
Abstract
Operations for esophageal and proximal gastric cancers are increasing. The most common surgical intervention performed for this patient population is esophagectomy. Regardless of the technical approach pursued, creation of a neo-esophageal conduit imposes various anatomic and physiologic challenges. These patients often undergo additional endoscopic and surgical revision procedures to improve their quality of life. Some of the most common complications encountered by medical professionals managing these challenging patients include para-conduit hiatal hernias, acid and biliary reflux, and redundant or dysfunctional neo-esophageal conduit. As survival and long-term outcomes improve, clinicians are encountering novel complications including conduit neoplasia and tracheal conduit fistulas. This review highlights some of the common complications post esophagectomy with focus on initial diagnosis and management strategies.
Key Learning Points
• Paraconduit hiatal hernia post esophagectomy is thought to increase in prevalence with adoption of minimally invasive techniques and improved long-term outcomes in esophageal and proximal gastric cancer patients.
• Although rare, long-term survival in this patient population is leading to increased detection of neoplastic changes in the neo-esophageal conduits, which carries a significant mortality if not diagnosed early.
• Cooperation amongst surgeons, gastroenterologists, and oncologists is paramount for successful management of common complications encountered after major surgeries such as esophagectomy.
Introduction
Esophagectomy is most commonly performed for cancer of the esophagus or proximal stomach. These tumors remain an important cause of cancer death worldwide, with slowly increasing incidence (Table 1) and slowly improving 5-year survival. Surgical resection remains the mainstay of treatment for non-disseminated disease outside of superficial mucosal lesions (T1a)1-3 so most long term survivors of more locally advanced disease have undergone esophagectomy, either Ivor Lewis or transhiatal. Therefore, together with a small group of patients who have undergone esophageal resection for achalasia, peptic stricture, or caustic ingestion, there is a growing population of patients with chronic esophageal conduits (mostly gastric), some of whom develop problems with paraconduit hernia, stasis (related to antropyloric dysfunction, redundancy, and/or tortuosity), bile reflux, and/or conduit dysplasia/neoplasia. In this chapter we discuss the surgical approach to these problems and briefly discuss other more unusual problems with the esophageal replacement conduit such as non-anastomotic stricture, twist, and fistula to the airway. With continuing improvements in treatment for esophageal and proximal gastric cancer, an increasing number of cured post-surgical patients will present to the attention of foregut specialists, underscoring the importance of recognizing these nuanced challenges.
Trend of Relative Incidence Rates of Esophageal Adenocarcinoma, Esophageal Squamous Cell Carcinoma, and Gastric Adenocarcinoma in the US.
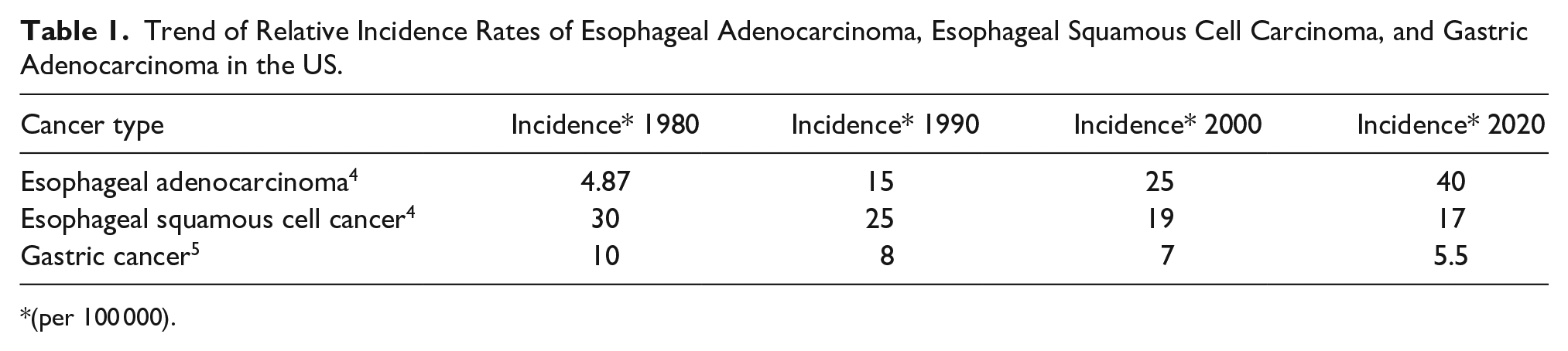
(per 100 000).
