the rubric of functional/dissociative seizures. He reported that one of his patients, a child with functional movements, used peppermint candies because the sharpness of the favour helped her break out of episodes (Email communication, 13 January 2026). Menthol is the primary active component of peppermint and activates a certain class of TRP channels (the TPRM8, the cold and menthol receptor).
Stella Li, a clinical psychologist at the Children's Hospital at Westmead (Australia), wrote, ‘Basically, intense sensations including touch, taste, and smells have been used as distress tolerance skills in DBT [dialectical behaviour therapy]. These can be using calming and comforting smells to self soothe or intense tastes or smells like lemons or I guess pickle juice! Marsha Linehan suggests they work by shifting attention away from internal distress/turmoil to external sensory input aka grounding. I have found them very effective clinically, especially with dysregulated teenagers’. In the DBT theoretical framework, intense sensory input is conceptualised as helping to shift attentional focus or reduce arousal during acute distress (Linehan, 2015). Our homeostatic sensory-reset hypothesis adds a new perspective. It proposes that a homeostatic sensory-reset mechanism is also at play. Notwithstanding, Stella Li’s comment – as well as comments from other readers – raises an important question: do pungent foods shift focus-of-attention, and is this shift of attention part of the proposed homeostatic sensory-reset mechanism? We address this question in the latter part of this article.
And finally, two of the authors – CF and JO – have been working with patients to examine whether pungent foods might be useful in the management of hallucinations, panic symptoms, and ‘autistic meltdowns’. Akin to functional/dissociative seizures, these presentations are all characterised by a state of high arousal associated with a subjective sense of sensory or emotional overwhelm. CF and JO have developed a Homeostatic Sensory-Reset Worksheet for clinicians (Fitzgibbon and O’Sullivan, 2026).
Use of pickle juice and other pungent foods with posttraumatic stress disorder
We received the question ‘have you used the pickle juice and other pungent foods for posttraumatic stress disorder (PTSD)?’ and presume that the question concerns the use of pungent foods in relation to the re-experiencing subtype of PTSD. The answer to this question is yes. In our original article, in order to keep the text focused, we had focused on the use of TRP channel activators in shutdown states, including the dissociative PTSD subtype (see Vignettes 1 and 2 in the original article) (O’Sullivan et al., 2026). In the clinical setting, however, we use TRP channel activators in PTSD to both help individuals disrupt dissociative shutdown states (dissociative subtype of PTSD) and also to help individuals disrupt flashbacks (re-experiencing subtype of PTSD). A longer version of our answer is found below.
Individuals who are diagnosed with PTSD fall into one of three groups: those who re-experience the trauma (re-experiencing subtype of PTSD), those who retreat into a ‘shutdown’ state (dissociative subtype of PTSD), and those who experience both symptom patterns (Lanius et al., 2002; Lanius et al., 2003; Nicholson et al., 2017). – The re-experiencing subtype involves under-modulation of the periaqueductal grey (PAG) and amygdala alarm centres, along with under-modulation of arousal and somatosensory information, with the consequence that the individual is flooded with negatively valanced sensory stimuli (see Figure 1) (Kearney and Lanius, 2022). Under- and overmodulation of emotion and arousal in trauma-related conditions. The left-hand image shows the re-experiencing subtype of PTSD (identified as PTSD), in which the limbic (e.g., amygdala) and midbrain regions (e.g., PAG) are undermodulated by the prefrontal cortex. The patient experiences an increase in information: high levels of arousal and bodily sensations; strong feelings of anger, fear, or terror; trauma-related memories (e.g., dissociative flashbacks); and a strong motivation to act (e.g., motivation for flight or fight). The right-hand image shows the dissociative subtype of PTSD (identified as PTSD + DS), in which the limbic regions (e.g., amygdala) and midbrain regions (e.g., PAG) are overmodulated by the prefrontal cortex. The patient experiences a decrease in information: low level of arousal; an absence of bodily sensations; a subjective sense of being disconnected from the self; an absence of memories; and a lack of motivation to act (or even tonic immobility, a subjective sense of being unable to move when active defense responses [e.g., flight or fight] are physiologically switched off (Kozlowska et al., 2015)). Abbreviations: am, amygdala; mPFC, medial prefrontal cortex; PAG, periaqueductal grey. © Breanne E. Kearney and Ruth A. Lanius 2022. From Kearney BE, Lanius RA. The brain-body disconnect: A somatic sensory basis for trauma-related disorders. Front Neurosci 2022; 16: 1015749. Figure 1 was created with BioRender (www.biorender.com). – The dissociative subtype involves over-modulation of the PAG and amygdala alarm centres, along with over-modulation of arousal and somatosensory information, with the consequence that somatosensory information is blocked top-down and cannot ascend from the body to the brain (see Figure 1) (Kearney and Lanius, 2022). In this scenario the individual feels emotionally numb, spacey, and disconnected from the self and the here-and-now.
