
Abstract
Paraesophageal hernias (PEH) represent a minority of hiatal hernias and yet have the highest potential for catastrophic consequences for patients. Patients with paraesophageal hernias tend to be older with more comorbidities. The risk to benefit calculation in the treatment of patients with a minimally symptomatic PEH can complicated. Surgical repair and management of hiatal hernias has come a long way since the first repairs were undertaken. Surgical risk has become minimal, while gains in quality of life have increased. Decisions for surgery should be undertaken by well informed patients who have benefited from consultation with a gastroenterologist and foregut surgeon. For most patients suffering with a symptomatic PEH, the risk benefit calculation has swung firmly toward surgical repair when a multi-specialty approach is taken.
Since the first half of the 20th century, surgeons have struggled with themselves, and the medical community at large, over the ideal operative indications, timing of intervention, and operative technique for hiatal hernias. Soresi, Harrington, Sweet, Allison, Barrett, Belsey, and Nissen all wrote on this conundrum. In 1919 Soresi was the first to challenge us to listen to the patient for signs or symptoms of a “small” hernia. Small, in 1919, was anything less than a complete intrathoracic stomach. I quote and refer you to his paper.
“It is the purpose of this paper to call to the attention of internists and of surgeons the frequency of diaphragmatic hernias, because patients suffering from this condition are not properly treated. . .This lack of interest is not easily explained, because diaphragmatic hernias give rise to so many complicated and serious symptoms, which if not properly attended to, will lead the patient to an unfortunate life and premature death.”
1
It would seem that modern medicine and surgery have advanced so far in the 100 years since Soresi’s publication that we have come full circle, needing to examine the management of paraesophageal hernias.
Paraesophageal hernias (PEHs) represent a minority subset (14%) of all hiatal hernias. 2 However, from this minority stems the majority of potentially serious and life-threatening complications from hiatal hernias. Hiatal hernias are classified into 4 types, with PEHs represented by types II to IV. Type II hernias involve displacement of the gastric fundus into the mediastinum only, while the gastroesophageal junction remains anchored at the esophageal hiatus. Type III hernias, the most common of PEHs, involve displacement of both the fundus and gastroesophageal junction into the mediastinum. 3 Type IV involves the additional herniation of any abdominal organs—commonly small intestine, colon, or spleen.
The truly asymptomatic paraesophageal hernia is rare. Patients will almost always exhibit one or more of the following signs or symptoms:
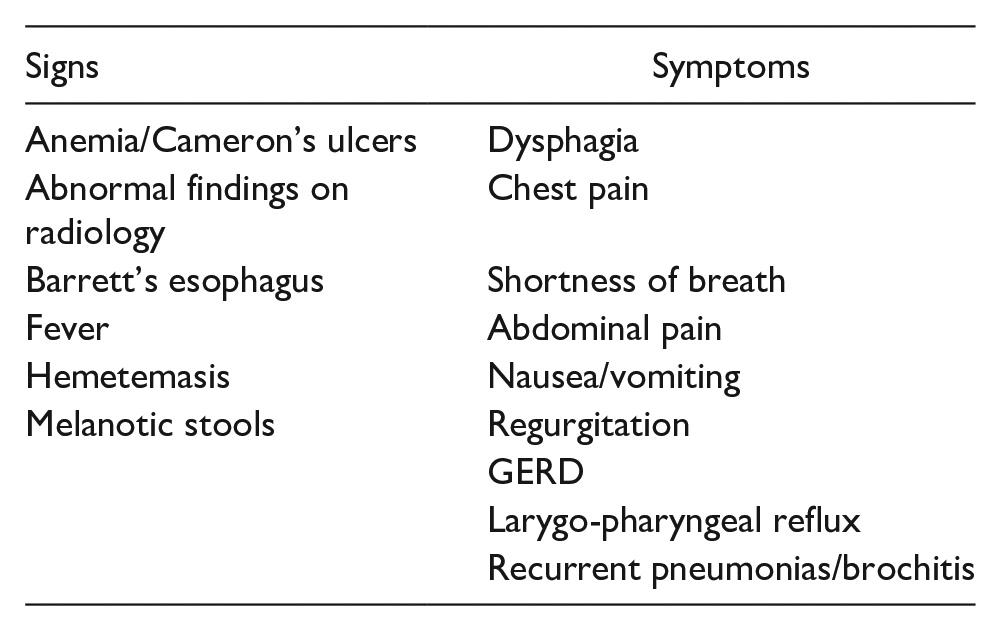
Life threatening complications may develop from kinking of the left gastric artery or significant organo-axial/meso-axial rotation leading to eventual devitalization of the stomach and eventual perforation. Anemia from Cameron’s ulcers may also be life threatening as it is often insidious and may lead to a cardiac event in addition to all of the other symptoms of anemia.
Early common thinking was that all paraesophageal hernias should be repaired due to these potential devastating complications. Skinner and Belsey reported in 1967 that in patients with known PEH, 26% died of complications directly related to the PEH. 4 Treacy et al 5 noted that 45% of patients medically managed will have symptom progression. More recently, several authors have found that this complication rate may be as low as 14%.6,7 With advancements in medical therapy, specifically proton pump inhibitors, these studies may overstate both the morbidity and mortality of the unrepaired PEHs. However, there is no question that patient suffering and potentially preventable mortality occurs when surgical management is not entertained, a trend that continues today.