Conduit Complications
Para-Conduit Hiatal Hernia (PCHH)
The true incidence and natural history of paraconduit hiatal hernia (PCHH) following esophagectomy are both unknown, and the management is controversial. The reported incidence in the literature ranges from 1% to 30%. Studies which include routine review of postoperative imaging studies report a higher incidence. Most patients can be managed expectantly. Bowel necrosis is rare but possible.
The natural history of PCHH is variable. If this finding is absent 2 years post esophagectomy, it is unlikely to develop later. Usually the hernia contains bowel, most commonly colon but often small bowel too. Herniation of spleen or left lateral liver is unusual. Most of the time, the bulk of the hernia contents are in the left chest, but occasionally the hernia is predominantly right sided or bilateral. In some patients, the amount of viscera in the chest remains stable for years, but in general the hernia will enlarge over time. Serial imaging is required to determine the rate of enlargement, which can be quite variable.
Utilization of minimally invasive esophagectomy (MIE) (laparoscopic and robotic) has increased exponentially over the last decade.6,7 The advantages include decreased post-operative pain, pulmonary complications, and decreased length of hospital stay as well as similar oncologic outcomes as compared to the standard open surgical approach.2,6,7 However, one of the shortcomings of this technique is the increased rate of developing paraconduit hiatal hernias (PCHH) (Figures 1 and 2).8,9 The incidence in one retrospective analysis was 10% in all MIE patients with a median time to diagnosis of 258 days. 10 It should be noted that a majority of patients with PCHH were asymptomatic and were discovered at the time of interval imaging for oncologic follow up.8-10 Potential reasons for PCHH in the setting of MIE include decreased post-operative adhesions, difficulty performing a hiatoplasty, and use of insufflation gas.8,9
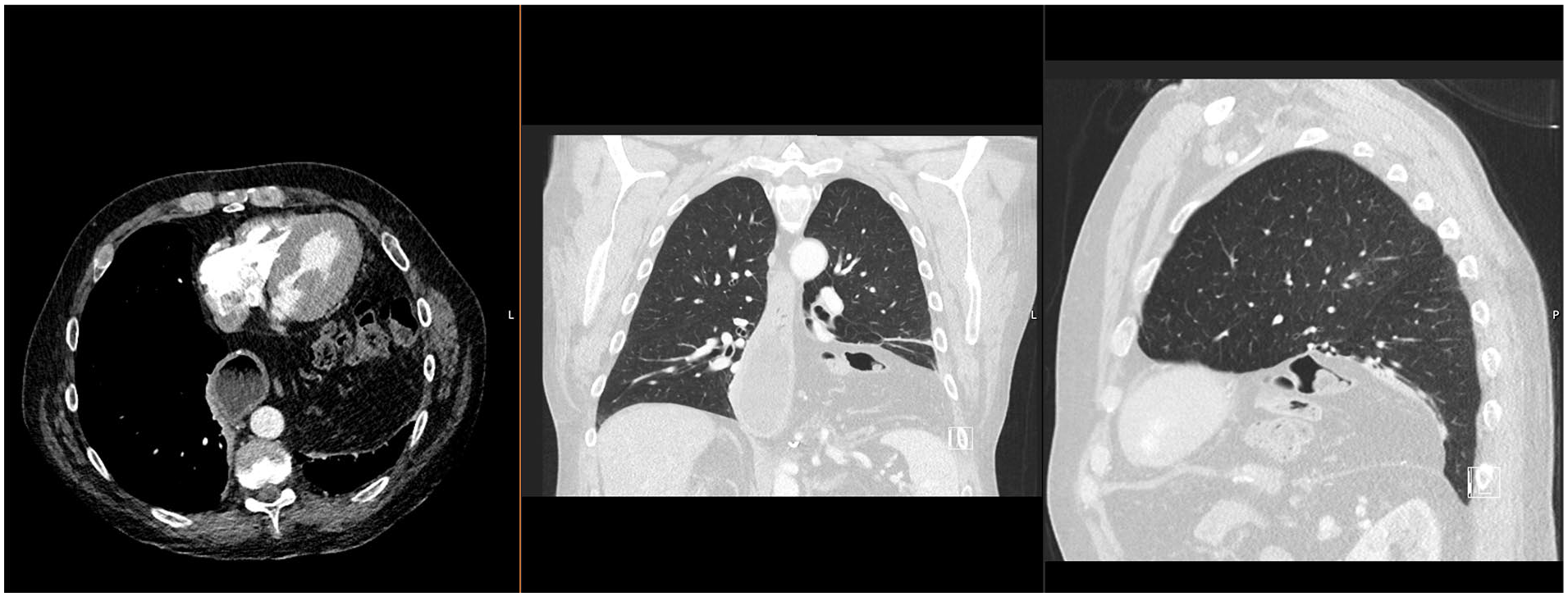
Large paraconduit hernia in a patient with distal esophageal adenocarcinoma who is status post minimally invasive transhiatal esophagectomy with gastric pull-up. Colon and other peritoneal contents can be seen in the thoracic cavity leading to pulmonary and cardiac compression.