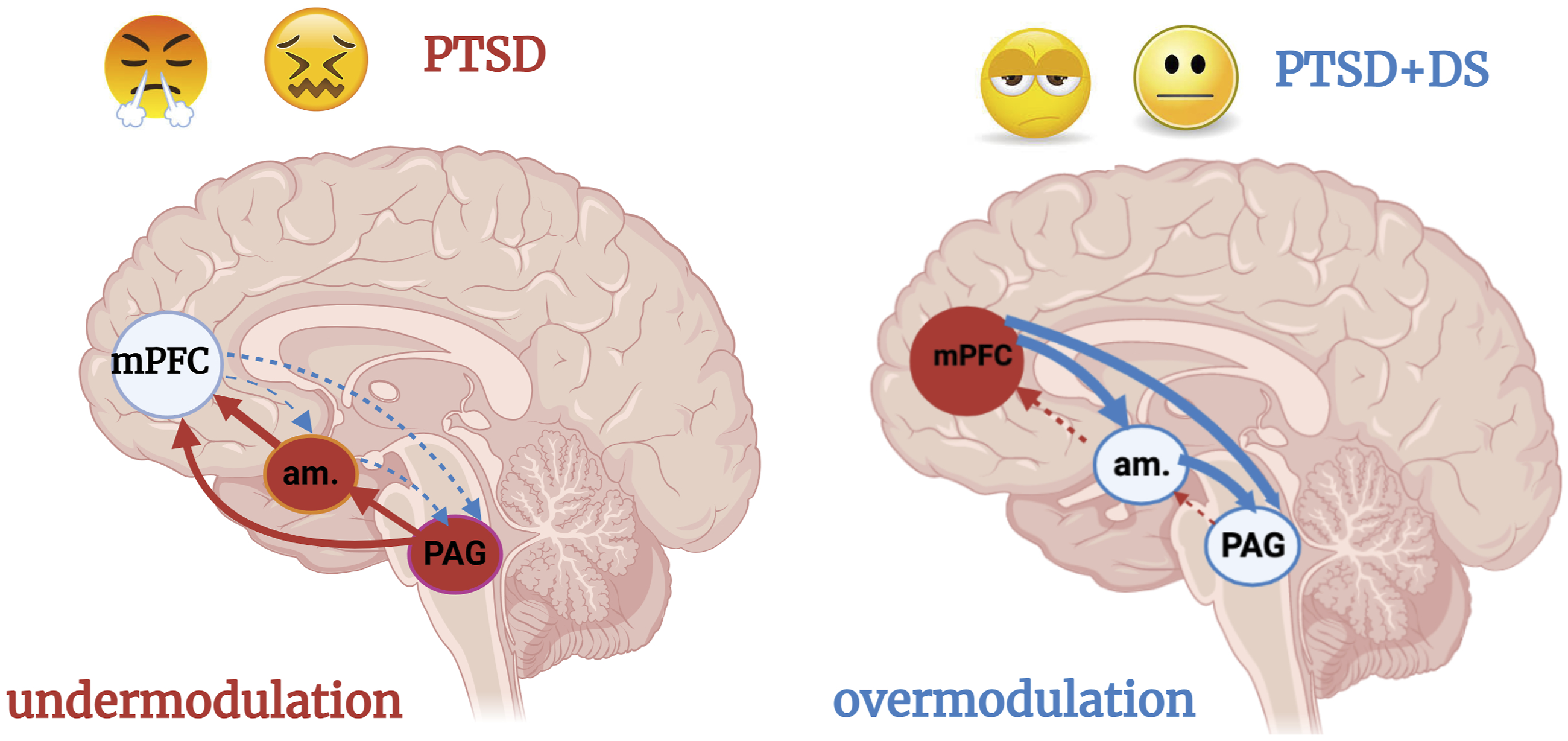
Viewed via the lens of somatosensory processing – as proposed by Breanne Kearney and Ruth Lanius – PTSD can be conceptualised as a loss of balance or an ‘off balance’ in the neural pathways crucial for the processing and integration of somatic, or body-based, sensations as a result of trauma experiences (p. 2) (Kearney and Lanius, 2022).
In the dissociative PTSD scenario, the homeostatic-reset hypothesis patients can use TRP channel activators to give the interoceptive/homeostatic/system a ‘jolt’, as it were, overriding the top-down over-modulation and resetting the system, thereby allowing somatosensory information to ascend from the body to the brain. Because TRP channels are also activated by sensory stimuli such as pain, temperature, acid, inflammation, and other noxious stimuli – all of which may signal ‘danger’ in the form of potential threats to homeostasis – the information from this system may have survival value and may be given ‘priority’, enabling it to override the shutdown state. Activation at the level of the insula also allows for the formation of a mental image – the subjective awareness of the noxious stimulus – thereby facilitating a shift in focus-of-attention to the present moment (see subsequent section).
In the re-experiencing PTSD scenario, patients can also use TRP channel activators to help them break out of the ‘flashback’ state. On the homeostatic sensory-reset hypothesis, ingestion of TRP channel activators when a patient is beginning to experience a flashback gives the homeostatic/interoceptive system a ‘jolt’, interrupting current processing and forcing the system to process information about the jolting stimulus. In this way, the somatosensory input from pungent foods feeds into the brain’s interoceptive/homeostatic system, activates it, and allows the system to reset itself – and associated neural networks – in a way that supports, once again, the individual’s subjective sense of connection to the environment and the here and now. As noted above, activation at the level of the insula also allows for the formation of a mental image – the subjective awareness of the jolting stimulus – allowing focus-of-attention to shift to the present moment, (see subsequent section). Interestingly, the current version of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5-TR) refers to the flashbacks that occur as part of the re-experiencing subtype of PTSD as ‘dissociative reactions’ because they involve a loss of connection to the present moment in response to reminders of the trauma, leading the individual to feel or act as if the traumatic event(s) were recurring (American Psychiatric Association, 2022).
We offer readers the following clinical example for a patient with re-experiencing PTSD. A 70-year-old woman with a diagnosis of PTSD presented with frequent flashbacks and re-experiencing of past trauma. Following a recommendation to trial pickle juice during these episodes, the woman began keeping pickle juice in the refrigerator and consuming it in small amounts when experiencing flashbacks. She reported that this intervention has successfully halted her flashbacks each time it was used. In cases of more intense flashbacks or re-experiencing, she found that consuming up to three small glasses of pickle juice was necessary to effectively alleviate symptoms.
In sum, because PTSD involves a loss of balance in the somatosensory pathways (Kearney and Lanius, 2022), activation of these pathways via TRP channel activators – coupled with a reset of the interoceptive/homeostatic system – allows patients to utilise pungent foods to disrupt both forms of dissociation: those involving decreased top-down modulation (flashbacks and reenactment) and those involving increased top-down modulation (‘shutdown’ symptoms such as emotional numbness, spaciness, and derealization/depersonalization).
Use of smelling salts for homeostatic sensory reset
Neurologist Jon Stone of the University of Edinburgh asked if ‘there is a strong connection in all this [TRP channel activators, the somatosensory sensory system, and our hypothesis about a homeostatic reset in that system] to smelling salts for swooning – which when prolonged has always been functional’ (Email communication, 13 January 2026). He suggested that it would be very helpful if we the authors were able to ‘sort out neurobiology of smelling salts!’ (Email communication, 14 January 2026).