From a surgical standpoint, laparoscopy has multiple known benefits over the open approach to most operations and PEH repair is no exception. In the early laparoscopic era, this was considered a tour-de-force operation, with operative times ranging from 3 to 4 hours and a lenght of stay of 2 to 4 days.8 -10 However, with improvements in both technique and technology, the modern laparoscopic approach to PEH repair has transformed this formerly morbid operation into an outpatient procedure with minimal morbidity and less than 1% mortality.11,12
Today, PEH repair remains a technically challenging operation and should be performed by specially trained, high-volume surgeons in hospitals capable of caring for these complex patients. The literature is consistent and replete in its support that significant gains in quality of life, with low morbidity and near zero mortality can be obtained in high volume surgical practices. Schlottman et al, advocate that, “High volume hospitals are associated with higher rates of laparoscopic operations, decreased surgical morbidity, and shorter length of hospital stay.” Volume standards should be implemented in order to obtain better postoperative outcomes. 13 Whealon et al, found an inverse relationship between hospital volumes and mortality, noting a 10% reduction in adjusted odds of in-hospital mortality for every increase in 10 cases per year. Additionally, hospitals performing less that 10 cases per year had double the mortality of high-volume hospitals. 14 The recurrent PEH requiring reoperation represents additional complexity and operative risk, but further centralization of care should provide consistent symptom improvement while maintaining excellent outcomes. Lovece et al reported their results recently and demonstrated nearly a 20 point improvement in quality of life scores with no patients needing revisional surgery at 56 months follow-up. 15
Taking into account the patient’s symptom profile, overall medical condition, quality of life scores, and individual patient goals; it is up to the responsible, appropriately qualified, high-volume surgeon to be able to assess the risks and benefits of surgical intervention. This conversation should be held in the spirit of shared decision making to ensure the patient, family, gastroenterologist, and surgeon are all aware of the preoperative work-up, medical risk assessment, potential need for preoperative optimization, as well as the perioperative nutritional needs, expected post-operative course, and long-term outcomes.
Patients undergoing a PEH repair for symptoms should expect to find relief of classic reflux symptoms and improvement in their quality of life. Hall et al, 16 found statistically significant improvement in SF-36, GERD HRQL, LPR-RSI scores at 3 years post PEH repair. In a meta-analysis Louie and colleagues 17 found similar global improvement in symptoms, with patients over the age of 70 exhibiting greatest degree of improvement. Extraesophageal symptoms are less well studied, but substantial evidence exists that pulmonary function as well as anemia from Cameron’s ulceration are all improved after PEH repair.18 -20
A common postoperative concern, repair durability and hernia recurrence have been studied extensively, culminating in an excess of conflicting results with inconsistent methodology and terminologies. Single center studies, different types of repair, meta-analyses, time to recurrence, what is a recurrence? How was it found? Are they being looked for?—the literature can be exhausting.
While it is beyond the scope of this paper to perform a complete review, my discussions with patients on the subject are informed by the literature and our own longitudinal continuous quality improvement database. Jobe et al found that at 3 years postoperative, 86% of patients rated their outcome as excellent, while 32% were found to have a recurrence on objective follow-up esophagram, though most did not require reoperation. Mattar et al, 21 found similar results at the 3 year postoperative mark, with 74% of patients off PPIs, 90% of patients satisfied with their outcomes, and a recurrence rate of 33% with most not needing surgical intervention. Finally, the study that should inform our conversations around recurrence and long-term outcomes is the seminal study by Oelschlager et al, a prospective, randomized trial looking at the use of biologic mesh versus no mesh during PEH repair. At nearly 5 years follow-up, they found statistically significant improvements in quality of life even though 44% were on a PPI or other antacid. The recurrence rate was high at 59% (no mesh) and 54% (mesh) but only 3.5% required reoperation for symptoms. 22 The lessons gleaned from the studies above and throughout the literature are that recurrence rates are relatively high, especially when we go looking for them in the asymptomatic patient. However, patient satisfaction is high as well. As mentioned above, PPI use should not be an indicator of failure—but rather viewed as a tool in both the gastroenterologist’s and surgeon’s toolbox to improve quality of life. Certainly, the mere fact that recurrences happen should not be a reason to deny a patient a life-changing and potentially life-saving operation.
In conclusion, the completely asymptomatic patient with a paraesophageal hernia is rare. Most patients exhibit a myriad of signs/symptoms and suffer from significantly diminished quality of life. The “wait and see” approach to a patient with a PEH is likely of historic importance only given the well-established progression of symptoms and potentially catastrophic consequences. The modern laparoscopic approach and improved surgical tools and techniques has yielded operative therapy that is both safe and effective. The patient with a known PEH will likely benefit greatly from surgical repair, with the expectation of improved quality of life and diminished, or even cessation, of PPI reliance for symptom control. We need only to “listen” to our patients and be willing to “hear” what they are telling us about their symptoms and the burden they represent, easily quantified using PRO instruments like the GERD-HRQL, LPR-RSI, and other widely available GERD-specific surveys. Early involvement of a qualified foregut surgeon is paramount, both to assist in clinical decision making, as well as to ensure the best possible outcomes in patients undergoing surgery repair. We would encourage foregut surgeons to follow their own patients longitudinally so that their discussions with patients, gastroenterologists, and other medical providers can be informed by both the current literature as well as their own results. Renewed attention to patients with a PEH by gastroenterologists and surgeons alike will allow for continued fostering of collaborative efforts for all patients suffering from diseases of the foregut.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.