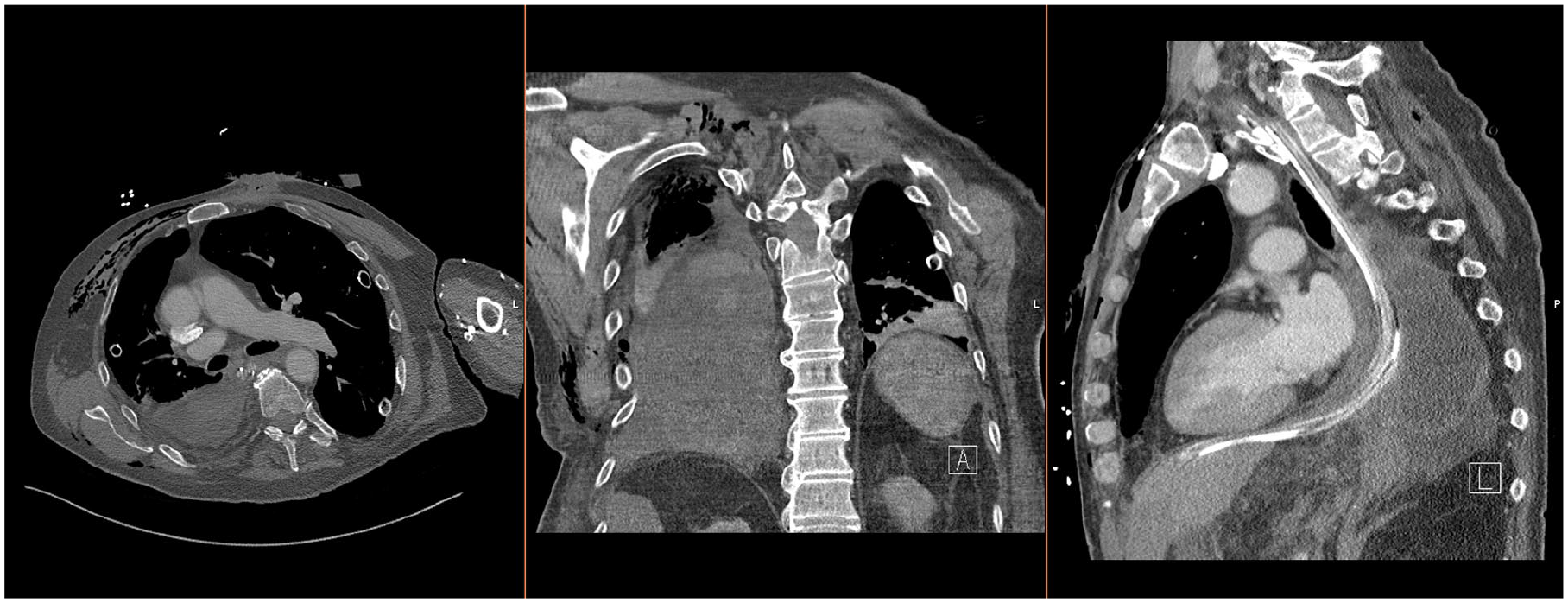
Patient with gastric volvulus secondary to paraconduit hernia leading to gastric ischemia, necrosis, and perforation. There are gastric contents in the pleural cavity with the sagittal view demonstrating fluid outside of the area of the nasogastric tube.