In response to Jon’s challenge, we undertook an interesting journey of discovery. The short answer to Jon’s question is yes. Yes, because ammonia does activate TRP channels that sit in the nose and are part of the trigeminal chemosensory system. These TRP channels are typically located on the nerve endings of trigeminal polymodal nociceptor neurons whose cell bodies sit in the trigeminal ganglion. The information is carried via the trigeminal nerve (fifth cranial nerve) to the medulla oblongata in the brainstem, where it is relayed and joins the same interoceptive/homeostatic system we have described for pungent food (see Figure 2, further below). In this way, ammonia, like pungent foods, can activate the homeostatic integrating centres from the brainstem to the insula and limbic cortex to initiate a homeostatic reset. Ammonia does so by activating TRP channels in the nose, and pungent foods do so by activating TRP channels in the gastrointestinal track. For individuals who use ammonia salts for the management of dissociative states, the reset of the interoceptive/homeostatic system supports, once again, the individual’s subjective sense of connection to the body, emotional self, and environment. The long answer to Jon’s question is provided below. Updated diagram of the interoceptive/homeostatic system (O’Sullivan et al., 2026) now including the trigeminal somatosensory input. The upper panel (A) shows the ascending and descending pathways of the interoceptive/homeostatic system on a stylised view of the mammalian brain. In black is the descending (motor) pathway connecting the cerebral cortex (insula and limbic system), brainstem, and spinal cord integrating centres that control the peripheral organs involved in homeostatic regulation. In blue is the ascending interoceptive pathway that is activated by transient receptor potential channels (TRPs) in the gastrointestinal tract, skin, and nasal epithelium. This ascending interoceptive sensory pathway targets and modulates all the integrating centres of the descending pathway from the medulla to the hypothalamus, limbic system, and insular cortex. The lower panel (B) is a block diagram showing the same descending and ascending pathways. For a more extensive description of the interoceptive/homeostatic system, see Appendix B: A more complete account of the neurophysiological effects of ammonia. Abbreviations: ACTH, adrenocorticotropic hormone; Ext Amyg, extended amygdala; DMNX, dorsal motor nucleus of the vagus; Hyp, hypothalamus; LPAG, lateral periaqueductal grey; PAG, periaqueductal grey; PBN, parabrachial nucleus; RVMP, rostral ventral medulla and pons; Sp5, Spinal trigeminal nucleus; VLPAG, ventrolateral periaqueductal grey; Sol, solitary nucleus; Thal, thalamus; TRPs, transient receptor potential channels. © Pascal Carrive and Kasia Kozlowska 2026.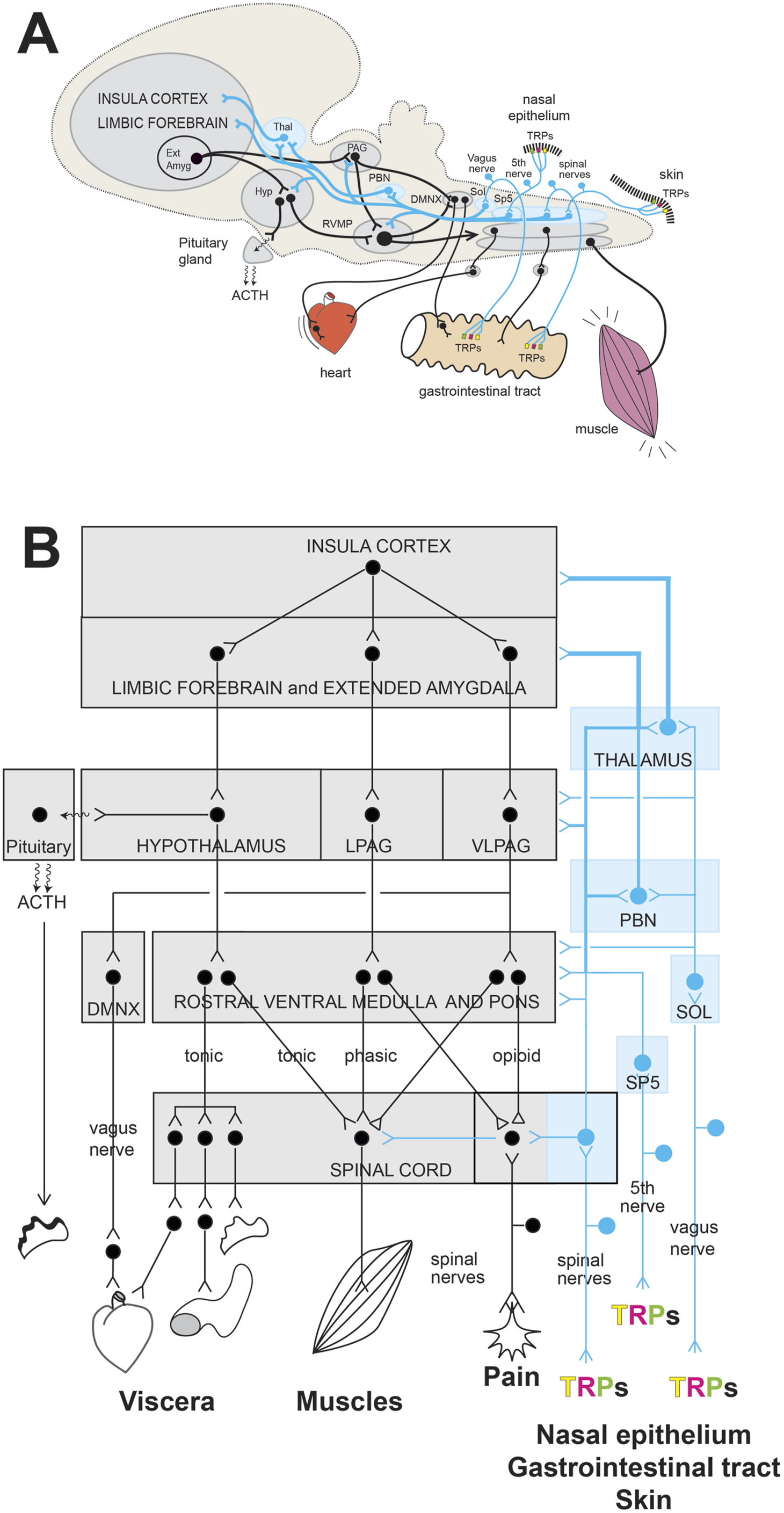
‘Ammonia is a noxious volatile chemical and is commonly encountered in household cleansers, artificial fertilizers, industrial pollutants, and in human and animal waste. Exposure to ammonia … elicits a distinctive pungent sensation in the nose’ (p. 153) (Dhaka et al., 2009). Most of us are familiar with this pungent sensation. Smelling salts are ammonia-based products used to prevent fainting or to revive someone who has fainted. They go back to the thirteenth century – or even earlier – and were at one time a staple of the doctor’s medicine bag (Richardson, 2019). ‘In the 17th century chemists obtained ammonium carbonate by crystallizing an aqueous solution of ammonia that was obtained through the distillation of horn and hoof shavings from harts (male red deer). The carbonate was initially called “spirits of hartshorn.” The addition of perfume to the ammonium carbonate resulted in a preparation that became known as smelling salts’ (Britannica, nd). In the 1800s, because of Queen Victoria’s interest in English lavender, salts of lavender became a popular choice (Museum, 2022). In Victorian Britain, smelling salts were carried around by upper-class women in decorative containers called vinaigrettes,
1
which held sponges infused with the smelling salts (Britannica, nd; Museum, 2022). Their popularity was related, in large part, to the fashion of restrictive corsets, within which women were often laced so tightly that diaphragmatic breathing was restricted, leading to faintness (see Text Box 1) (Isaac, 2017; Museum, 2022). The problem was sufficiently widespread that it was common for police constables to carry a container of smelling salt (Museum, 2022). According to the fashion historian Kass McGann, corsets have gone through many iterations. The ‘first surviving historical object we can reasonably call a “corset” … [is] the funerary garments of Eleanora of Toledo, Duchess of Florence’. Its function was, she says, as a foundation for the elaborate gown worn over it rather than ‘to form the body in a way that was unnatural’. It was in the seventeenth century that heavy boning came into bodices and ‘only with the development of metal eyelets in the 1830s where corsets became tight-laced’ (quoted from Guardian article by Ellie Violet Bramley (2024)). The Lancet and Edinburgh Medical Journal published a number of articles about the health risks associated with the corset, including death from syncope (Lancet, 1890), displacement of ribs and internal organs (Symington, 1892), and inability to breath using the diaphragm (Fish, 1909). According to Bramley (2024), a 2017 Charleston Museum exhibit, and a New York Times fashion column, the trend of wearing corsets is coming back into fashion (Friedman, 2026).Text Box 1. The corset
Modern preparations of smelling salts come in little packets that consist of ammonia, ethanol, water, and scented oils such as lavender, lemon, nutmeg, or eucalyptus (James Alexander Corporation, 2021; Museum, 2022). The inner vial is broken by crushing between the thumb and forefinger. The inhalant is then passed back and forth close to the nose of the affected person several times. Product descriptions describe the use of contemporary preparations ‘only to prevent and treat fainting’ (p. 1) (James Alexander Corporation, 2021). Off-label, smelling salts are used in professional sports by boxers, football players, soccer players, ice hockey players, and other athletes to increase alertness and to ‘get them back into the match quickly, even after a big hit’ (Bender and Popkin, 2024; Richardson, 2019). This use of smelling salts in sport is more controversial and may in some situations be associated with concerns about safety (see below).