Regardless of the surgical approach employed, there are several other risk factors that might predispose to the development of PCHH for esophageal cancer patients, including preoperative hiatal hernia, diaphragmatic resection, postoperative wretching, neoadjuvant treatment, and transhiatal approach.
In a study by Iwasaki et al, 11 nearly 90% of the patients in their cohort that developed PCHH had pre-operative chemoradiotherapy. 8 These observations are supported by other small scale retrospective analyses.12-15 However, there is a considerable debate in the literature regarding the effect of neoadjuvant therapy on development of PCHH. Lung et al 10 demonstrated that in their cohort preoperative treatment, particularly with radiation, led to decrease in PCHH risk. There are no prospective studies evaluating risk factors for post esophagectomy hiatal hernia. Our group reviewed postoperative follow up imaging in 258 patients at a median of 2 years post esophagectomy and found that 79 had hiatal herniation of bowel (31%). 16 On univariate analysis, neoadjuvant therapy, higher clinical tumor stage, minimally invasive approach, and transhiatal approach were all significantly associated with the development of hernia. On multivariate analysis the only significant factors were neoadjuvant therapy and transhiatal approach.
Management of PCHH
PCHH management is guided by patients’ functional status, effect on the quality of life, and presence of emergent findings. 8 Recurrence is common after repair and most patients can be managed nonoperatively. In our study, 56% of the 79 patients with paraconduit hernia had symptoms that might have been related to the hernia, but only 17 patients (22%) underwent surgical repair and none of the 79 patients died of complications related to the hernia or repair. The most common indications for repair of PCHH are pain (chronic or acute), exertional dyspnea related to mass effect, and bowel obstruction. Acute pain and bowel obstruction should prompt operation. Repair of PCHH can be difficult both for the surgeon and the patient. Herniated colon is usually adherent to surrounding structures but herniated small bowel may be free and easily reduced. If symptoms are thought to be due to the volume of herniated small bowel (lung compression or small bowel obstruction), laparoscopic reduction and closure of the hiatal defect (to the left of the conduit) with omentum and/or mesh can be effective and quite durable. The largest hernias require a thoracoabdominal approach. Dissection/reduction of hernia contents can put the conduit blood supply at risk. Rarely bowel and/or conduit necrosis (Figure 2) requires a damage control approach with foregut diversion and defunctionalization (esophagostomy and gastrostomy/enterostomy). Ensuring that there is no oncologic recurrence via endoscopic and cross-sectional imaging techniques are paramount prior to elective surgical intervention for PCHH.
Surgically Correctable Conduit Stasis
Though vagus sparing esophagectomy has been described, typically the gastric conduit is vagotomized leading to abnormalities in gastric peristalsis and antropyloric function. This together with the pressure dynamics between the chest and abdomen conspire to cause delayed emptying of the gastric conduit in most esophagectomy patients. In those who are severely symptomatic (major weight loss, recurrent aspiration pneumonia, intractable vomiting, stercoral ulceration, etc), a search should be made for potentially surgically correctable causes including pyloric spasm, conduit redundancy or tortuosity, hiatal constriction, and conduit twist. Most patients with the latter 2 problems have been symptomatic since the esopohagectomy, while those with the former 2 problems tend to get worse over time. In patients thought to have conduit stasis possibly amenable to operation, EGD, barium swallow, and emptying scintigraphy are informative. If pyloric spasm is thought to be the diagnosis and Botox injection improves symptoms, then G-poem or operation (pyloroplasty or Roux drainage of the prepyloric antrum) should be considered. Severe hiatal constriction requires abdominal operation (open or laparoscopic) to cut the hiatal ring (usually anteriorly or on the left side) without injuring or devascularizing the conduit. Endoscopic dilation or stenting does not work well for constriction of the conduit by a hiatal aperture that is too small. Both a chronic twist in the conduit and ischemic stricture might respond to stenting and remodeling. Surgical options include gastro-gastrostomy, stricturoplasty, segmental resection, and conduit replacement or substernal bypass with colon interposition.
Redundant conduit is more complicated. This condition is physiologically equivalent to end-stage achalasia. 17 Kent et al 17 have proposed various factors that lead to redundancy in the conduit, which include 7 : (1) excess conduit (often associated with an esophagogastric anastomosis placed too low in the left or right chest—this is usually evident on early postoperative imaging studies); (2) Mechanical obstruction (pyloric spasm, hiatal constriction, distal twist; and (3) gastric dysmotility leading to functional outflow obstruction.
Redundant conduits lead to lack of emptying from the horizontal redundant portion of the neo-esophagus. Ultimately, this can lead to dysphagia and recurrent aspiration causing significant morbidity in these patients. The diagnosis can be corroborated endoscopically, and by CT scan, and barium swallow study. Some studies interpreted as “redundant conduit” require no treatment (figure 3) Kent et al, in their retrospective analysis demonstrated that temporary endoluminal stent placement can alleviate these symptoms but >90% of their patients required surgical revision. In this instance, tubularizing the conduit and removing excess gastric tissue may provide durable symptom relief. 17 Injury to the gastroepiploic arcaded is avoided.

“Redundant stomach” near the conduit anastomosis after transhiatal esophagectomy usually requires no treatment.
If severe foregut symptoms are thought to be due to a redundant colon interposition, consideration can be given to surgical tubularization or sleeve resection. But the care team must realize that injury to the blood supply may sentence the patient to another colon interposition graft or jejunal free graft.
Twisting
During esophagectomy, the gastric conduit is appropriately oriented prior to delivery into the thoracic cavity. However, during this transition, the conduit could be twisted and anastomosed in an incorrect orientation.17,18 Patients with >180° of twist typically develop ischemia above the twist while those with <180° twist usually develop regurgitation and severe dysphagia shortly after the procedure. 19 The diagnosis is made using cross sectional imaging where the lesser curvature conduit staple line does not appear in the correct position. 17 Additionally, endoscopic evaluation can demonstrate swirling of the rugal folds above the twist. 17 Similar to redundant conduit, the twisting does not usually respond to endoscopic palliation long term and often necessitates surgical revision. 20
Dysplasia and gastric conduit adenocarcinoma (GCA)
Given its rich blood supply, ample length, technical ease of harvesting for tension free anastomosis, approximately 90% of esophageal replacement conduits are gastric.21,22 However, the distal stomach used in reconstruction remains at risk for de novo adenocarcinoma development, the incidence of which is debated, ranging between 0.2% and 3.5%.21,22 Putative risk factors include helicobacter, bile reflux, and genetics. The majority of the primary cancers in the tubulirized gastric conduit are distal. It should be noted that a significant portion of the reported results are from parts of the world where gastric adenocarcinoma is endemic; thus GCA risk might not be related to esophagectomy status.
Patients with symptomatic GCA are often advanced stage and prognosis remains poor. Most survival benefit from treatment has been in patients with incidental early-stage gastric tube carcinoma detected on screening endoscopy.21,23-26 Ho et al describe the use of narrow-band imaging and chemoendoscopy (Lugol’s iodine and indigo carmine) for identifying concerning lesions. Most early GCA can be treated endoscopically, usually with endoscopic submucosal dissection (ESD)21,22 but complication rates are appreciable (bleeding, perforation, stricture). Transthoracic (not transhiatal) completion gastrectomy and colon interposition may be of benefit to a small number of well selected patients. 22
Gastric conduit reflux
Acid reflux
Reflux disease is thought to be an unavoidable side-effect of gastric conduit reconstruction,27-31 since the LES is resected and the vagotomized stomach is transposed into the chest. Many post-esophagectomy patients report GI side effects that affect their quality of life (QOL), most commonly regurgitation (~40%), delayed gastric emptying (DGE) (37%), dumping syndrome (21.4%). 28 Dysphagia, chest pain, and atypical respiratory symptoms are also not uncommon. Troublesome gastroesophageal reflux into the residual esophagus is surprisingly uncommon if the GE anastomosis is high in the chest or in the neck, but quite common if the anastomosis is low in the chest. Troublesome symptoms thought to be due to acid GE reflux can be treated empirically with high dose PPI. If there is no improvement, EGD and pH impedance should be considered off acid suppression. If acid GE reflux is confirmed, a strong attempt should be made to manage this with diet and PPI (and perhaps prokinetics). If there is nothing seriously wrong with the gastric conduit, and the anastomosis is appropriately high, there is generally no role for surgery except in the rare patient where completion gastrectomy and colon interposition may be warranted. If the acid GE reflux is associated with a surgically correctable conduit issue (vide supra) or low thoracic GE anastomosis, then operation may be considered.28,32,33 Most surgeons keep postesophagectomy patients on acid suppressive medication.