To understand the neurobiology of smelling salts one must understand a little about the chemosensory cells that are part of the nasal mucosa in humans (See Text Box 2). Free ammonia released from smelling salts is a lipophilic irritant that is detected by one of the four chemosensory systems in the human nose: trigeminal polymodal nociceptor neurons that are part of the trigeminal chemosensory system. These neurons also detect other irritants that permeate the epithelium: air pollutants (e.g., sulphur dioxide), ethanol (liquor), acetic acid (vinegar), carbon dioxide (in soft drinks), menthol (in various inhalants), and capsaicin (in chilli peppers) (Purves, 2001b). The nasal cavity is able to sense a broad range of substances that are subjectively experienced as smells, pleasant or unpleasant, or as irritants. The four known chemosensory systems found in the nose are described below: The extended olfactory system includes the olfactory epithelium (olfactory sensory neurons in the nasal mucosa), the septal organ (a small patch of specialised olfactory sensory epithelium), and the vomeronasal organ (specialised in detecting pheromones). The olfactory sensory neurons have cilia – olfactory hairs – that sit on the surface of the nasal mucosa and react to odours to stimulate the olfactory receptor neurons and axons that make up the first cranial nerve and project directly to the olfactory bulb in the forebrain. The olfactory bulb sends projections to the primary olfactory cortex (including piriform cortex and corticomedial amygdala). The primary olfactory cortex, in turn, sends projections to the thalamus and hypothalamus, medial amygdala and hippocampus, and orbitofrontal cortex and insula. In this way, information about odorants reaches a variety of brain regions and brain networks, allowing olfactory cues to influence homeostatic, visceral, emotional, and cognitive responses and behaviours (Martial et al., 2023; Purves, 2001a). The scented oils that are added to smelling salts – lavender, lemon, nutmeg, or eucalyptus – activate this system (Fung et al., 2021). More broadly, substances used in aromatherapy also activate this system (Cui et al., 2022). Trigeminal polymodal nociceptive neurons have nerve endings that sit in the nasal epithelium, cell bodies that sit in the trigeminal ganglion, and axons that run in the trigeminal nerve (cranial nerve V) and terminate in the trigeminal nuclei located in the medulla oblongata (Purves, 2001b). The trigeminal ganglion is, in the head (the cranial nerve system), the equivalent of the dorsal root ganglia for the rest of the body (the spinal nerve system). Because TRP channels sensitive to ammonia have been demonstrated in dorsal root ganglia neurons (Dhaka et al., 2009), it is assumed that the same TRP channels are found in trigeminal polymodal nociceptive neurons. Thus, free ammonia that enters the nose activates TRP channels located on the free nerve endings of trigeminal polymodal nociceptive neurons. TRP channels convert the stimulus into action potentials, which are then transmitted in sensory trigeminal nerve fibres to trigeminal nuclei in the medulla and, from there, to the ascending pathway of the interoceptive/homeostatic system (see Figure 2) (Craig, 2002). Trigeminal polymodal nociceptive neurons detect, in addition to ammonia, a broad range of other irritants. In the nose these irritants are experienced as homeostatic feelings: burning, stinging, itching, tickling, cooling, warming, pungent, perception of atmospheric humidity, and so on (Brand, 2006). Solitary chemosensory cells (SCCs) are sentinel cells that sit in the nasal epithelium. These cells detect other classes of odorous irritants – including molecules produced by bacteria – ‘that are impermeable to epithelial tight junctions, and therefore unable to reach the trigeminal nerve fibers’ described above (p. 2 of 15) (Xi et al., 2023). Solitary chemosensory cells are innervated by trigeminal nerve fibres that relay information to the central nervous system, possibly into the ascending pathway of the interoceptive/homeostatic system. They can also trigger the release of neuropeptides into the nasal mucosa, evoking protective reflexes and pro-inflammatory responses (Xi et al., 2023 #17399). The vomeronasal (Jacobson’s) organ is a specialised chemosensory organ in the nasal septum of many vertebrates that detects pheromones and non-volatile chemical cues to trigger innate social, reproductive, and defense behaviours. It acts independently of the main olfactory system, sending signals to the accessory olfactory bulb and hypothalamus. The vomeronasal system is nonfunctional in humans. In the human embryo, the organ develops, and some of its cells migrate toward the hypothalamus. The organ then regresses, and the neural connections disappear (Trotier, 2011).Text Box 2. Chemosensory systems in the nose
Olfactory system
Trigeminal chemosensory system (trigeminal polymodal nociceptor neurons)
Trigeminal chemosensory system (solitary chemosensory cells)
The vomeronasal (Jacobson’s) organ
Stimulation of the trigeminal chemosensory system by ammonia and other irritants evokes respiratory protective reflexes coupled with an increase in heart rate (part of an arousal response) (Perry et al., 2016; Xi et al., 2023). Sneezing, coughing, breath-holding and exhalation help limit and clear the airways, protecting them from further exposure to the irritant (Nishino, 2000). An associated withdrawal reflex of the head or body also facilitates movement away from the irritant stimulus (Bender and Popkin, 2024). Both respiratory and cardiovascular responses are orchestrated at the level of the brainstem (RVMP, see Figure 2).