Bile reflux
Some esophagectomy patients with debilitating chest pain, heartburn, regurgitation, and/or nausea/vomiting will have abnormal duodenogastric reflux (Figure 4). In these patients, typically the vomitus or refluxate contains bile, there is bile pooling in the gastric conduit on EGD, and/or the pH/impedance study shows nonacid reflux into the proximal conduit or remaining esophagus. After esophagectomy with gastric conduit, abnormal chronic duodenogastric reflux may occur whether or not a pyloroplasty has been performed. Once thought necessary to avoid vagotomy associated gastric stasis following esophagectomy, pyloroplasty is no longer routinely performed because of both the concern for bile reflux and its questionable effect on gastric emptying.
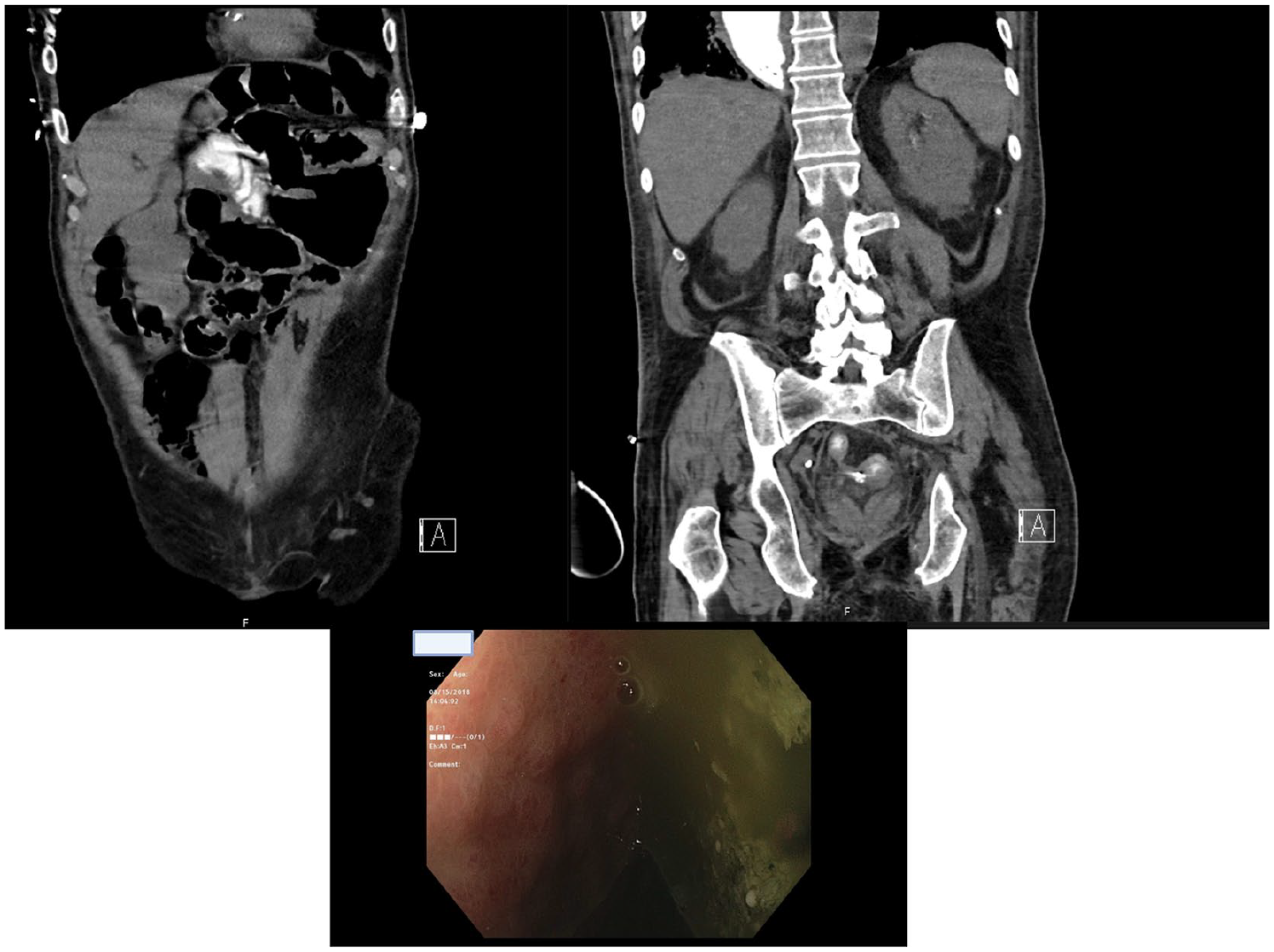
Patient status post esophagectomy and J-tube placement with contrast given through J tube (top left). Contrast seen refluxing into the conduit (top right). Endoscopic evaluation demonstrated bile pooling in the conduit (bottom).