Beyond the level of the brainstem, information about ammonia continues its way up within the ascending pathway of the interoceptive/homeostatic system (shown in blue, in Figure 2) to target and modulate those integrating centres in the midbrain, hypothalamus, limbic system, and insular cortex that will orchestrate the homeostatic reset (shown in black in Figure 2). The insula – which is at the cortex system level – may be considered the top integration hub. Within the insula itself, information is processed along ‘a posterior-to-anterior gradient of increasingly complex integration’, representing shift from primary interoceptive/homeostatic processing to higher-order cognitive and emotional awareness (p. 223) (Craig, 2009; Craig, 2016). In this way, at the level of the insula, the interoceptive signal from the nose and other interoceptive information is transformed into a representation (mental image) of body state (Craig, 2009; Strigo et al., 2025). This cortical representation enables subjective awareness of body state – which is referred to as homeostatic emotions (Craig, 2016), homeostatic feelings, or physiological feelings (Pace-Schott et al., 2019).
In this way, information about ammonia, sensed by the trigeminal chemosensory system in the nose, ascends via the ascending pathway of the interoceptive/homeostatic system and is processed to yield both a homeostatic reset response via the descending pathway and a homeostatic emotion. These homeostatic emotions – the subjective experience of these irritants and pungent stimuli – are experienced as the ‘sting’ of ammonia, the ‘cooling effect’ of menthol, and the burning ‘heat’ of chilli peppers. Importantly, menthol and chilli peppers activate TRP channels at multiple sites. When inhaled, they are sensed by TRP channels in the nose, and when ingested, they are sensed by TRP channels in the gastrointestinal system.
Text Box 3 provides an overview of the neurophysiological effects of mild to moderate ammonia exposure that, in clinical settings, would be expected to disrupt patients’ dissociative states (shutdown dissociative states, flashbacks, or functional/dissociative seizures) or to help a patient wake up at the end of a fainting episode. In Appendix B to this article, we expand on this with additional information about the response to strong ammonia exposure in other settings – for example, to study the nasotrigeminal or diving reflex. On inhalation, free ammonia from smelling salts (NH3 gas) causes activation of trigeminal polymodal nociceptor neurons that are part of the trigeminal chemosensory system in the nose. Activation of these neurons (see Text Box 2) is thought to cause the following cascade of responses once the information enters the brain and ascends the interoceptive/homeostatic system starting from the brainstem (see Figure 2): The first response is a breath-hold coupled with a withdrawal reflex of the head or body to minimise inhalation and move away from the irritant stimulus (Bender and Popkin, 2024). The breath-hold is followed by a forced exhalation to clear the nasal passage (Bender and Popkin, 2024; Britannica, nd; Dhaka et al., 2009). The withdrawal reflex is associated with an increase in heart rate (Perry et al., 2016). The increase in heart rate is sympathetically mediated and generated from the brainstem. The stimulus information continues to ascend along the pathway of the interoceptive/homeostatic system (see Figure 2), reaching the insula, where the subjective awareness of the ‘sting’ of ammonia captures focus-of-attention to the present moment: the unpleasant sensation of ammonia. Our sensory-reset hypothesis posits that ammonia – in the same way as pungent foods – overrides the decrease in sensory information that is part of shutdown dissociative states and resets the central circuitry that modulates processing within the brain’s interoceptive/homeostatic system and associated networks. Ammonia inhalation has been shown to cause an increase in cerebral vascular conductance (a dilation of cerebral arteries) with an actual increase in blood flow in the middle cerebral artery, which is coupled to a sympathetically mediated increase in peripheral vascular resistance (a vasoconstriction of arteries in trunk and limbs) (Perry et al., 2016). These two vascular events essentially contribute to a redistribution and increase in blood flow to the brain, which will make the subject more alert. Interestingly, no significant increase in blood pressure has been reported (Perry et al., 2016). A more direct effect of ammonia on the cerebral vasculature after absorption in the blood stream has been proposed but has not been verified (Andersson et al., 1981; Chodobski et al., 1986; Perry et al., 2016).Text Box 3. Presumed neurophysiological effects of mild to moderate ammonia exposure in the clinical setting
Protective reflex
Increase in heart rate
Homeostatic emotion (sensation of the irritant)
Homeostatic reset of the brain’s interoceptive/homeostatic system
Vasodilation of cerebral arteries
We turn briefly to the use of ammonia salts in sports because in our current cultural setting, ammonia inhalation by athletes is common. An intriguing finding from the sports literature is that the use of ammonia by athletes does not yield any change to their muscular performance (Bender and Popkin, 2024; Perry et al., 2016). These data suggest that ammonia inhalation is used by athletes to feel more alert (clearer in the mind) due to the increase in arousal and associated cardiovascular changes, increase in blood flow (cerebrovascular dilatation), and the shift of attention to the ‘sting of ammonia’ (homeostatic emotion), coupled with a perception of performance enhancement (see Text Box 3). The potential risks of ammonia inhalation in sports is briefly summarised in Text Box 4. Potential risks of ammonia inhalant use and misuse in sports have been reported (Bender and Popkin, 2024). – The activating effects of ammonia may potentially mask the symptoms of a neurological injury – and decrease in the level of consciousness – so that the injured person continues to play, rather than being pulled out of the game. – Use of ammonia inhalants in episodes involving head injury may cause the injured person to reflexively move the head away from the irritant (ammonia), thereby exacerbating an underlying injury. – In sports involving heavy upright resistance exercise that necessitates the use of the Valsalva manoeuvre – as in weightlifting – hypotension may be induced, thereby causing dizziness or syncope (a paradoxical response).Text Box 4. Potential risks of ammonia use in sports
Pickle juice and other pungent foods as a strong distractor
A number of physicians commented on the use of pickle juice and other pungent foods as a distraction mechanism. Jon Stone, the neurologist, wrote, ‘It makes sense to use a strong distractor. We need practical ideas like this’ (Email communication, 13 January 2026). And Gaston Baslet, a Harvard Medical School neuropsychiatrist, wrote ‘While the biological explanation is hypothetical, I think that sensory stimulation as a way to reset attention, top-down resources that breaks symptoms (even temporarily) is a plausible mechanism’ (Email communication, 14 January 2026).
Here we note that the interoceptive/homeostatic system that processes information about pungent foods is the same system that processes information about pain, itch, temperature, pH (potential of hydrogen), and other homeostatic information about body state. The idea that ‘pain interrupts and demands attention’ was put forward by Chris Eccleston and Geert Crombez in 1999 in a landmark article, ‘Pain Demands Attention: A Cognitive-Affective Model of the Interruptive Function of Pain’ (p. 356) (Eccleston and Crombez, 1999). But as we all know, any of these stimuli, when they are unpleasant, irritating, or jolting in some way, demand attention. In the above article the authors defined attention in the following way Attention is defined as selection for action. Intrinsic to the selection of pain is the urge to escape … The selection of pain interrupts attention, ruptures behavior, and imposes a new action priority to escape. (p. 356)
At that time (in 1999), A. D. (Bud) Craig, an anatomist and neuroscientist whose groundbreaking work at the Barrow Neurological Institute was to advance our ‘understanding of the neuroanatomical basis of the bodily self, emotion, and subjective time’, had only just begun his life-long work (p. 1) (Strigo et al., 2025). In time, Craig was to map an ascending neural pathway for homeostatic information from the body to the brain, determining that in the brain of primates (including humans), the insular cortex was responsible for making representations of these elemental feelings, with the anterior insular enabling for subjective representations (mental images) of the physiological condition of the body (see also previous section) (Craig, 2002; Craig, 2013a). In this way, we not only respond to homeostatic information implicitly and automatically, but we also hold a mental image of the physiological condition of the body and are therefore aware of the feeling of pain, itch, the sensation caused by pungent foods and irritants (like ammonia), and so on. And when the stimulus is unpleasant or salient in some other way, our attention is ‘caught’ by these stimuli.
These homeostatic feelings from the body (in the insular cortex) are ‘conjoined with homeostatic motivations that guide adaptive behaviours (in the cingulate cortex)’ (Strigo and Craig, 2016). The cingulate cortex guides both implicit/autonomic/non-voluntary behaviours and conscious explicit/voluntary behaviours (Pearson et al., 2011). Put simply, homeostatic feelings are the perceptual correlate of a behavioural motivation (Craig, 2013a).
The above-described understanding of the interoceptive/homeostatic system helps us answer Stone’s and Baslet’s question about pungent foods – and also ammonia – as a distractor. When homeostatic feelings signal danger or potential danger, they capture attention and shift focus-of-attention to the here and now, thereby enabling conscious decision-making to be recruited into the action-response process. Thus, the individual can replace the lid on the offending cleaning agent and don a protective face mask to minimise inhalation fumes whilst proceeding with the task of cleaning. It is important to note, however, that at this point in the process – when homeostatic feelings become conscious – automatic responses such as protective reflexes, increase in arousal, and so on will already have been implemented by the nervous system, and, where relevant, the override of top-down over-modulation will have already occurred (see previous section on PTSD). In this manner, the ‘distractor’ element of the interoceptive/homeostatic response to irritants and other danger signals is just one component of a larger package of responses. In our view it is this larger package of responses to pungent foods, ammonia, and other irritants – the sum total of responses – that work together to enable disruption of states of dissociation.
The homeostatic sensory-reset hypothesis and the predictive-coding model of FND and dissociative disorders
In a new, 2026 article in Brain, Stanley Lyndon of Harvard Medical School (Lyndon, 2026) updates and expands the predictive-coding model of FND published by Mark Edwards and colleagues in 2012 (Edwards et al., 2012). The articulation of this new model, which includes both FND and dissociative symptoms, prompted us authors to consider how activation of the brain’s interoceptive/homeostatic system by pungent foods may potentially dovetail with the predictive-coding model of brain function.
As Lyndon explains, predictive coding views the brain as a layered system that constantly compares prior predictions (expectations shaped by past experience) with incoming sensory signals, and shows how an unhelpful prediction can dominate perception and action when it is given too much weight or confidence (precision). Within this framework, predictions reflect the brain’s best estimate of current or impending states, while precision refers to the weighting assigned to those predictions relative to sensory feedback. (p. 2, Epub ahead of print) (Lyndon, 2026)
What Lyndon’s new model adds is to embed precision control within a four-level hierarchy – affective, interoceptive, proprioceptive, and spinal. In this model, increases in arousal play a key role in ‘igniting’ surges in any combination of channels or symptom streams. The channels include motor, sensory, cognitive, and visceral symptoms that are commonly seen, in various combinations, in patients with functional and dissociative disorders.
Using this elaborated predictive-coding model, Lydon postulates that ‘when autonomic arousal crosses a channel-specific threshold, the system can briefly overtrust whatever prediction is active at that moment, producing a rapid surge in precision that can momentarily flood the system and lock a symptom into place’ (pp. 5–6, Epub ahead of print). In other words, ‘autonomic arousal can temporarily increase the brain’s confidence in its own predictions faster than sensory feedback can correct them’ (p. 6, Epub ahead of print). Over time, ‘as precision rises and falls, symptoms wax and wane, and selective focus can transiently shift precision weighting within the attended channel’ (p. 8, Epub ahead of print). According to the model, changes in focus-of-attention also shift confidence in predictions, thereby causing symptoms to amplify or wane. Attention to symptoms increases the brain’s confidence in the prediction (symptoms amplify), and attention away from symptoms decreases the brain’s confidence in the prediction (symptoms wane).
In this updated predictive-coding model, irritants and pungent foods would potentially recalibrate the brain’s predictive-coding system via two mechanisms. First, they provide a strong interoceptive signal that – akin to pain, temperature, acid, and inflammation (TRP channel activators) – represents a potential threat to homeostasis and cannot be dampened down and ignored. In this way, irritants and pungent foods may lead the brain to recalibrate the weight given to incoming sensory information, enabling it to update and potentially correct aberrant predictions. Second, as part of this same homeostatic process, the subjective awareness of the sensations produced by pungent foods – such as the burning ‘heat’ of chilli peppers, the ‘cooling effect’ of menthol, or the ‘bite’ of wasabi and other mustards – shifts the focus-of-attention and enables aberrant processes to wane.
What about aromatherapy?
As we noted earlier, in response to our article about the use of pungent foods as a grounding strategy to disrupt dissociative shutdown, Lucia Tesolin, the Peruvian neurologist, told us about a current study that is examining the use of olfactory stimuli in patients with functional/dissociative seizures (Tesolin, nd). In that study, patients trial a range of olfactory stimuli – palo santo (Bursera graveolens, a native tree,), galán de noche (night jasmin), eucalyptus, fresh coffee, cinnamon, anise, aromatic fruits (mango, guava, lime), and Amazonian fruits such as aguaje – and use them as olfactory stimuli and early self-regulation tools when dissociative symptoms begin to emerge, to avert the functional/dissociative seizure (Personal communication 2 March 2026). Tesolin’s comment raises the question as to the neurobiology of aromatherapy and its potential use in dissociative states (including functional/dissociative seizures).
Essential oils – also known as scented oils, volatile oils, volatile chemicals, or odour molecules – ‘are the naturally aromatic oily liquids produced by plants, which are responsible for their essence or odor … [They] can be extracted from different parts of plants, including their leaves, barks, flowers, buds, seeds, and peels … [They] are a concentrated hydrophobic mixture of hydrocarbon volatile compounds that easily evaporate at room temperatures … In most plants, the major components of [essential oils] are terpenoid and phenylpropanoid derivatives. Terpenoids are the main components (comprising approximately 80%), but phenylpropanoid provides the flavour and odour of the [essential oils]’ (pp. 1–2) (Sattayakhom et al., 2023). Essential oils in which the terpenoid component has been removed are called terpeneless essential oils (Gattefossé, 1993 [1937]).