Some patients with chronic bilious vomiting, food intolerance, and chest pain after esophagectomy will benefit from an operation to keep the bile out of the gastric conduit and facilitate conduit drainage. Perhaps about 3% of patients who (1) are at least 6 months post esophagectomy with gastric pull-up and (2) otherwise have a good prognosis, might be candidates for this operation. Using an abdominal approach and avoiding damage to the right gastroepiploic pedicle, the duodenum is divided with a GIA stapler just distal to the pylorus. A 60-cm Roux limb is then anastomosed to the prepyloric antrum. Preoperative imaging will confirm the location of the pylorus which is rarely above the diaphragm so the addition of a thoracotomy is rarely if ever needed. We have done this operation several times with good results. D’Journo et al 30 reported 80% improvement in subjective symptoms using the diversion approach in their case series. It is also a useful option for patients with debilitating bile reflux after a proximal gastrectomy with esophago-antrostomy.
Tracheobronchial-conduit fistula
Although a rare complication (0.3%-0.5%), tracheobronchial-conduit fistula (colonic or gastric) is a life-threatening finding that requires urgent detection and intervention. Literature on this entity is mainly limited to case reports.34-36
The primary cause of tracheobronchial fistulas after esophagectomy is anastomotic leak leading to peri-conduit inflammation and erosion into the airway.34,35 Partial thickness damage and/or ischemia to the membranous portion of trachea or main stem bronchi during esophagectomy may also play a role. Stenting for esophageal anastomotic leaks and vigorous dilation of proximal esophageal anastomotic strictures have also been implicated. Fistulas secondary to anastomotic complications are mostly found as an upper tracheal lesion while fistulas due to conduit leak and/or necrosis are found as lower tracheal or main stem bronchial lesions. The patients usually present with cough (often worse with drinking or eating), and recurrent pneumonia. Some patients present with respiratory failure, pulmonary sepsis, and life threatening mediastinitis.
Diagnostic testing for this condition should be started swiftly shortly after clinical suspicion arises. Cross sectional imaging with oral contrast can demonstrate the fistula which can be confirmed with flouroscopic studies. Larger fistulas can be visualized from both sides with GI endoscopy and bronchoscopy. 37
Given the rarity of this condition, there are no standardized treatment options that are supported by literature. Treatments can be divided into conservative care which includes endoscopic placement of a covered stent into the conduit with clip or covering the airway orifice with a stent if the location of the fistula allows. (Figure 5) A small case series reported the use of histoacryl based skin glues to successfully plug the fistula. 35 If the patient does not respond to conservative approaches, surgical intervention could be attempted. Nardella et al 34 demonstrated successful closure of both fistulous connections through a right thoracotomy.