Aromatherapy is the use of essential oils from plants as therapy for the purpose of provoking psychological or physiological responses to improve physical, mental, and spiritual well-being (National Cancer Institute, 2023; Schneider et al., 2019). The practice of using essential oils for healing – because of their antimicrobial, anti-inflammatory, antioxidant, analgesic, antispasmodic, and sedative properties – goes back to antiquity. Text Box 5 provides a brief summary of the historical use of substances with olfactory qualities – including essential oils – in Greco-Roman, Byzantine, and Arabic medicine, with a particular emphasis on FND. The term aromatherapy is of more recent origin. It was coined by Maurice Gattefossé, who, in the early 1900s, worked as a chemist in a family-owned perfume company in France (Gattefossé, 1993 [1937]). Historian Helen King describes how, in the texts of the Hippocratic corpus (450–250 BC), some of the writers conceptualised female medical problems – including a range of functional symptoms such as functional/dissociative seizures – as being caused by the movement of the womb (Helen, 2024). In this conceptualisation the womb would end up at some deviant destination in the body, resulting in suffocation (suffocation of the womb) and a range of associated physical symptoms. Substances with olfactory qualities were often used to treat this condition. ‘The pattern [was] usually that fragrant substances [were] applied to the vulva, in order to attract the womb back, while foul-smelling substances are placed under the nostrils to drive the womb away from the upper parts of the body’ (p. 21). Fragrant substances included various essential oils, whist foul-smelling substances included cabbage, garlic, onion, bitumen, and castoreum (from beaver caster sacs). ‘In addition – and in apparent contradiction – fragrant oils [could] be rubbed on the head and strong-smelling substances drunk, often in wine’ (p. 21). Various versions of ‘scent therapy’ continued to be used across centuries in Greco-Roman medicine, Byzantine medicine, and Arabic medicine. Translation of texts from Arabia returned some of the classic knowledge back to Europe in eleventh and twelfth centuries, where it had been lost during the early Middle Ages (sometimes known as the Dark Ages). Notwithstanding, not all knowledge was lost. A Latin manuscript from Western Europe from the eighth and ninth centuries – titled ‘De causis feminarum [On the Causes of Women]’ gave ‘practical advice on what to do “si vulva suffocantur” [if the womb is suffocated] … The patient should be given burned and pulverized stag’s horn in wine’ (p. 54) (Helen, 2024). At that time, burned and pulverized stag’s horn was a source of ammonia salts (see ammonia salts section). The use of essential oils continued into the twentieth century. In his 1937 book about aromatherapy, René-Maurice Gattefossé made reference to various plant extracts for the treatment of functional/dissociative seizures. In his discussion of asafoetida – a gum extract from the roots of the ferula plant common in Central Asia – Gattefossé reports ‘serious attacks of [functional/dissociative seizures
2
] can be greatly helped by inhalation of the essential oil, stopping attacks almost immediately’ (p. 30). Asafoetida has a pungent, unpleasant odour and is used in small amounts as a garlic-and-onion substitute or to add an umami flavour to food. Gattefossé also notes that other clinicians report the use of pleasant-smelling scents for the same ailment: ‘the odours given off by heliotrope and vanilla are antispasmodic and help sooth emotional manifestations of varying degrees of gravity, commonly known as [functional dissociative seizures
3
]’ (p. 69).Text Box 5. A historical perspective on the use of essential oils for the treatment of functional symptoms
The contemporary scientific literature about aromatherapy is characterised by multiple methodological difficulties. A broad definition of aromatherapy refers to the use of essential oils via a range of modes of administration: the nose (inhalation), skin (ointments, compresses, massage, and bathing), oral administration, or rectal or vaginal suppositories. In contrast, more narrow definitions – for example, restricting aromatherapy to inhalation aromatherapy – coupled with clarity about the quality of the preparation, dosage, and administration mode, are more amenable to comparative research and critical appraisal (Schneider et al., 2019) (see Text Box 6). Notwithstanding, differences in the chemical composition of essential oils due to extraction method, growing conditions, harvest season, and place of cultivation, along with the introduction of impurities and synergistic effects of constituents, remain important confounders (Ali et al., 2023; Girão, 2024; Girão et al., 2024; Khan et al., 2023). Moreover, because essential oils are known by their odour, there is also the difficulty of blinding the patient group and controlling for the concurrent therapeutic effects of the brain’s placebo response and the effect of positive expectation (Girão et al., 2024). All of the above factors – coupled with a lack of standardized research – make it challenging to establish a good evidence base about the efficacy of essential oils and about adverse-effect profiles. Schneider and colleagues (2019) put forth the following basic preconditions for effective aromatherapy (Schneider et al., 2019). It must involve the following: – The use of ‘volatile compounds of essential oils by inhalation’ (p. 4) – Delivery method to ‘directly and specifically target the nose’ – for example, by lipstick-sized nasal inhalers (p. 4). The reason is that ‘regular breathing only results in 5–10% of the inhaled air reaching the olfactory epithelium in the nose’ (p. 7) – Administration ‘in high enough molecule concentrations that are able to trigger physiological changes’ (p. 4) – ‘Natural essential oil compounds of high phytochemical quality’ (p. 4) – Sufficient potency ‘to strongly stimulate the olfactory system without causing habituation’ (p. 4)Text Box 6. Effective aromatherapy
Text Box 7. Administration routes for aromatherapy and potential neurophysiological modes of action (developed from information in ‘Men and Colleagues’ [2025])
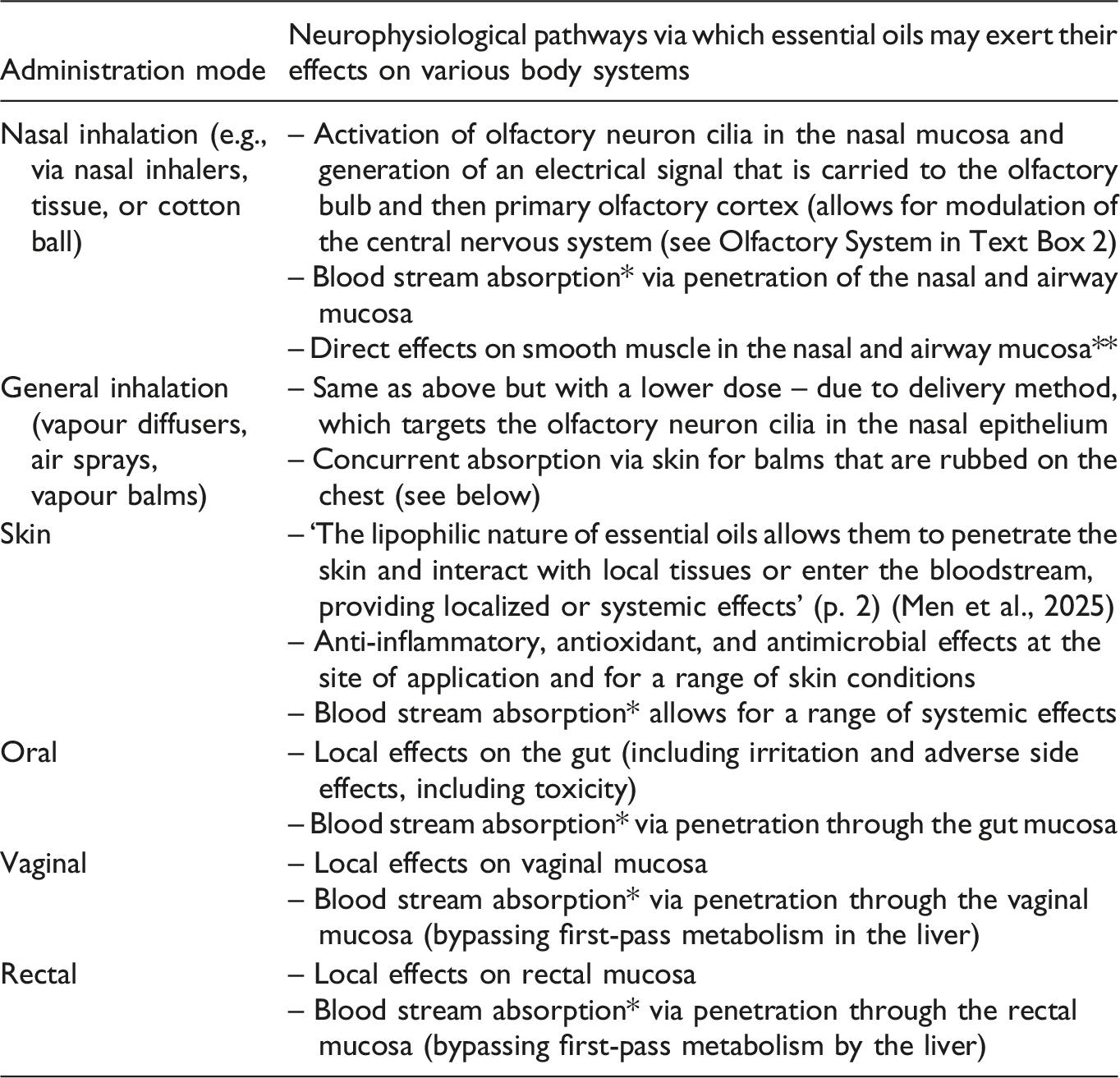
*Absorption into the bloodstream allows for systemic effects, including those on the central nervous system (CNS) because certain olfactory molecules are capable of crossing the blood–brain barrier, directly targeting CNS structures.
**For example, rosemary extracts or eucalyptus oil extracts relax smooth muscle in the airways.
In the discussion that follows, we examine the neurobiology of essential oils: how do they work? In this discussion, we restrict the meaning of aromatherapy to inhalation aromatherapy because this route of administration is the one that both patients and their families are likely to use in the context of dissociative states.
In the nose, the primary effect of essential oils is stimulation of the olfactory system (cranial nerve 1) (see Text Box 2) (Brand, 2006). Activation of the olfactory system is responsible for the therapeutic effects of essential oils—for example, the calming effect of linalool found in basil, bergamot, coriander, ho wood, lavender, and rosewood oils and in many other plants (Harada et al., 2018). When essential oil molecules hit the nasal mucosa, they activate G protein–coupled receptors located on the cilia of olfactory sensory neurons in the nasal epithelium, and an electrical signal is generated (Chen et al., 2022). This signal ascends via the olfactory tract – the nasal-brain pathway – to the primary olfactory cortex located at the medial base of the frontal lobe and antero-medial part of the temporal lobe. It includes the piriform cortex and corticomedial amygdala. From there, projections to multiple brain regions (including the thalamus, hypothalamus, medial amygdala, insula, and orbitofrontal cortex) allow essential oils to modulate multiple neural and neuroendocrine systems involved in stress-system activation, perception, cognition, and behaviour. Animal research suggests that ‘the direct link to the brain operates at a transmission speed of about 200 milliseconds and exceeds that of most other physiological senses, and that one single molecule suffices to trigger an action potential on the receptor site’ (p. 2) (Khan and Sobel, 2004; Schneider et al., 2019; Su et al., 2009). In other words, the threshold for an olfactory response (odour threshold) is very low.
Some essential oils – but not all – may also activate the trigeminal system (cranial nerve 5), allowing for processing via the interoceptive/homeostatic system. Activation of the trigeminal system, however, requires a higher dose, with the consequence that the stimulus is experienced as an irritant (Cometto-Muñiz et al., 1998). In other words, the threshold for a trigeminal response (pungency threshold) is much higher, and the resulting sensation is different to that of an odour.
Integration of the two systems – the olfactory and interoceptive/homeostatic – may occur at the level of the insula or earlier at the level of the mediodorsal thalamus, which also projects to the insula, as both receive feed-in from the primary olfactory cortex (Brand, 2006). In this way, information about odour – whether the trigeminal system is activated or not – also ascends to the insula, where it yields a mental image of the odour, allowing for our subjective experience: the smell of the given scent (see discussion in previous section, and Figure 2) (Perszyk et al., 2023). A scent on its own, however, may not produce the fast and powerful homeostatic reset that is produced by a trigeminal stimulation. This may be because the source of an odorous stimuli is likely distant and therefore no concurrent threat to homeostasis, whereas the source of a trigeminal stimulus is already in close proximity to the body, therefore posing a threat to homeostasis (high salience) and requiring an immediate response.
Future research will need to determine whether odorous sensations that are pleasurable (utilising the olfactory system only) or those that are also pungent (utilising both the olfactory and trigeminal system) have greater utility for individuals who are using odorous sensations as a grounding strategy to disrupt dissociative states.
Conclusion
We conclude by thanking those who wrote to us asking questions and initiating what proved to be such engaging conversations about the neurobiology of pungent foods, ammonia salts, and aromatherapy – including the role of mental representations and focus-of-attention. We are grateful to our readers for challenging us to expand our analysis and consider so many new scientific and clinical issues.
As noted by the neurologist Jon Stone, we clinicians need a range of practical ideas – such as those discussed above – to provide our patients with options as to how they manage dissociative states (including functional-dissociative seizures), panic, dysregulation, anxiety, states of high arousal, or distressing memories that may arise because of past trauma. Being able to offer suggestions for strategies that harness the body’s own regulatory systems, which patients can trial and experiment with, allows for a broader range of options for everyone involved in the healing process.
Footnotes
Acknowledgements
We thank all the readers of our first article, ‘Pickle Juice – and Other Pungent Foods – as a Grounding Strategy for Managing Episodes of Dissociative Shutdown’, for taking the time to write to us, to comment on the article using other communication platforms, or to engage in face-to-face discussions during teaching sessions. The issues raised by your questions formed the basis for the current work. We thank the patient who kindly gave consent to include her vignette in the article. We also thank all those who are named in the article for consent that allowed us to quote your thoughtful response, reflections, and questions.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.