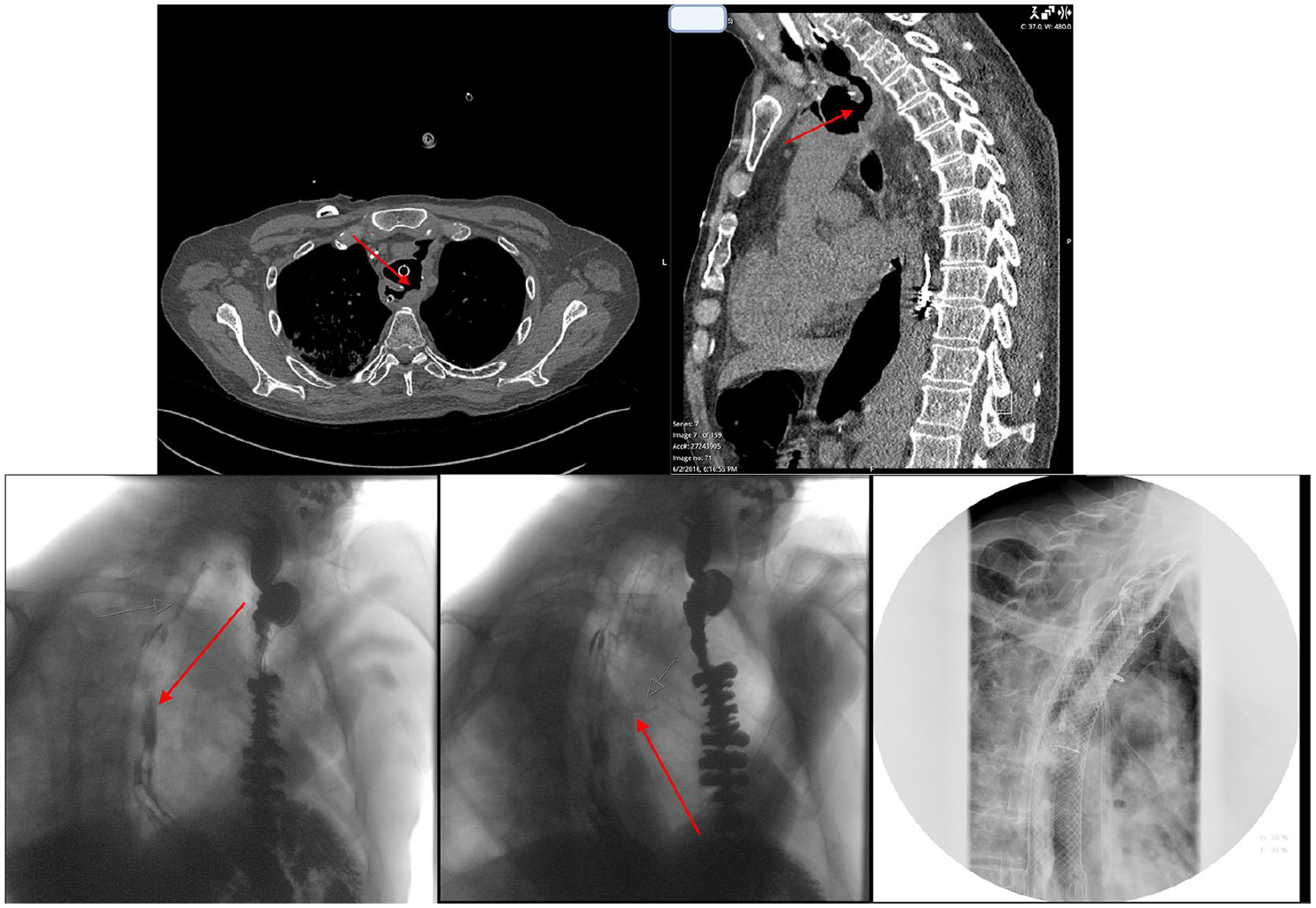
(Top) Patient with a tracheoesophageal fistula after a colonic transposition (Red arrows demonstrate fistulus connection between conduit and tracheal orifice.
Additionally some have reported successful closure using musculocutaneous flaps including sternocleidomastoid muscle, pectoralis major muscle, and intercostal muscles. Regardless, the condition remains highly fatal with nearly 50% peri-hospital mortality, further underscoring the necessity of early diagnosis and referral to experienced specialists. We have successfully managed 3 patients with life threatening airway fistulas (2 between the esophagogastric anastomosis and the trachea, and 1 between the gastric conduit and the right main stem bronchus) by defunctionalizing the conduit (disconnect from esophagus above and pylorus below with Roux to antrum) and re-establishing continuity with substernal colon interposition between the cervical esophagus and jejunum.
Conclusion
Because of improved long-term survival after esophagectomy, once rare long-term complications potentially amenable to surgical correction are becoming more common. These problems include hiatal herniation, conduit stasis, bile reflux, and airway fistula. Careful patient selection for a well-planned operation, together with management of both care team and patient expectations, will optimize clinical outcomes in this difficult group.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Azari was supported by the training grant in Surgical Oncology by the National Institutes of Health (T32CA251063-01), the Society of Thoracic Surgeons Thoracic Surgery Foundation Research Award, and the Stephen CC Cheung Fellowship in Surgical Oncology. Dr. Kennedy was supported by the American Philosophical Society and the National Institutes of Health (grant F32 CA254210-01).